
No Correlation between Positive Fructose Hydrogen Breath Test and Clinical Symptoms in Children with Functional Gastrointestinal Disorders: A Retrospective Single-Centre Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rezaie, A.; Buresi, M.; Lembo, A.; Lin, H.; McCallum, R.; Rao, S.; Schmulson, M.; Valdovinos, M.; Zakko, S.; Pimentel, M. Hydrogen and methane-based breath testing in gastrointestinal disorders: The North American Consensus. Am. J. Gastroenterol. 2017, 112, 775–784. [Google Scholar] [CrossRef] [Green Version]
- Fedewa, A.; Rao, S.S. Dietary fructose intolerance, fructan intolerance and FODMAPs. Curr. Gastroenterol. Rep. 2014, 16, 370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, Y.K.; Johlin, F.C.; Summers, R.W.; Jackson, M.; Rao, S.S. Fructose intolerance: An under-recognized problem. Am. J. Gastroenterol. 2003, 98, 1348–1353. [Google Scholar] [CrossRef] [PubMed]
- Pituch, A.; Matczuk, P.; Neścioruk, M. Żywienie dzieci w zdrowiu i chorobie. Nietolerancja fruktozy. In Gastroenterologia Dziecięca. Poradnik Lekarza Praktyka; Czelej: Lublin, Poland, 2014; pp. 336–338. [Google Scholar]
- Nowak, M.; Gulbicka, P.; Grzymisławski, M. Wodorowe testy oddechowe jako narzędzie w diagnostyce schorzeń gastroenterologicznych. Forum Zaburzeń Metab. 2015, 6, 124–135. [Google Scholar]
- Tsampalieros, A.; Beauchamp, J.; Boland, M.; Mack, D.R. Dietary fructose intolerance in children and adolescents. Arch. Dis. Child. 2008, 93, 1078. [Google Scholar] [CrossRef] [PubMed]
- Putkonen, L.; Yao, C.K.; Gibson, P.R. Fructose malabsorption syndrome. Curr. Opin. Clin. Nutr. Metab. Care 2013, 16, 473–477. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Azcona, O.; Moreno-Álvarez, A.; Seoane-Pillado, T.; Niño-Grueiro, I.; Ramiro-Comesaña, A.; Menéndez-Riera, M.; Pérez-Domínguez, M.; Solar-Boga, A.; Leis-Trabazo, R. Fructose malabsorption in asymptomatic children and in patients with functional chronic abdominal pain: A prospective comparative study. Eur. J. Pediatr. 2019, 178, 1395–1403. [Google Scholar] [CrossRef]
- Biesiekierski, J.R. Fructose-induced symptoms beyond malabsorption in FGID. United Eur. Gastroenterol. J. 2014, 2, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Hyams, J.S.; Di Lorenzo, C.; Saps, M.; Shulman, R.J.; Staiano, A.; van Tilburg, M. Childhood Functional Gastrointestinal Disorders: Child/Adolescent. Gastroenterology 2016, 150, 1456–1468. [Google Scholar] [CrossRef]
- Hammer, V.; Hammer, K.; Memaran, N.; Huber, W.D.; Hammer, K.; Hammer, J. Relationship between abdominal symptoms and fructose ingestion in children with chronic abdominal pain. Dig. Dis. Sci. 2018, 63, 1270–1279. [Google Scholar] [CrossRef] [Green Version]
