
Alternative Fish Species for Nutritional Management of Children with Fish-FPIES—A Clinical Approach

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Fish in the Human Diet
2.1. Classification of Fish
2.2. Fish Allergy and Fish Allergens
2.3. Parvalbumins
3. Food Protein-Induced Enterocolitis Syndrome (FPIES) Caused by Fish
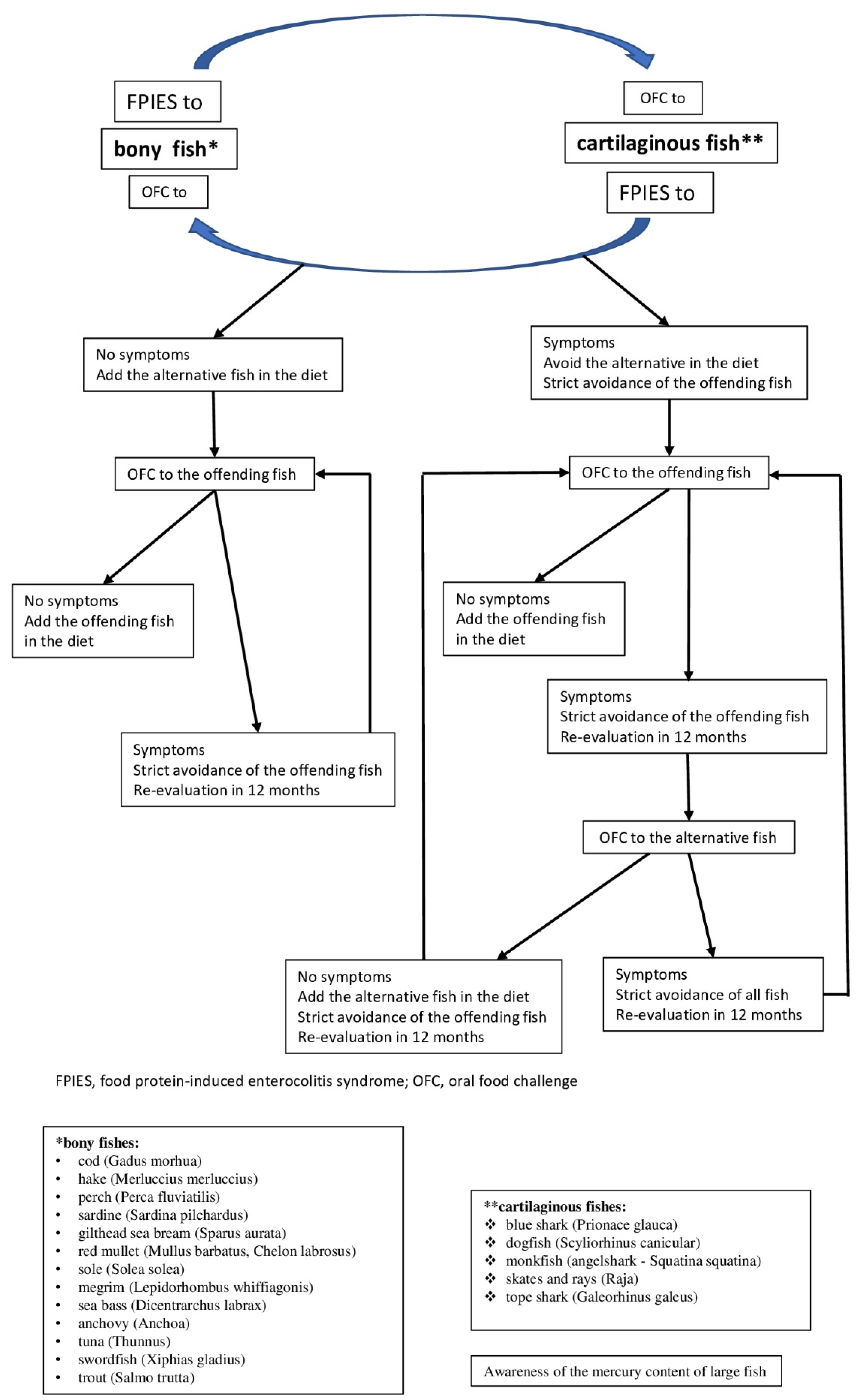
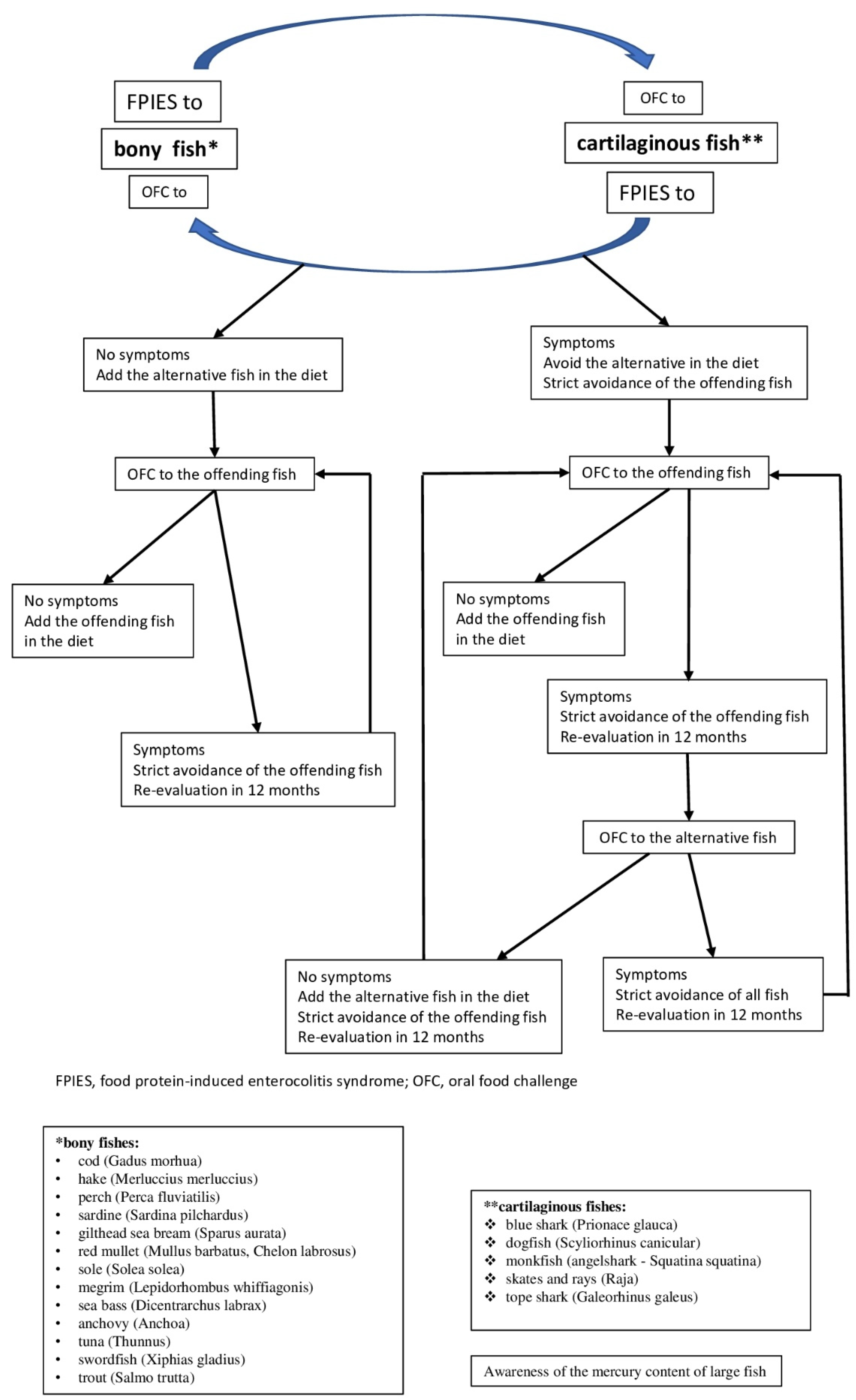
4. The Clinical Approach to Investigation of Tolerance across Fish Species
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Zapatero Remón, L.; Alonso Lebrero, E.; Martin Fernández, E.; Martinez Molero, M. Food protein-induced Enterocolitis Syndrome Caused by Fish. Allergol. Immunopathol. 2005, 33, 312–316. [Google Scholar] [CrossRef]
- Sopo, S.M.; Giorgio, V.; Dello Iacono, I.; Novembre, E.; Mori, F.; Onesimo, R. A multicentre retrospective study of 66 Italian children with food protein-induced enterocolitis syndrome: Different management for different phenotypes. Clin. Exp. Allergy 2012, 42, 1257–1265. [Google Scholar] [CrossRef]
- Miceli Sopo, S.; Monaco, S.; Badina, L.; Barni, S.; Longo, G.; Novembre, E.; Viola, S.; Monti, G. Food protein-induced enterocolitis syndrome caused by fish and/or shellfish in Italy. Pediatr. Allergy Immunol. 2015, 26, 731–736. [Google Scholar] [CrossRef] [PubMed]
- Vila, L.; García, V.; Rial, M.J.; Novoa, E.; Cacharron, T. Fish is a major trigger of solid food protein–induced enterocolitis syndrome in Spanish children. J. Allergy Clin. Immunol. Pract. 2015, 3, 621–623. Available online: https://www.ncbi.nlm.nih.gov/pubmed/25869583 (accessed on 1 November 2021). [CrossRef]
- Vazquez-Ortiz, M.; Machinena, A.; Dominguez, O.; Alvaro, M.; Calvo-Campoverde, K.; Giner, M.T.; Jiménez-Feijoo, R.; Lozano, J.; Piquer, M.; Dias, M.; et al. Food protein–induced enterocolitis syndrome to fish and egg usually resolves by age 5 years in Spanish children. J. Allergy Clin. Immunol. Pract. 2017, 5, 512–515.e1. Available online: https://www.ncbi.nlm.nih.gov/pubmed/28283165 (accessed on 1 November 2021). [CrossRef] [PubMed]
