
Relationship between Dietary Magnesium Intake and Metabolic Syndrome

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
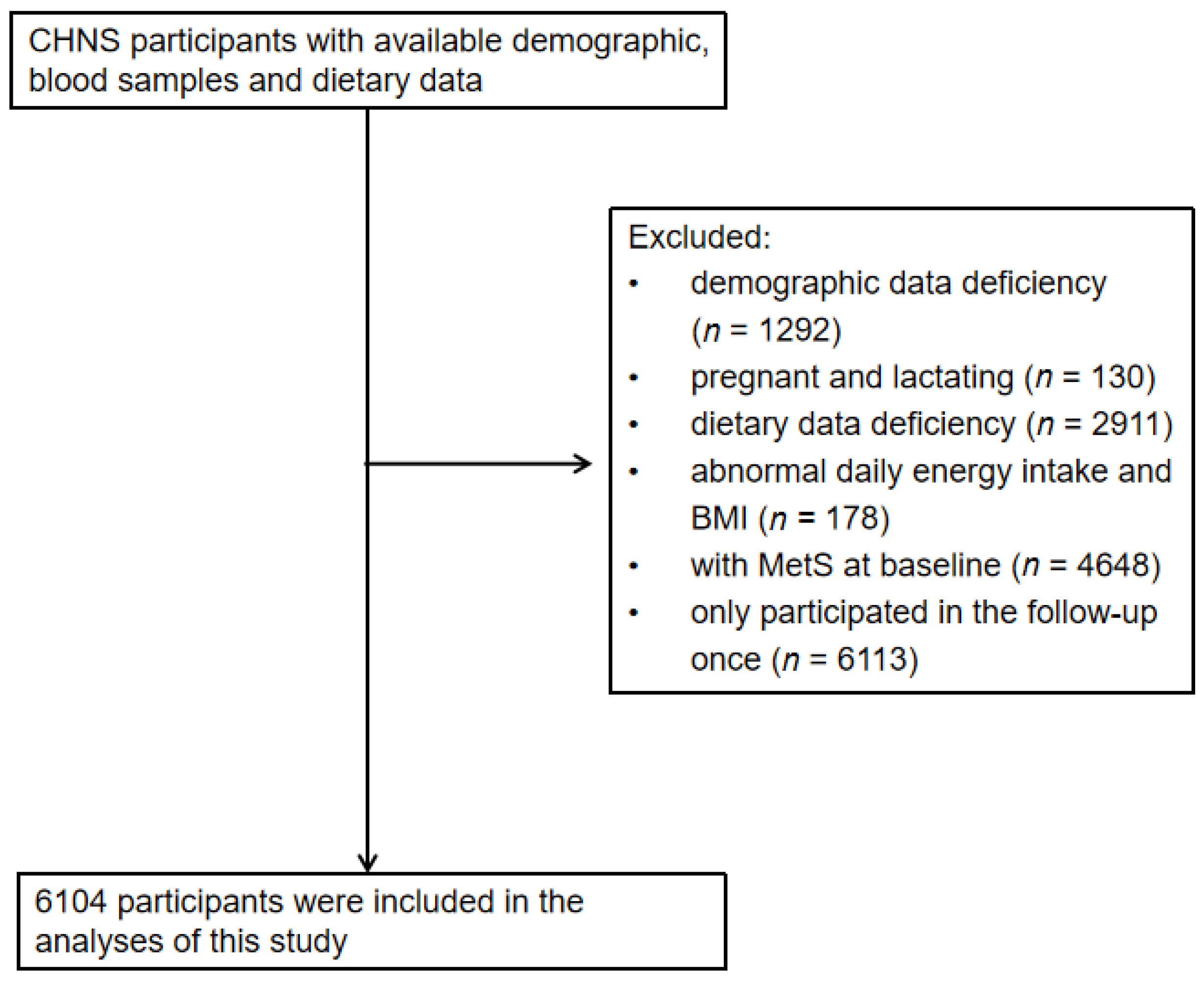
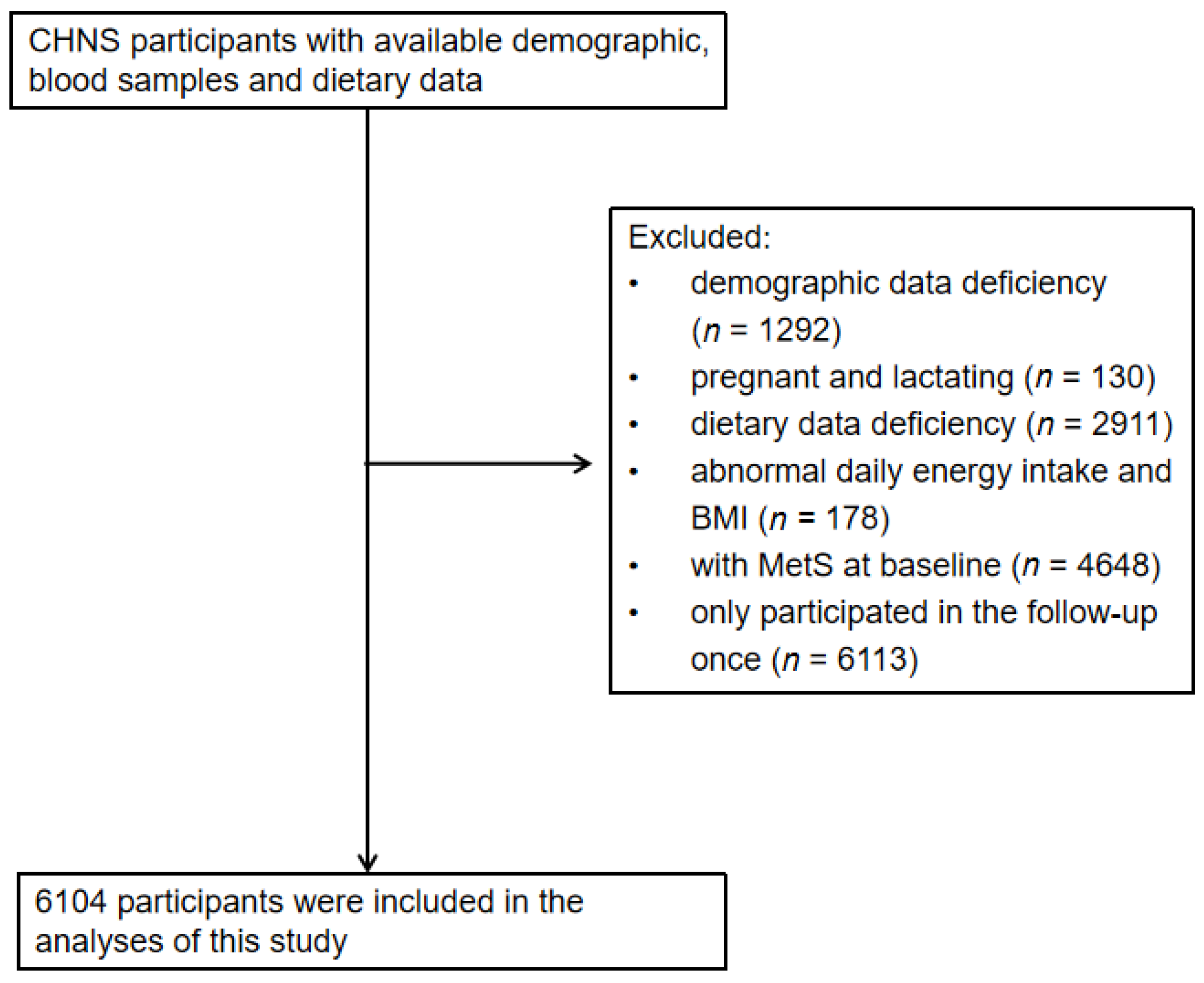
2.1. Study Design and Subjects
2.2. Evaluation Indicators
2.2.1. Dietary Nutrients
2.2.2. Diagnostic Criteria for MetS
2.2.3. Measurement of Indicators
2.2.4. Other Variables
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Multivariate Cox Proportional Risk Regression Analysis of Dietary Magnesium Intake to MetS and Its Components
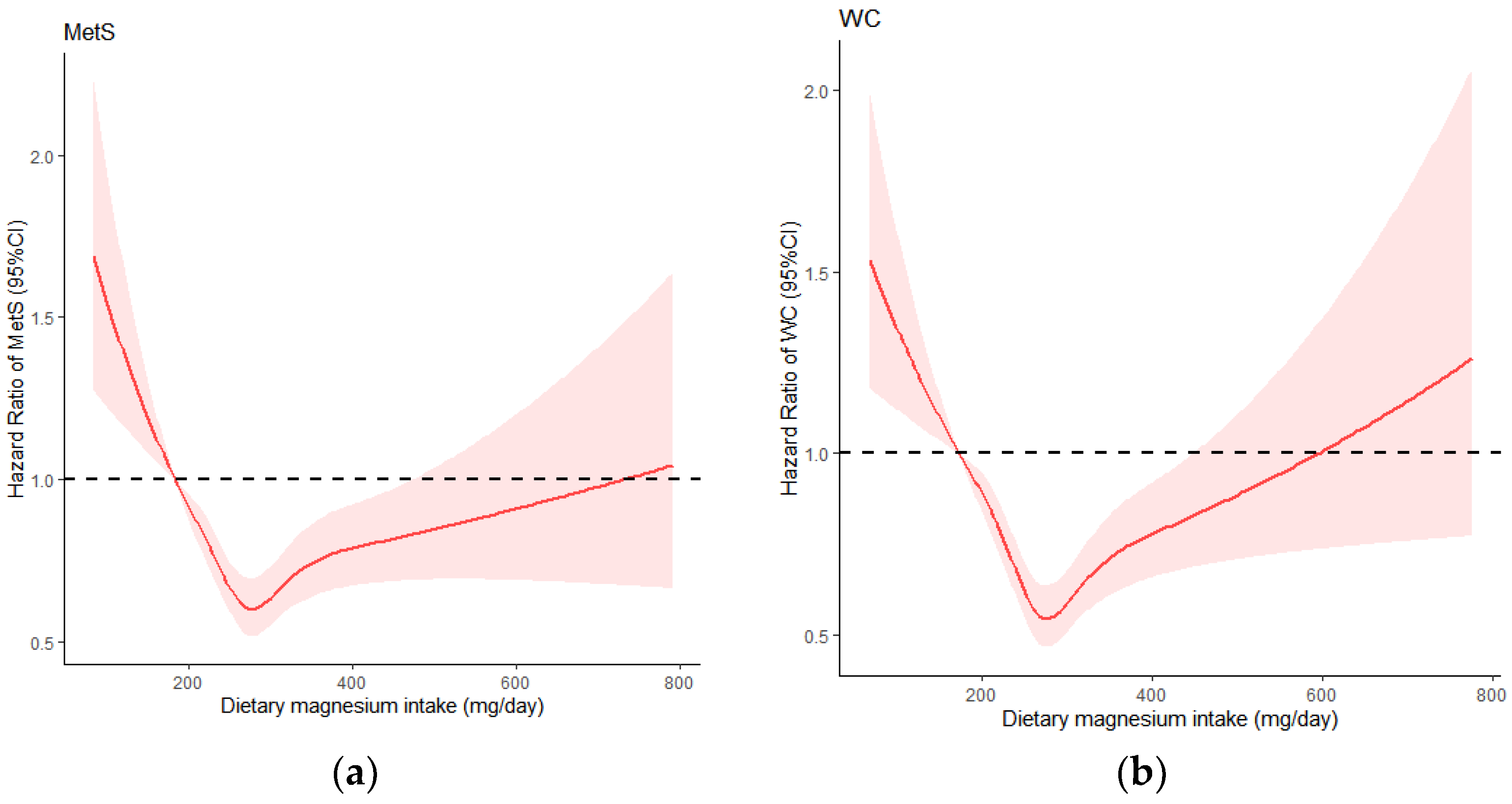
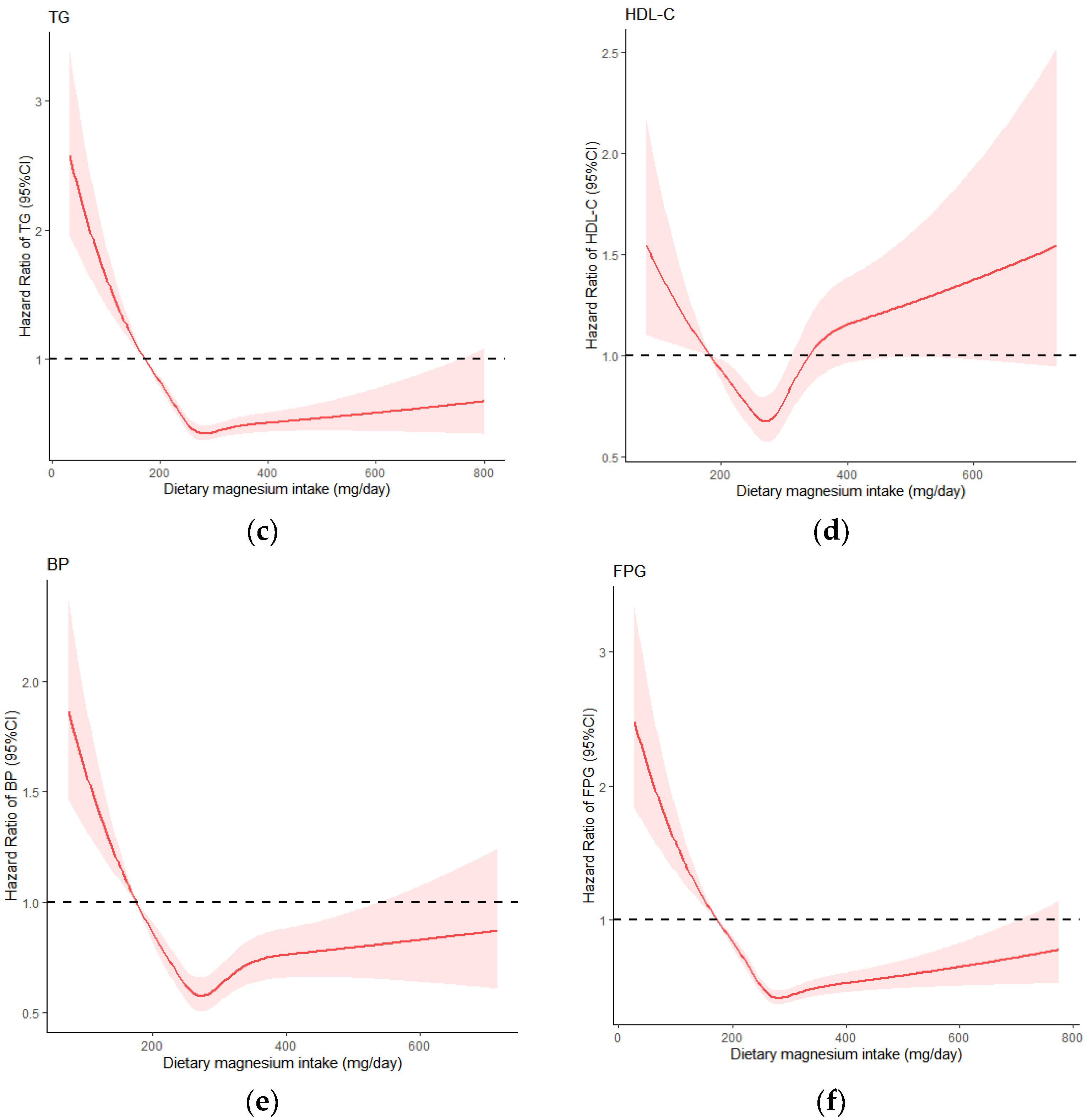
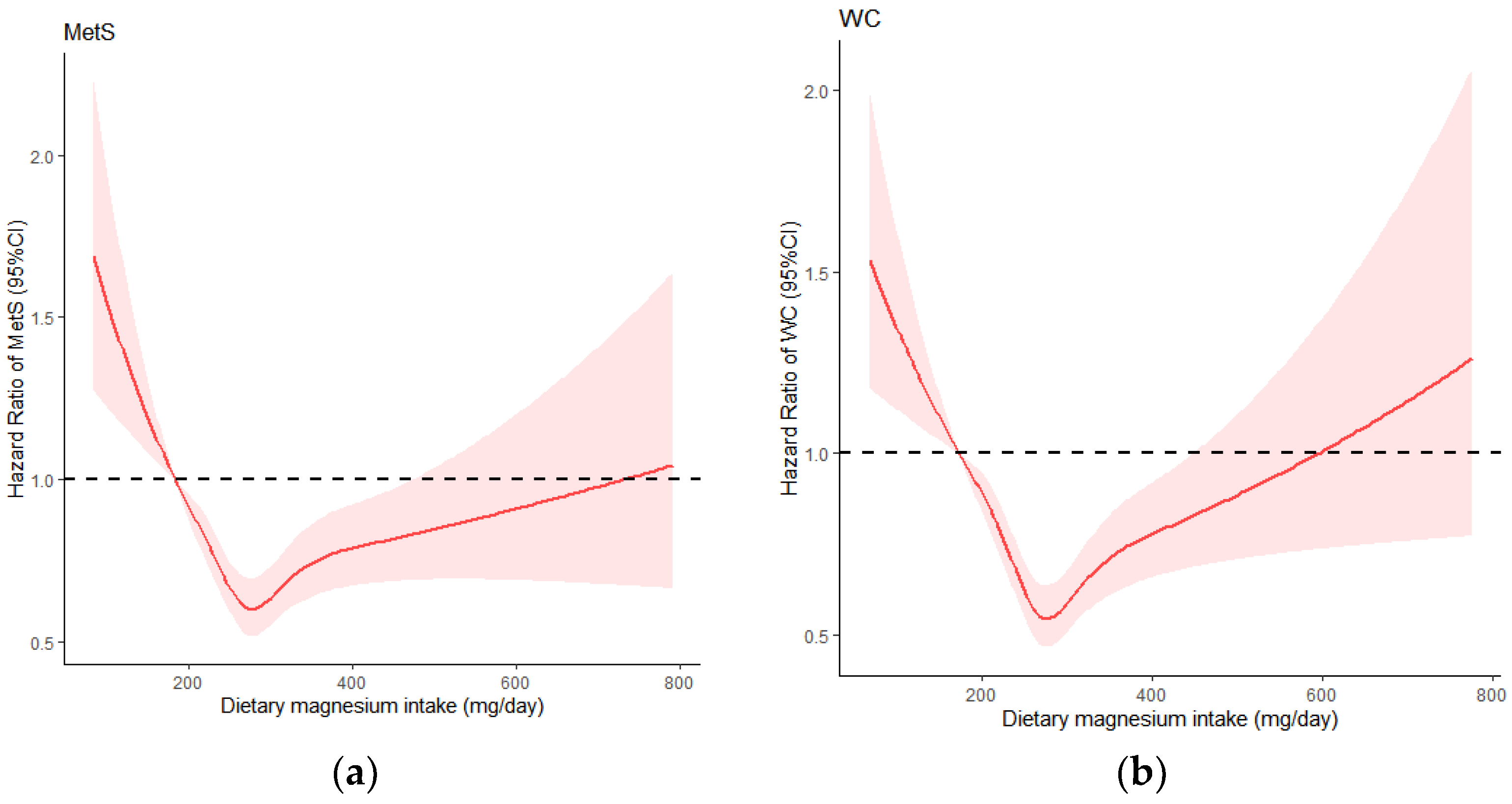
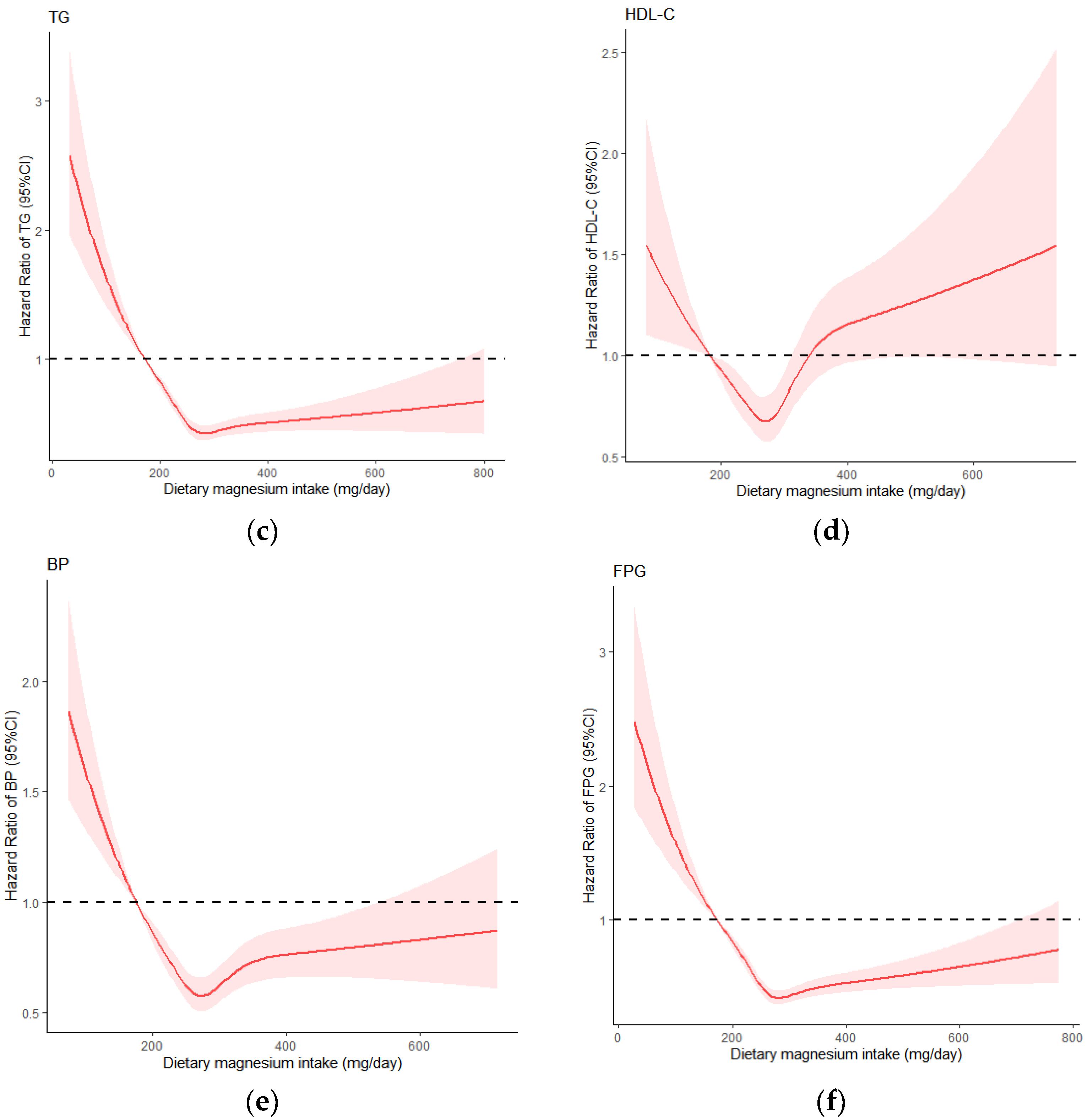
3.3. Dose-Response Relationship between Dietary Magnesium Intake and MetS and Its Components
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C.; et al. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De la Iglesia, R.; Loria-Kohen, V.; Zulet, M.A.; Martinez, J.A.; Reglero, G.; Ramirez de Molina, A. Dietary Strategies Implicated in the Prevention and Treatment of Metabolic Syndrome. Int. J. Mol. Sci. 2016, 17, 1877. [Google Scholar] [CrossRef] [Green Version]
- He, Y.-N.; Zhao, W.-H.; Zhao, L.-Y.; Yu, D.-M.; Zhang, J.; Yang, X.-G.; Ding, G.-Q. Prevalence of metabolic syndrome in Chinese adults in 2010–2012. Chin. J. Epidemiol. 2017, 38, 212–215. [Google Scholar] [CrossRef]
- Wu, W.; Chen, S.-Y.; Ji, G.-Y.; Tu, H.-W.; Zheng, C.-J. Correlation analysis between metabolic syndrome and dietary nutrients in adult residents. China Food Saf. Mag. 2020, 76–80. [Google Scholar] [CrossRef]
- Ford, E.S.; Li, C.; McGuire, L.C.; Mokdad, A.H.; Liu, S. Intake of dietary magnesium and the prevalence of the metabolic syndrome among U.S. adults. Obesity 2007, 15, 1139–1146. [Google Scholar] [CrossRef]
- Tarleton, E.K. Factors influencing magnesium consumption among adults in the United States. Nutr. Rev. 2018, 76, 526–538. [Google Scholar] [CrossRef]
