
Smoflipid Is Better Than Lipofundin for Long-Term Neurodevelopmental Outcomes in Preterm Infants


Abstract
:1. Introduction
2. Materials and Methods
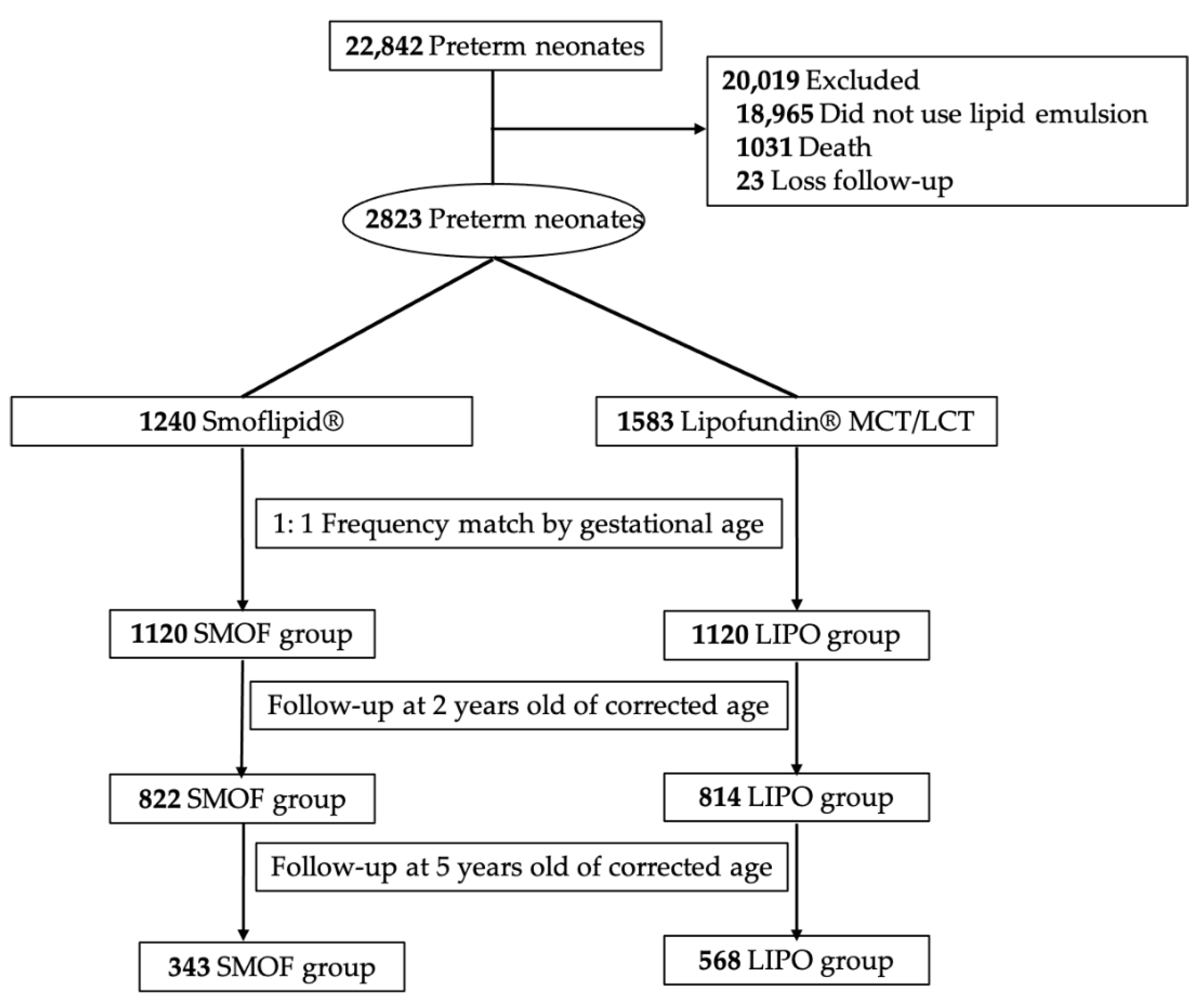
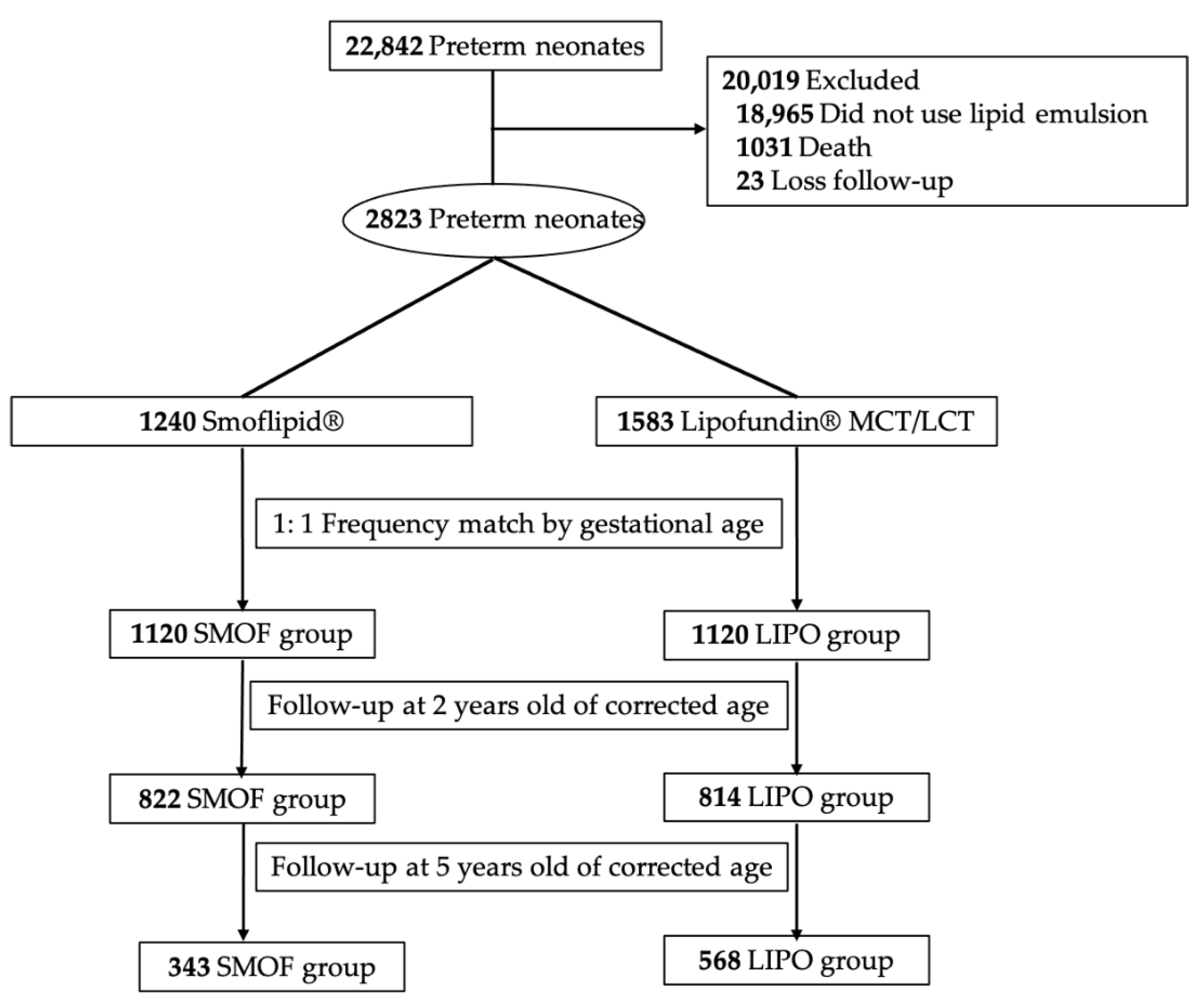
2.1. Data Source
2.2. Nutritional Strategies
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Blencowe, H.; Cousens, S.; Oestergaard, M.Z.; Chou, D.; Moller, A.B.; Narwal, R.; Adler, A.; Vera Garcia, C.; Rohde, S.; Say, L.; et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: A systematic analysis and implications. Lancet 2012, 379, 2162–2172. [Google Scholar] [CrossRef] [Green Version]
- Stoll, B.J.; Hansen, N.I.; Bell, E.F.; Walsh, M.C.; Carlo, W.A.; Shankaran, S.; Laptook, A.R.; Sanchez, P.J.; Van Meurs, K.P.; Wyckoff, M.; et al. Trends in care practices, morbidity, and mortality of extremely preterm neonates, 1993–2012. JAMA 2015, 314, 1039–1051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zsou, G.-Y. Prognosis of Neuromotor Development in Very Low birth WEIGHT Premature Infants in Taiwan—A Ten-Year Change. Available online: https://www.pbf.org.tw/service_02_04 (accessed on 1 June 2021).
