
Association between Dietary Factors and Constipation in Adults Living in Luxembourg and Taking Part in the ORISCAV-LUX 2 Survey



Abstract
:1. Introduction
2. Materials and Methods
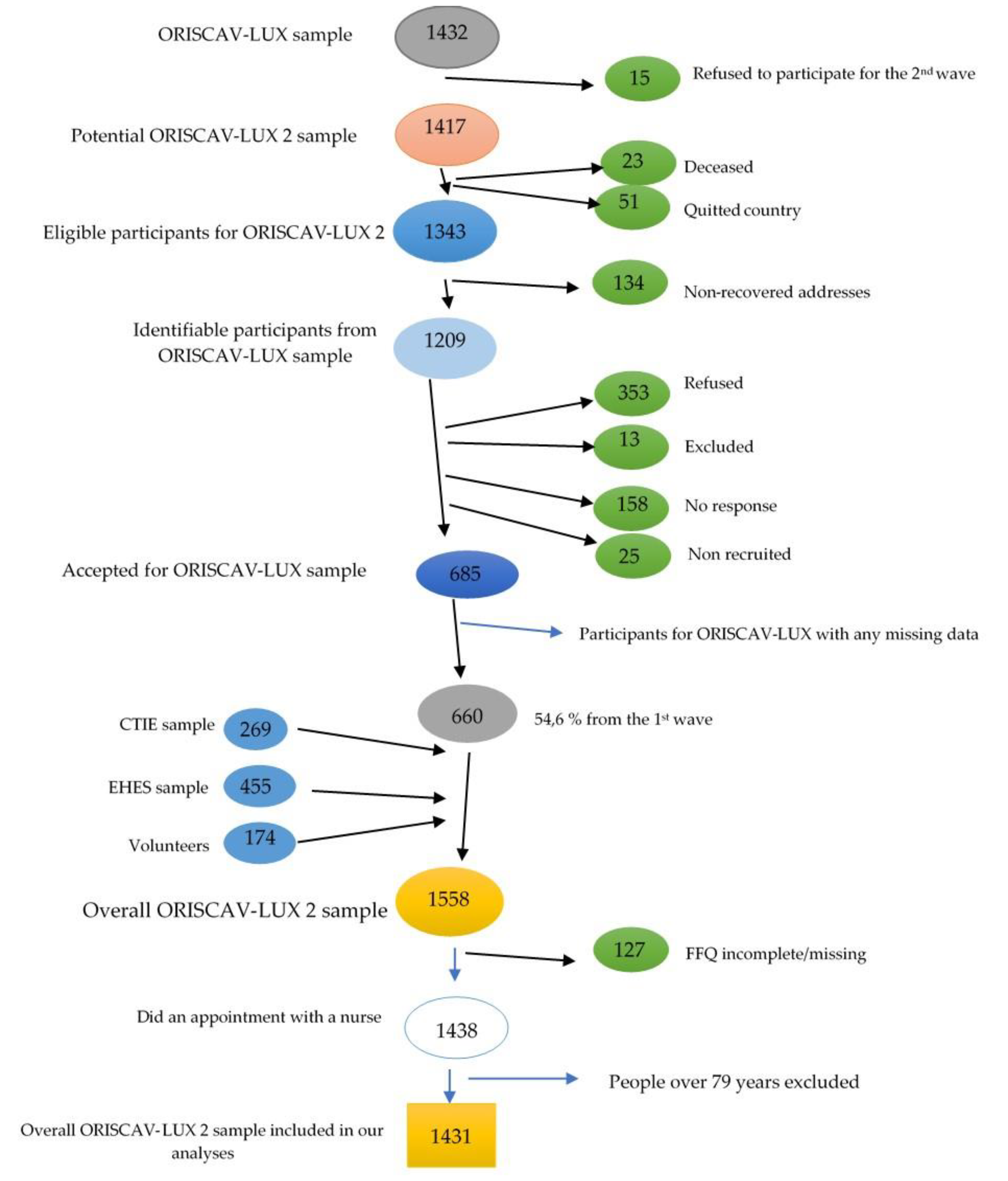
2.1. Study Population and Design
2.2. Data Collection
2.3. Measurement of Constipation Score
2.4. Assessment of Dietary Habits
2.5. Assessment of Physical Activity
2.6. Measurement of Blood/Urine Markers
2.7. Data Management
2.8. Statistical Analyses
2.8.1. General Aspects
2.8.2. Bivariate and Partial Correlations
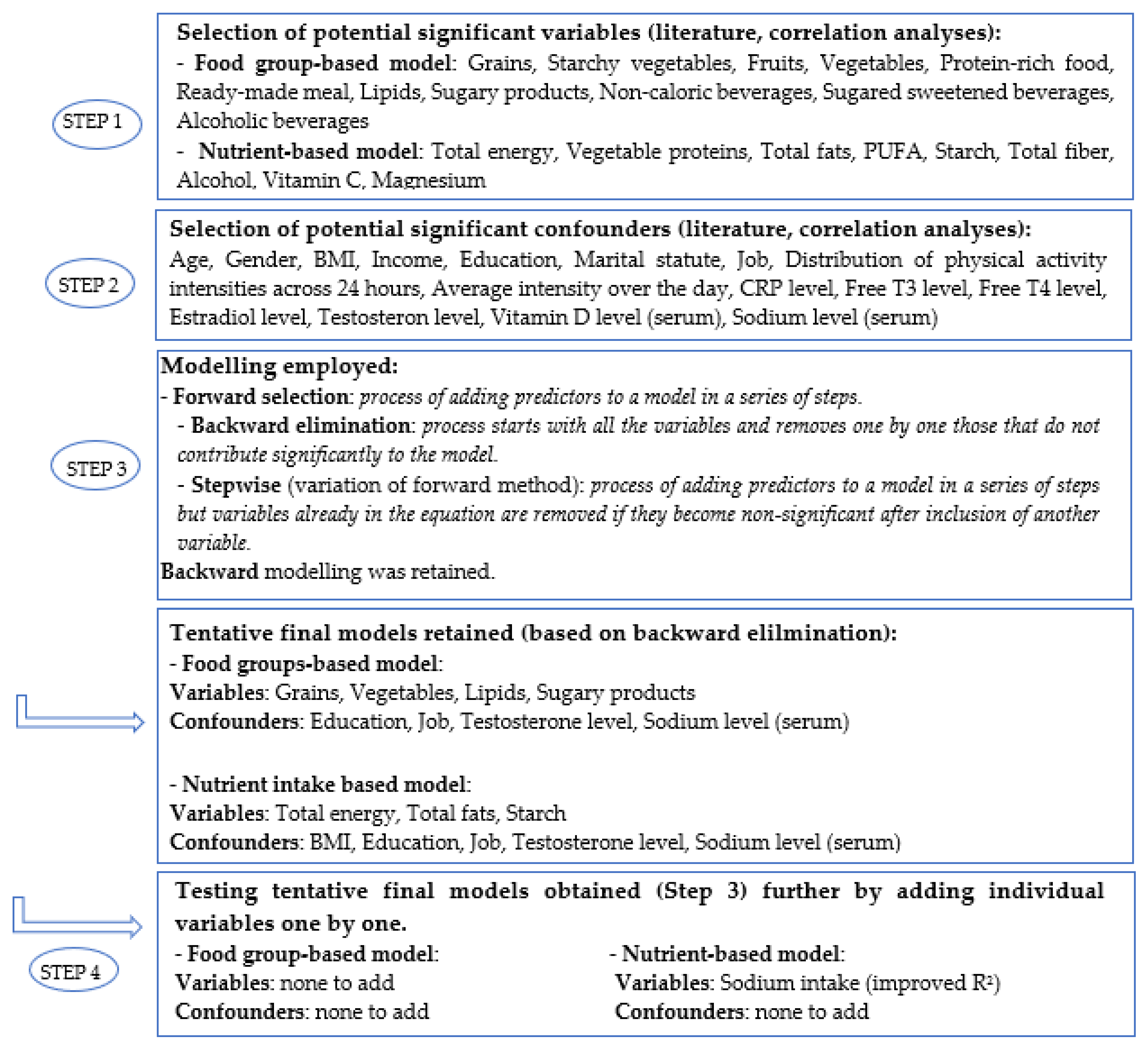
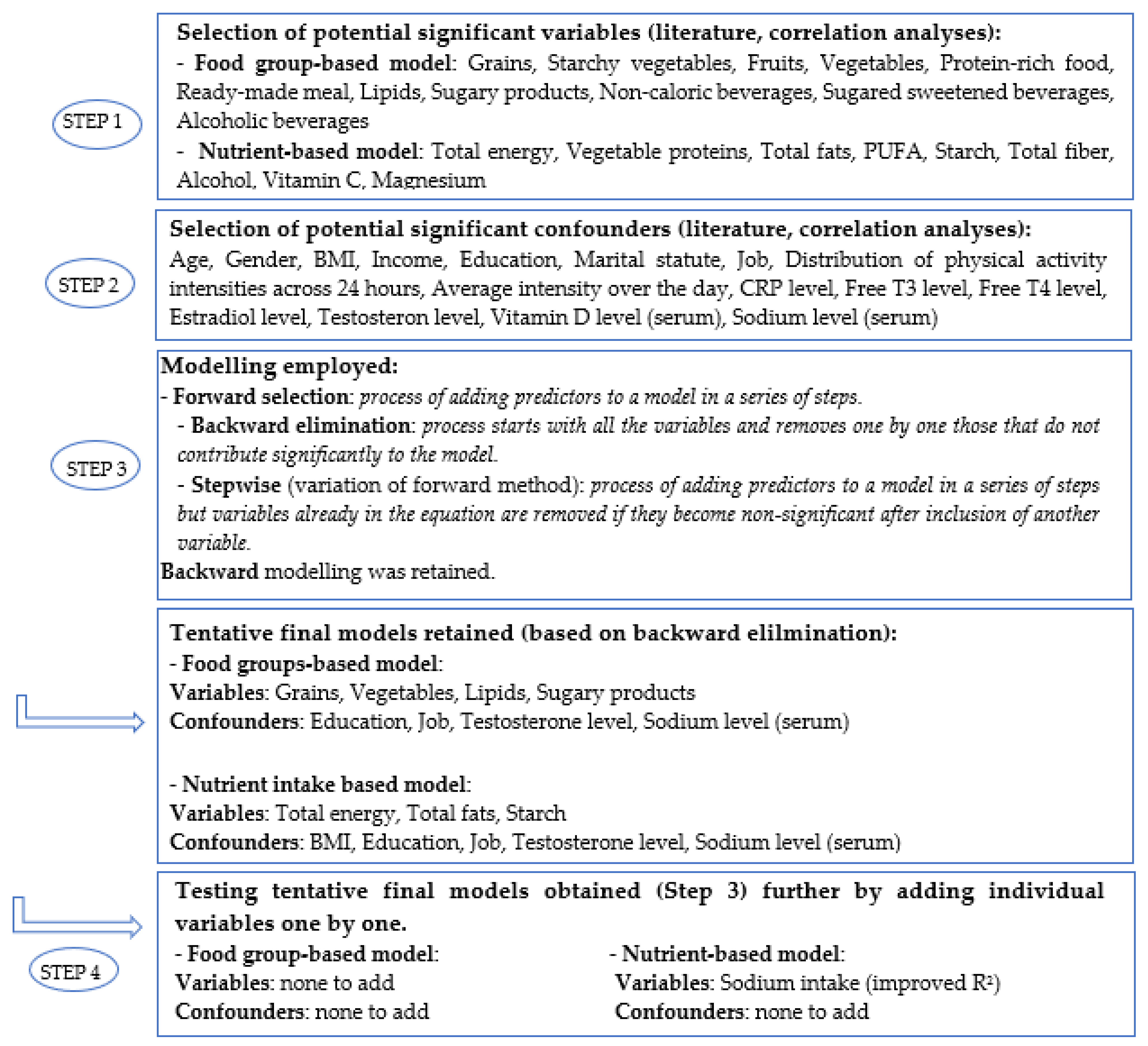
2.8.3. Multivariable Linear and Logistic Regression Modeling
3. Results
3.1. Description of the Study Participants and Dietary Patterns
3.2. Bivariate and Partial Correlation Analyses
3.3. Multivariable Linear and Logistic Regression Modeling
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grabitske, H.A.; Slavin, J.L. Laxation and the Like: Assessing Digestive Health. Nutr. Today 2008, 43, 193–198. [Google Scholar] [CrossRef]
- Rose, C.; Parker, A.; Jefferson, B.; Cartmell, E. The Characterization of Feces and Urine: A Review of the Literature to Inform Advanced Treatment Technology. Crit. Rev. Environ. Sci. Technol. 2015, 45, 1827–1879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitsuhashi, S.; Ballou, S.; Jiang, Z.G.; Hirsch, W.; Nee, J.; Iturrino, J.; Cheng, V.; Lembo, A. Characterizing Normal Bowel Frequency and Consistency in a Representative Sample of Adults in the United States (NHANES). Am. J. Gastroenterol. 2018, 113, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Sperber, A.D.; Bangdiwala, S.I.; Drossman, D.A.; Ghoshal, U.C.; Simren, M.; Tack, J.; Whitehead, W.E.; Dumitrascu, D.L.; Fang, X.; Fukudo, S.; et al. Worldwide Prevalence and Burden of Functional Gastrointestinal Disorders, Results of Rome Foundation Global Study. Gastroenterology 2021, 160, 99–114.e3. [Google Scholar] [CrossRef]
- Perler, B.K.; Ungaro, R.; Baird, G.; Mallette, M.; Bright, R.; Shah, S.; Shapiro, J.; Sands, B.E. Presenting symptoms in inflammatory bowel disease: Descriptive analysis of a community-based inception cohort. BMC Gastroenterol. 2019, 19, 47. [Google Scholar] [CrossRef] [Green Version]
- Schmulson, M.J.; Drossman, D.A. What Is New in Rome IV. J. Neurogastroenterol. Motil. 2017, 23, 151–163. [Google Scholar] [CrossRef]
- Sanjoaquin, M.A.; Appleby, P.N.; Spencer, E.A.; Key, T.J. Nutrition and lifestyle in relation to bowel movement frequency: A cross-sectional study of 20630 men and women in EPIC-Oxford. Public Health Nutr. 2004, 7, 77–83. [Google Scholar] [CrossRef]