- Dibaba, D.T.; Xun, P.; He, K. Dietary magnesium intake is inversely associated with serum C-reactive protein levels: Meta-analysis and systematic review. Eur. J. Clin. Nutr. 2014, 68, 510–516. [Google Scholar] [CrossRef] [Green Version]
- Găman, M.A.; Dobrică, E.C.; Cozma, M.A.; Antonie, N.I.; Stănescu, A.; Găman, A.M.; Diaconu, C.C. Crosstalk of Magnesium and Serum Lipids in Dyslipidemia and Associated Disorders: A Systematic Review. Nutrients 2021, 13, 1411. [Google Scholar] [CrossRef]
- Banjanin, N.; Belojevic, G. Relationship of dietary magnesium intake and serum magnesium with hypertension: A review. Magnes Res. 2021, 34, 166–171. [Google Scholar] [CrossRef]
- Houston, M. The role of magnesium in hypertension and cardiovascular disease. J. Clin. Hypertens. 2011, 13, 843–847. [Google Scholar] [CrossRef]
- Sarrafzadegan, N.; Khosravi-Boroujeni, H.; Lotfizadeh, M.; Pourmogaddas, A.; Salehi-Abargouei, A. Magnesium status and the metabolic syndrome: A systematic review and meta-analysis. Nutrition 2016, 32, 409–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ju, S.Y.; Choi, W.S.; Ock, S.M.; Kim, C.M.; Kim, D.H. Dietary magnesium intake and metabolic syndrome in the adult population: Dose-response meta-analysis and meta-regression. Nutrients 2014, 6, 6005–6019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dibaba, D.T.; Xun, P.; Fly, A.D.; Yokota, K.; He, K. Dietary magnesium intake and risk of metabolic syndrome: A meta-analysis. Diabet Med. 2014, 31, 1301–1309. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.K.; Bae, Y.J. Relationship between dietary magnesium, manganese, and copper and metabolic syndrome risk in Korean adults: The Korea National Health and Nutrition Examination Survey (2007–2008). Biol. Trace Elem. Res. 2013, 156, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Noori, N.; Nafar, M.; Poorrezagholi, F.; Ahmadpoor, P.; Samadian, F.; Firouzan, A.; Einollahi, B. Dietary intakes of fiber and magnesium and incidence of metabolic syndrome in first year after renal transplantation. J. Ren. Nutr. 2010, 20, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Huang, Q.-M.; Wang, L.-S.; Zhang, B. Wan (autonomous regions) of China from 1991 to 2015. J. Environ. Occup. Med. 2019, 36, 410–417. [Google Scholar] [CrossRef]