- Adams-Chapman, I.; Heyne, R.J.; DeMauro, S.B.; Duncan, A.F.; Hintz, S.R.; Pappas, A.; Vohr, B.R.; McDonald, S.A.; Das, A.; Newman, J.E.; et al. Neurodevelopmental impairment among extremely preterm infants in the neonatal research network. Pediatrics 2018, 141, e20173091. [Google Scholar] [CrossRef] [Green Version]
- Peralta-Carcelen, M.; Carlo, W.A.; Pappas, A.; Vaucher, Y.E.; Yeates, K.O.; Phillips, V.A.; Gustafson, K.E.; Payne, A.H.; Duncan, A.F.; Newman, J.E.; et al. Behavioral Problems and Socioemotional Competence at 18 to 22 Months of Extremely Premature Children. Pediatrics 2017, 139, e20161043. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coviello, C.; Keunen, K.; Kersbergen, K.J.; Groenendaal, F.; Leemans, A.; Peels, B.; Isgum, I.; Viergever, M.A.; de Vries, L.S.; Buonocore, G.; et al. Effects of early nutrition and growth on brain volumes, white matter microstructure, and neurodevelopmental outcome in preterm newborns. Pediatric Res. 2018, 83, 102–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shim, S.Y.; Ahn, H.M.; Cho, S.J.; Park, E.A. Early aggressive nutrition enhances language development in very low-birthweight infants. Pediatrics Int. 2014, 56, 845–850. [Google Scholar] [CrossRef]
- Kamino, D.; Studholme, C.; Liu, M.; Chau, V.; Miller, S.P.; Synnes, A.; Rogers, E.E.; Barkovich, A.J.; Ferriero, D.M.; Brant, R.; et al. Postnatal polyunsaturated fatty acids associated with larger preterm brain tissue volumes and better outcomes. Pediatric Res. 2018, 83, 93–101. [Google Scholar] [CrossRef] [Green Version]
- Rogers, L.K.; Valentine, C.J.; Keim, S.A. DHA supplementation: Current implications in pregnancy and childhood. Pharmacol. Res. 2013, 70, 13–19. [Google Scholar] [CrossRef] [Green Version]
- Weiser, M.J.; Butt, C.M.; Mohajeri, M.H. Docosahexaenoic acid and cognition throughout the lifespan. Nutrients 2016, 8, 99. [Google Scholar] [CrossRef]
- Jensen, C.L.; Maude, M.; Anderson, R.E.; Heird, W.C. Effect of docosahexaenoic acid supplementation of lactating women on the fatty acid composition of breast milk lipids and maternal and infant plasma phospholipids. Am. J. Clin. Nutr. 2000, 71, 292S–299S. [Google Scholar] [CrossRef] [Green Version]
- Brenna, J.T.; Varamini, B.; Jensen, R.G.; Diersen-Schade, D.A.; Boettcher, J.A.; Arterburn, L.M. Docosahexaenoic and arachidonic acid concentrations in human breast milk worldwide. Am. J. Clin. Nutr. 2007, 85, 1457–1464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, T.-C.; Lau, B.-H.; Chen, P.-H.; Wu, L.-T.; Tang, R.-B. Fatty acid composition of Taiwanese human milk. J. Chin. Med. Assoc. 2010, 73, 581–588. [Google Scholar] [CrossRef] [Green Version]
