
Association of Nut Consumption with Risk of Stroke and Cardiovascular Disease: The Million Veteran Program

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Assessment of Nut Intake
2.3. Outcome Ascertainment
2.4. Assessment of Covariates
2.5. Statistical Analysis
3. Results
3.1. Participant Characteristics
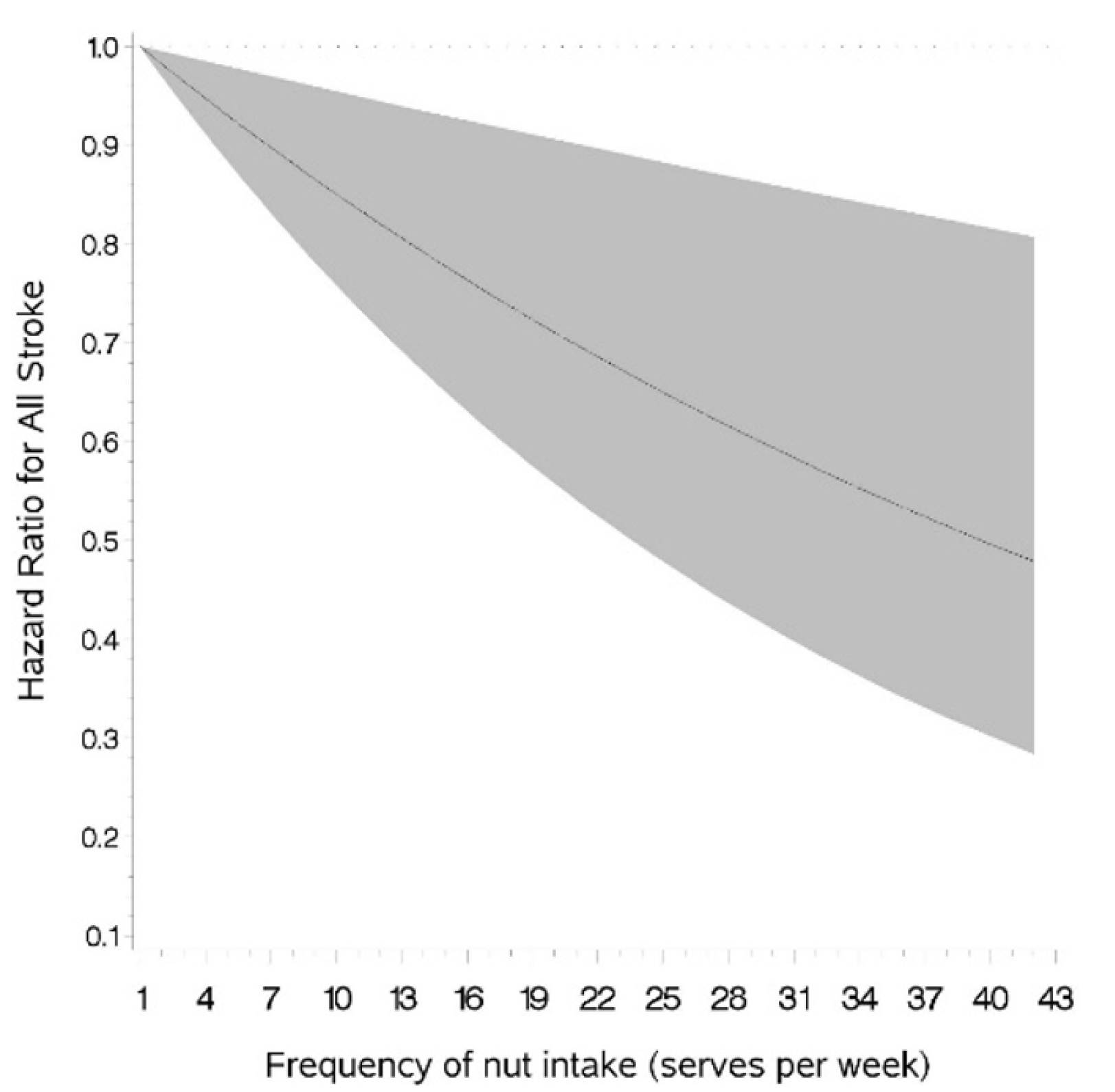
3.2. Association of Nut Intake with Risk of Stroke
3.3. Association of Peanut Butter Intake with Risk of Stroke
3.4. Association of Nut Intake with Risk of Coronary Artery Disease (CAD) and Mortality Form Cardiovascular Disease
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R. Heart disease and stroke statistics—2019 update: A report from the American Heart Association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef]
- Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Ruiz-Gutiérrez, V.; Covas, M.I.; Fiol, M.; Gómez-Gracia, E.; López-Sabater, M.C.; Vinyoles, E. Effects of a Mediterranean-style diet on cardiovascular risk factors: A randomized trial. Ann. Intern. Med. 2006, 145, 1–11. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J. Primary prevention of cardiovascular disease with a Mediterranean diet. N. Engl. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, G.; Guasch-Ferré, M.; Hu, Y.; Li, Y.; Hu, F.B.; Rimm, E.B.; Manson, J.E.; Rexrode, K.M.; Sun, Q. Nut consumption in relation to cardiovascular disease incidence and mortality among patients with diabetes mellitus. Circ. Res. 2019, 124, 920–929. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Keum, N.; Giovannucci, E.; Fadnes, L.T.; Boffetta, P.; Greenwood, D.C.; Tonstad, S.; Vatten, L.J.; Riboli, E.; Norat, T. Nut consumption and risk of cardiovascular disease, total cancer, all-cause and cause-specific mortality: A systematic review and dose-response meta-analysis of prospective studies. BMC Med. 2016, 14, 207. [Google Scholar] [CrossRef] [Green Version]