- The China Health and Nutrition Survey Research Team. The trends of nutrients intake of Chinese residents in nine provinces from 1989 to 2009(I) “the China health and nutrition survey” project design. Acta Nutr. Sin. 2011, 33, 234–236. [Google Scholar] [CrossRef]
- Popkin, B.M.; Du, S.; Zhai, F.; Zhang, B. Cohort Profile: The China Health and Nutrition Survey--monitoring and understanding socio-economic and health change in China, 1989–2011. Int. J. Epidemiol. 2010, 39, 1435–1440. [Google Scholar] [CrossRef] [Green Version]
- Zhang, B.; Wang, H.-J.; Du, W.-W.; Zhang, J.-G.; Su, C.; Wang, Z.-H.; Liu, A.-D.; Ma, Y.-X. Progress in cohort studies and its implications for China health and Nutrition Survey. Chin. J. Prev. Med. 2011, 45, 295–298. [Google Scholar] [CrossRef]
- Yang, Y.-X.; He, M.; Pan, X.-C. Chinese Food Composition Table 2004; Peking University Medical Press: Beijing, China, 2004. [Google Scholar]
- Yang, Y.-X.; Wang, G.-Y.; Pan, X.-C. Chinese Food Composition Table; Peking University Medical Press: Beijing, China, 2009. [Google Scholar]
- Willett, W.C.; Howe, G.R.; Kushi, L.H. Adjustment for total energy intake in epidemiologic studies. Am. J. Clin. Nutr. 1997, 65, 1220S–1231S. [Google Scholar] [CrossRef]
- Ng, S.W.; Popkin, B.M. Time use and physical activity: A shift away from movement across the globe. Obes. Rev. 2012, 13, 659–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sallis, J.F.; Haskell, W.L.; Wood, P.D.; Fortmann, S.P.; Rogers, T.; Blair, S.N.; Paffenbarger, R.S. Physical activity assessment methodology in the Five-City Project. Am. J. Epidemiol. 1985, 121, 91–106. [Google Scholar] [CrossRef] [PubMed]
