
Involving Parents in Promoting Healthy Energy Balance-Related Behaviors in Preschoolers: A Mixed Methods Impact and Process Evaluation of SuperFIT

 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. SuperFIT Intervention Approach
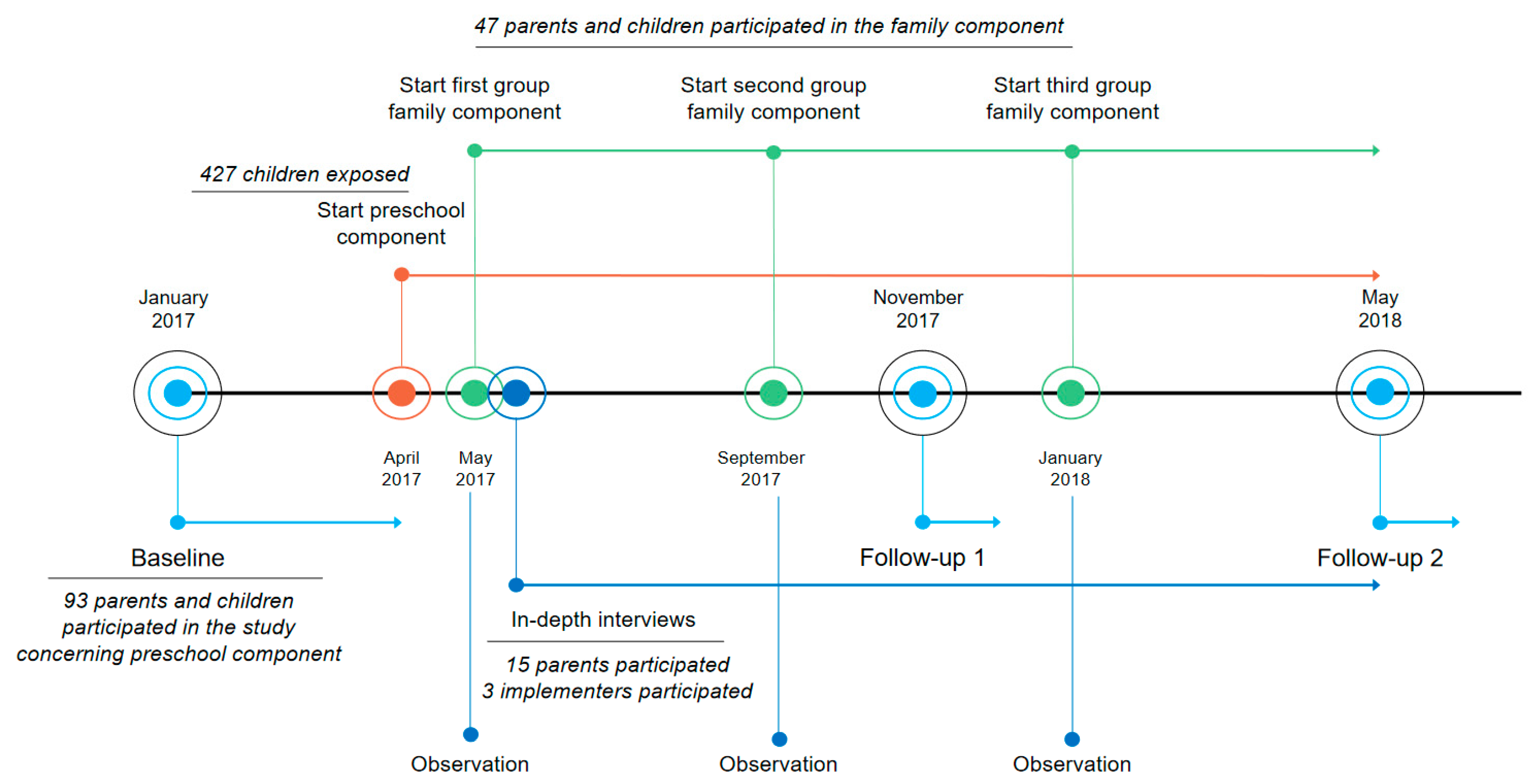
2.3. Timeline
2.4. Study Population
2.5. Measurements
2.5.1. In-Depth Interviews
2.5.2. Observations of FC Intervention Activities
2.5.3. Questionnaires
2.6. Data Processing and Analysis
3. Results
3.1. Reach
3.1.1. Participants of the FC
3.1.2. Communication
3.1.3. Attendance
3.2. Adoption
Non-adopters of the FC chose ‘no time’ and ‘no need’ most frequently in the questionnaire as reasons for not participating. A small percentage (13%) also indicated that the planning of the FC sessions conflicted with their child’s nap, one of the multiple-choice options. In interviews, both parents and implementers suspected that families who would have benefitted the most from participation (e.g., low SES, unhealthy lifestyles) were not participating.
