
Prevalence and Determinants of the Co-Occurrence of Overweight or Obesity and Micronutrient Deficiencies among Adults in the Philippines: Results from a National Representative Survey


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Study Population
2.2. Sociodemographic Characteristics and Health-Related Behavior Measurement
2.3. Anthropometric and Biochemical Assessments
2.4. Double Burden of Malnutrition Definitions
2.5. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
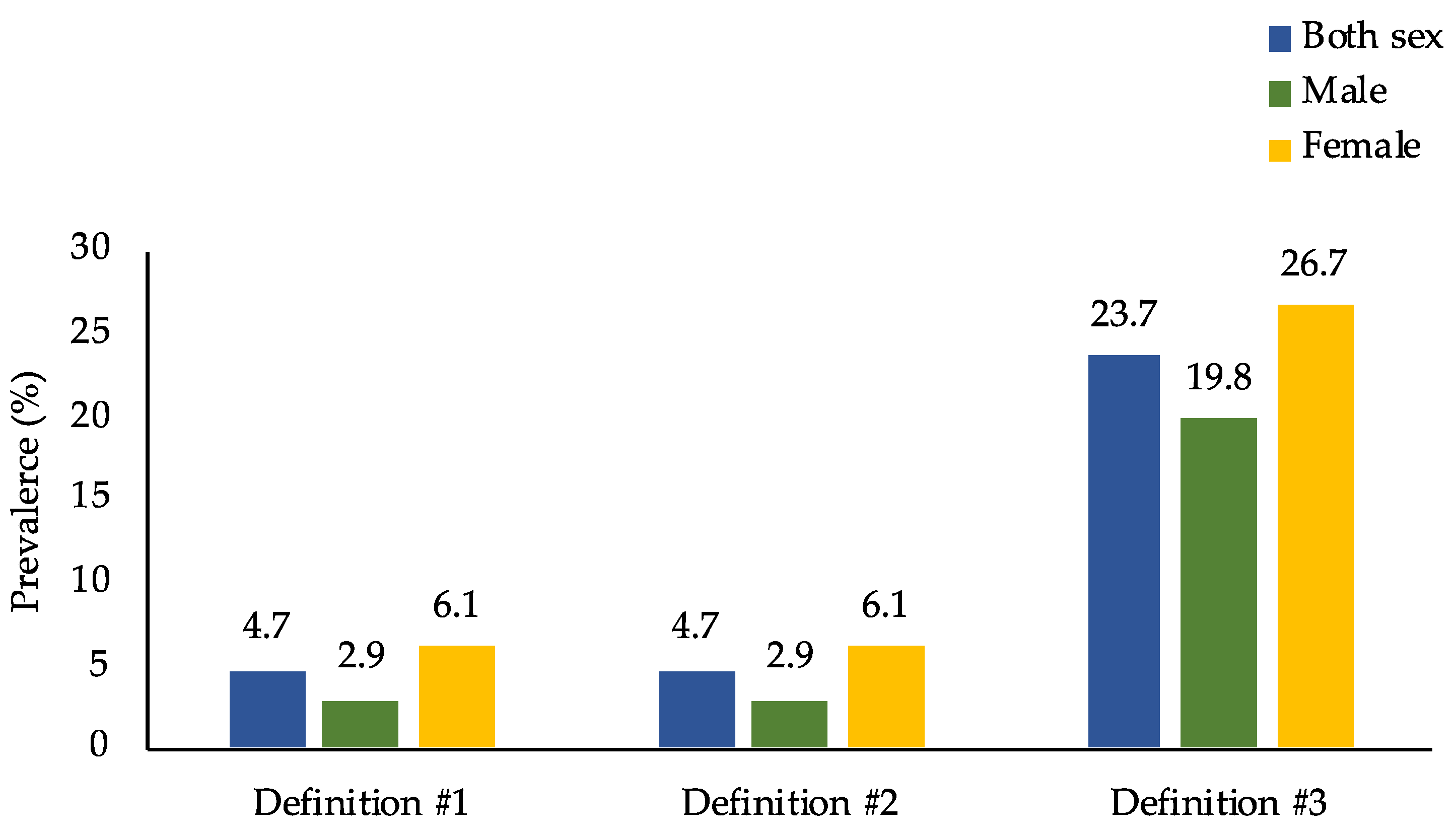
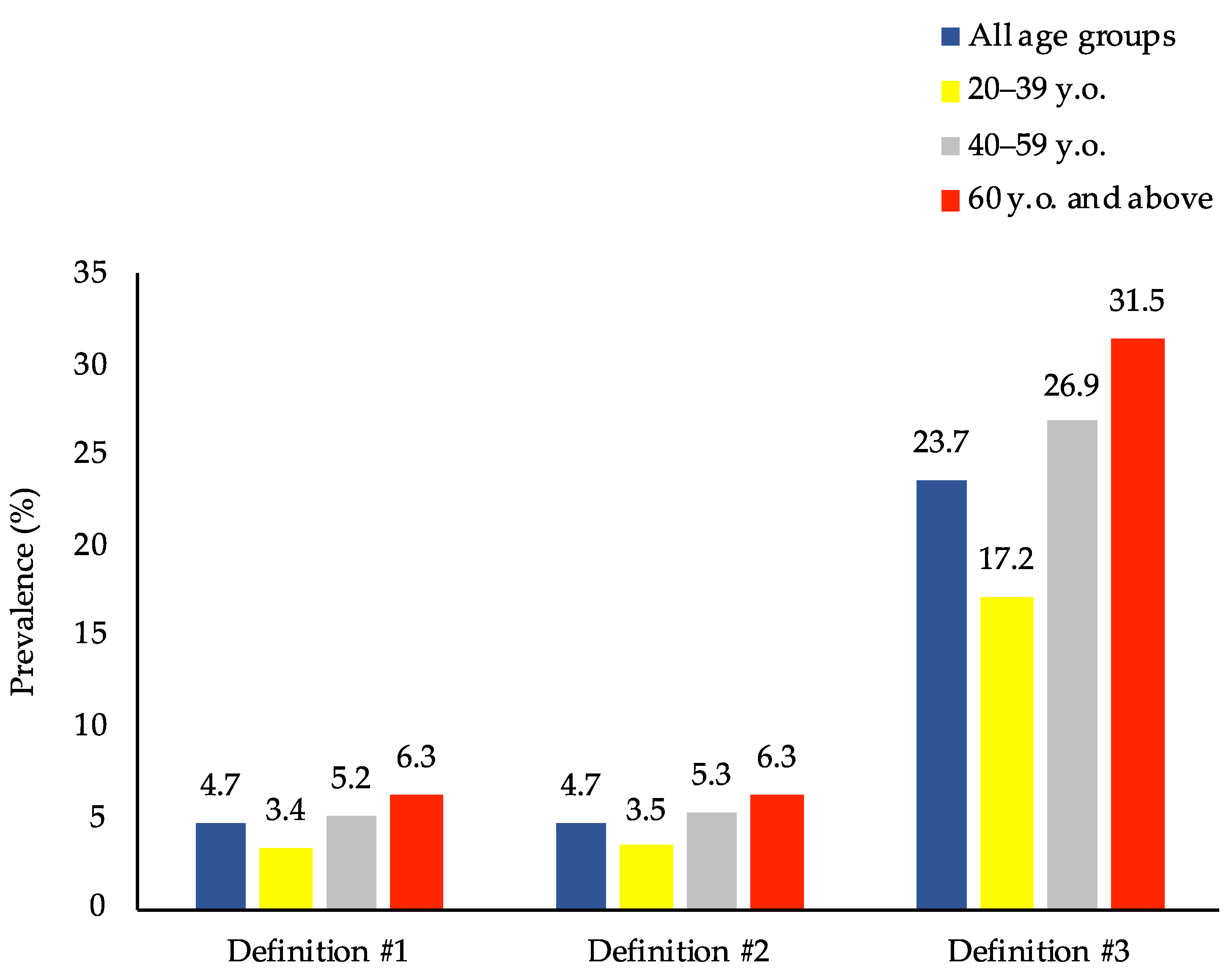
3.2. Prevalence of the Double Burden of Malnutrition
3.3. Factors Associated with the Double Burden of Malnutrition
3.4. Determinants of the Double Burden of Malnutrition
4. Discussion
4.1. Main Findings
4.2. Interpretations
4.3. Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Popkin, B.M.; Corvalan, C.; Grummer-Strawn, L.M. Dynamics of the double burden of malnutrition and the changing nutrition reality. Lancet 2020, 395, 65–74. [Google Scholar] [CrossRef]
- World Health Organization. The Double Burden of Malnutrition Policy Brief; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Nugent, R.; Levin, C.; Hale, J.; Hutchinson, B. Economic effects of the double burden of malnutrition. Lancet 2020, 395, 156–164. [Google Scholar] [CrossRef]
- Wells, J.C.; Sawaya, A.L.; Wibaek, R.; Mwangome, M.; Poullas, M.S.; Yajnik, C.S.; Demaio, A. The double burden of malnutrition: Aetiological pathways and consequences for health. Lancet 2020, 395, 75–88. [Google Scholar] [CrossRef]
- Rhodes, E.C.; Suchdev, P.S.; Veknat Narayan, K.V.; Cunningham, S.; Weber, M.B.; Tripp, K.; Mapango, C.; Ramakrishnan, U.; Hennink, M.; Williams, A.M. The co-occurrence of overweight and micronutrient deficiencies or anemia among women of reproductive age in Malawi. J. Nutr. 2020, 150, 1554–1565. [Google Scholar] [CrossRef] [PubMed]
- Fongar, A.; Godecke, T.; Qaim, M. Various forms of double burden of malnutrition problems exist in rural Kenya. BMC Public Health 2019, 19, 1543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Q.; Wang, L.; Jiang, H.; Wang, H.; Zhang, B.; Zhang, J.; Jia, X.; Wang, Z. Intra-individual double burden of malnutrition among adults in China: Evidence from the China Health and Nutrition Survey 2015. Nutrients 2020, 12, 2811. [Google Scholar] [CrossRef] [PubMed]