- He, K.; Liu, K.; Daviglus, M.L.; Morris, S.J.; Loria, C.M.; Van Horn, L.; Jacobs, D.R.; Savage, P.J., Jr. Magnesium intake and incidence of metabolic syndrome among young adults. Circulation 2006, 113, 1675–1682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Daghri, N.M.; Khan, N.; Alkharfy, K.M.; Al-Attas, O.S.; Alokail, M.S.; Alfawaz, H.A.; Alothman, A.; Vanhoutte, P.M. Selected dietary nutrients and the prevalence of metabolic syndrome in adult males and females in Saudi Arabia: A pilot study. Nutrients 2013, 5, 4587–4604. [Google Scholar] [CrossRef] [Green Version]
- Bo, S.; Durazzo, M.; Guidi, S.; Carello, M.; Sacerdote, C.; Silli, B.; Rosato, R.; Cassader, M.; Gentile, L.; Pagano, G. Dietary magnesium and fiber intakes and inflammatory and metabolic indicators in middle-aged subjects from a population-based cohort. Am. J. Clin. Nutr. 2006, 84, 1062–1069. [Google Scholar] [CrossRef] [Green Version]
- Mirmiran, P.; Shab-Bidar, S.; Hosseini-Esfahani, F.; Asghari, G.; Hosseinpour-Niazi, S.; Azizi, F. Magnesium intake and prevalence of metabolic syndrome in adults: Tehran Lipid and Glucose Study. Public Health Nutr. 2012, 15, 693–701. [Google Scholar] [CrossRef] [Green Version]
- Yang, N.; He, L.; Li, Y.; Xu, L.; Ping, F.; Li, W.; Zhang, H. Reduced Insulin Resistance Partly Mediated the Association of High Dietary Magnesium Intake with Less Metabolic Syndrome in a Large Chinese Population. Diabetes Metab. Syndr. Obes. 2020, 13, 2541–2550. [Google Scholar] [CrossRef]
- Roberts, C.K.; Sindhu, K.K. Oxidative stress and metabolic syndrome. Life Sci. 2009, 84, 705–712. [Google Scholar] [CrossRef]
- Piuri, G.; Zocchi, M.; Della Porta, M.; Ficara, V.; Manoni, M.; Zuccotti, G.V.; Pinotti, L.; Maier, J.A.; Cazzola, R. Magnesium in Obesity, Metabolic Syndrome, and Type 2 Diabetes. Nutrients 2021, 13, 320. [Google Scholar] [CrossRef]
- Corre, T.; Arjona, F.J.; Hayward, C.; Youhanna, S.; de Baaij, J.; Belge, H.; Nägele, N.; Debaix, H.; Blanchard, M.G.; Traglia, M.; et al. Genome-Wide Meta-Analysis Unravels Interactions between Magnesium Homeostasis and Metabolic Phenotypes. J. Am. Soc. Nephrol. 2018, 29, 335–348. [Google Scholar] [CrossRef]