- Ebert, K.; Witt, H. Fructose malabsorption. Mol. Cell Pediatr. 2016, 3, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Ledochowski, M.; Ledochowski, L. Hydrogen Breath Tests; Manual of Bedfont Scientific Ltd., Akadmed-Verlag: Salzburg-Innsbruck, Austria, 2011. [Google Scholar]
- Eisenmann, A.; Amann, A.; Said, M.; Datta, B.; Ledochowski, M. Implementation and interpretation of hydrogen breath tests. J. Breath Res. 2008, 2, 046002. [Google Scholar] [CrossRef] [PubMed]
- Kyaw, M.H.; Mayberry, J.F. Fructose malabsorption: True condition or a variance from normality. J. Clin. Gastroenterol. 2011, 45, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Hoekstra, J.H.; van Kempen, A.A.; Bijl, S.B.; Kneepkens, C.M. Fructose breath hydrogen tests. Arch. Dis. Child. 1993, 68, 136–138. [Google Scholar] [CrossRef] [Green Version]
- Jones, H.F.; Butler, R.N.; Moore, D.J.; Brooks, D.A. Developmental changes and fructose absorption in children: Effect on malabsorption testing and dietary management. Nutr. Rev. 2013, 71, 300–309. [Google Scholar] [CrossRef]
- Wirth, S.; Klodt, C.; Wintermeyer, P.; Berrang, J.; Hensel, K.; Langer, T.; Heusch, A. Positive or negative fructose breath test results do not predict response to fructose restricted diet in children with recurrent abdominal pain: Results from a prospective randomized trial. Klin. Padiatr. 2014, 226, 268–273. [Google Scholar] [CrossRef]
- Frieling, T.; Kuhlbusch-Zicklam, R.; Kalde, S.; Heise, J. Fructose malabsorption: How much fructose can a healthy subject tolerate? Digestion 2011, 84, 269–272. [Google Scholar] [CrossRef]
- Amieva-Balmori, M.; Coss-Adame, E.; Rao, N.S.; Dávalos-Pantoja, B.M.; Rao, S.S.C. Diagnostic Utility of Carbohydrate Breath Tests for SIBO, Fructose, and Lactose Intolerance. Dig. Dis. Sci. 2020, 65, 1405–1413. [Google Scholar] [CrossRef]
- Posovszky, C.; Roesler, V.; Becker, S.; Iven, E.; Hudert, C.; Ebinger, F.; Calvano, C.; Warschburger, P. Roles of lactose and fructose malabsorption and dietary outcomes in children presenting with chronic abdominal pain. Nutrients 2019, 11, 3063. [Google Scholar] [CrossRef] [Green Version]
- Gijsbers, C.F.M.; Kneepkens, C.M.F.; Büller, H.A. Lactose and fructose malabsorption in children with recurrent abdominal pain: Results of double-blinded testing. Acta Paediatr. 2012, 101, 411–415. [Google Scholar] [CrossRef]
- Escobar, M.A.; Lustig, D.; Pflugeisen, B.M.; Amoroso, P.J.; Sherif, D.; Saeed, R.; Shamdeen, S.; Tuider, J.; Abdullah, B. Fructose intolerance/malabsorption and recurrent abdominal pain in children. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 498–501. [Google Scholar] [CrossRef] [PubMed]