- Gonzalez-Delgado, P.G.; Caparrós, E.; Moreno, M.V.; Clemente, F.; Flores, E.; Velásquez, L.; Rubio, G.; Fernández, J. Clinical and immunological characteristics of a pediatric population with food protein-induced enterocolitis syndrome (FPIES) to fish. Pediatr. Allergy Immunol. 2016, 27, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Alonso, S.B.; Ezquiaga, J.G.; Berzal, P.T.; Tardón, S.D.; José, M.M.S.; López, P.A.; Bermejo, T.B.; Teruel, S.Q.; Zudaire, L.Á.E. Food protein–induced enterocolitis syndrome: Increased prevalence of this great unknown—Results of the PREVALE study. J. Allergy Clin. Immunol. 2018, 143, 430–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Douros, K.; Tsabouri, S.; Feketea, G.; Grammeniatis, V.; Koliofoti, E.G.; Papadopoulos, M.; Sardeli, O.; Triga, M.; Priftis, K.N. Retrospective study identified fish and milk as the main culprits in cases of food protein-induced enterocolitis syndrome. Acta Paediatr. 2019, 108, 1901–1904. Available online: https://www.ncbi.nlm.nih.gov/pubmed/30883926 (accessed on 1 November 2021). [CrossRef] [PubMed]
- Xepapadaki, P.; Kitsioulis, N.A.; Manousakis, E.; Manolaraki, I.; Douladiris, N.; Papadopoulos, N.G. Remission Patterns of Food Protein-Induced Enterocolitis Syndrome in a Greek Pediatric Population. Int. Arch. Allergy Immunol. 2019, 180, 113–119. [Google Scholar] [CrossRef]
- Papadopoulou, A.; Lagousi, T.; Hatzopoulou, E.; Korovessi, P.; Kostaridou, S.; Mermiri, D.-Z. Atypical Food protein-induced enterocolitis syndrome in children: Is IgE sensitization an issue longitudinally? Allergol. Immunopathol. 2021, 49, 73–82. [Google Scholar] [CrossRef]