- Heaton, K.W.; Radvan, J.; Cripps, H.; Mountford, R.A.; Braddon, F.E.; Hughes, A.O. Defecation frequency and timing, and stool form in the general population: A prospective study. Gut 1992, 33, 818–824. [Google Scholar] [CrossRef] [Green Version]
- Soenen, S.; Rayner, C.K.; Jones, K.L.; Horowitz, M. The ageing gastrointestinal tract. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 12–18. [Google Scholar] [CrossRef]
- Sileri, P.; Franceschilli, L.; De Lorenzo, A.; Mezzani, B.; Todisco, P.; Giorgi, F.; Gaspari, A.L.; Jacoangeli, F. Defecatory disorders in anorexia nervosa: A clinical study. Tech. Coloproctol. 2014, 18, 439–444. [Google Scholar] [CrossRef]
- Emerenziani, S.; Guarino, M.P.L.; Trillo Asensio, L.M.; Altomare, A.; Ribolsi, M.; Balestrieri, P.; Cicala, M. Role of Overweight and Obesity in Gastrointestinal Disease. Nutrients 2019, 12, 111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballou, S.; Katon, J.; Singh, P.; Rangan, V.; Lee, H.N.; McMahon, C.; Iturrino, J.; Lembo, A.; Nee, J. Chronic Diarrhea and Constipation Are More Common in Depressed Individuals. Clin. Gastroenterol. Hepatol. 2019, 17, 2696–2703. [Google Scholar] [CrossRef] [PubMed]
- Vandeputte, D.; Falony, G.; Vieira-Silva, S.; Tito, R.Y.; Joossens, M.; Raes, J. Stool consistency is strongly associated with gut microbiota richness and composition, enterotypes and bacterial growth rates. Gut 2016, 65, 57–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamps, L.W. Infectious Disorders of the GI Tract. In Surgical Pathology of the GI Tract, Liver, Biliary Tract, and Pancreas; Elsevier: Amsterdam, The Netherlands, 2009; pp. 51–79. [Google Scholar] [CrossRef]
- de Oliveira, E.P.; Burini, R.C. The impact of physical exercise on the gastrointestinal tract. Curr. Opin. Clin. Nutr. Metab. Care 2009, 12, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Orr, W.C.; Fass, R.; Sundaram, S.S.; Scheimann, A.O. The effect of sleep on gastrointestinal functioning in common digestive diseases. Lancet Gastroenterol. Hepatol. 2020, 5, 616–624. [Google Scholar] [CrossRef]
- Schneeman, B. Food factors and gastrointestinal function: A critical interface. Biofactors 2004, 21, 85–88. [Google Scholar] [CrossRef]
- Rao, S.S.; Kavelock, R.; Beaty, J.; Ackerson, K.; Stumbo, P. Effects of fat and carbohydrate meals on colonic motor response. Gut 2000, 46, 205–211. [Google Scholar] [CrossRef]
- Calbet, J.A.; MacLean, D.A. Role of caloric content on gastric emptying in humans. J. Physiol. 1997, 498 Pt 2, 553–559. [Google Scholar] [CrossRef]
- Von Schönfeld, J.; Evans, D.F.; Renzing, K.; Castillo, F.D.; Wingate, D.L. Human small bowel motor activity in response to liquid meals of different caloric value and different chemical composition. Dig. Dis. Sci. 1998, 43, 265–269. [Google Scholar] [CrossRef]