- Grosso, G.; Yang, J.; Marventano, S.; Micek, A.; Galvano, F.; Kales, S.N. Nut consumption on all-cause, cardiovascular, and cancer mortality risk: A systematic review and meta-analysis of epidemiologic studies. Am. J. Clin. Nutr. 2015, 101, 783–793. [Google Scholar] [CrossRef] [Green Version]
- Djousse, L.; Gaziano, J.M.; Kase, C.S.; Kurth, T. Nut consumption and risk of stroke in US male physicians. Clin. Nutr. 2010, 29, 605–609. [Google Scholar] [CrossRef] [Green Version]
- Weng, Y.Q.; Yao, J.; Guo, M.L.; Qin, Q.J.; Li, P. Association between nut consumption and coronary heart disease: A meta-analysis. Coron. Artery Dis. 2016, 27, 227–232. [Google Scholar] [CrossRef]
- Luo, C.; Zhang, Y.; Ding, Y.; Shan, Z.; Chen, S.; Yu, M.; Hu, F.B.; Liu, L. Nut consumption and risk of type 2 diabetes, cardiovascular disease, and all-cause mortality: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2014, 100, 256–269. [Google Scholar] [CrossRef] [Green Version]
- Gaziano, J.M.; Concato, J.; Brophy, M.; Fiore, L.; Pyarajan, S.; Breeling, J.; Whitbourne, S.; Deen, J.; Shannon, C.; Humphries, D.; et al. Million Veteran Program: A mega-biobank to study genetic influences on health and disease. J. Clin. Epidemiol. 2016, 70, 214–223. [Google Scholar] [CrossRef] [Green Version]
- U.S. Department of Veterans Affairs. System of Records Notice 97VA10P1: Consolidated Data Information System-VA; 76 FR 25409; U.S. Department of Veterans Affairs: Washington, DC, USA, 4 May 2011.
- Center of Excellence for Suicide Prevention. Joint Department of Veterans Affairs (VA) and Department of Defense (DoD) Suicide Data Repository—National Death Index (NDI). Available online: http://vaww.virec.research.va.gov/Mortality/Overview.htm (accessed on 26 August 2021).