- Argiz, L.; Infante, S.; Machinena, A.; Bracamonte, T.; Echeverria, L.; Prieto, A.; Garriga, T.; Vila, L.; Gonzalez-Delgado, P.; Garcia-Magan, C.; et al. Children with acute food protein-induced enterocolitis syndrome from Spain and Italy usually tolerate all other food groups. Clin. Exp. Allergy 2021, 51, 1238–1241. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.; Nowak-Węgrzyn, A.; Vadas, P. FPIES in adults. Ann. Allergy Asthma Immunol. 2018, 121, 736–738. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Delgado, P.; Caparrós, E.; Moreno, M.V.; Cueva, B.; Fernández, J. Food protein–induced enterocolitis-like syndrome in a population of adolescents and adults caused by seafood. J. Allergy Clin. Immunol. Pract. 2018, 7, 670–672. [Google Scholar] [CrossRef]
- Du, Y.J.; Gonzalez-Delgado, P.; Vadas, P. Food protein–induced enterocolitis syndrome: Not just in children. Ann. Allergy Asthma Immunol. 2021, 127, 291–292. [Google Scholar] [CrossRef] [PubMed]
- Crespo, J.; Skrabski, F.; Pérez-Pallise, M.E.; De Castro-Martínez, F.J.; Zubeldia, J.M.; Infante, S. Relevant features of adult-onset food protein–induced enterocolitis syndrome. J. Allergy Clin. Immunol. Pract. 2020, 9, 1759–1760. [Google Scholar] [CrossRef] [PubMed]
- Infante, S.; Marco, G.; Sánchez-Domínguez, M.; Rodríguez-Fernández, A.; Fuentes-Aparicio, V.; Alvarez-Perea, A.; Cabrera-Freitag, P.; Morales-Cabeza, C.; Zubeldia, J.M.; Zapatero, L. Food protein-induced enterocolitis syndrome by fish: Not necessarily a restricted diet. Allergy 2017, 73, 728–732. Available online: https://www.ncbi.nlm.nih.gov/pubmed/29052246 (accessed on 1 November 2021). [CrossRef] [PubMed]
- Institute of Medicine. Seafood Choices: Balancing Benefits and Risks; The National Academies Press: Washington, DC, USA, 2007. [Google Scholar]
- European Commission. The EU Fish Market 2019 Edition Is Out: Everything You Wanted to Know about the EU Market for Fish and Seafood. EUMOFA’s Annual Report “The EU Fish Market”. Available online: https://ec.europa.eu/newsroom/mare/items/664022.2021 (accessed on 1 November 2021).