- Little, M.; Humphries, S.; Dodd, W.; Patel, K.; Dewey, C. Sociodemographic patterning of the individual-level double burden of malnutrition in a rural population in South India: A cross-sectional study. BMC Public Health 2020, 20, 675. [Google Scholar] [CrossRef]
- Traissac, P.; El Ati, J.; Gartner, A.; Ben Gharbia, H.; Delpeuch, F. Gender inequalities in excess adiposity and anaemia combine in a large double burden of malnutrition gap detrimental to women in an urban area in North Africa. Public Health Nutr. 2016, 19, 1428–1437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, E.A.; Finkelstein, J.L.; Brannon, P.M.; Bonam, W.; Russell, D.G.; Glesby, M.J.; Mehta, S. Nutritional assessment among adult patients with suspected or confirmed active tuberculosis disease in rural India. PLoS ONE 2020, 15, e0233306. [Google Scholar] [CrossRef]
- Zeba, A.N.; Delisle, H.F.; Renier, G. Dietary patterns and physical inactivity, two contributing factors to the double burden of malnutrition among adults in Burkina Faso, West Africa. J. Nutr. Sci. 2014, 3, e50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Department of Science and Technology-Food; Nutrition Research Institute. eNutrition, Facts and Figure 2013 National Nutrition Survey. Available online: https://www.fnri.dost.gov.ph/index.php/19-nutrition-statistic/175-national-nutrition-survey#facts-and-figures (accessed on 3 September 2020).
- Barcenas, M.L. The development of the 2003 Master Sample (MS) for Philippine Household Surveys. In Proceedings of the 9th National Nutrition on Statistics, Manila, Philippines, 4–5 October 2004. [Google Scholar]
- Patalen, C.F.; Ikeda, N.; Angeles-Agdeppa, I.; Vargas, M.B.; Nishi, N.; Duante, C.A.; Capanzana, M.V. Data Resource Profile: The Philippine National Nutrition Survey (NNS). Int. J. Epidemiol. 2020, 49, 742–743f. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO STEPS Surveillance Manual: The WHO STEPwise Approach to Chronic Disease Risk Factor Surveillance; WHO: Geneva, Switzerland, 2005. [Google Scholar]
- World Health Organization. Global Status Report on Alcohol and Health 2018; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- World Health Organization. WHO Technical Report Series on Obesity: Preventing and Managing the Global Epidemic; WHO: Geneva, Switzerland, 2000. [Google Scholar]