3.3. Implementation
3.3.1. Content
3.3.2. Design of the FC
3.4. Impact
3.4.1. Parents
3.4.2. Physical Home Environment
3.4.3. Child EBRBs
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Interview Guide for Parents FC Group 1
- How much interest do you attach to healthy eating and proper exercise in a child at this age?
- Were you in need of a program to improve nutrition and movement habits for your child?Prompt: Who do you think is responsible for the correct nutrition and movement of your child?
- Have you ever been in contact with a program that targets improved nutrition and movement habits before?Prompt: What did you think of that?
- How did you get in contact with SuperFIT for the first time?
- What are your thoughts on the promotion of SuperFIT?Provide examples:
- Folder
- Poster
- Grand opening
- Would you have liked to be able to have some more (or more extensive) try-outs?
- Pedagogical staff
- Research team
- Monetary reward
- What made you decide to participate in SuperFIT?Provide example:
- Discussion with others (spouse, pedagogical staff)
- Could you describe what SuperFIT entails?Prompts: Which activities and steps to follow. Is it hard to understand?
- What are the positive consequences of participating in SuperFIT?Prompts: Concerning nutrition, physical activity, and impact on daily life.
- What are the negative consequences of participating in SuperFIT?Prompts: Concerning nutrition, physical activity, and impact on daily life.
- How does SuperFIT match your lifestyle?Prompts: Match with worldview or ideals.
- Do you think you are able to execute every aspect of SuperFIT?Provide examples:
- Planning
- Resources
- Transport
- Cheap healthy foods
- What, in your opinion, do others think of SuperFIT?Prompts: Was this of influence? Do you think it is important that others are aware that you’re participating in SuperFIT?Provide examples:
- Spouse
- Pedagogical staff
- Parents
- To what extent do you think you are able to change your child’s current behavior?Prompts: What does SuperFIT contribute to that?
- What effects do you already notice from SuperFIT?Prompts: To what extent are these effects visible?
- Which goals do you value to achieving with SuperFIT?Prompts: To what extent do you think these goals will be achieved?
- To what extent does SuperFIT match your expectations?
- What aspects of SuperFIT do you value/not value?
- Would you like to be able to receive feedback on your daily life situations?Prompts: Does SuperFIT provide enough opportunity for this?
- Could you describe the ambiance at the SuperFIT meetings?Prompts: Fun, received attention and safe environment
- What did you think of the first family meeting?Prompts: Concerning nutrition, physical activity.
- What did you think of the second family meeting?Prompts: Concerning nutrition, physical activity.
- How would you grade the facilitators?Prompts: Expertise, trust and ambiance.
- Would you like to add something to this interview?
Appendix B
Interview Guide for Parents FC Group 2 and 3
- There were five family sessions (three parent sessions, two parent-child sessions and three child sessions parallel with the parent sessions). How many sessions did you attend and which ones?
- Could you give an example of something you perceived as being good during these sessions, and why?
- Which activity or activities appealed to you the most, and why?Provide examples:
- Different themes: nutrition, physical activity, parenting
- The setup or design: different sessions for parents and children
- Duration
- Location
- Planning
- Number of sessions
- Could you give an example of something you perceived as less appealing during the sessions?Provide examples:
- Duration
- Location
- Planning
- Number of sessions
- What did you miss within the sessions?
- What do you think of the materials used?Provide examples:
- Presentations
- Triple P sheets
- Tip sheets concerning physical activity or nutrition
- Activities concerning physical activity or nutrition
- Were the materials easy to understand/clear?Prompts: If not, what could we improve?
- Did the received information comply with your expectations of the sessions?Prompts: If not, what could we improve?
- How did your child experience the sessions?Provide examples:
- Nutritional session: making healthy treats, tasting new foods
- Physical activity session: activity games, track made from play equipment
- What is your experience with the communication concerning the SuperFIT and the family component?Prompts: Sufficient information concerning session content, sufficient information concerning logistics?
- How were you informed about the family sessions?
- Do you have any ideas about how we could reach new parents for our family sessions?