- Vlaardingerbroek, H.; Veldhorst, M.A.; Spronk, S.; van den Akker, C.H.; van Goudoever, J.B. Parenteral lipid administration to very-low-birth-weight infants--early introduction of lipids and use of new lipid emulsions: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2012, 96, 255–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molina, T.L.; Stoll, B.; Mohammad, M.; Mohila, C.A.; Call, L.; Cui, L.; Guthrie, G.; Kunichoff, D.; Lin, S.; Welch-Jernigan, R.; et al. New generation lipid emulsions increase brain DHA and improve body composition, but not short-term neurodevelopment in parenterally-fed preterm piglets. Brain Behav. Immun. 2020, 85, 46–56. [Google Scholar] [CrossRef] [PubMed]
- Janssen, C.I.; Kiliaan, A.J. Long-chain polyunsaturated fatty acids (LCPUFA) from genesis to senescence: The influence of LCPUFA on neural development, aging, and neurodegeneration. Prog. Lipid Res. 2014, 53, 1–17. [Google Scholar] [CrossRef]
- American Academy of Pediatrics Committee on Nutrition: Nutritional needs of low-birth-weight infants. Pediatrics 1985, 75, 976–986.
- Su, B.H. Optimizing nutrition in preterm infants. Pediatrics Neonatol. 2014, 55, 5–13. [Google Scholar] [CrossRef] [Green Version]
- Torgalkar, R.; Shah, J.; Dave, S.; Yang, J.; Ostad, N.; Kotsopoulos, K.; Unger, S.; Kelly, E.; Shah, P.S. Fish oil-containing multicomponent lipid emulsion vs soy-based lipid emulsion and neurodevelopmental outcomes of children born <29 weeks’ gestation. J. Perinatol. 2020, 40, 1712–1718. [Google Scholar] [PubMed]
- Keim, S.A.; Gracious, B.; Boone, K.M.; Klebanoff, M.A.; Rogers, L.K.; Rausch, J.; Coury, D.L.; Sheppard, K.W.; Husk, J.; Rhoda, D.A. omega-3 and omega-6 fatty acid supplementation may reduce autism symptoms based on parent report in preterm toddlers. J. Nutr. 2018, 148, 227–235. [Google Scholar] [CrossRef]
- Clandinin, M.T.; Chappell, J.E.; Leong, S.; Heim, T.; Swyer, P.R.; Chance, G.W. Intrauterine fatty acid accretion rates in human brain: Implications for fatty acid requirements. Early Hum. Dev. 1980, 4, 121–129. [Google Scholar] [CrossRef]
- Farooqui, A.A. Beneficial Effects of Fish Oil on Human Brain; Springer: New York, NY, USA, 2009. [Google Scholar]
- Tanaka, K.; Farooqui, A.A.; Siddiqi, N.J.; Alhomida, A.S.; Ong, W.Y. Effects of docosahexaenoic acid on neurotransmission. Biomol. Ther. 2012, 20, 152–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayurasakorn, K.; Williams, J.J.; Ten, V.S.; Deckelbaum, R.J. Docosahexaenoic acid: Brain accretion and roles in neuroprotection after brain hypoxia and ischemia. Curr. Opin. Clin. Nutr. Metab. Care 2011, 14, 158–167. [Google Scholar] [CrossRef] [Green Version]