- International Committee for Standardization in Haematology. International Committee for Standardization in Haematology: Protocol for type testing equipment and apparatus used for haematological analysis. J. Clin. Pathol. 1978, 31, 275–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization; United Nations Children’s Fund; United Nations University. Iron Deficiency Anaemia: Assessment, Prevention and Control, a Guide for Programme Managers; WHO: Geneva, Switzerland, 2001. [Google Scholar]
- Furr, H.C.; Tanmihardjo, S.A.; Olson, J.A. Training Manual for Assessing Vitamin A Status by Use of the Modified Relative Dose Response and Relative Dose Response Assays; United States Agency for International Development: Washington, DC, USA, 1992. [Google Scholar]
- Sommer, A. Vitamin A Deficiency and Its Consequences: A Field Guide to Detection and Control, 3rd ed.; World Health Organization: Geneva, Switzerland, 1995; pp. 19–33. [Google Scholar]
- Dunn, J.T.; Crutchfield, H.E.; Gutekunst, R.; Dunn, A.D. Methods for Measuring Iodine in Urine; International Council for Control of Iodine Deficiency Disorders (ICCIDD): Wageningen, The Netherlands, 1993. [Google Scholar]
- World Health Organization. Assessment of Iodine Deficiency Disorders and Monitoring Their Elimination: A Guide for Programme Managers; WHO: Geneva, Switzerland, 2001. [Google Scholar]
- Barth-Jaeggi, T.; Zandberg, L.; Bahruddinov, M.; Kiefer, S.; Rahmarulloev, S.; Wyss, K. Nutritional status of Tajik children and women: Transition towards a double burden of malnutrition. Matern. Child Nutr. 2020, 16, e12886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosu, W.K. An overview of the nutrition transition in West Africa: Implications for non-communicable diseases. Proc. Nutr. Soc. 2015, 74, 466–477. [Google Scholar] [CrossRef] [PubMed]
- Lipoeto, N.I.; Lin, K.G.; Angeles-Agdeppa, I. Food consumption patterns and nutrition transition in South-East Asia. Public Health Nutr. 2013, 16, 1637–1643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amarya, S.; Singh, K.; Sabharwal, M. Changes during aging and their association with malnutrition. J. Clin. Gerontol. Geriatr. 2015, 6, 78–84. [Google Scholar] [CrossRef] [Green Version]
- Angeles-Agdeppa, I.; Sun, Y.; Denney, L.; Tanda, K.V.; Octavio, R.A.D.; Carriquiry, A.; Capanzana, M.V. Food sources, energy and nutrient intakes of adults: 2013 Philippines National Nutrition Survey. Nutr. J. 2019, 18, 59. [Google Scholar] [CrossRef] [PubMed]