- Castellanos-Gutiérrez, A.; Sánchez-Pimienta, T.G.; Carriquiry, A.; da Costa, T.; Ariza, A.C. Higher dietary magnesium intake is associated with lower body mass index, waist circumference and serum glucose in Mexican adults. Nutr. J. 2018, 17, 114. [Google Scholar] [CrossRef] [PubMed]
- Han, H.; Fang, X.; Wei, X.; Liu, Y.; Jin, Z.; Chen, Q.; Fan, Z.; Aaseth, J.; Hiyoshi, A.; He, J.; et al. Dose-response relationship between dietary magnesium intake, serum magnesium concentration and risk of hypertension: A systematic review and meta-analysis of prospective cohort studies. Nutr. J. 2017, 16, 26. [Google Scholar] [CrossRef] [PubMed]
- Xu, T.; Chen, G.C.; Zhai, L.; Ke, K.F. Nonlinear Reduction in Risk for Type 2 Diabetes by Magnesium Intake: An Updated Meta-Analysis of Prospective Cohort Studies. Biomed. Environ. Sci. 2015, 28, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, F.H. Guidance for the determination of status indicators and dietary requirements for magnesium. Magnes Res. 2016, 29, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, F.H. Dietary Magnesium and Chronic Disease. Adv. Chronic. Kidney Dis. 2018, 25, 230–235. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Quintile of Dietary Magnesium Intake (mg/day) | ||||||
|---|---|---|---|---|---|---|
| Q1 (<225.89 mg/day) | Q2 (225.89~256.12 mg/day) | Q3 (256.12~287.23 mg/day) | Q4 (287.23~329.91 mg/day) | Q5 (≥329.91 mg/day) | p-Value | |
| Age, % | 0.22 | |||||
| 18~49 | 51.31 | 53.48 | 51.92 | 48.98 | 48.81 | |
| 50~64 | 36.15 | 33.82 | 33.58 | 36.61 | 37.10 | |
| 65~ | 12.54 | 12.69 | 14.50 | 14.41 | 14.09 | |
| Male, % | 49.51 | 44.64 | 45.37 | 45.45 | 46.36 | 0.13 |
| Household incomeper capita, % | <0.05 | |||||
| Low | 27.62 | 31.20 | 34.97 | 36.20 | 36.69 | |
| Median | 31.72 | 30.30 | 35.30 | 35.22 | 34.07 | |
| High | 40.66 | 38.49 | 29.73 | 28.58 | 29.24 | |
| Education, % | <0.05 | |||||
| Primary and below | 33.61 | 32.19 | 36.94 | 37.18 | 40.13 | |
| Middle and high | 47.62 | 46.19 | 46.6 | 46.93 | 45.21 | |
| College and above | 18.77 | 21.62 | 16.46 | 15.89 | 14.66 | |