- Gomara, R.E.; Halata, M.S.; Newman, L.J.; Bostwick, H.E.; Berezin, S.H.; Cukaj, L.; See, M.C.; Medow, M.S. Fructose intolerance in children presenting with abdominal pain. J. Pediatr. Gastroenterol. Nutr. 2008, 47, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Mehta, M.; Beg, M. Fructose Intolerance: Cause or Cure of Chronic Functional Constipation. Glob. Pediatr. Health 2018, 5, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilder-Smith, C.H.; Materna, A.; Wermelinger, C.; Schuler, J. Fructose and lactose intolerance and malabsorption testing: The relationship with symptoms in functional gastrointestinal disorders. Aliment. Pharmacol. Ther. 2013, 37, 1074–1083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gasbarrini, A.; Corazza, G.R.; Gasbarrini, G.; Montalto, M.; Di Stefano, M.; Basilisco, G.; Parodi, A.; Usai-Satta, P.; Vernia, P.; Anania, C.; et al. Methodology and indications of H2-breath testing in gastrointestinal diseases: The Rome Consensus Conference. Aliment. Pharmacol. Ther. 2009, 29, 1–49. [Google Scholar] [CrossRef]
- Misselwitz, B.; Fox, M. The Fructose Hydrogen Breath Test: Nothing Behind the Sweet Fog? Digestion 2019, 99, 191–193. [Google Scholar] [CrossRef] [Green Version]
- De Roest, R.H.; Dobbs, B.R.; Chapman, B.A.; Batman, B.; O’Brien, L.A.; Leeper, J.A.; Hebblethwaite, C.R.; Gearry, R.B. The low FODMAP diet improves gastrointestinal symptoms in patients with irritable bowel syndrome: A prospective study. Int. J. Clin. Pract. 2013, 67, 895–903. [Google Scholar] [CrossRef]
- Bellini, M.; Tonarelli, S.; Nagy, A.G.; Pancetti, A.; Costa, F.; Ricchiuti, A.; de Bortoli, N.; Mosca, M.; Marchi, S.; Rossi, A. Low FODMAP diet: Evidence, doubts, and hopes. Nutrients 2020, 12, 148. [Google Scholar] [CrossRef] [Green Version]
- Altobelli, E.; Del Negro, V.; Angeletti, P.M.; Latella, G. Low-FODMAP diet improves irritable bowel syndrome symptoms: A meta-analysis. Nutrients 2017, 9, 940. [Google Scholar] [CrossRef]
- Jones, H.F.; Burt, E.; Dowling, K.; Davidson, G.; Brooks, D.A.; Butler, R.N. Effect of age on fructose malabsorption in children presenting with gastrointestinal symptoms. J. Pediatr. Gastroenterol. Nutr. 2011, 52, 581–584. [Google Scholar] [CrossRef]

{kind=link}
| Parameter | Mean ± SD or Number (%) |
|---|---|
| Age | 10.67 ± 4.3 |
| Male (%) | 144 (44.6%) |
| Female (%) | 179 (55.4%) |
| Height (cm) | 141.08 ± 22.03 |
| Weight (kg) | 38.3 ± 17.67 |
| BMI (kg/m2) | 18.07 ± 3.81 |