- Teachman, J. Body weight, marital status, and changes in marital status. J. Fam. Issues 2016, 37, 74–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuovinen, E.L.; Saarni, S.E.; Männistö, S.; Borodulin, K.; Patja, K.; Kinnunen, T.H.; Kaprio, J.; Korhonen, T. Smoking status and abdominal obesity among normal and overweight/obese adults: Population-based FINRISK study. Prev. Med. Rep. 2016, 4, 324–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, A.M.; Guo, J.; Addo, O.Y.; Ismaily, S.; Namaste, S.M.L.; Oaks, B.M.; Rohner, F.; Suchdev, P.S.; Young, M.F.; Flores-Ayala, R.; et al. Intraindividual double burden of overweight or obesity and micronutrient deficiencies or anemia among women of reproductive age in 17 population-based surveys. Am. J. Clin. Nutr. 2020, 112, 468S–477S. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total | Male | Female | p-Value |
|---|---|---|---|---|
| (n = 17,010) | (n = 8536) | (n = 8474) | ||
| Sex | - | |||
| Male | 50.1 | - | - | |
| Female | 49.9 | - | - | |
| Age group (years) | <0.001 | |||
| 20–39 | 46.0 | 48.8 | 43.2 | |
| 40–59 | 38.8 | 37.4 | 40.1 | |
| ≥60 | 15.2 | 13.8 | 16.7 | |
| Educational attainment 2 | 0.001 | |||
| Elementary and lower | 31.9 | 33.7 | 30.0 | |
| High school | 38.3 | 38.5 | 38.1 | |
| College and higher | 29.8 | 27.8 | 31.9 | |
| Marital status | <0.001 | |||
| Single | 23.3 | 26.5 | 20.1 | |
| Married | 67.1 | 68.3 | 65.8 | |
| Others | 9.6 | 5.2 | 14.0 | |
| Employment status | <0.001 | |||
| Employed | 60.2 | 77.2 | 43.2 | |
| Unemployed | 39.8 | 22.8 | 56.8 | |
| Household size | 0.309 | |||
| 1–3 | 33.1 | 32.9 | 33.4 | |
| 4–6 | 44.5 | 44.4 | 44.7 | |
| ≥7 | 22.3 | 22.8 | 21.9 | |
| Wealth quintile | <0.001 | |||
| Poorest | 17.3 | 19.1 | 15.6 | |
| Poor | 19.3 | 20.3 | 18.3 | |
| Middle | 20.6 | 20.7 | 20.4 | |
| Rich | 21.2 | 20.3 | 22.1 | |
| Richest | 21.6 | 19.6 | 23.6 | |
| Current smoker 2 | <0.001 | |||
| Yes | 27.2 | 46.2 | 8.2 | |
| No | 72.8 | 53.8 | 91.8 | |
| Current alcohol drinker 2 | <0.001 | |||
| Yes | 51.6 | 72.7 | 30.5 | |
| No | 48.4 | 27.3 | 69.5 | |
| Physical activity 2 | <0.001 | |||
| Low | 43.3 | 35.4 | 51.2 | |
| High | 56.7 | 64.6 | 48.8 |
| Variables | Total | Male | Female | p-Value |
|---|---|---|---|---|
| (n = 17,010) | (n = 8536) | (n = 8474) | ||
| Body mass index | <0.001 | |||
| Underweight | 11.2 | 10.6 | 11.8 | |
| Normal weight | 59.3 | 63.2 | 55.3 | |
| Overweight | 23.4 | 21.5 | 25.3 | |