- Collins, C.T.; Makrides, M.; McPhee, A.J.; Sullivan, T.R.; Davis, P.G.; Thio, M.; Simmer, K.; Rajadurai, V.S.; Travadi, J.; Berry, M.J.; et al. Docosahexaenoic acid and bronchopulmonary dysplasia in preterm infants. N. Engl. J. Med. 2017, 376, 1245–1255. [Google Scholar] [CrossRef] [PubMed]
- Marc, I.; Piedboeuf, B.; Lacaze-Masmonteil, T.; Fraser, W.; Mâsse, B.; Mohamed, I.; Qureshi, M.; Afifi, J.; Lemyre, B.; Caouette, G.; et al. Effect of maternal docosahexaenoic acid supplementation on bronchopulmonary dysplasia-free survival in breastfed preterm infants: A randomized clinical trial. JAMA 2020, 324, 157–167. [Google Scholar] [CrossRef]
- Bhutta, A.T.; Cleves, M.A.; Casey, P.H.; Cradock, M.M.; Anand, K.J. Cognitive and behavioral outcomes of school-aged children who were born preterm: A meta-analysis. JAMA 2002, 288, 728–737. [Google Scholar] [CrossRef] [PubMed]
- Thomason, M.E.; Scheinost, D.; Manning, J.H.; Grove, L.E.; Hect, J.; Marshall, N.; Hernandez-Andrade, E.; Berman, S.; Pappas, A.; Yeo, L.; et al. Weak functional connectivity in the human fetal brain prior to preterm birth. Sci. Rep. 2017, 7, 39286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sciberras, E.; Mulraney, M.; Silva, D.; Coghill, D. Prenatal risk factors and the etiology of ADHD-review of existing evidence. Curr Psychiatry Rep. 2017, 19, 1. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.W.; Wang, S.T.; Wang, L.W.; Kao, Y.C.; Chu, C.L.; Wu, C.C.; Hsieh, Y.T.; Chiang, C.H.; Huang, C.C. Behavioral characteristics of autism spectrum disorder in very preterm birth children. Mol. Autism 2019, 10, 32. [Google Scholar] [CrossRef] [Green Version]
- Agrawal, S.; Rao, S.C.; Bulsara, M.K.; Patole, S.K. Prevalence of autism spectrum disorder in preterm infants: A meta-analysis. Pediatrics 2018, 142, e20180134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blumberg, S.J.; Bramlett, M.D.; Kogan, M.D.; Schieve, L.A.; Jones, J.R.; Lu, M.C. Changes in prevalence of parent-reported autism spectrum disorder in school-aged U.S. children: 2007 to 2011–2012. Natl. Health Stat. Rep. 2013, 65, 1–11. [Google Scholar]
- Larsson, H.; Chang, Z.; D’Onofrio, B.M.; Lichtenstein, P. The heritability of clinically diagnosed attention deficit hyperactivity disorder across the lifespan. Psychol. Med. 2013, 44, 2223–2229. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Fatty Acids | SMOFlipid®, 0.2 g/mL (%) | Lipofundin® MCT/LCT, 0.2 g/mL (%) |
|---|---|---|
| Oleic acid | 23 to 35 | - |
| Linoleic acid | 14 to 25 | 24 to 29 |
| α-linolenic acid | 1.5 to 3.5 | 2.5 to 5.5 |
| Eicosapentaenoic acid | 1 to 3.5 | - |