- Were you able to use the received information at home?Prompts: If not, why not? Too much information or not applicable?Prompts: If so, which information were you able to use?Provide examples:
- Availability of food products
- More PA games at home
- Less sedentary time, less screen time
- Increased awareness for positive parenting
- Sports memberships for child
- Do you feel that SuperFIT has changed things changed in your daily life or at home?Prompts: For example, the way in which you approach nutrition, physical activity and your child’s behavior?Prompts: If so, what exactly?Provide examples:
- Read materials at home
- Materials used
- Changes made in the home setting
- Do you feel your child’s behavior has changed due to SuperFIT?Provide examples:
- The extent to which your child is feeling good?
- The extent to which your child is trying new fruit and vegetables, at home or at preschool?
- The extent to which your child eat fruits and vegetables?
- The extent to which your child enjoys being physically active and eating fruits and vegetables?
- The extent to which your child has become curious about nutrition and physical activity?
- Are there fewer fights at the dinner table?
- The extent to which your child has physical complaints or pains?
- The extent to which your child easily adapts to new physical activity games?
- The extent to which your child is physically active?
- The extent to which your child is able to handle setbacks?
- Would you like to add something to this interview?
Appendix C
Interview Guide for Implementers
- What were your thoughts on the promotion of SuperFIT?Prompts: And for you as implementer?Provide examples:
- Folder
- Poster
- Kick-off event
- What do you think that others think of SuperFIT?Provide examples:
- Participants
- Non-participants
- Preschool staff
- Do you think you are able to change behaviors in families?Prompts: What is the contribution of SuperFIT in this change?
- What effects do you already notice?Prompts: In parents? Or yourself?
- Could you describe the ambiance of the different family sessions?
- How did you experience the family sessions?
- How would you describe the cooperation with parents?Prompts: Are they capable of understanding the given information? Do they trust you?
References
- Rennie, K.L.; Johnson, L.; Jebb, S.A. Behavioural determinants of obesity. Best Pract. Res. Clin. Endocrinol. Metab. 2005, 19, 343–358. [Google Scholar] [CrossRef] [PubMed]
- Craigie, A.M.; Lake, A.A.; Kelly, S.A.; Adamson, A.J.; Mathers, J.C. Tracking of obesity-related behaviours from childhood to adulthood: A systematic review. Maturitas 2011, 70, 266–284. [Google Scholar] [CrossRef]
- Telama, R.; Yang, X.; Leskinen, E.; Kankaanpaa, A.; Hirvensalo, M.; Tammelin, T.; Viikari, J.S.; Raitakari, O.T. Tracking of physical activity from early childhood through youth into adulthood. Med. Sci. Sports Exerc. 2014, 46, 955–962. [Google Scholar] [CrossRef]
- Northstone, K.; Emmett, P.M. Are dietary patterns stable throughout early and mid-childhood? A birth cohort study. Br. J. Nutr. 2008, 100, 1069–1076. [Google Scholar] [CrossRef] [PubMed]
- Bel-Serrat, S.; Ojeda-Rodríguez, A.; Heinen, M.M.; Buoncristiano, M.; Abdrakhmanova, S.; Duleva, V.; Sant’Angelo, V.F.; Fijałkowska, A.; Hejgaard, T.; Huidumac, C.; et al. Clustering of Multiple Energy Balance-Related Behaviors in School Children and its Association with Overweight and Obesity-WHO European Childhood Obesity Surveillance Initiative (COSI 2015–2017). Nutrients 2019, 11, 511. [Google Scholar] [CrossRef] [PubMed]
- Leech, R.M.; McNaughton, S.A.; Timperio, A. The clustering of diet, physical activity and sedentary behavior in children and adolescents: A review. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 4. [Google Scholar] [CrossRef] [PubMed]
- Birch, L.; Savage, J.S.; Ventura, A. Influences on the Development of Children’s Eating Behaviours: From Infancy to Adolescence. Can. J. Diet Pract. Res. 2007, 68, s1–s56. [Google Scholar]