| Obese | 6.2 | 4.6 | 7.7 | |
| Anemia | 0.002 | |||
| Yes | 6.5 | 5.2 | 7.7 | |
| No | 93.5 | 94.8 | 92.3 | |
| Vitamin A deficiency | 0.527 | |||
| Yes | 0.1 | 0.1 | 0.1 | |
| No | 99.9 | 99.9 | 99.9 | |
| Iodine insufficiency | 0.001 | |||
| Yes | 23.8 | 21.5 | 26.2 | |
| No | 76.2 | 78.5 | 73.8 | |
| Co-occurrence of Ow/Ob and micronutrient deficiencies | ||||
| #1. Ow/Ob + Ane 2 | 0.001 | |||
| Yes | 1.4 | 0.8 | 2.0 | |
| No | 98.6 | 99.2 | 98.0 | |
| #2. Ow/Ob + Ane/VAD 3 | 0.001 | |||
| Yes | 1.4 | 0.8 | 2.0 | |
| No | 98.6 | 99.2 | 98.0 | |
| #3. Ow/Ob + Ane/VAD/Iod-Ins 4 | <0.001 | |||
| Yes | 7.0 | 5.2 | 8.8 | |
| No | 93.0 | 94.8 | 91.2 |
| Characteristics | Definition #1 Ow/Ob + Ane 2 | Definition #3 Ow/Ob + Ane/VAD/Iod-Ins 3 | ||
|---|---|---|---|---|
| (n = 237) | p-Value | (n = 1241) | p-Value | |
| Sex | 0.001 | <0.001 | ||
| Male | 0.8 | 5.2 | ||
| Female | 2.0 | 8.8 | ||
| Age group (years) | 0.002 | <0.001 | ||
| 20–39 | 0.9 | 4.4 | ||
| 40–59 | 1.9 | 9.8 | ||
| ≥60 | 1.6 | 7.9 | ||
| Educational attainment 4,5 | 0.100 | 0.149 | ||
| Elementary and lower | 1.2 | 6.3 | ||
| High school | 1.7 | 7.4 | ||
| College and higher | 1.2 | 7.2 | ||
| Marital status | 0.001 | <0.001 | ||
| Single | 0.4 | 3.1 | ||
| Married | 1.6 | 8.1 | ||
| Others | 1.9 | 8.3 | ||
| Employment status | 0.023 | 0.068 | ||
| Employed | 1.1 | 6.6 | ||
| Unemployed | 1.7 | 7.6 | ||
| Household size | 0.327 | 0.052 | ||
| 1–3 | 1.6 | 7.8 | ||
| 4–6 | 1.3 | 6.7 | ||
| ≥7 | 1.2 | 6.3 | ||
| Wealth quintile | 0.015 | 0.001 | ||
| Poorest | 0.7 | 4.7 | ||
| Poor | 1.2 | 6.6 | ||
| Middle | 1.3 | 7.1 | ||
| Rich | 1.8 | 7.6 | ||
| Richest | 1.8 | 8.4 | ||
| Current smoker 4,5 | 0.007 | 0.001 | ||
| Yes | 0.7 | 4.1 | ||
| No | 1.6 | 8.1 | ||
| Current alcohol drinker 4,5 | 0.006 | 0.009 | ||
| Yes | 0.9 | 6.1 | ||
| No | 1.9 | 8.0 | ||
| Physical activity 4,5 | 0.140 | 0.629 | ||
| Low | 1.6 | 6.9 | ||
| High | 1.3 | 7.1 | ||
| Variables | Definition #1 2 | Definition #3 3 | ||||
|---|---|---|---|---|---|---|
| (n = 237) | (n = 1241) | |||||
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Female (ref = male) | 1.77 | 1.18–2.67 | 0.041 | 1.47 | 1.23–1.75 | 0.008 |
| Age group (ref = 20–39) | ||||||
| 40–59 | 1.84 | 1.28–2.67 | 0.022 | 2.11 | 1.77–2.51 | 0.000 |
| ≥60 | 1.34 | 0.84–2.14 | 0.280 | 1.70 | 1.34–2.17 | 0.007 |
| Educational attainment | ||||||
| Elementary and lower (ref) | ||||||