- Djoussé, L.; Ho, Y.L.; Nguyen, X.M.T.; Gagnon, D.R.; Wilson, P.W.; Cho, K.; Gaziano, J.M.; VA Million Veteran Program; Halasz, I.; Federman, D.; et al. DASH score and subsequent risk of coronary artery disease: The findings from Million Veteran Program. J. Am. Heart Assoc. 2018, 7, e008089. [Google Scholar] [CrossRef]
- Li, R.; Hertzmark, E.; Louie, M.; Chen, L.; Spiegelman, D. The SAS lgtphcurv9 Macro; Channing Lab: Boston, MA, USA, 2011. [Google Scholar]
- Coates, A.; Hill, A.; Tan, S. Nuts and cardiovascular disease prevention. Curr. Atheroscler. Rep. 2018, 20, 48. [Google Scholar] [CrossRef]
- Kim, Y.; Keogh, J.B.; Clifton, P.M. Benefits of nut consumption on insulin resistance and cardiovascular risk factors: Multiple potential mechanisms of actions. Nutrients 2017, 9, 1271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgillo, S.; Hill, A.M.; Coates, A.M. The effects of nut consumption on vascular function. Nutrients 2019, 11, 116. [Google Scholar] [CrossRef] [Green Version]
- Bsc, S.N.; Bsc, G.S. Oxalate content of foods and its effect on humans. Asia Pac. J. Clin. Nutr. 1999, 8, 64–74. [Google Scholar] [CrossRef]
- Coates, A.M.; Howe, P.R. Edible nuts and metabolic health. Curr. Opin. Lipidol. 2007, 18, 25–30. [Google Scholar] [CrossRef]
- Bitok, E.; Sabaté, J. Nuts and cardiovascular disease. Prog. Cardiovasc. Dis. 2018, 61, 33–37. [Google Scholar] [CrossRef]
- Ros, E. Nuts and CVD. Br. J. Nutr. 2015, 113, S111–S120. [Google Scholar] [CrossRef] [Green Version]
- Arya, S.S.; Salve, A.R.; Chauhan, S. Peanuts as functional food: A review. J. Food Sci. Technol. 2016, 53, 31–41. [Google Scholar] [CrossRef] [Green Version]
- U.S. Department of Agriculture; U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2020–2025, 9th ed.; U.S. Department of Agriculture: Washington, DC, USA, 2020.
- Guasch-Ferré, M.; Satija, A.; Blondin, S.A.; Janiszewski, M.; Emlen, E.; O’Connor, L.E.; Campbell, W.W.; Hu, F.B.; Willett, W.C.; Stampfer, M.J. Meta-analysis of randomized controlled trials of red meat consumption in comparison with various comparison diets on cardiovascular risk factors. Circulation 2019, 139, 1828–1845. [Google Scholar] [CrossRef]
- Kim, Y.; Keogh, J.B.; Clifton, P.M. Does nut consumption reduce mortality and/or risk of cardiometabolic disease? An updated review based on meta-analyses. Int. J. Environ. Res. Public Health 2019, 16, 4957. [Google Scholar] [CrossRef] [Green Version]
- Jafari Azad, B.; Daneshzad, E.; Azadbakht, L. Peanut and cardiovascular disease risk factors: A systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 2020, 60, 1123–1140. [Google Scholar] [CrossRef] [PubMed]
- Del Gobbo, L.C.; Falk, M.C.; Feldman, R.; Lewis, K.; Mozaffarian, D. Effects of tree nuts on blood lipids, apolipoproteins, and blood pressure: Systematic review, meta-analysis, and dose-response of 61 controlled intervention trials. Am. J. Clin. Nutr. 2015, 102, 1347–1356. [Google Scholar] [CrossRef] [Green Version]
- Moncada, S.; Higgs, A. The L-arginine-nitric oxide pathway. N. Engl. J. Med. 1993, 329, 2002–2012. [Google Scholar]
- Mohammadifard, N.; Salehi-Abargouei, A.; Salas-Salvadó, J.; Guasch-Ferré, M.; Humphries, K.; Sarrafzadegan, N. The effect of tree nut, peanut, and soy nut consumption on blood pressure: A systematic review and meta-analysis of randomized controlled clinical trials. Am. J. Clin. Nutr. 2015, 101, 966–982. [Google Scholar] [CrossRef] [Green Version]
- van den Brandt, P.A.; Schouten, L.J. Relationship of tree nut, peanut and peanut butter intake with total and cause-specific mortality: A cohort study and meta-analysis. Int. J. Epidemiol. 2015, 44, 1038–1049. [Google Scholar] [CrossRef] [Green Version]
- Hu, F.B.; Stampfer, M.J.; Manson, J.E.; Rimm, E.B.; Colditz, G.A.; Rosner, B.A.; Speizer, F.E.; Hennekens, C.H.; Willett, W.C. Frequent nut consumption and risk of coronary heart disease in women: Prospective cohort study. Br. Med. J. 1998, 317, 1341–1345. [Google Scholar] [CrossRef] [Green Version]
- Brandt, E.J.; Myerson, R.; Perraillon, M.C.; Polonsky, T.S. Hospital admissions for myocardial infarction and stroke before and after the trans-fatty acid restrictions in New York. JAMA Cardiol. 2017, 2, 627–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. Department of Agriculture; Agricultural Research Service. USDA Food and Nutrient Database for Dietary Studies 2017–2018. Food Surveys Research Group Home Page. 2020. Available online: http://www.ars.usda.gov/nea/bhnrc/fsrg (accessed on 20 July 2021).