- Golan, M.; Crow, S. Parents are key players in the prevention and treatment of weight-related problems. Nutr. Rev. 2004, 62, 39–50. [Google Scholar] [CrossRef]
- Kristiansen, A.L.; Bjelland, M.; Himberg-Sundet, A.; Lien, N.; Andersen, L.F. Associations between physical home environmental factors and vegetable consumption among Norwegian 3–5-year-olds: The BRA-study. Public Health Nutr. 2017, 20, 1173–1183. [Google Scholar] [CrossRef]
- Vereecken, C.; Rovner, A.; Maes, L. Associations of parenting styles, parental feeding practices and child characteristics with young children’s fruit and vegetable consumption. Appetite 2010, 55, 589–596. [Google Scholar] [CrossRef]
- Armstrong, G.P.; Maitland, C.; Lester, L.; Trost, S.G.; Trapp, G.; Boruff, B.; Al Marzooqi, M.K.; Christian, H.E. Associations between the home yard and preschoolers’ outdoor play and physical activity. Public Health Res. Pract. 2019, 29, 907. [Google Scholar] [CrossRef] [PubMed]
- Spurrier, N.J.; Magarey, A.A.; Golley, R.; Curnow, F.; Sawyer, M.G. Relationships between the home environment and physical activity and dietary patterns of preschool children: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 31. [Google Scholar] [CrossRef] [PubMed]
- Mazarello, P.V.; Ong, K.K.; Lakshman, R. Factors influencing obesogenic dietary intake in young children (0–6 years): Systematic review of qualitative evidence. BMJ Open 2015, 5, e007396. [Google Scholar] [CrossRef] [PubMed]
- Sleddens, E.F.; Gerards, S.M.; Thijs, C.; de Vries, N.K.; Kremers, S.P. General parenting, childhood overweight and obesity-inducing behaviors: A review. Pediatr. Obes. 2011, 6, e12–e27. [Google Scholar] [CrossRef]
- Vereecken, C.; Legiest, E.; De Bourdeaudhuij, I.; Maes, L. Associations between general parenting styles and specific food-related parenting practices and children’s food consumption. Am. J. Health Promot. 2009, 23, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Fiese, B.H.; Hammons, A.; Grigsby-Toussaint, D. Family mealtimes: A contextual approach to understanding childhood obesity. Econ. Hum. Biol. 2012, 10, 365–374. [Google Scholar] [CrossRef]
- Østbye, T.; Malhotra, R.; Stroo, M.; Lovelady, C.; Brouwer, R.; Zucker, N.; Fuemmeler, B. The effect of the home environment on physical activity and dietary intake in preschool children. Int. J. Obes. 2013, 37, 1314–1321. [Google Scholar] [CrossRef]
- Schlechter, C.R.; Rosenkranz, R.R.; Guagliano, J.M.; Dzewaltowski, D.A. A systematic review of children’s dietary interventions with parents as change agents: Application of the RE-AIM framework. Prev. Med. 2016, 91, 233–243. [Google Scholar] [CrossRef]
- Luesse, H.B.; Paul, R.; Gray, H.L.; Koch, P.; Contento, I.; Marsick, V. Challenges and Facilitators to Promoting a Healthy Food Environment and Communicating Effectively with Parents to Improve Food Behaviors of School Children. Matern. Child Health J. 2018, 22, 958–967. [Google Scholar] [CrossRef]
- Bleich, S.N.; Vercammen, K.A.; Zatz, L.Y.; Frelier, J.M.; Ebbeling, C.B.; Peeters, A. Interventions to prevent global childhood overweight and obesity: A systematic review. Lancet Diabetes Endocrinol. 2018, 6, 332–346. [Google Scholar] [CrossRef]
- Hingle, M.D.; O’Connor, T.M.; Dave, J.M.; Baranowski, T. Parental involvement in interventions to improve child dietary intake: A systematic review. Prev. Med. 2010, 51, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Kader, M.; Sundblom, E.; Elinder, L.S. Effectiveness of universal parental support interventions addressing children’s dietary habits, physical activity and bodyweight: A systematic review. Prev. Med. 2015, 77, 52–67. [Google Scholar] [CrossRef] [PubMed]
- Van de Kolk, I.; Verjans-Janssen, S.R.B.; Gubbels, J.S.; Kremers, S.P.J.; Gerards, S. Systematic review of interventions in the childcare setting with direct parental involvement: Effectiveness on child weight status and energy balance-related behaviours. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 110. [Google Scholar] [CrossRef] [PubMed]