| High school | 1.38 | 0.97–1.96 | 0.135 | 1.33 | 1.11–1.58 | 0.026 |
| College and higher | 0.94 | 0.60–1.46 | 0.782 | 1.31 | 1.06–1.63 | 0.058 |
| Marital status (ref = single) | ||||||
| Married | 2.64 | 1.44–4.85 | 0.026 | 2.10 | 1.65–2.67 | 0.002 |
| Others | 2.59 | 1.30–5.17 | 0.043 | 1.95 | 1.46–2.60 | 0.006 |
| Unemployed (ref = employed) | 0.81 | 0.58–1.13 | 0.268 | 0.95 | 0.81–1.10 | 0.496 |
| Household size (ref = 1–3) | ||||||
| 4–6 | 0.85 | 0.62–1.16 | 0.347 | 0.81 | 0.69–0.94 | 0.043 |
| ≥7 | 0.80 | 0.54–1.20 | 0.332 | 0.87 | 0.72–1.06 | 0.223 |
| Wealth quintile (ref = poorest) | ||||||
| Poor | 1.57 | 0.90–2.72 | 0.172 | 1.45 | 1.13–1.86 | 0.031 |
| Middle | 1.64 | 0.93–2.90 | 0.149 | 1.50 | 1.16–1.95 | 0.029 |
| Rich | 2.52 | 1.52–4.17 | 0.016 | 1.63 | 1.25–2.13 | 0.015 |
| Richest | 2.67 | 1.54–4.62 | 0.017 | 1.81 | 1.36–2.40 | 0.009 |
| Current smoker (ref = yes) | ||||||
| No | 1.36 | 0.85–2.18 | 0.259 | 1.62 | 1.28–2.05 | 0.010 |
| Current alcohol drinker (ref = yes) | ||||||
| No | 1.33 | 0.94–1.88 | 0.165 | 0.93 | 0.80–1.08 | 0.368 |
| Physical activity (ref = low) | ||||||
| High | 0.93 | 0.70–1.24 | 0.655 | 1.14 | 0.99–1.32 | 0.126 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Juras, A.R.; Hsu, W.-C.; Hu, S.C. Prevalence and Determinants of the Co-Occurrence of Overweight or Obesity and Micronutrient Deficiencies among Adults in the Philippines: Results from a National Representative Survey. Nutrients 2021, 13, 2339. https://doi.org/10.3390/nu13072339
de Juras AR, Hsu W-C, Hu SC. Prevalence and Determinants of the Co-Occurrence of Overweight or Obesity and Micronutrient Deficiencies among Adults in the Philippines: Results from a National Representative Survey. Nutrients. 2021; 13(7):2339. https://doi.org/10.3390/nu13072339
Chicago/Turabian Stylede Juras, Aileen R., Wan-Chen Hsu, and Susan C. Hu. 2021. "Prevalence and Determinants of the Co-Occurrence of Overweight or Obesity and Micronutrient Deficiencies among Adults in the Philippines: Results from a National Representative Survey" Nutrients 13, no. 7: 2339. https://doi.org/10.3390/nu13072339
APA Stylede Juras, A. R., Hsu, W.-C., & Hu, S. C. (2021). Prevalence and Determinants of the Co-Occurrence of Overweight or Obesity and Micronutrient Deficiencies among Adults in the Philippines: Results from a National Representative Survey. Nutrients, 13(7), 2339. https://doi.org/10.3390/nu13072339