| Docosahexaenoic acid | 1 to 3.5 | - |
| Medium-chain triglycerides | 30 | 50 |
| SMOF Group (n = 1120) | LIPO Group (n = 1120) | p Value | |
|---|---|---|---|
| Gestational age, mean (SD), week | 32.15 (2.38) | 32.15 (2.38) | 1 |
| Gender, no. (%) | |||
| Female | 521 (46.5) | 503 (44.9) | 0.42 |
| Male | 599 (53.4) | 617 (55.1) | |
| Birth length, mean (SD), cm | 41.4 (4.07) | 40.8 (4.26) | 0.0006 |
| Birth weight, mean (SD), g | 1759.8 (514.6) | 1764.9 (558.7) | 0.82 |
| Body temperature, mean (SD), ℃ | 36.5 (0.58) | 36.4 90.67) | 0.0040 |
| Head circumference, mean (SD), cm | 29.6 (2.49) | 29.5 (2.73) | 0.47 |
| AS1, mean (SD) | 7.2 (1.74) | 6.5 (2.01) | <0.0001 |
| AS5, mean (SD) | 8.7 (1.28) | 8.2 (1.52) | <0.0001 |
| Duration of lipid, mean (SD), day | 17.1 (21.18) | 15.2 (15.58) | 0.05 |
| Comorbidities, no. (%) | |||
| Meningitis | 2 (0.17) | 6 (0.53) | 0.29 |
| Perinatal asphyxia | 46 (4.10) | 44 (3.93) | 0.83 |
| Hydrocephalus | 16 (1.42) | 23 (2.05) | 0.33 |
| Intraventricular hemorrhage | 108 (9.64) | 97 (8.66) | 0.38 |
| Periventricular leukomalacia | 11(0.98) | 17 (1.51) | 0.34 |
| Patent ductus arteriosus | 88 (7.85) | 186 (16.60) | <0.0001 |
| PDA ligation | 31 (2.76) | 54 (4.82) | 0.0149 |
| Retinopathy of prematurity | 308 (27.50) | 394 (35.17) | 0.0003 |
| Surgical management for ROP | 16 (1.42) | 13 (1.16) | 0.58 |
| Bronchopulmonary dysplasia | 133 (11.87) | 82 (7.32) | 0.0002 |
| Necrotizing enterocolitis | 18 (1.60) | 7 (0.62) | 0.0269 |
| No (%) | SMOF Group (n = 822) | LIPO Group (n = 814) | Logistic Regression * | ||
|---|---|---|---|---|---|
| OR | 95% CI | p Value | |||
| Epilepsy | 26 (3.2) | 45 (5.5) | 2.111 | 1.144–3.895 | 0.0168 |
| Cerebral palsy | 15 (1.8) | 33 (4.0) | 2.444 | 1.166–5.121 | 0.0179 |
| Language delay | 51 (6.2) | 67 (8.2) | 1.291 | 0.835–1.995 | 0.25 |
| Developmental delay | 2016 (12.7) | 153 (18.8) | 1.408 | 1.027–1.931 | 0.0335 |
| ADHD | 20 (2.4) | 68 (8.3) | 3.063 | 1.732–5.416 | 0.0001 |
| Autism | 2 (0.2) | 2 (0.2) | 0.615 | 0.053–7.153 | 0.70 |
| Birth weight < 1500 g | 302 (36.7) | 295 (36.2) | |||
| Epilepsy | 11 (3.6) | 20 (6.8) | 1.629 | 0.638–4.158 | 0.31 |
| Cerebral palsy | 6 (2.0) | 18 (6.1) | 2.681 | 0.885–8.121 | 0.0812 |
| Language delay | 35 (11.6) | 33 (11.2) | 0.928 | 0.505–1.705 | 0.81 |
| Developmental delay | 65 (21.5) | 90 (30.5) | 1.427 | 0.918–2.218 | 0.11 |
| ADHD | 11 (3.6) | 37 (12.5) | 4.189 | 1.874–9.365 | 0.0005 |
| Autism | 0 (0) | 1 (0.3) | 0.99 | ||
| Birth weight ≥ 1500 g | 520 (63.3) | 519 (63.8) | |||
| Epilepsy | 15 (2.9) | 25 (4.8) | 2.612 | 1.131–6.030 | 0.0245 |
| Cerebral palsy | 9 (1.7) | 14 (2.7) | 2.061 | 0.758–5.604 | 0.16 |