- Waters, E.; de Silva-Sanigorski, A.; Hall, B.J.; Brown, T.; Campbell, K.J.; Gao, Y.; Armstrong, R.; Prosser, L.; Summerbell, C.D. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2011, 12, 1871. [Google Scholar] [CrossRef] [PubMed]
- Bronfenbrenner, U. The Ecology of Human Development; Harvard University Press: Cambridge, MA, USA, 1979. [Google Scholar]
- Bradley, R.H. From home to day care: Chaos in the family/child-care mesosystem. In Chaos and Its Influence on Children’s Development: An Ecological Perspective; Decade of Behavior (Science Conference); American Psychological Association: Washington, DC, USA, 2010; pp. 135–153. [Google Scholar]
- Gubbels, J.S.; Stessen, K.; van de Kolk, I.; de Vries, N.K.; Thijs, C.; Kremers, S.P.J. Energy balance-related parenting and child-care practices: The importance of meso-system consistency. PLoS ONE 2018, 13, e0203689. [Google Scholar] [CrossRef]
- van de Kolk, I.; Gerards, S.; Harms, L.S.E.; Kremers, S.P.J.; van Dinther-Erkens, A.; Snellings, M.; Gubbels, J.S. Study Protocol for the Evaluation of “SuperFIT”, a Multicomponent Nutrition and Physical Activity Intervention Approach for Preschools and Families. Int. J. Environ. Res. Public Health 2020, 17, 603. [Google Scholar] [CrossRef]
- van de Kolk, I.; Gerards, S.; Harms, L.S.E.; Kremers, S.P.J.; Gubbels, J.S. The Effects of a Comprehensive, Integrated Obesity Prevention Intervention Approach (SuperFIT) on Children’s Physical Activity, Sedentary Behavior, and BMI Z-Score. Int. J. Environ. Res. Public Health 2019, 16, 5016. [Google Scholar] [CrossRef]
- Harms, L.S.E.; Gubbels, J.S.; Van de Kolk, I.; Vanbelle, S.; Bessems, K.M.H.H.; Hahnraths, M.T.H.; Kremers, S.P.J.; Gerards, S.M.P.L. The effects of SuperFIT; a comprehensive, integrated intervention approach, on pre-schoolers dietary intake. 2020; submitted for publication. [Google Scholar]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. Int. J. Nurs. Stud. 2013, 50, 587–592. [Google Scholar] [CrossRef]
- Oakley, A.; Strange, V.; Bonell, C.; Allen, E.; Stephenson, J. Process evaluation in randomised controlled trials of complex interventions. BMJ 2006, 332, 413–416. [Google Scholar] [CrossRef]
- Van de Kolk, I.; Gerards, S.M.; Verhees, A.H.; Kremer, P.J.; Gubbels, J.S. Changing the preschool setting to promote healthy energy balance-related behaviours of pre-schoolers: A process and impact evaluation of the SuperFIT approach. 2021; submitted for publication. [Google Scholar]
- Jang, M.; Chao, A.; Whittemore, R. Evaluating Intervention Programs Targeting Parents to Manage Childhood Overweight and Obesity: A Systematic Review Using the RE-AIM Framework. J. Pediatr. Nurs. 2015, 30, 877–887. [Google Scholar] [CrossRef]
- Norman, Å.; Nyberg, G.; Elinder, L.S.; Berlin, A. One size does not fit all-qualitative process evaluation of the Healthy School Start parental support programme to prevent overweight and obesity among children in disadvantaged areas in Sweden. BMC Public Health 2016, 16, 37. [Google Scholar] [CrossRef]
- Gaglio, B.; Shoup, J.A.; Glasgow, R.E. The RE-AIM framework: A systematic review of use over time. Am. J. Public Health 2013, 103, e38–e46. [Google Scholar] [CrossRef]
- Glasgow, R.E.; Vogt, T.M.; Boles, S.M. Evaluating the public health impact of health promotion interventions: The RE-AIM framework. Am. J. Public Health 1999, 89, 1322–1327. [Google Scholar] [CrossRef] [PubMed]
- Swinburn, B.; Egger, G.; Raza, F. Dissecting obesogenic environments: The development and application of a framework for identifying and prioritizing environmental interventions for obesity. Prev. Med. 1999, 29, 563–570. [Google Scholar] [CrossRef]
- Bartlett, J.A. The Lifestyle Triple P Multilevel System of Parenting and Family Support for the Prevention and Treatment of Childhood Obesity. Ph.D. Thesis, University of Queensland, Queensland, Australia, 2017. [Google Scholar]