- Sharp, M.F.; Lopata, A.L. Fish Allergy: In Review. Clin. Rev. Allergy Immunol. 2013, 46, 258–271. Available online: https://www.ncbi.nlm.nih.gov/pubmed/23440653 (accessed on 1 November 2021). [CrossRef]
- Stephen, J.N.; Sharp, M.F.; Ruethers, T.; Taki, A.; Campbell, D.E.; Lopata, A.L. Allergenicity of bony and cartilaginous fish—Molecular and immunological properties. Clin. Exp. Allergy 2017, 47, 300–312. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Sustainable Fisheries/Seafood Markets/Commercial Designations. Available online: https://fish-commercial-names.ec.europa.eu/fish-names/species_en?sn=15306 (accessed on 1 November 2021).
- Food and Agriculture Organization of the United Nations. The State of World Fisheries and Aquaculture 2020. Available online: https://www.fao.org/state-of-fisheries-aquaculture (accessed on 1 November 2021).
- Matricardi, P.M.; Kleine-Tebbe, J.; Hoffmann, H.J.; Valenta, R.; Hilger, C.; Hofmaier, S.; Aalberse, R.C.; Agache, I.; Asero, R.; Ballmer-Weber, B.; et al. EAACI Molecular Allergology User’s Guide. Pediatr. Allergy Immunol. 2016, 27 (Suppl. 2), 1–250. Available online: https://onlinelibrary.wiley.com/doi/abs/10.1111/pai.12563 (accessed on 1 November 2021). [CrossRef] [PubMed]
- Kyne, M.P.; Jabado, R.W. Most rhino rays (sawfishes, wedgefishes, giant guitarfishes, guitarfishes, banjo rays) are threatened with extinction. In Reference Module in Earth Systems and Environmental Sciences; Elsevier: Amsterdam, The Netherlands, 2021. [Google Scholar]
- Berkovitz, B.; Shellis, P. Chapter 4—Bony fishes. In The Teeth of Non-Mammalian Vertebrates; Academic Press: London, UK, 2017. [Google Scholar] [CrossRef]
- Helfman, G.S. Biodiversity of Fish. In Encyclopedia of Biodiversity; Levin, S.A., Ed.; Elsevier: New York, NY, USA, 2001; pp. 755–782. [Google Scholar]
- Kobayashi, A.; Tanaka, H.; Hamada, Y.; Ishizaki, S.; Nagashima, Y.; Shiomi, K. Comparison of allergenicity and allergens between fish white and dark muscles. Allergy 2006, 61, 357–363. [Google Scholar] [CrossRef]
- Froese, R.; Pauly, D. Fishbase. World Wide Web Electronic Publication. Available online: www.Fishbase.org (accessed on 1 November 2021).
- U.S. Food & Drug Administration. Advice about Eating Fish for Those Who Might Become or Are Pregnant or Breastfeeding and Children Ages 1–11 Years. 2021. Available online: https://www.fda.gov/food/consumers/advice-about-eating-fish (accessed on 12 November 2021).
- Food Safety Authority of Ireland. Mercury and Fish Consumption. 2017. Available online: https://www.fsai.ie/faq/mercury_and_fish_consumption.html (accessed on 15 November 2021).
- European Food Safety Authority (EFSA) Panel on Contaminants in the Food Chain (CONTAM). Scientific Opinion on the risk for public health related to the presence of mercury and methylmercury in food. EFSA J. 2012, 10, 2985. [Google Scholar] [CrossRef]
- European Food Safety Authority. Mercury in Food—EFSA Updates Advice on Risks for Public Health. 2014. Available online: https://www.efsa.europa.eu/en/press/news/121220 (accessed on 15 November 2021).