| Urban, % | 30.49 | 33.82 | 37.26 | 34.73 | 34.97 | <0.05 |
| Never smoked, % | 70.82 | 71.25 | 70.68 | 69.7 | 71.01 | 0.93 |
| Never drunk alcohol, % | 68.77 | 67.73 | 68.39 | 68.39 | 67.98 | 0.99 |
| Physical activity, % | <0.05 | |||||
| Low | 35.90 | 32.51 | 33.82 | 32.76 | 31.61 | |
| Median | 35.33 | 36.45 | 33.01 | 31.37 | 30.55 | |
| High | 28.77 | 31.04 | 33.17 | 35.87 | 37.84 | |
| BMI (kg/m2), % | 0.08 | |||||
| <18.5 | 6.72 | 7.21 | 6.63 | 7.37 | 5.16 | |
| 18.5~23.9 | 62.46 | 60.85 | 62.65 | 59.79 | 59.05 | |
| ≥24.0 | 30.82 | 31.94 | 30.71 | 32.84 | 35.79 | |
| Energy(kcal/day) | 2201.10 ± 795.07 | 2049.50 ± 658.96 | 2014.17 ± 611.07 | 2043.68 ± 625.45 | 2335.93 ± 744.84 | <0.05 |
| Dietary fibre (mg/day) | 9.02 ± 4.68 | 9.86 ± 5.15 | 10.83 ± 5.51 | 12.34 ± 5.67 | 18.44 ± 11.58 | <0.05 |
| Calcium (mg/day) | 295.52 ± 134.24 | 325.25 ± 142.77 | 368.85 ± 221.44 | 406.62 ± 167.17 | 554.98 ± 334.05 | <0.05 |
| WC (cm) | 79.69 ± 10.35 | 79.69 ± 9.66 | 79.85 ± 9.96 | 80.66 ± 9.53 | 80.83 ± 11.62 | <0.05 |
| TG (mmol/L) | 1.19 ± 0.70 | 1.19 ± 0.73 | 1.20 ± 0.73 | 1.19 ± 0.83 | 1.21 ± 0.90 | 0.99 |
| HDL-C(mmol/L) | 1.44 ± 0.34 | 1.47 ± 0.36 | 1.50 ± 0.38 | 1.50 ± 0.50 | 1.49 ± 0.40 | <0.05 |
| SBP (mmHg) | 120.43 ± 15.95 | 120.47 ± 16.43 | 121.58 ± 16.40 | 121.21 ± 16.27 | 122.47 ± 15.00 | <0.05 |
| DBP (mmHg) | 77.43 ± 9,85 | 77.53 ± 9,84 | 78.69 ± 9.92 | 78.29 ± 10.19 | 79.32 ± 9.42 | <0.05 |
| FPG (mmol/L) | 5.09 ± 0.87 | 5.13 ± 1.07 | 5.10 ± 0.87 | 5.02 ± 0.84 | 5.03 ± 0.97 | <0.05 |
| Quintile of Dietary Magnesium Intake (mg/day) | ||||||
|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | Q5 | p trend | |
| Metabolic syndrome a | ||||||
| Median (mg/day) | 202.82 | 242.35 | 271.36 | 305.33 | 370.72 | |
| Model 1 | 1.00 (ref) | 0.77 (0.67, 0.90) * | 0.74 (0.64, 0.85) * | 0.81 (0.70, 0.93) * | 0.91 (0.79, 1.04) | 0.96 |
| Model 2 | 1.00 (ref) | 0.79 (0.68, 0.91) * | 0.76 (0.65, 0.88) * | 0.84 (0.72, 0.96) * | 0.95 (0.82,1.09) | 0.60 |