- Towers, A.L.; Burgio, K.L.; Locher, J.L.; Merkel, I.S.; Safaeian, M.; Wald, A. Constipation in the elderly: Influence of dietary, psychological, and physiological factors. J. Am. Geriatr. Soc. 1994, 42, 701–706. [Google Scholar] [CrossRef]
- Delgado-Aros, S.; Locke, G.R., 3rd; Camilleri, M.; Talley, N.J.; Fett, S.; Zinsmeister, A.R.; Melton, L.J., 3rd. Obesity is associated with increased risk of gastrointestinal symptoms: A population-based study. Am. J. Gastroenterol. 2004, 99, 1801–1806. [Google Scholar] [CrossRef]
- Guelinckx, I.; Tavoularis, G.; König, J.; Morin, C.; Gharbi, H.; Gandy, J. Contribution of Water from Food and Fluids to Total Water Intake: Analysis of a French and UK Population Surveys. Nutrients 2016, 8, 630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nneli, R.O.; Nwafia, W.C.; Orji, J.O. Diets/dietary habits and certain gastrointestinal disorders in the tropics: A review. Niger. J. Physiol. Sci. 2007, 22, 1–2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rakhra, V.; Galappaththy, S.L.; Bulchandani, S.; Cabandugama, P.K. Obesity and the Western Diet: How We Got Here. Mo. Med. 2020, 117, 536–538. [Google Scholar]
- Vermorken, A.J.; Andres, E.; Cui, Y. Bowel movement frequency, oxidative stress and disease prevention. Mol. Clin. Oncol. 2016, 5, 339–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mudgil, D.; Barak, S. Composition, properties and health benefits of indigestible carbohydrate polymers as dietary fiber: A review. Int. J. Biol. Macromol. 2013, 61, 1–6. [Google Scholar] [CrossRef]
- Goyal, O.; Nohria, S.; Dhaliwal, A.S.; Goyal, P.; Soni, R.K.; Chhina, R.S.; Sood, A. Prevalence, overlap, and risk factors for Rome IV functional gastrointestinal disorders among college students in northern India. Indian J. Gastroenterol. 2021, 40, 144–153. [Google Scholar] [CrossRef] [PubMed]
- Tuck, C.J.; Vanner, S.J. Dietary therapies for functional bowel symptoms: Recent advances, challenges, and future directions. Neurogastroenterol. Motil. 2018, 30, e13238. [Google Scholar] [CrossRef]
- Alkerwi, A.; Pastore, J.; Sauvageot, N.; Coroller, G.L.; Bocquet, V.; d’Incau, M.; Aguayo, G.; Appenzeller, B.; Bejko, D.; Bohn, T.; et al. Challenges and benefits of integrating diverse sampling strategies in the observation of cardiovascular risk factors (ORISCAV-LUX 2) study. BMC Med. Res. Methodol. 2019, 19, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Luxembourg Institute of Health. ORISCAV-LUX 2. Available online: https://oriscav.lih.lu/Oriscav-Lux/ORISCAV-LUX-2 (accessed on 27 September 2021).