- Maurice, L.; Le Croizier, G.; Morales, G.; Carpintero, N.; Guayasamin, J.M.; Sonke, J.; Páez-Rosas, D.; Point, D.; Bustos, W.; Ochoa-Herrera, V. Concentrations and stable isotopes of mercury in sharks of the Galapagos Marine Reserve: Human health concerns and feeding patterns. Ecotoxicol. Environ. Saf. 2021, 215, 112122. [Google Scholar] [CrossRef] [PubMed]
- Taylor, D.L.; Kutil, N.J.; Malek, A.J.; Collie, J.S. Mercury bioaccumulation in cartilaginous fishes from Southern New England coastal waters: Contamination from a trophic ecology and human health perspective. Mar. Environ. Res. 2014, 99, 20–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sicherer, S.H.; Sampson, H.A. Food allergy: Epidemiology, pathogenesis, diagnosis, and treatment. J. Allergy Clin. Immunol. 2014, 133, 291–307.e5. [Google Scholar] [CrossRef]
- Boyce, J.A.; Assa’Ad, A.; Burks, A.W.; Jones, S.M.; Sampson, H.A.; Wood, R.A.; Plaut, M.; Cooper, S.F.; Fenton, M.J.; Arshad, S.H.; et al. Guidelines for the Diagnosis and Management of Food Allergy in the United States: Summary of the NIAID-Sponsored Expert Panel Report. J. Allergy Clin. Immunol. 2010, 126, 1105–1118. [Google Scholar] [CrossRef]
- Tsabouri, S.; Triga, M.; Makris, M.; Kalogeromitros, D.; Church, M.K.; Priftis, K.N. Fish and shellfish allergy in children: Review of a persistent food allergy. Pediatr. Allergy Immunol. 2012, 23, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Ekuehn, A.; Eswoboda, I.; Earumugam, K.; Hilger, C.; Hentges, F. Fish Allergens at a Glance: Variable Allergenicity of Parvalbumins, the Major Fish Allergens. Front. Immunol. 2014, 5, 179. [Google Scholar] [CrossRef] [Green Version]
- Kuehn, A.; Hilger, C.; Lehners-Weber, C.; Codreanu-Morel, F.; Morisset, M.; Metz-Favre, C.; Pauli, G.; De Blay, F.; Revets, D.; Muller, C.P.; et al. Identification of enolases and aldolases as important fish allergens in cod, salmon and tuna: Component resolved diagnosis using parvalbumin and the new allergens. Clin. Exp. Allergy 2013, 43, 811–822. [Google Scholar] [CrossRef] [PubMed]
- Goodman, M.; Pechére, J.-F.; Haiech, J.; Demaille, J.G. Evolutionary diversification of structure and function in the family of intracellular calcium-binding proteins. J. Mol. Evol. 1979, 13, 331–352. [Google Scholar] [CrossRef] [PubMed]
- Murua, H. The Biology and Fisheries of European Hake, Merluccius merluccius, in the North-East Atlantic. Adv. Marine Biol. 2010, 58, 97–154. [Google Scholar] [CrossRef]
- Kuehn, A.; Scheuermann, T.; Hilger, C.; Hentges, F. Important Variations in Parvalbumin Content in Common Fish Species: A Factor Possibly Contributing to Variable Allergenicity. Int. Arch. Allergy Immunol. 2010, 153, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Griesmeier, U.; Vãzquez-Cortãs, S.; Bublin, M.; Radauer, C.; Ma, Y.; Briza, P.; Fernãndez-Rivas, M.; Breiteneder, H. Expression levels of parvalbumins determine allergenicity of fish species. Allergy 2010, 65, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, A.; Kobayashi, Y.; Shiomi, K. Fish allergy in patients with parvalbumin-specific immunoglobulin E depends on parvalbumin content rather than molecular differences in the protein among fish species. Biosci. Biotechnol. Biochem. 2016, 80, 2018–2021. [Google Scholar] [CrossRef] [Green Version]
- Lee, P.-W.; Nordlee, J.A.; Koppelman, S.J.; Baumert, J.L.; Taylor, S.L. Measuring parvalbumin levels in fish muscle tissue: Relevance of muscle locations and storage conditions. Food Chem. 2012, 135, 502–507. [Google Scholar] [CrossRef]