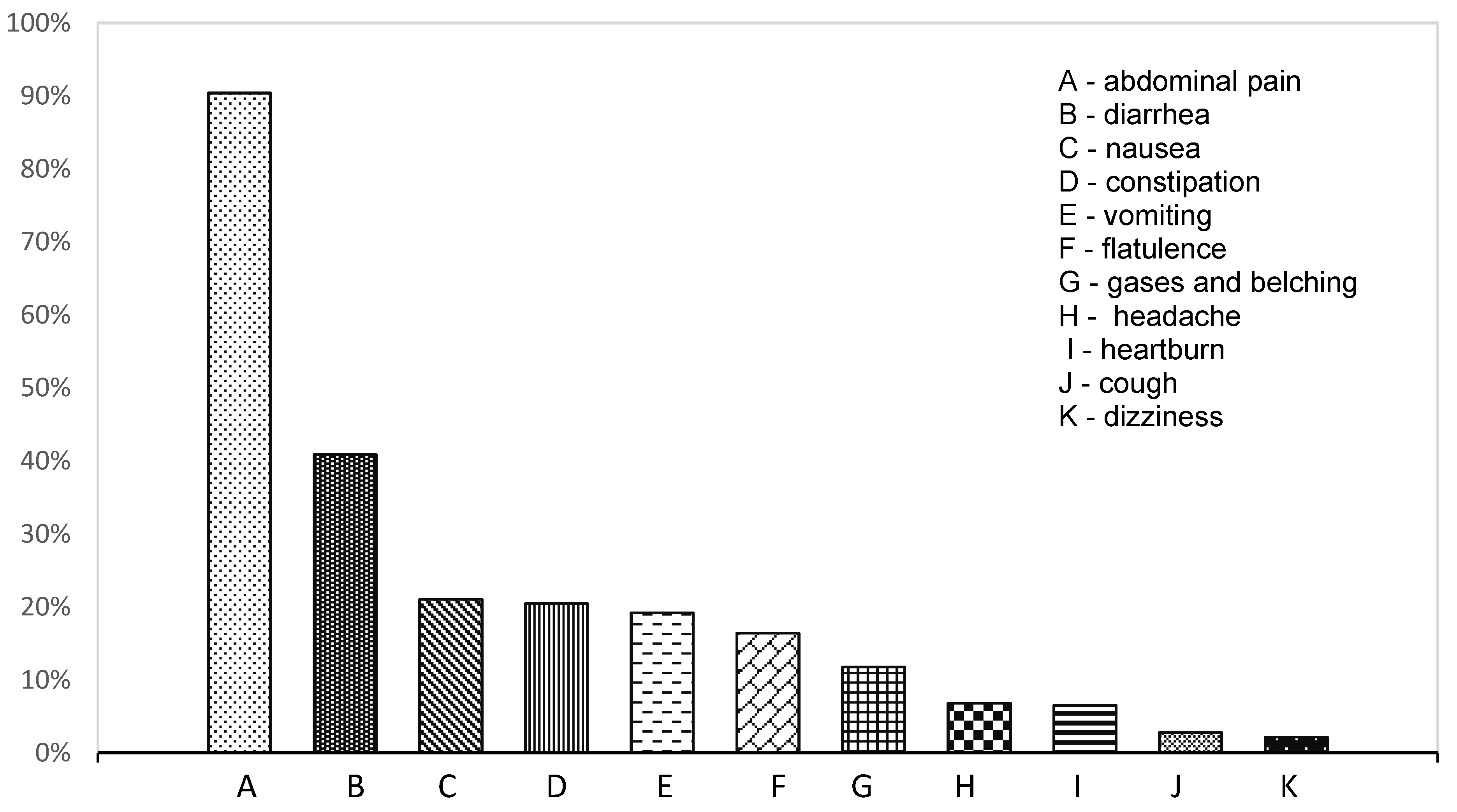
| Scheme | Positive HBT Patients | Negative HBT Patients | p Value |
|---|---|---|---|
| Abdominal pain | 102 (89.47%) | 190 (90.9%) | n.s. |
| Diarrhoea | 46 (40.35%) | 86 (41.15%) | n.s. |
| Nausea | 23 (20.18%) | 45 (21.63%) | n.s. |
| Vomiting | 23 (20.18%) | 39 (18.75%) | n.s. |
| Flatulence | 23 (20.18%) | 30 (14.35%) | n.s. |
| Constipation | 20 (17.54%) | 46 (22.01%) | n.s. |
| Gases and belching | 10 (8.77%) | 28 (13.4%) | n.s. |
| Headache | 6 (5.26%) | 16 (7.66%) | n.s. |
| Heartburn | 5 (4.39%) | 16 (7.66%) | n.s. |
| Cough | 4 (3.51%) | 5 (2.39%) | n.s. |
| Dizziness | 1 (0.88%) | 6 (2.87%) | n.s. |
| Final Diagnosis of FGID | Number of Patients | Positive HBT Patients | p Value |
|---|---|---|---|
| Irritable bowel syndrome | 102 | 35 (34.3%) | n.s. |
| Functional abdominal pain | 100 | 38 (38.0%) | n.s. |
| Functional dyspepsia | 35 | 11 (31.4%) | n.s. |
| Functional constipation | 35 | 9 (25.7%) | n.s. |
| Functional diarrhoea | 33 | 13 (39.4%) | n.s. |
| Cyclic vomiting syndrome | 18 | 8 (44.4%) | n.s. |
| Total | 323 | 114 (35.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwiecień, J.; Hajzler, W.; Kosek, K.; Balcerowicz, S.; Grzanka, D.; Gościniak, W.; Górowska-Kowolik, K. No Correlation between Positive Fructose Hydrogen Breath Test and Clinical Symptoms in Children with Functional Gastrointestinal Disorders: A Retrospective Single-Centre Study. Nutrients 2021, 13, 2891. https://doi.org/10.3390/nu13082891
Kwiecień J, Hajzler W, Kosek K, Balcerowicz S, Grzanka D, Gościniak W, Górowska-Kowolik K. No Correlation between Positive Fructose Hydrogen Breath Test and Clinical Symptoms in Children with Functional Gastrointestinal Disorders: A Retrospective Single-Centre Study. Nutrients. 2021; 13(8):2891. https://doi.org/10.3390/nu13082891
Chicago/Turabian StyleKwiecień, Jarosław, Weronika Hajzler, Klaudia Kosek, Sylwia Balcerowicz, Dominika Grzanka, Weronika Gościniak, and Katarzyna Górowska-Kowolik. 2021. "No Correlation between Positive Fructose Hydrogen Breath Test and Clinical Symptoms in Children with Functional Gastrointestinal Disorders: A Retrospective Single-Centre Study" Nutrients 13, no. 8: 2891. https://doi.org/10.3390/nu13082891
APA StyleKwiecień, J., Hajzler, W., Kosek, K., Balcerowicz, S., Grzanka, D., Gościniak, W., & Górowska-Kowolik, K. (2021). No Correlation between Positive Fructose Hydrogen Breath Test and Clinical Symptoms in Children with Functional Gastrointestinal Disorders: A Retrospective Single-Centre Study. Nutrients, 13(8), 2891. https://doi.org/10.3390/nu13082891