| Model 3 | 1.00 (ref) | 0.76 (0.65, 0.88) * | 0.72 (0.62, 0.82) * | 0.79 (0.68, 0.92) * | 0.92 (0.78,1.09) | 0.86 |
| Model 4 | 1.00 (ref) | 0.75 (0.64, 0.88) * | 0.69 (0.59, 0.80) * | 0.76 (0.65, 0.88) * | 0.84 (0.71, 0.99) * | 0.32 |
| Central obesity b | ||||||
| Median (mg/day) | 195.81 | 238.45 | 268.15 | 304.03 | 369.22 | |
| Model 1 | 1.00 (ref) | 0.80 (0.69, 0.93) * | 0.65 (0.56, 0.75) * | 0.70 (0.61, 0.81) * | 0.89 (0.77,1.02) | 0.13 |
| Model 2 | 1.00 (ref) | 0.80 (0.69, 0.93) * | 0.66 (0.57, 0.77) * | 0.70 (0.60, 0.81) * | 0.89 (0.77,1.02) | 0.12 |
| Model 3 | 1.00 (ref) | 0.77 (0.66, 0.90) * | 0.63 (0.54, 0.74) * | 0.66 (0.57, 0.78) * | 0.88 (0.74,1.04) | 0.07 |
| Model 4 | 1.00 (ref) | 0.80 (0.68, 0.94) * | 0.64 (0.54, 0.75) * | 0.65 (0.55, 0.77) * | 0.82 (0.69, 0.98) * | <0.05 |
| Elevated TG c | ||||||
| Median (mg/day) | 194.14 | 236.18 | 265.51 | 300.72 | 365.54 | |
| Model 1 | 1.00 (ref) | 0.70 (0.61, 0.80) * | 0.57 (0.50, 0.65) * | 0.57 (0.50, 0.65) * | 0.66 (0.58, 0.75) * | <0.05 |
| Model 2 | 1.00 (ref) | 0.71 (0.62, 0.81) * | 0.59 (0.51, 0.67) * | 0.58 (0.50, 0.66) * | 0.67 (0.59, 0.77) * | <0.05 |
| Model 3 | 1.00 (ref) | 0.66 (0.58, 0.75) * | 0.54 (0.47, 0.62) * | 0.52 (0.45, 0.59) * | 0.60 (0.51, 0.70) * | <0.05 |
| Model 4 | 1.00 (ref) | 0.67 (0.59, 0.77) * | 0.56 (0.49, 0.65) * | 0.52 (0.45, 0.60) * | 0.59 (0.51, 0.70) * | <0.05 |
| Decreased HDL-C d | ||||||
| Median (mg/day) | 202.89 | 243.64 | 273.21 | 307.60 | 371.13 | |
| Model 1 | 1.00 (ref) | 0.93 (0.79,1.10) | 0.78 (0.66, 0.92) * | 0.97 (0.82,1.13) | 1.11 (0.95,1.30) | <0.05 |
| Model 2 | 1.00 (ref) | 0.94 (0.79,1.11) | 0.78 (0.66, 0.92) * | 0.96 (0.82,1.13) | 1.12 (0.95,1.31) | <0.05 |
| Model 3 | 1.00 (ref) | 0.93 (0.78,1.10) | 0.77 (0.65, 0.92) * | 0.98 (0.82,1.16) | 1.23(1.03,1.48) * | <0.05 |
| Model 4 | 1.00 (ref) | 0.91 (0.76,1.09) | 0.77 (0.65, 0.93) * | 0.96 (0.80,1.14) | 1.21(1.00,1.47) * | <0.05 |
| Elevated BP e | ||||||
| Median (mg/day) | 196.72 | 238.93 | 269.01 | 304.21 | 365.07 | |
| Model 1 | 1.00 (ref) | 0.73(0,64, 0.84) * | 0.71 (0.62, 0.81) * | 0.72 (0.64, 0.82) * | 0.83 (0.73, 0.94) * | 0.10 |