- Alkerwi, A.; Sauvageot, N.; Donneau, A.F.; Lair, M.L.; Couffignal, S.; Beissel, J.; Delagardelle, C.; Wagener, Y.; Albert, A.; Guillaume, M. First nationwide survey on cardiovascular risk factors in Grand-Duchy of Luxembourg (ORISCAV-LUX). BMC Public Health 2010, 10, 468. [Google Scholar] [CrossRef] [Green Version]
- Sauvageot, N.; Guillaume, M.; Albert, A. Validation of the food frequency questionnaire used to assess the association between dietary habits and cardiovascular risk factors in the NESCAV study. J. Food Sci. 2013, 3. [Google Scholar] [CrossRef] [Green Version]
- Agachan, F.; Chen, T.; Pfeifer, J.; Reissman, P.; Wexner, S.D. A constipation scoring system to simplify evaluation and management of constipated patients. Dis. Colon Rectum 1996, 39, 681–685. [Google Scholar] [CrossRef] [PubMed]
- Sauvageot, N.; Alkerwi, A.; Albert, A.; Guillaume, M. Use of food frequency questionnaire to assess relationships between dietary habits and cardiovascular risk factors in NESCAV study: Validation with biomarkers. Nutr. J. 2013, 12, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- French Agency for Food, Environmental and Occupational Health & Safety. ANSES-CIQUAL French Food Composition Table for Nutritional Intakes Calculation CALNUT. Available online: https://ciqual.anses.fr/ (accessed on 27 September 2021).
- Migueles, J.H.; Cadenas-Sanchez, C.; Ekelund, U.; Delisle Nyström, C.; Mora-Gonzalez, J.; Löf, M.; Labayen, I.; Ruiz, J.R.; Ortega, F.B. Accelerometer Data Collection and Processing Criteria to Assess Physical Activity and Other Outcomes: A Systematic Review and Practical Considerations. Sports Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef]
- Rowlands, A.V.; Dawkins, N.P.; Maylor, B.; Edwardson, C.L.; Fairclough, S.J.; Davies, M.J.; Harrington, D.M.; Khunti, K.; Yates, T. Enhancing the value of accelerometer-assessed physical activity: Meaningful visual comparisons of data-driven translational accelerometer metrics. Sports Med. Open 2019, 5, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Alkerwi, A.; Sauvageot, N.; El Bahi, I.; Delagardelle, C.; Beissel, J.; Noppe, S.; Roderick, P.J.; Mindell, J.S.; Stranges, S. Prevalence and related risk factors of chronic kidney disease among adults in Luxembourg: Evidence from the observation of cardiovascular risk factors (ORISCAV-LUX) study. BMC Nephrol. 2017, 18, 358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, O.B.; Bosci-Pinto, C.; Lopez, A.D.; Murray, J.L.C.; Lozano, R.; Inoue, M. Age Standardization of Rates: A New WHO Standard; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- World Health Organization. Body mass index—BMI. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 5 August 2021).
- Gupta, S.; Hawk, T.; Aggarwal, A.; Drewnowski, A. Characterizing Ultra-Processed Foods by Energy Density, Nutrient Density, and Cost. Front. Nutr. 2019, 6, 70. [Google Scholar] [CrossRef] [Green Version]
- Renny, A.; Snape, W.J., Jr.; Sun, E.A.; London, R.; Cohen, S. Role of cholecystokinin in the gastrocolonic response to a fat meal. Gastroenterology 1983, 85, 17–21. [Google Scholar] [CrossRef]
- Mukai, R. High-fat diet and constipation. Free Rad. Biol. Med. 2018, 120, S134–S135. [Google Scholar] [CrossRef]
- Wibisono, C.; Rowe, N.; Beavis, E.; Kepreotes, H.; Mackie, F.E.; Lawson, J.A.; Cardamone, M. Ten-year single-center experience of the ketogenic diet: Factors influencing efficacy, tolerability, and compliance. J. Pediatr. 2015, 166, 1030–1036.e1031. [Google Scholar] [CrossRef]
- Kang, H.C.; Chung, D.E.; Kim, D.W.; Kim, H.D. Early-and late-onset complications of the ketogenic diet for intractable epilepsy. Epilepsia 2004, 45, 1116–1123. [Google Scholar] [CrossRef]
- Reichardt, F.; Chassaing, B.; Nezami, B.G.; Li, G.; Tabatabavakili, S.; Mwangi, S.; Uppal, K.; Liang, B.; Vijay-Kumar, M.; Jones, D.; et al. Western diet induces colonic nitrergic myenteric neuropathy and dysmotility in mice via saturated fatty acid- and lipopolysaccharide-induced TLR4 signalling. J. Physiol. 2017, 595, 1831–1846. [Google Scholar] [CrossRef] [Green Version]
- Forsyth, J.S.; Varma, S.; Colvin, M. A randomised controlled study of the effect of long chain polyunsaturated fatty acid supplementation on stool hardness during formula feeding. Arch. Dis. Child. 1999, 81, 253–256. [Google Scholar] [CrossRef]
- Michalak, A.; Mosińska, P.; Fichna, J. Polyunsaturated Fatty Acids and Their Derivatives: Therapeutic Value for Inflammatory, Functional Gastrointestinal Disorders, and Colorectal Cancer. Front. Pharmacol. 2016, 7, 459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Górska-Warsewicz, H.; Rejman, K.; Laskowski, W.; Czeczotko, M. Butter, margarine, vegetable oils, and olive oil in the average polish diet. Nutrients 2019, 11, 2935. [Google Scholar] [CrossRef] [Green Version]
- Holesh, J.E.; Aslam, S.; Martin, A. Physiology, Carbohydrates; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Roberfroid, M.; Gibson, G.R.; Hoyles, L.; McCartney, A.L.; Rastall, R.; Rowland, I.; Wolvers, D.; Watzl, B.; Szajewska, H.; Stahl, B.; et al. Prebiotic effects: Metabolic and health benefits. Br. J. Nutr. 2010, 104 (Suppl. S2), S1–S63. [Google Scholar] [CrossRef] [Green Version]
- Quigley, E.M. Probiotics in the management of functional bowel disorders: Promise fulfilled? Gastroenterol. Clin. 2012, 41, 805–819. [Google Scholar] [CrossRef] [PubMed]
- De Vries, J.; Miller, P.E.; Verbeke, K. Effects of cereal fiber on bowel function: A systematic review of intervention trials. World J. Gastroenterol. 2015, 21, 8952–8963. [Google Scholar] [CrossRef] [PubMed]
- Hillemeier, C. An overview of the effects of dietary fiber on gastrointestinal transit. Pediatrics 1995, 96, 997–999. [Google Scholar] [CrossRef]
- Yang, J.; Wang, H.P.; Zhou, L.; Xu, C.F. Effect of dietary fiber on constipation: A meta analysis. World J. Gastroenterol. 2012, 18, 7378–7383. [Google Scholar] [CrossRef]
- Ho, K.S.; Tan, C.Y.; Mohd Daud, M.A.; Seow-Choen, F. Stopping or reducing dietary fiber intake reduces constipation and its associated symptoms. World J. Gastroenterol. 2012, 18, 4593–4596. [Google Scholar] [CrossRef] [PubMed]
- Vanegas, S.M.; Meydani, M.; Barnett, J.B.; Goldin, B.; Kane, A.; Rasmussen, H.; Brown, C.; Vangay, P.; Knights, D.; Jonnalagadda, S.; et al. Substituting whole grains for refined grains in a 6-wk randomized trial has a modest effect on gut microbiota and immune and inflammatory markers of healthy adults. Am. J. Clin. Nutr. 2017, 105, 635–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United States Department of Agriculture. How Much Fiber Is in Whole Grains versus Refined Grains/non Whole Grains? Available online: https://ask.usda.gov/s/article/How-much-fiber-is-in-whole-grains-versus-refined-grains-non-whole-grains (accessed on 27 September 2021).