- Sabaté, J.; Sranacharoenpong, K.; Harwatt, H.; Wien, M.; Soret, S. The environmental cost of protein food choices. Public Health Nutr. 2015, 18, 2067–2073. [Google Scholar] [CrossRef] [Green Version]
- Volpe, R.; Messineo, S.; Volpe, M.; Messineo, A. Carbon footprint of tree nuts based consumer products. Sustainability 2015, 7, 14917–14934. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Frequency of Nut Consumption | |||||
|---|---|---|---|---|---|
| <1/Month | 1–3/Month | 1/Week | 2–4/Week | ≥5/Week | |
| Number | 37,075 | 50,238 | 35,863 | 33,500 | 23,151 |
| CHARACTERISTICS | |||||
| Age (years ) | 64.6 ± 11.7 | 63.7 ± 12.1 | 63.5 ± 12.1 | 64.1 ± 11.9 | 65.2 ± 12.0 |
| BMI (kg/m2) | 29.2 ± 5.9 | 29.5 ± 5.5 | 29.4 ± 5.4 | 29.0 ± 5.2 | 28.3 ± 5.1 |
| Male (%) | 90.6 | 89.9 | 90.3 | 89.8 | 88.7 |
| Race | |||||
| White (%) | 84.1 | 83.7 | 84.8 | 84.8 | 86.5 |
| Black (%) | 11.8 | 11.7 | 10.7 | 10.9 | 9.3 |
| Education | |||||
| <Highschool (%) | 4.2 | 2.3 | 1.6 | 1.3 | 1.2 |
| Highschool/GED (%) | 26.9 | 20.2 | 16.8 | 14.8 | 12.6 |
| College/AA/Bachelors (%) | 59.9 | 64.4 | 65.3 | 65.1 | 62.9 |
| Postgraduate degree (%) | 9.0 | 13.2 | 16.3 | 18.8 | 23.4 |
| Smoking | |||||
| Never (%) | 25.2 | 30.1 | 31.9 | 33.5 | 35.1 |
| Former (%) | 50.1 | 51.6 | 51.7 | 52.5 | 53.7 |
| Current (%) | 24.6 | 18.3 | 16.4 | 14.0 | 11.2 |
| Exercise | |||||
| <1 time /week (%) | 51.6 | 44.2 | 37.7 | 33.2 | 29.7 |
| 1 time/week (%) | 12.3 | 14.1 | 15.4 | 14.2 | 12.9 |
| 2–4 time/week (%) | 23.1 | 28.7 | 32.9 | 36.4 | 37.0 |
| ≥ 5 times/week (%) | 13.0 | 13.0 | 14.0 | 16.2 | 20.5 |
| Peanut butter (Tbs/day ) | 0.2 ± 0.4 | 0.2 ± 0.4 | 0.2 ± 0.4 | 0.3 ± 0.4 | 0.4 ± 0.7 |
| DASH score | 18.9 ± 4.8 | 20.1 ± 4.6 | 21.4 ± 4.5 | 23.2 ± 4.4 | 25.1 ± 4.4 |
| Alcohol | |||||
| Abstainer (%) | 7.8 | 7.1 | 6.4 | 6.5 | 7.3 |
| Former (%) | 45.7 | 36.0 | 33.3 | 30.5 | 31.5 |
| Current (%) | 46.5 | 56.9 | 60.3 | 62.9 | 61.2 |
| Frequency of Nut Intake | p Value | |||||
|---|---|---|---|---|---|---|
| <1/Month | 1–3/Month | 1/Week | 2–4/Week | ≥5/Week | (Linear Trend) | |
| Number of participants | 37,075 | 50,238 | 35,863 | 33,500 | 23,151 | |
| Total stroke (n) | 959 | 1036 | 647 | 546 | 382 | |
| Crude | 1.00 (ref) | 0.79 (0.72, 0.86) | 0.70 (0.63, 0.77) | 0.64 (0.57, 0.71) | 0.65 (0.57, 0.73) | <0.0001 |