- O’Connor, T.M.; Cerin, E.; Hughes, S.O.; Robles, J.; Thompson, D.I.; Mendoza, J.A.; Baranowski, T.; Lee, R.E. Psychometrics of the preschooler physical activity parenting practices instrument among a Latino sample. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 3. [Google Scholar] [CrossRef] [PubMed]
- Musher-Eizenman, D.; Holub, S. Comprehensive Feeding Practices Questionnaire: Validation of a new measure of parental feeding practices. J. Pediatr. Psychol. 2007, 32, 960–972. [Google Scholar] [CrossRef] [PubMed]
- Ward, D.S.; Mazzucca, S.; McWilliams, C.; Hales, D. Use of the Environment and Policy Evaluation and Observation as a Self-Report Instrument (EPAO-SR) to measure nutrition and physical activity environments in child care settings: Validity and reliability evidence. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 124. [Google Scholar] [CrossRef]
- Portney, L.G. Foundations of Clinical Research: Applications to Practice, 2nd ed.; Prentice Hall: Upper Saddle River, NJ, USA, 2000. [Google Scholar]
- Heath, S.M.; Wigley, C.A.; Hogben, J.H.; Fletcher, J.; Collins, P.; Boyle, G.L.; Eustice, S. Patterns in Participation: Factors Influencing Parent Attendance at Two, Centre-Based Early Childhood Interventions. J. Child Fam. Stud. 2018, 27, 253–267. [Google Scholar] [CrossRef]
- Marmot, M. Social determinants of health inequalities. Lancet Lond. Engl. 2005, 365, 1099–1104. [Google Scholar] [CrossRef]
- Walton, K.; Ambrose, T.; Annis, A.; Ma, D.W.; Haines, J. Putting family into family-based obesity prevention: Enhancing participant engagement through a novel integrated knowledge translation strategy. BMC Med. Res. Methodol. 2018, 18, 126. [Google Scholar] [CrossRef]
- Morgan, P.J.; Lubans, D.R.; Plotnikoff, R.C.; Callister, R.; Burrows, T.; Fletcher, R.; Okely, A.D.; Young, M.D.; Miller, A.; Clay, V.; et al. The ‘Healthy Dads, Healthy Kids’ community effectiveness trial: Study protocol of a community-based healthy lifestyle program for fathers and their children. BMC Public Health 2011, 11, 876. [Google Scholar] [CrossRef] [PubMed]
- Dwyer, J.; Needham, L.; Simpson, J.R.; Heeney, E.S. Parents report intrapersonal, interpersonal, and environmental barriers to supporting healthy eating and physical activity among their preschoolers. Appl. Physiol. Nutr. Metab. 2008, 33, 338–346. [Google Scholar] [CrossRef] [PubMed]
- Martin-Biggers, J.; Spaccarotella, K.; Hongu, N.; Alleman, G.; Worobey, J.; Byrd-Bredbenner, C. Translating it into real life: A qualitative study of the cognitions, barriers and supports for key obesogenic behaviors of parents of preschoolers. BMC Public Health 2015, 15, 189. [Google Scholar] [CrossRef] [PubMed]
- O’Kane, C.; Wallace, A.; Wilson, L.; Annis, A.; Ma, D.W.L.; Haines, J. Family-Based Obesity Prevention: Perceptions of Canadian Parents of Preschool-Age Children. Can. J. Diet Pract. Res. 2018, 79, 13–17. [Google Scholar] [CrossRef]
- Velardo, S. The Nuances of Health Literacy, Nutrition Literacy, and Food Literacy. J. Nutr. Educ. Behav. 2015, 47, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Douglas, F.; Clark, J.; Craig, L.; Campbell, J.; McNeill, G. “It’s a balance of just getting things right”: Mothers’ views about pre-school childhood obesity and obesity prevention in Scotland. BMC Public Health 2014, 14, 1009. [Google Scholar] [CrossRef]
- Ensaff, H.; Canavon, C.; Crawford, R.; Barker, M.E. A qualitative study of a food intervention in a primary school: Pupils as agents of change. Appetite 2015, 95, 455–465. [Google Scholar] [CrossRef]


{kind=link}
| Themes | Data Source | Concept | Example Question(s) or Content | ||
|---|---|---|---|---|---|
| 1 | Reach | Qualitative | Parental interviews | Communication Recruitment Strengths and limitations | How did you come into contact with SuperFIT? How were you informed about the FC? |
| Implementer interviews | Recruitment Strengths and limitations | What were your thoughts on the promotion of SuperFIT? (kick-off session, information folder) | |||