- Jung, S.J.; Oh, M.R.; Park, S.H.; Chae, S.W. Effects of rice-based and wheat-based diets on bowel movements in young Korean women with functional constipation. Eur. J. Clin. Nutr. 2020, 74, 1565–1575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lunn, J.; Buttriss, J. Carbohydrates and dietary fibre. Nutr. Bull. 2007, 32, 21–64. [Google Scholar] [CrossRef]
- van Munster, I.P.; Tangerman, A.; Nagengast, F.M. Effect of resistant starch on colonic fermentation, bile acid metabolism, and mucosal proliferation. Dig. Dis. Sci. 1994, 39, 834–842. [Google Scholar] [CrossRef]
- Kruis, W.; Forstmaier, G.; Scheurlen, C.; Stellaard, F. Effect of diets low and high in refined sugars on gut transit, bile acid metabolism, and bacterial fermentation. Gut 1991, 32, 367–371. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Huang, A.-P.; Wang, L.-Q.; Yu, X.-L. Empirically derived dietary patterns and constipation among a middle-aged population from China, 2016–2018. Nutr. J. 2019, 18, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Mäkinen, K.K. Gastrointestinal Disturbances Associated with the Consumption of Sugar Alcohols with Special Consideration of Xylitol: Scientific Review and Instructions for Dentists and Other Health-Care Professionals. Int. J. Dent. 2016, 2016, 5967907. [Google Scholar] [CrossRef] [Green Version]
- Ishimoto, T.; Lanaspa, M.A.; Rivard, C.J.; Roncal-Jimenez, C.A.; Orlicky, D.J.; Cicerchi, C.; McMahan, R.H.; Abdelmalek, M.F.; Rosen, H.R.; Jackman, M.R. High-fat and high-sucrose (western) diet induces steatohepatitis that is dependent on fructokinase. Hepatology 2013, 58, 1632–1643. [Google Scholar] [CrossRef] [Green Version]
- Dreher, M.L. Whole Fruits and Fruit Fiber Emerging Health Effects. Nutrients 2018, 10, 1833. [Google Scholar] [CrossRef] [Green Version]
- Bae, S.H. Diets for constipation. Pediatr. Gastroenterol. Hepatol. Nutr. 2014, 17, 203–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fabbri, A.D.T.; Crosby, G.A. A review of the impact of preparation and cooking on the nutritional quality of vegetables and legumes. Int. J. Gastron. Food Sci. 2016, 3, 2–11. [Google Scholar] [CrossRef] [Green Version]
- Agócs, R.; Sugár, D.; Szabó, A.J. Is too much salt harmful? Yes. Pediatr. Nephrol. 2020, 35, 1777–1785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korošec, Ž.; Pravst, I. Assessing the average sodium content of prepacked foods with nutrition declarations: The importance of sales data. Nutrients 2014, 6, 3501–3515. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Huang, Z.; Yu, K.; Ding, R.; Ye, K.; Dai, C.; Xu, X.; Zhou, G.; Li, C. High-Salt Diet Has a Certain Impact on Protein Digestion and Gut Microbiota: A Sequencing and Proteome Combined Study. Front. Microbiol. 2017, 8, 1838. [Google Scholar] [CrossRef] [Green Version]
- Rinninella, E.; Raoul, P.; Cintoni, M.; Franceschi, F.; Miggiano, G.A.D.; Gasbarrini, A.; Mele, M.C. What is the Healthy Gut Microbiota Composition? A Changing Ecosystem across Age, Environment, Diet, and Diseases. Microorganisms 2019, 7, 14. [Google Scholar] [CrossRef] [Green Version]
- Murakami, K.; Sasaki, S.; Okubo, H.; Takahashi, Y.; Hosoi, Y.; Itabashi, M. Association between dietary fiber, water and magnesium intake and functional constipation among young Japanese women. Eur. J. Clin. Nutr. 2007, 61, 616–622. [Google Scholar] [CrossRef] [Green Version]
- Dupont, C.; Campagne, A.; Constant, F. Efficacy and safety of a magnesium sulfate-rich natural mineral water for patients with functional constipation. Clin. Gastroenterol. Hepatol. 2014, 12, 1280–1287. [Google Scholar] [CrossRef] [Green Version]
- Steele, S.R.; Mellgren, A. Constipation and obstructed defecation. Clin. Colon Rectal Surg. 2007, 20, 110–117. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Question | Answer | Score |
|---|---|---|
| Frequency of bowel movements | 1–2 times per 1–2 days | 0 |
| 2 times per week | 1 | |
| once per week | 2 | |
| <once per week | 3 | |
| <once per month | 4 | |
| Difficulty of evacuation (painful) | Never | 0 |
| Rarely | 1 | |