- Saptarshi, S.R.; Sharp, M.F.; Kamath, S.; Lopata, A.L. Antibody reactivity to the major fish allergen parvalbumin is determined by isoforms and impact of thermal processing. Food Chem. 2014, 148, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Koyama, H.; Kakami, M.; Kawamura, M.; Tokuda, R.; Kondo, Y.; Tsuge, I.; Yamada, K.; Yasuda, T.; Urisu, A. Grades of 43 Fish Species in Japan Based on IgE-binding Activity. Allergol. Int. 2006, 55, 311–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, Y.; Kuriyama, T.; Nakagawara, R.; Aihara, M.; Hamada-Sato, N. Allergy to fish collagen: Thermostability of collagen and IgE reactivity of patients’ sera with extracts of 11 species of bony and cartilaginous fish. Allergol. Int. 2016, 65, 450–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, D.L.-C.; Neo, K.H.; Goh, D.L.-M.; Shek, L.P.-C.; Lee, B.W. Missing parvalbumin: Implications in diagnostic testing for tuna allergy. J. Allergy Clin. Immunol. 2005, 115, 874–875. [Google Scholar] [CrossRef] [PubMed]
- Pecoraro, L.; Infante, S.; Fuentes-Aparicio, V.; Cabrera-Freitag, P.; Antonucci, N.; Alvarez-Perea, A. IgE-mediated fish allergy in pediatric age: Does canned tuna have a chance for tolerance? Pediatr. Allergy Immunol. 2021, 32, 1114–1117. [Google Scholar] [CrossRef]
- Jiang, X.; Rao, Q. Effect of Processing on Fish Protein Antigenicity and Allergenicity. Foods 2021, 10, 969. [Google Scholar] [CrossRef] [PubMed]
- Mehr, S.; Frith, K.; Barnes, E.H.; Campbell, D.E.; Allen, K.; Gold, M.; Joshi, P.; Kakakios, A.; Loh, R.; Peake, J.; et al. Food protein–induced enterocolitis syndrome in Australia: A population-based study, 2012–2014. J. Allergy Clin. Immunol. 2017, 140, 1323–1330. [Google Scholar] [CrossRef] [Green Version]
- Tan, J.A.; Smith, W. Non–IgE-mediated gastrointestinal food hypersensitivity syndrome in adults. J. Allergy Clin. Immunol. Pract. 2014, 2, 355–357.e1. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, B.N.; Boyle, R.J.; Gore, C.; Simpson, A.; Custovic, A. Food protein–induced enterocolitis syndrome can occur in adults. J. Allergy Clin. Immunol. 2012, 130, 1199–1200. [Google Scholar] [CrossRef] [PubMed]
- Leonard, S.A.; Pecora, V.; Fiocchi, A.; Nowak-Wegrzyn, A. Food protein-induced enterocolitis syndrome: A review of the new guidelines. World Allergy Organ. J. 2018, 11, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leonard, S.A.; Nowak-Wegrzyn, A. Food protein–induced enterocolitis syndrome: An update on natural history and review of management. Ann. Allergy Asthma Immunol. 2011, 107, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Baker, M.G.; Nowak-Wegrzyn, A. Food protein-induced enterocolitis syndrome: Epidemiology and comorbidities. Curr. Opin. Allergy Clin. Immunol. 2020, 20, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Maciag, M.C.; Bartnikas, L.M.; Sicherer, S.H.; Herbert, L.J.; Young, M.C.; Matney, F.; Westcott-Chavez, A.A.; Petty, C.R.; Phipatanakul, W.; Bingemann, T.A. A Slice of Food Protein–Induced Enterocolitis Syndrome (FPIES): Insights from 441 Children with FPIES as Provided by Caregivers in the International FPIES Association. J. Allergy Clin. Immunol. Pract. 2020, 8, 1702–1709. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-García, M.; Díez, C.E.; García, S.S.; del Rio, P.R.; Ibáñez, M.D. Diagnosis and natural history of food protein-induced enterocolitis syndrome in children from a tertiary hospital in central Spain. J. Investig. Allergol. Clin. Immunol. 2014, 24, 354–356. [Google Scholar] [PubMed]
- Ocak, M.; Akarsu, A.; Sahiner, U.M.; Soyer, O.; Sekerel, B.E. Phenotypes and natural history of food protein-induced enterocolitis syndrome in the east Mediterranean region. Allergy Asthma Proc. 2020, 41, 420–427. [Google Scholar] [CrossRef]
- Nowak-Węgrzyn, A.; Chehade, M.; Groetch, M.E.; Spergel, J.; Wood, R.A.; Allen, K.; Atkins, D.; Bahna, S.; Barad, A.V.; Berin, C.; et al. International consensus guidelines for the diagnosis and management of food protein–induced enterocolitis syndrome: Executive summary—Workgroup Report of the Adverse Reactions to Foods Committee, American Academy of Allergy, Asthma & Immunology. J. Allergy Clin. Immunol. 2017, 139, 1111–1126.e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Infante, S.; Pérez-Pallisé, E.; Skrabski, F.; Cabrera-Freitag, P.; Morales-Cabeza, C.; Fuentes-Aparicio, V.; Alvarez-Perea, A.; Zubeldia, J.M. Poor prognosis of food protein–induced enterocolitis syndrome to fish. Pediatr. Allergy Immunol. 2020, 32, 560–565. [Google Scholar] [CrossRef]