| Age-adjusted | 1.00 (ref) | 0.81 (0.74, 0.88) | 0.72 (0.65, 0.79) | 0.64 (0.57, 0.71) | 0.62 (0.55, 0.70) | <0.0001 |
| Multivariate-adjusted a | 1.00 (ref) | 0.90 (0.83, 0.99) | 0.85 (0.77, 0.95) | 0.80 (0.72, 0.89) | 0.81 (0.72, 0.92) | 0.002 |
| Atherosclerotic ischemic stroke (n) | 904 | 981 | 602 | 516 | 359 | |
| Crude | 1.00 (ref) | 0.79 (0.72, 0.87) | 0.69 (0.62, 0.77) | 0.64 (0.57, 0.71) | 0.64 (0.57, 0.73) | <0.0001 |
| Age-adjusted | 1.00 (ref) | 0.81 (0.74, 0.89) | 0.71 (0.64, 0.78) | 0.64 (0.57, 0.71) | 0.62 (0.55, 0.70) | <0.0001 |
| Multivariate-adjusted a | 1.00 (ref) | 0.91 (0.83, 1.00) | 0.84 (0.76, 0.93) | 0.80 (0.71, 0.89) | 0.81 (0.71, 0.92) | 0.005 |
| Hemorrhagic stroke (n) | 75 | 71 | 57 | 76 | ||
| Crude | 1.00 (ref) | 0.69 (0.50, 0.96) | 0.79 (0.56, 1.12) | 0.67 (0.49, 0.93) | 0.046 | |
| Age-adjusted | 1.00 (ref) | 0.71 (0.51, 0.98) | 0.81 (0.57, 1.14) | 0.67 (0.48, 0.91) | 0.030 | |
| Multivariate-adjusted a | 1.00 (ref) | 0.80 (0.58, 1.11) | 0.99 (0.69, 1.41) | 0.85 (0.61, 1.20) | 0.160 | |
| Frequency of Nut Intake | p Value | |||||
|---|---|---|---|---|---|---|
| <1/Month | 1–3/Month | 1/Week | 2–4/Week | ≥5/Week | (Linear Trend) | |
| Number of participants | 43,897 | 44,716 | 35,729 | 35,035 | 19,395 | |
| Total stroke (n) | 949 | 873 | 681 | 645 | 384 | |
| Crude | 1.00 (ref) | 0.90 (0.82, 0.99) | 0.90 (0.81, 0.99) | 0.86 (0.78, 0.95) | 0.93 (0.82, 1.04) | 0.94 |
| Age-adjusted | 1.00 (ref) | 0.93 (0.85, 1.02) | 0.90 (0.82, 0.99) | 0.84 (0.76, 0.93) | 0.89 (0.79, 1.00) | 0.54 |
| Multivariate-adjusted a | 1.00 (ref) | 0.94 (0.85, 1.03) | 0.93 (0.84, 1.03) | 0.88 (0.79, 0.97) | 0.94 (0.83, 1.06) | 0.90 |
| Atherosclerotic ischemic stroke (n) | 896 | 814 | 641 | 612 | 363 | |
| Crude | 1.00 (ref) | 0.89 (0.81, 0.98) | 0.89 (0.81, 0.99) | 0.87 (0.78, 0.96) | 0.93 (0.82, 1.05) | 0.76 |
| Age-adjusted | 1.00 (ref) | 0.92 (0.84, 1.02) | 0.90 (0.81, 0.99) | 0.84 (0.76, 0.93) | 0.89 (0.79, 1.00) | 0.71 |
| Multivariate-adjusted a | 1.00 (ref) | 0.92 (0.84, 1.01) | 0.92 (0.83, 1.02) | 0.88 (0.79, 0.97) | 0.94 (0.83, 1.06) | 0.79 |
| Hemorrhagic stroke (n) | 70 | 71 | 56 | 78 | ||
| Crude | 1.00 (ref) | 1.00 (0.72, 1.39) | 1.00 (0.70, 1.42) | 0.91 (0.66, 1.26) | 0.53 | |
| Age-adjusted | 1.00 (ref) | 1.03 (0.74, 1.44) | 1.01 (0.71, 1.43) | 0.88 (0.64, 1.22) | 0.40 | |