| Quantitative | Registration forms | Attendance | Number of parents attending the FC intervention activities. | ||
| Parental questionnaires | Demographics | Characteristics of participants of the FC. | |||
| 2 | Adoption by parents | Qualitative | Parental interviews | Expectations Reasons to participate | What made you decide to participate? |
| Non adoption by parents | Quantitative | Questionnaires for PC participants | Reasons to decline participation | What was your reason for not participating in the FC? (multiple choice) | |
| 3 | Implementation | ||||
| 3a | FC content | Qualitative | Parental interviews | Appreciation of FC intervention activities Strengths and limitations | Can you give an example of something that you liked or disliked during the sessions? Which part or parts appealed to you the most, and why? What did you think of the materials used? |
| Implementers interviews | Experiences | How did you experience the first family session? | |||
| Observations | Contextual factors | Group dynamics, questions asked | |||
| Quantitative | Parental questionnaires | Appreciation of FC activities (scoring) | Did you find the program educational? What did you think of the activities concerning nutrition? | ||
| 3b | FC design | Qualitative | Parental interviews | Appreciation of the FC set-up, Strengths and limitations | What did you think of the intervention design, the various session types? What did you think of the timing and number of sessions? |
| Implementers interviews | Experiences Strengths and limitations | How would you describe the cooperation with the parents? | |||
| Observations | Contextual factors | ||||
| Quantitative | Parental questionnaires | Appreciation of the FC set-up (scoring) Duration Time investment | What did you think of the duration of the program? | ||
| 4 | Impact | ||||
| 4a | Parent(s) | Qualitative | Parental interviews | Self-reported impact on own behavior | Do you feel that there has been a change in the way you deal with your child’s (healthy) EBRBs? |
| Quantitative | Parental questionnaires | PA parenting practices (PPAPP) Nutritional parenting practices (CFPQ) | How often do you go on a walk with your child? Do you encourage this child to eat healthy foods before unhealthy ones? | ||
| 4b | Physical home environment | Qualitative | Parental interviews | Self-reported impact on family daily life or home setting | Were you able to use the received information at home? How? Why not? |
| Quantitative | Parental questionnaires (EPAO_SR) | Availability of play equipment | Which of the following play equipment is available inside the house? | ||
| 4c | Child EBRBs | Qualitative | Parental interviews | Self-reported impact on child behavior | Do you feel that there are changes in the behavior of your child due to SuperFIT? What was the situation before participating in SuperFIT? |
| Demographics | Questionnaires on Parenting Practices | Questionnaire on Quantitative Evaluation of FC | Interviews |
|---|---|---|---|
| n (%) 1 | n (%) 1 | n (%) 1 | |
| Parents n (%) 1 | 41 (100) | 19 (100) | 15 (100) |
| Gender, female | 16 (84.2) | 13 (86.7) | |
| T0 | 25 (80.6) | ||
| T1 | 20 (83.3) | ||
| T2 | 23 (92.0) | ||
| Number of children | |||
| -one | 14 (45.2) | 4 (26.7) | 4 (26.7) |
| -two | 15 (48.4) | 9 (60.0) | 8 (53.3) |
| -three | 2 (6.5) | 2 (13.3) | 3 (20.0) |
| Educational level 2 | |||
| -low | 5 (12.5) | 1 (5.3) | 1 (7.1) |
| -middle | 12 (30.0) | 8 (42.1) | 5 (35.7) |
| -high | 23 (57.5) | 10 (52.6) | 8 (57.1) |
| Employment status | |||
| -unemployed | 10 (32.3) | 3 (20.0) | 3 (20.0) |
| -employed (full-time or part-time) | 21 (67.7) | 12 (80.0) | 12 (80.0) |
| Country of birth | |||
| The Netherlands | 37 (92.5) | 18 (94.7) | n.a. |
| Implementers n (%) | 3 (100) | ||
| Percentage of females | 2 (66.7) | ||
| Educational level | |||
| -high | 3 (100.0) | ||
| Employment status | |||
| -part-time | 2 (66.7) | ||
| -full-time | 1 (33.3) | ||
| Country of birth | |||
| -Netherlands | 3 (100.0) |