- Xepapadaki, P.; Christopoulou, G.; Stavroulakis, G.; Freidl, R.; Linhart, B.; Zuidmeer, L.; Lakoumentas, J.; van Ree, R.; Valenta, R.; Papadopoulos, N.G. Natural History of IgE-Mediated Fish Allergy in Children. J. Allergy Clin. Immunol. Pract. 2021, 9, 3147–3156.e5. [Google Scholar] [CrossRef] [PubMed]
- Järvinen, K.M.; Nowak-Węgrzyn, A. Food Protein-Induced Enterocolitis Syndrome (FPIES): Current Management Strategies and Review of the Literature. J. Allergy Clin. Immunol. Pract. 2013, 1, 317–322.e4. [Google Scholar] [CrossRef] [PubMed]
- Bird, J.A.; Barni, S.; Brown-Whitehorn, T.F.; du Toit, G.; Infante, S.; Nowak-Wegrzyn, A. Food protein-induced enterocolitis syndrome oral food challenge. Ann. Allergy Asthma Immunol. 2021, 126, 506–515. [Google Scholar] [CrossRef] [PubMed]
- Nicolaides, R.; Bird, J.A.; Cianferoni, A.; Brown-Whitehorn, T.; Nowak-Wegrzyn, A. Oral Food Challenge for FPIES in Practice—A Survey: Report from the Work Group on FPIES Within the Adverse Reactions to Foods Committee, FAED IS, AAAAI. J. Allergy Clin. Immunol. Pract. 2021, 9, 3608–3614.e1. [Google Scholar] [CrossRef]
- Infante, S.; Marco-Martín, G.; Zubeldia, J.M.; Fuentes-Aparicio, V.; Alvarez-Perea, A.; Cabrera-Freitag, P.; Morales-Cabeza, C.; Zapatero, L. Oral Food Challenge in Food Protein-Induced Enterocolitis Syndrome by Fish: Is There Any Room for Improvement? Int. Arch. Allergy Immunol. 2019, 179, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Calderon-Rodriguez, S.; Pineda, F.; Perez, R.; Muñoz, C. Tolerability to dogfish in children with fish allergy. Allergol. Immunopathol. 2016, 44, 167–169. [Google Scholar] [CrossRef] [PubMed]
- Kalic, T.; Morel-Codreanu, F.; Radauer, C.; Ruethers, T.; Taki, A.; Swoboda, I.; Hilger, C.; Hoffmann-Sommergruber, K.; Ollert, M.; Hafner, C.; et al. Patients Allergic to Fish Tolerate Ray Based on the Low Allergenicity of Its Parvalbumin. J. Allergy Clin. Immunol. Pract. 2018, 7, 500–508.e11. [Google Scholar] [CrossRef] [PubMed]
- Mehr, S.; Kakakios, A.; Frith, K.; Kemp, A.S. Food Protein-Induced Enterocolitis Syndrome: 16-Year Experience. Pediatrics 2009, 123, e459–e464. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.; Campbell, D.E.; Barnes, E.H.; Mehr, S.S. Resolution of acute food protein-induced enterocolitis syndrome in children. J. Allergy Clin. Immunol. Pract. 2017, 5, 486–488.e1. [Google Scholar] [CrossRef] [PubMed]
- Ludman, S.; Harmon, M.; Whiting, D.; du Toit, G. Clinical presentation and referral characteristics of food protein-induced enterocolitis syndrome in the United Kingdom. Ann. Allergy Asthma Immunol. 2014, 113, 290–294. [Google Scholar] [CrossRef] [PubMed]
- Caubet, J.C.; Ford, L.S.; Sickles, L.; Järvinen, K.M.; Sicherer, S.H.; Sampson, H.A.; Nowak-Węgrzyn, A. Clinical features and resolution of food protein–induced enterocolitis syndrome: 10-year experience. J. Allergy Clin. Immunol. 2014, 134, 382–389.e4. [Google Scholar] [CrossRef]
- Ullberg, J.; Fech-Bormann, M.; Fagerberg, U.L. Clinical presentation and management of food protein-induced enterocolitis syndrome in 113 Swedish children. Allergy 2021, 76, 2115–2122. [Google Scholar] [CrossRef] [PubMed]
- Stiefel, G.; Alviani, C.; Afzal, N.A.; Byrne, A.; Toit, G.D.; DunnGalvin, A.; Hourihane, J.; Jay, N.; Michaelis, L.J.; Erlewyn-Lajeunesse, M. Food protein-induced enterocolitis syndrome in the British Isles. Arch. Dis. Child. 2021. [Google Scholar] [CrossRef] [PubMed]
- Díaz, J.J.; Espín, B.; Segarra, O.; Domínguez-Ortega, G.; Blasco-Alonso, J.; Cano, B.; Rayo, A.; Moreno, A. Food Protein-induced Enterocolitis Syndrome: Data from a Multicenter Retrospective Study in Spain. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 232–236. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.; Barnes, E.H.; Mehr, S.; Campbell, D.E. An exploration of factors associated with food protein-induced enterocolitis syndrome: Birth, infant feeding and food triggers. Pediatr. Allergy Immunol. 2021, 32, 742–749. [Google Scholar] [CrossRef] [PubMed]