| Language delay | 16 (3.0) | 33 (6.4) | 2.252 | 1.135–4.467 | 0.0202 |
| Developmental delay | 40 (7.7) | 62 (12.0) | 1.493 | 0.926–2.405 | 0.10 |
| ADHD | 9 (1.7) | 31 (6.0) | 2.481 | 1.075–5.724 | 0.0332 |
| Autism | 2 (0.4) | 1 (0.2) | 0.000 | - | 0.99 |
| No. (%) | SMOF Group (n = 343) | LIPO Group (n = 568) | Logistic Regression * | ||
|---|---|---|---|---|---|
| OR | 95% CI | p Value | |||
| Epilepsy | 12 (3.5) | 38 (6.7) | 2.635 | 1.114–6.232 | 0.0274 |
| Cerebral palsy | 14 (4.0) | 40 (7.0) | 1.562 | 0.727–3.358 | 0.25 |
| Language delay | 31 (9.0) | 87 (15.3) | 1.706 | 1.040–2.799 | 0.0344 |
| Developmental delay | 65 (18.9) | 134 (23.6) | 1.101 | 0.746–1.625 | 0.63 |
| ADHD | 17 (5.0) | 77 (13.5) | 2.473 | 1.347–4.543 | 0.0035 |
| Autism | 2 (0.6) | 35 (6.1) | 7.055 | 1.581–31.486 | 0.0105 |
| Birth weight < 1500 g | 113 (32.9) | 203 (35.7) | |||
| Epilepsy | 6 (5.3) | 18 (8.8) | 1.765 | 0.584–5.335 | 0.31 |
| Cerebral palsy | 5 (4.4) | 26 (12.8) | 1.606 | 0.503–5.126 | 0.42 |
| Language delay | 17 (15.0) | 40 (19.7) | 1.360 | 0.674–2.741 | 0.39 |
| Developmental delay | 35 (30.9) | 69 (34.0) | 0.948 | 0.535–1.680 | 0.86 |
| ADHD | 9 (7.9) | 36 (17.7) | 2.912 | 1.209–7.012 | 0.0172 |
| Autism | 1 (0.8) | 21 (3.7) | 12.793 | 1.595–102.581 | 0.0164 |
| Birth weight ≥ 1500 g | 230 (67.0) | 365 (64.3) | |||
| Epilepsy | 6 (2.6) | 20 (5.5) | 4.481 | 0.963–20.847 | 0.06 |
| Cerebral palsy | 9 (3.9) | 18 (4.9) | 1.412 | 0.504–3.959 | 0.51 |
| Language delay | 14 (6.1) | 46 (12.6) | 2.308 | 1.105–4.820 | 0.0260 |
| Developmental delay | 30 (13.0) | 64 (17.5) | 1.306 | 0.751–2.272 | 0.34 |
| ADHD | 8 (3.4) | 41 (11.2) | 2.268 | 0.952–5.403 | 0.06 |
| Autism | 1 (0.4) | 14 (3.9) | 2.351 | 0.244–22.679 | 0.46 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, I.-L.; Hung, C.-H.; Huang, H.-C. Smoflipid Is Better Than Lipofundin for Long-Term Neurodevelopmental Outcomes in Preterm Infants. Nutrients 2021, 13, 2548. https://doi.org/10.3390/nu13082548
Chen I-L, Hung C-H, Huang H-C. Smoflipid Is Better Than Lipofundin for Long-Term Neurodevelopmental Outcomes in Preterm Infants. Nutrients. 2021; 13(8):2548. https://doi.org/10.3390/nu13082548
Chicago/Turabian StyleChen, I-Lun, Chih-Hsing Hung, and Hsin-Chun Huang. 2021. "Smoflipid Is Better Than Lipofundin for Long-Term Neurodevelopmental Outcomes in Preterm Infants" Nutrients 13, no. 8: 2548. https://doi.org/10.3390/nu13082548
APA StyleChen, I.-L., Hung, C.-H., & Huang, H.-C. (2021). Smoflipid Is Better Than Lipofundin for Long-Term Neurodevelopmental Outcomes in Preterm Infants. Nutrients, 13(8), 2548. https://doi.org/10.3390/nu13082548