| Scale | Items | Cronbach’s Alpha (T0) | Baseline (n = 28) | Follow-Up 1 7–10 Months (n = 22) | Follow-Up 2 13–16 Months (n = 25) |
|---|---|---|---|---|---|
| Mean (SD) | Change in Mean | Change in Mean | |||
| Nutritional parenting practices 1 | |||||
| Scales that promote healthy EBRBs | |||||
| Encouraging balance/variety | 4 | 0.82 | 4.38 (0.68) | +0.10 | +0.03 |
| Providing a healthy food environment | 3 | 0.56 | 3.30 (0.81) | +0.35 | +0.18 |
| Involving child with food | 3 | 0.63 | 4.05 (0.77) | +0.01 | +0.14 |
| Modelling healthy food intake | 4 | 0.84 | 4.38 (0.81) | +0.03 | +0.14 |
| Monitoring diet child | 2 | 0.74 | 3.48 (1.12) | +0.38 | +0.24 |
| Teaching child about nutrition | 4 | 0.66 | 3.73 (0.89) | +0.36 | +0.28 |
| Scales that inhibit healthy EBRBs healthy EBRBs | |||||
| Using food for emotional regulation | 3 | 0.72 | 1.73 (0.65) | −0.18 | −0.11 |
| Using food as reward | 3 | 0.61 | 2.69 (0.92) | −0.43 | −0.54 |
| Pressuring to eat | 3 | 0.60 | 3.22 (0.83) | +0.26 | −0.05 |
| Single items that promote/inhibit healthy EBRBs | |||||
| Child allowed to choose between different healthy products (environment) | 3.75 (1.04) | +0.34 | +0.13 | ||
| Child pressured to finish plate (pressure) | 2.14 (1.21) | −0.23 | +0.18 | ||
| Child allowed to choose food (control) | 3.04 (0.79) | +0.01 | +0.20 | ||
| Child allowed to choose food served (control) | 3.29 (0.81) | +0.12 | +0.59 | ||
| Preparing other food for child (control) | 2.25 (1.14) | +0.07 | −0.33 | ||
| Child allowed to snack (control) | 2.71 (0.90) | −0.53 | −0.11 | ||
| Child allowed to leave table early (control) | 2.27 (1.16) | +0.23 | +0.41 | ||
| PA parenting practices 1 | |||||
| Scales that promote healthy EBRBs | |||||
| Parental engagement | 13 | 0.87 | 3.61 (0.51) | +0.12 | +0.10 |
| Scales that inhibit healthy EBRBs | |||||
| Promoting screen time | 2 | 0.61 | 2.75 (0.71) | −0.05 | −0.25 |
| Using psychological control of PA | 5 | 0.60 | 2.10 (0.52) | −0.03 | −0.06 |
| Restricting PA | 3 | 0.72 | 1.68 (0.73) | +0.19 | +0.33 |
| Single items that promote/inhibit healthy EBRBs | |||||
| Child allowed to play outside (restriction) | 3.93 (0.66) | +0.07 | +0.27 | ||
| Availability of play equipment outside (engagement) | 4.57 (0.63) | −0.25 | +0.11 | ||
| Carrying child (promote inactivity) | 2.41 (0.81) | −0.23 | −0.57 | ||
| Using stroller (promote inactivity) | 2.14 (1.08) | −0.23 | −0.54 | ||
| Using the car while distance is walkable (promote inactivity) | 2.71 (0.90) | −0.30 | −0.35 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harms, L.S.E.; Gerards, S.M.P.L.; Kremers, S.P.J.; Bessems, K.M.H.H.; van Luijk, C.; Arslan, T.; Mombers, F.M.; Gubbels, J.S. Involving Parents in Promoting Healthy Energy Balance-Related Behaviors in Preschoolers: A Mixed Methods Impact and Process Evaluation of SuperFIT. Nutrients 2021, 13, 1605. https://doi.org/10.3390/nu13051605
Harms LSE, Gerards SMPL, Kremers SPJ, Bessems KMHH, van Luijk C, Arslan T, Mombers FM, Gubbels JS. Involving Parents in Promoting Healthy Energy Balance-Related Behaviors in Preschoolers: A Mixed Methods Impact and Process Evaluation of SuperFIT. Nutrients. 2021; 13(5):1605. https://doi.org/10.3390/nu13051605
Chicago/Turabian StyleHarms, Lisa S. E., Sanne M. P. L. Gerards, Stef P. J. Kremers, Kathelijne M. H. H. Bessems, Carsten van Luijk, Tülay Arslan, Femke M. Mombers, and Jessica S. Gubbels. 2021. "Involving Parents in Promoting Healthy Energy Balance-Related Behaviors in Preschoolers: A Mixed Methods Impact and Process Evaluation of SuperFIT" Nutrients 13, no. 5: 1605. https://doi.org/10.3390/nu13051605
APA StyleHarms, L. S. E., Gerards, S. M. P. L., Kremers, S. P. J., Bessems, K. M. H. H., van Luijk, C., Arslan, T., Mombers, F. M., & Gubbels, J. S. (2021). Involving Parents in Promoting Healthy Energy Balance-Related Behaviors in Preschoolers: A Mixed Methods Impact and Process Evaluation of SuperFIT. Nutrients, 13(5), 1605. https://doi.org/10.3390/nu13051605