- Sopo, S.M.; Fantacci, C.; Bersani, G.; Romano, A.; Monaco, S. Loss of tolerance for fishes previously tolerated in children with fish food protein induced enterocolitis syndrome. Allergol. Immunopathol. 2018, 46, 394–396. [Google Scholar] [CrossRef] [PubMed]
- D’Amelio, C.; Gastaminza, G.; Vega, O.; Bernad, A.; Madamba, R.C.; Ferrer, M.; Goikoetxea, M.J.; Martínez-Aranguren, R. Induction of tolerance to different types of fish through desensitization with hake. Pediatr. Allergy Immunol. 2016, 28, 96–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sopo, M.S.; Sinatti, D.; Gelsomino, M. Oral desensitization in egg acute food protein-induced enterocolitis syndrome. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 5766–5768. [Google Scholar] [CrossRef]

{kind=link}
| Fish Species | Number of Cases (%) | Tolerance to Other Species | Country, City | Publication |
|---|---|---|---|---|
| hake, whiting, sole, perch, anchovy, monkfish | 16 | Unspecified | Spain, Alicante | [6] |
| hake | 3 (37.5%) | Unspecified | Spain, Madrid | [7] |
| hake, sole, megrim, cod, canned tuna, sardine, swordfish | 80 | canned tuna and swordfish | Spain, Madrid | [16] |
| cod, perch, sardine, tope, sea bream | 56 (56%) | 5 subjects tolerated a type of fish other than the culprit species | Greece, Athens | [10] |
| cod, tope shark, tuna | 25 (34.7%) | Unspecified | Greece, Athens | [9] |
| unspecified | 42 (53.8%) | Unspecified | Greece, multicenter | [8] |
| unspecified fish, white fish, tuna, salmon | 12 (5%) | Unspecified | Australia (multicenter) | [52] |
| hake (14) monkfish (6), sole and megrim (4) | 17 (80%) | Unspecified | Spain, La Coruna | [4] |
| hake, sole, cork float | 14 | Unspecified | Spain, Madrid | [1] |
| sole, cod, sea bass, gilthead, anchovy | 70 | cod, salmon, swordfish, bass, red mullet, anchovy, canned tuna, gilthead, trout | Italy, multicenter | [3] |
| hake (19), sole (9), monkfish (7), canned tuna (4), salmon (2), swordfish (1), fresh tuna (1), dogfish (1) | 44 (54.3%) | Other fish species were not tested. | Spain, Barcelona | [5] |
| unspecified fish | 5 (3.12%) | US, New York | [73] | |
| cod, sole, sea bream, salmon, trout | 8 (12%) | three were tolerant to different fish types (salmon + swordfish, cod + tuna, sea bream + cod + perch) | Italy multicenter | [2] |
| unspecified | 102 (57%) | 41% reacted to more than one fish species and 78/102 (76%) were avoiding all fish. | Spain, Italy, 12 centers | [11] |
| unspecified | 28 (25%) | Unspecified | Sweden, multicenter | [74] |
| unspecified | 19 (14%) | Unspecified | UK and Ireland | [75] |
| unspecified | 39 (32.5%) | Unspecified | Spain, multicenter | [76] |
| unspecified | 19 (11%) | Unspecified | Australia | [77] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feketea, G.; Vassilopoulou, E.; Geropanta, F.; Berghea, E.C.; Bocsan, I.C. Alternative Fish Species for Nutritional Management of Children with Fish-FPIES—A Clinical Approach. Nutrients 2022, 14, 19. https://doi.org/10.3390/nu14010019
Feketea G, Vassilopoulou E, Geropanta F, Berghea EC, Bocsan IC. Alternative Fish Species for Nutritional Management of Children with Fish-FPIES—A Clinical Approach. Nutrients. 2022; 14(1):19. https://doi.org/10.3390/nu14010019
Chicago/Turabian StyleFeketea, Gavriela, Emilia Vassilopoulou, Foteini Geropanta, Elena Camelia Berghea, and Ioana Corina Bocsan. 2022. "Alternative Fish Species for Nutritional Management of Children with Fish-FPIES—A Clinical Approach" Nutrients 14, no. 1: 19. https://doi.org/10.3390/nu14010019
APA StyleFeketea, G., Vassilopoulou, E., Geropanta, F., Berghea, E. C., & Bocsan, I. C. (2022). Alternative Fish Species for Nutritional Management of Children with Fish-FPIES—A Clinical Approach. Nutrients, 14(1), 19. https://doi.org/10.3390/nu14010019