| Sometimes | 2 | |
| Usually | 3 | |
| Always | 4 | |
| Incomplete feeling of evacuation | Never | 0 |
| Rarely | 1 | |
| Sometimes | 2 | |
| Usually | 3 | |
| Always | 4 | |
| Abdominal pain | Never | 0 |
| Rarely | 1 | |
| Sometimes | 2 | |
| Usually | 3 | |
| Always | 4 | |
| Minutes spent in lavatory per attempt | <5 min | 0 |
| 5–10 min | 1 | |
| 10–20 min | 2 | |
| 20–30 min | 3 | |
| >30 min | 4 | |
| Assistance: type of assistance | Without assistance | 0 |
| Simulative laxatives | 1 | |
| Digital assistance or aenema | 2 | |
| Unsuccessful attempts for evacuation/24 h | Never | 0 |
| 1–3 | 1 | |
| 3–6 | 2 | |
| 6–9 | 3 | |
| >9 | 4 | |
| Duration of constipation | 0 | 0 |
| 1–5 years | 1 | |
| 5–10 years | 2 | |
| 10–20 years | 3 | |
| >20 years | 4 | |
| Total sum | 30 | |
| Variables | Median (IQR) or Number (%) | ||||||
|---|---|---|---|---|---|---|---|
| Total (n = 1431) | Women (n = 761) | Men (n = 670) | p-Value ꝉ,Ƌ | CS1 (n = 1078) | CS2 (n = 353) | p-Value ꝉ,Ƌ | |
| Age (year) | 50.77 (17.99) | 51.5 (17.6) | 50.1 (18.4) | 0.397 | 50.8 (18.5) | 50.8 (16.8) | 0.888 |
BMI (kg/m2)
| 655 (45.8%) 499 (34.9%) 288 (18.7%) 9 (0.6%) | 417 (54.8%) 219 (28.7%) 118 (15.5%) 7 (0.9%) | 238 (35.5%) 280 (41.8%) 150 (22.3%) 2 (0.3%) | <0.001 | 495 (45.9%) 371 (34.4%) 206 (19.1%) 6 (0.6%) | 160 (45.3%) 128 (36.3%) 62 (17.6%) 3 (0.8%) | 0.734 |
Education
| 188 (13.1%) 504 (35.3%) 612 (42.7%) 127 (8.9%) | 108 (14.2%) 279 (36.7%) 297 (39.0%) 77 (10.1%) | 80 (11.9%) 225 (33.6%) 315 (47.0%) 50 (7.5%) | 0.015 | 130 (12.1%) 378 (35.1%) 474 (44.0%) 96 (8.9%) | 58 (16.4%) 126 (35.7%) 138 (39.1%) 31 (8.8%) | 0.146 |
Job
| 940 (65.7%) 153 (10.7%) 319 (22.3%) 19 (1.3%) | 476 (62.5%) 126 (16.6%) 149 (19.6%) 10 (1.3%) | 646 (69.3%) 27 (4.0%) 170 (25.4%) 9 (1.3%) | <0.001 | 697 (64.7%) 115 (10.7%) 253 (23.5%) 13 (1.2%) | 243 (68.8%) 38 (10.8%) 66 (18.7%) 6 (1.7%) | 0.271 |
Monthly income (Euro)
| 4 (0.3%) 23 (1.6%) 51 (3.6%) 82 (5.7%) 340 (23.8%) 487 (34.0%) 117 (8.2%) 327 (22.9%) | 1 (0.1%) 15 (2.0%) 32 (4.2%) 57 (7.5%) 171 (22.5%) 236 (31.0%) 48 (6.3%) 201 (26.4%) | 3 (0.4%) 8 (1.2%) 19 (2.8%) 25 (3.7%) 169 (25.2%) 251 (37.5%) 69 (10.3) 126 (18.8%) | <0.001 | 2 (0.2%) 20 (1.9%) 32 (3.2%) 59 (5.5%) 257 (23.8%) 383 (35.5%) 93 (8.6%) 232 (21.5%) | 2 (0.6%) 3 (0.8%) 19 (5.4%) 23 (6.5%) 83 (23.5%) 104 (29.5%) 24 (6.8%) 95 (26.9%) | 0.033 |
Constipation score
| 1186 (82.8%) 158 (11.0%) 81 (5.7%) 6 (0.5%) | 586 (77.0%) 105 (13.8%) 64 (8.4%) 6 (0.8%) | 600 (89.6%) 53 (7.9%) 17 (2.5%) 0 (0%) | <0.001 | |||
Physical activity
| 655.6 (680.5) 54.1 (76.5) 0.7 (2.0) 23.3 (12.4) | 637.1 (659.8) 56.3 (79.6) 0.6 (1.7) 24.2 (11.6) | 682.3 (696.4) 52.6 (73.7) 0.7 (2.1) 22.2 (12.7) | 0.880 0.450 0.022 0.408 | 656.6 (681.2) 54.4 (77.2) 0.7 (2.0) 23.5 (12.5) | 651.4 (670.7) 53.8 (77.3) 0.6 (1.7) 23.1 (12.5) | 0.700 0.637 0.238 0.359 |
| Biological measurements Testosterone serum level | 0.47 (4.90) | 0.27 (0.13) | 5.3 (2.6) | <0.001 | 2.37 (5.18) | 0.34 (4.09) | <0.001 |
| Sodium serum level | 141.0 (2.0) | 141.0 (3.0) | 141.0 (2.0) | <0.001 | 141.0 (3.0) | 141.0 (2.0) | 0.158 |
| Variables | Median (IQR) | ||||||
|---|---|---|---|---|---|---|---|
| Total (n = 1431) | Women (n = 761) | Men (n = 670) | p-Value ꝉ,* | CS1 (n = 1078) | CS2 (n = 353) | p-Value ꝉ,* | |
| Grains (g) | 135.9 (119.3) | 121.3 (107.5) | 155.2 (141.0) | <0.001 | 137.8 (116.8) | 122.9 (123.2) | 0.027 |
| Starchy vegetables (g) | 57.1 (61.1) | 52.8 (62.4) | 64.3 (69.4) | <0.001 | 59.5 (65.0) | 53.5 (60.5) | 0.069 |
| Fruits (g) | 294.6 (281.7) | 307.5 (281.0) | 283.4 (275.7) | 0.223 | 285.9 (269.2) | 331.4 (316.5) | 0.009 |
| Vegetables (g) | 224.0 (181.6) | 229.3 (197.2) | 217.3 (172.8) | <0.001 | 222.4 (174.5) | 227.9 (212.5) | 0.104 |
| Protein-rich foods (g) | 209.3 (145.8) | 184.6 (122.0) | 242.7 (164.8) | <0.001 | 209.6 (145.6) | 208.7 (150.1) | 0.998 |
| Ready-made meals (g) | 94.76 (104.6) | 74.0 (85.6) | 120.1 (116.0) | <0.001 | 96.3 (109.5) | 91.8 (91.8) | 0.099 |
| Dairy products (g) | 177.7 (201.9) | 179.7 (203.8) | 174.5 (202.3) | 0.210 | 175.5 (202.3) | 181.8 (205.4) | 0.677 |