| Model 2 | 1.00 (ref) | 0.74 (0.64, 0.84) * | 0.71 (0.62, 0.81) * | 0.72 (0.63, 0.82) * | 0.83 (0.73, 0.94) * | 0.10 |
| Model 3 | 1.00 (ref) | 0.71 (0.62, 0.82) * | 0.68 (0.59, 0.78) * | 0.69 (0.60, 0.79) * | 0.83 (0.71, 0.96) * | 0.16 |
| Model 4 | 1.00 (ref) | 0.72 (0.63, 0.83) * | 0.67 (0.58, 0.77) * | 0.70 (0.61, 0.81) * | 0.80 (0.69, 0.94) * | 0.08 |
| Elevated FPG f | ||||||
| Median (mg/day) | 195.46 | 237.58 | 267.21 | 303.01 | 366.81 | |
| Model 1 | 1.00 (ref) | 0.71 (0.63, 0.80) * | 0.56 (0.50, 0.63) * | 0.57 (0.51, 0.64) * | 0.63 (0.56, 0.70) * | <0.05 |
| Model 2 | 1.00 (ref) | 0.73 (0.64, 0.82) * | 0.57 (0.51, 0.65) * | 0.58 (0.51, 0.65) * | 0.64 (0.57, 0.72) * | <0.05 |
| Model 3 | 1.00 (ref) | 0.68 (0.60, 0.77) * | 0.53 (0.47, 0.60) * | 0.52 (0.46, 0.60) * | 0.60 (0.52, 0.69) * | <0.05 |
| Model 4 | 1.00 (ref) | 0.68 (0.60, 0.77) * | 0.53 (0.46, 0.60) * | 0.51 (0.45, 0.58) * | 0.58 (0.50, 0.67) * | <0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiao, Y.; Li, W.; Wang, L.; Jiang, H.; Wang, S.; Jia, X.; Wang, Z.; Wang, H.; Zhang, B.; Ding, G. Relationship between Dietary Magnesium Intake and Metabolic Syndrome. Nutrients 2022, 14, 2013. https://doi.org/10.3390/nu14102013
Jiao Y, Li W, Wang L, Jiang H, Wang S, Jia X, Wang Z, Wang H, Zhang B, Ding G. Relationship between Dietary Magnesium Intake and Metabolic Syndrome. Nutrients. 2022; 14(10):2013. https://doi.org/10.3390/nu14102013
Chicago/Turabian StyleJiao, Yingying, Weiyi Li, Liusen Wang, Hongru Jiang, Shaoshunzi Wang, Xiaofang Jia, Zhihong Wang, Huijun Wang, Bing Zhang, and Gangqiang Ding. 2022. "Relationship between Dietary Magnesium Intake and Metabolic Syndrome" Nutrients 14, no. 10: 2013. https://doi.org/10.3390/nu14102013
APA StyleJiao, Y., Li, W., Wang, L., Jiang, H., Wang, S., Jia, X., Wang, Z., Wang, H., Zhang, B., & Ding, G. (2022). Relationship between Dietary Magnesium Intake and Metabolic Syndrome. Nutrients, 14(10), 2013. https://doi.org/10.3390/nu14102013