| Multivariate-adjusted a | 1.00 (ref) | 1.05 (0.76, 1.47) | 1.07 (0.75, 1.53) | 0.96 (0.69, 1.33) | 0.56 | |
| Frequency of Nut Intake | p Value | |||||
|---|---|---|---|---|---|---|
| <1/Month | 1–3/Month | 1/Week | 2–4/Week | ≥5/Week | (Linear Trend) | |
| Number of participants | 37,075 | 50,238 | 35,863 | 33,500 | 23,151 | |
| Coronary artery disease (n) | 2501 | 2911 | 1877 | 1599 | 1020 | |
| Crude | 1.00 (ref) | 0.85 (0.81, 0.90) | 0.78 (0.73, 0.82) | 0.71 (0.67, 0.76) | 0.66 (0.61, 0.71) | <0.0001 |
| Age-adjusted | 1.00 (ref) | 0.87 (0.82, 0.92) | 0.79 (0.75, 0.84) | 0.71 (0.67, 0.76) | 0.64 (0.59, 0.69) | <0.0001 |
| Multivariate-adjusted a | 1.00 (ref) | 0.93 (0.89, 0.99) | 0.89 (0.84, 0.95) | 0.83 (0.78, 0.89) | 0.78 (0.72, 0.84) | <0.0001 |
| Cardiovascular disease mortality (n) | 361 | 393 | 218 | 192 | 147 | |
| Crude | 1.00 (ref) | 0.80 (0.69, 0.92) | 0.63 (0.53, 0.74) | 0.59 (0.50, 0.71) | 0.66 (0.55, 0.80) | 0.004 |
| Age-adjusted | 1.00 (ref) | 0.86 (0.74, 0.99) | 0.68 (0.57, 0.80) | 0.61 (0.51, 0.73) | 0.61 (0.50, 0.74) | 0.0001 |
| Multivariate-adjusted a | 1.00 (ref) | 0.95 (0.82, 1.10) | 0.79 (0.66, 0.94) | 0.74 (0.62, 0.89) | 0.76 (0.63, 0.93) | 0.040 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ivey, K.L.; Nguyen, X.-M.T.; Quaden, R.M.; Ho, Y.-L.; Cho, K.; Gaziano, J.M.; Djoussé, L. Association of Nut Consumption with Risk of Stroke and Cardiovascular Disease: The Million Veteran Program. Nutrients 2021, 13, 3031. https://doi.org/10.3390/nu13093031
Ivey KL, Nguyen X-MT, Quaden RM, Ho Y-L, Cho K, Gaziano JM, Djoussé L. Association of Nut Consumption with Risk of Stroke and Cardiovascular Disease: The Million Veteran Program. Nutrients. 2021; 13(9):3031. https://doi.org/10.3390/nu13093031
Chicago/Turabian StyleIvey, Kerry L., Xuan-Mai T. Nguyen, Rachel M. Quaden, Yuk-Lam Ho, Kelly Cho, J. Michael Gaziano, and Luc Djoussé. 2021. "Association of Nut Consumption with Risk of Stroke and Cardiovascular Disease: The Million Veteran Program" Nutrients 13, no. 9: 3031. https://doi.org/10.3390/nu13093031
APA StyleIvey, K. L., Nguyen, X.-M. T., Quaden, R. M., Ho, Y.-L., Cho, K., Gaziano, J. M., & Djoussé, L. (2021). Association of Nut Consumption with Risk of Stroke and Cardiovascular Disease: The Million Veteran Program. Nutrients, 13(9), 3031. https://doi.org/10.3390/nu13093031