| Lipids (fats and oils) (g) | 61.6 (51.6) | 58.9 (48.4) | 65.2 (58.1) | <0.001 | 61.6 (51.8) | 61.1 (53.6) | 0.088 |
| Sugary products (g) | 34.5 (41.2) | 32.0 (37.6) | 38.5 (43.5) | <0.001 | 33.6 (40.8) | 35.8 (42.8) | 0.282 |
| Non-caloric beverages (mL) | 1665 (999.3) | 1668 (1105) | 1660 (983.2) | 0.455 | 1662 (992.1) | 1673 (983.8) | 0.875 |
| Sugar-sweetened beverages (mL) | 70.2 (236.7) | 70.2 (233.3) | 70.2 (236.6) | 0.435 | 66.8 (236.6) | 72.0 (233.3) | 0.217 |
| Alcoholic beverages (mL) | 76.9 (157.4) | 42.8 (93.8) | 132.9 (226.1) | <0.001 | 85.4 (169.4) | 59.5 (108.5) | 0.038 |
| Variables | Median (IQR) | ||||||
|---|---|---|---|---|---|---|---|
| ORISCAV-LUX 2 (n = 1431) | Women (n = 761) | Men (n = 670) | p-Value ꝉ,* | CS1 (n = 1078) | CS2 (n = 353) | p-Value ꝉ,* | |
| Total energy (kcal) | 2375 (1143) | 2133 (920.5) | 2687 (1210) | <0.001 | 2395 (1129) | 2303 (1124) | 0.291 |
| Water (g) | 3080 (1263) | 3002 (1140) | 3161 (1390) | 0.004 | 3081 (1259) | 3057 (1228) | 0.692 |
| Protein total (g) | 89.0 (45.7) | 79.7 (38.5) | 102.3 (49.5) | <0.001 | 89.0 (45.3) | 89.0 (47.4) | 0.752 |
| Vegetable protein (g) | 26.9 (14.5) | 24.7 (12.5) | 29.4 (16.2) | <0.001 | 27.0 (14.6) | 25.8 (14.4) | 0.107 |
| Animal protein (g) | 60.1 (37.4) | 53.2 (31.3) | 69.4 (41.6) | <0.001 | 60.1 (37.3) | 60.8 (37.7) | 0.801 |
| Total fats (g) | 116.0 (65.5) | 108.0 (56.1) | 128.4 (68.0) | <0.001 | 117.4 (64.4) | 113.7 (68.3) | 0.423 |
| SFA (g) | 39.7 (23.3) | 36.0 (20.1) | 44.5 (25.3) | <0.001 | 40.1 (23.2) | 38.3 (23.6) | 0.499 |
| MUFA (g) | 46.9 (26.6) | 43.0 (22.4) | 52.7 (28.8) | <0.001 | 46.8 (27.0) | 47.2 (26.8) | 0.587 |
| PUFA (g) | 20.8 (13.6) | 19.6 (12.5) | 22.6 (14.6) | <0.001 | 20.9 (13.4) | 20.2 (14.5) | 0.269 |
| LA (g) | 17.3 (11.9) | 16.2 (11.2) | 18.8 (12.7) | <0.001 | 17.4 (11.7) | 16.8 (12.6) | 0.198 |
| ALA (g) | 1.80 (1.44) | 1.68 (1.49) | 1.93 (1.38) | <0.001 | 1.79 (1.47) | 1.82 (1.43) | 0.792 |
| ARA (g) | 0.19 (0.13) | 0.17 (0.11) | 0.22 (0.16) | <0.001 | 0.19 (0.13) | 0.19 (0.14) | 0.960 |
| EPA (g) | 0.20 (0.23) | 0.18 (0.23) | 0.21 (0.25) | <0.001 | 0.19 (0.23) | 0.20 (0.24) | 0.819 |
| DPA (g) | 0.08 (0.07) | 0.07 (0.07) | 0.08 (0.08) | <0.001 | 0.07 (0.07) | 0.08 (0.07) | 0.931 |
| DHA (g) | 0.28 (0.32) | 0.26 (0.31) | 0.29 (0.34) | <0.001 | 0.28 (0.31) | 0.29 (0.32) | 0.776 |
| Cholesterol (mg) | 356.2 (205.7) | 320.7 (169.7) | 395.4 (228.5) | <0.001 | 356.3 (206.4) | 354.3 (199.9) | 0.909 |
| Total carbohydrates (g) | 218.3 (110.4) | 197.1 (92.4) | 242.0 (119.2) | <0.001 | 219.7 (111.0) | 213.8 (113.2) | 0.339 |
| Simple sugars (g) | 101.3 (60.0) | 96.6 (55.3) | 109.2 (61.7) | <0.001 | 99.6 (58.4) | 105.3 (68.5) | 0.099 |
| Added simple sugars (g) | 28.7 (27.6) | 26.1 (24.1) | 32.4 (30.6) | <0.001 | 28.3 (26.9) | 29.3 (28.4) | 0.343 |
| Starch (g) | 103.7 (63.6) | 90.6 (52.9) | 119.1 (66.2) | <0.001 | 106.8 (63.6) | 94.8 (60.0) | 0.003 |
| Total fiber (g) | 23.2 (12.3) | 22.9 (11.8) | 24.0 (13.3) | 0.008 | 23.3 (11.9) | 23.1 (14.1) | 0.975 |
| Soluble fiber (g) | 4.75 (2.48) | 4.74 (2.46) | 4.74 (2.49) | 0.492 | 4.72 (2.38) | 4.81 (2.81) | 0.312 |
| Insoluble fiber (g) | 18.5 (10.1) | 18.1 (9.5) | 19.0 (10.7) | 0.002 | 18.4 (9.6) | 18.4 (11.5) | 0.819 |
| Alcohol (g) | 5.6 (11.5) | 3.3 (7.6) | 9.3 (15.8) | <0.001 | 6.4 (12.3) | 4.4 (8.7) | 0.010 |
| Beta-carotene (µg) | 4978 (4125) | 5157 (4472) | 4713 (3843) | 0.009 | 4960 (3956) | 5062 (5132) | 0.133 |
| Vitamin A (retinol, µg) | 476.8 (343.7) | 425.1 (281.2) | 547.7 (385.6) | <0.001 | 478.4 (336.0) | 460.5 (382.4) | 0.860 |
| Vitamin D (µg) | 5.1 (4.7) | 4.8 (4.4) | 5.6 (4.9) | <0.001 | 5.1 (4.6) | 5.0 (4.8) | 0.899 |
| Vitamin E (α-tocopherol equivalents, mg) | 18.3 (11.8) | 16.7 (9.6) | 20.3 (13.7) | <0.001 | 18.3 (11.5) | 18.3 (12.5) | 0.614 |
| Vitamin C (mg) | 145.6 (104.8) | 150.9 (104.6) | 142.4 (101.2) | 0.159 | 143.4 (101.8) | 157.5 (120.9) | 0.009 |
| Vitamin B1 (mg) | 1.5 (0.8) | 1.4 (0.6) | 1.7 (0.9) | <0.001 | 1.5 (0.8) | 1.5 (.08) | 0.819 |
| Vitamin B2 (mg) | 1.8 (1.0) | 1.6 (0.8) | 2.1 (1.1) | <0.001 | 1.8 (0.9) | 1.8 (1.0) | 0.592 |
| Vitamin B3 (mg) | 23.0 (12.1) | 20.1 (9.7) | 26.2 (13.3) | <0.001 | 23.0 (11.8) | 22.3 (12.3) | 0.930 |
| Vitamin B5 (mg) | 5.8 (2.9) | 5.3 (2.5) | 6.5 (3.4) | <0.001 | 5.8 (2.8) | 5.7 (3.2) | 0.734 |
| Vitamin B6 (mg) | 2.4 (1.3) | 2.2 (1.0) | 2.6 (1.4) | <0.001 | 2.3 (1.2) | 2.3 (1.3) | 0.596 |
| Vitamin B9 (µg) | 350.8 (174.9) | 340.3 (164.3) | 363.7 (187.7) | <0.001 | 351.2 (170.7) | 347.3 (190.4) | 0.740 |
| Vitamin B12 (µg) | 6.3 (4.5) | 5.5 (4.0) | 7.4 (5.0) | <0.001 | 6.2 (4.4) | 6.3 (4.9) | 0.850 |
| Calcium (mg) | 930.5 (452.8) | 893.8 (431.1) | 984.1 (477.8) | <0.001 | 938.5 (450.3) | 899.8 (474.8) | 0.807 |
| Iron (mg) | 14.3 (6.8) | 13.2 (6.0) | 15.8 (7.8) | <0.001 | 14.3 (6.7) | 14.2 (7.4) | 0.622 |
| Iodide (µg) | 154.3 (80.3) | 143.9 (72.2) | 166.9 (86.8) | <0.001 | 155.2 (78.9) | 152.1 (83.3) | 0.846 |
| Magnesium (mg) | 372.1 (162.4) | 352.5 (144.1) | 405.6 (176.0) | <0.001 | 373.2 (162.8) | 371.1 (167.3) | 0.794 |
| Sodium (mg) | 3310 (1968) | 2929 (1536) | 3870 (2210) | <0.001 | 3339 (1978) | 3229 (2005) | 0.533 |
| Potassium (mg) | 3547 (1563) | 3370 (1452) | 3725 (1685) | <0.001 | 3544 (1505) | 3562 (1749) | 0.112 |
| Phosphorous (mg) | 1326 (622) | 1205 (538) | 1504 (712) | <0.001 | 1329 (624.6) | 1295 (617.4) | 0.671 |
| Variables | ORISCAV-LUX 2 (n = 1431) | |||
|---|---|---|---|---|
| All | Gender | Age Categories | BMI Categories | |
| Total energy (kcal) | −0.058 * | – | – | – |
| Vegetable protein (g) | −0.059 * | – | – | – |
| Total fats (g) | −0.053 * | – | – | – |
| PUFA (g) | −0.054 * | – | −0.114 *,e | −0.129 *,i |
| Starch (g) | −0.092 ** | – | −0.140 **,e | −0.093 *,g |
| Alcohol (g) | −0.083 ** | – | −0.143 *,a,d −0.108 *,a,e | −0.182 **,h |
| Vitamin C (mg) | 0.054 *,a | – | – | – |
| Grains (g) | −0.078 ** | – | −0.107 *,f | −0.084 *,g |
| Starchy vegetables (g) | −0.061 * | – | – | – |
| Fruits (g) | 0.067 *,a | 0.105 **,a,b | – | – |
| Vegetables (g) | 0.062 *,a | 0.076 *,a,c | – | – |
| Lipids (g) | −0.068 * | – | −0.127 *,d | −0.129 *,i |
| Alcoholic beverages (mL) | −0.083 ** | – | −0.143 *,a,d | −0.121 *,h |
| Variables | ORISCAV-LUX 2 (n = 1431) | |||
|---|---|---|---|---|
| Beta Non-Standardized | Beta Standardized | CI 95% | p-Value | |
| Grains (g) | −0.616 | −0.059 | −1.183, −0.048 | 0.033 |
| Vegetables (g) | 0.545 | 0.044 | -0.097, 1.186 | 0.096 |
| Lipids (g) | −0.838 | −0.063 | −1.551, −0.126 | 0.021 |
| Sugary products (g) | 0.540 | 0.068 | 0.105, 0.974 | 0.015 |
| Variables | ORISCAV-LUX 2 (n = 1431) | |||
|---|---|---|---|---|
| Beta Non-Standardized | Beta Standardized | CI 95% | p-Value | |
| Total energy (kcal) | 5.239 | 0.225 | 0.366, 10.112 | 0.035 |
| Total fats (g) | −4.170 | −0.207 | −7.455, −0.885 | 0.013 |
| Starch (g) | −2.912 | −0.171 | −4.466, −1.358 | <0.001 |
| Sodium intake (mg) | 2.040 | 0.109 | 0.206, 3.874 | 0.029 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rollet, M.; Bohn, T.; Vahid, F.; on behalf of the ORISCAV Working Group. Association between Dietary Factors and Constipation in Adults Living in Luxembourg and Taking Part in the ORISCAV-LUX 2 Survey. Nutrients 2022, 14, 122. https://doi.org/10.3390/nu14010122
Rollet M, Bohn T, Vahid F, on behalf of the ORISCAV Working Group. Association between Dietary Factors and Constipation in Adults Living in Luxembourg and Taking Part in the ORISCAV-LUX 2 Survey. Nutrients. 2022; 14(1):122. https://doi.org/10.3390/nu14010122
Chicago/Turabian StyleRollet, Maurane, Torsten Bohn, Farhad Vahid, and on behalf of the ORISCAV Working Group. 2022. "Association between Dietary Factors and Constipation in Adults Living in Luxembourg and Taking Part in the ORISCAV-LUX 2 Survey" Nutrients 14, no. 1: 122. https://doi.org/10.3390/nu14010122
APA StyleRollet, M., Bohn, T., Vahid, F., & on behalf of the ORISCAV Working Group. (2022). Association between Dietary Factors and Constipation in Adults Living in Luxembourg and Taking Part in the ORISCAV-LUX 2 Survey. Nutrients, 14(1), 122. https://doi.org/10.3390/nu14010122