
Histamine Intolerance in Children: A Narrative Review

 , ,
, ,
Abstract
:1. Introduction
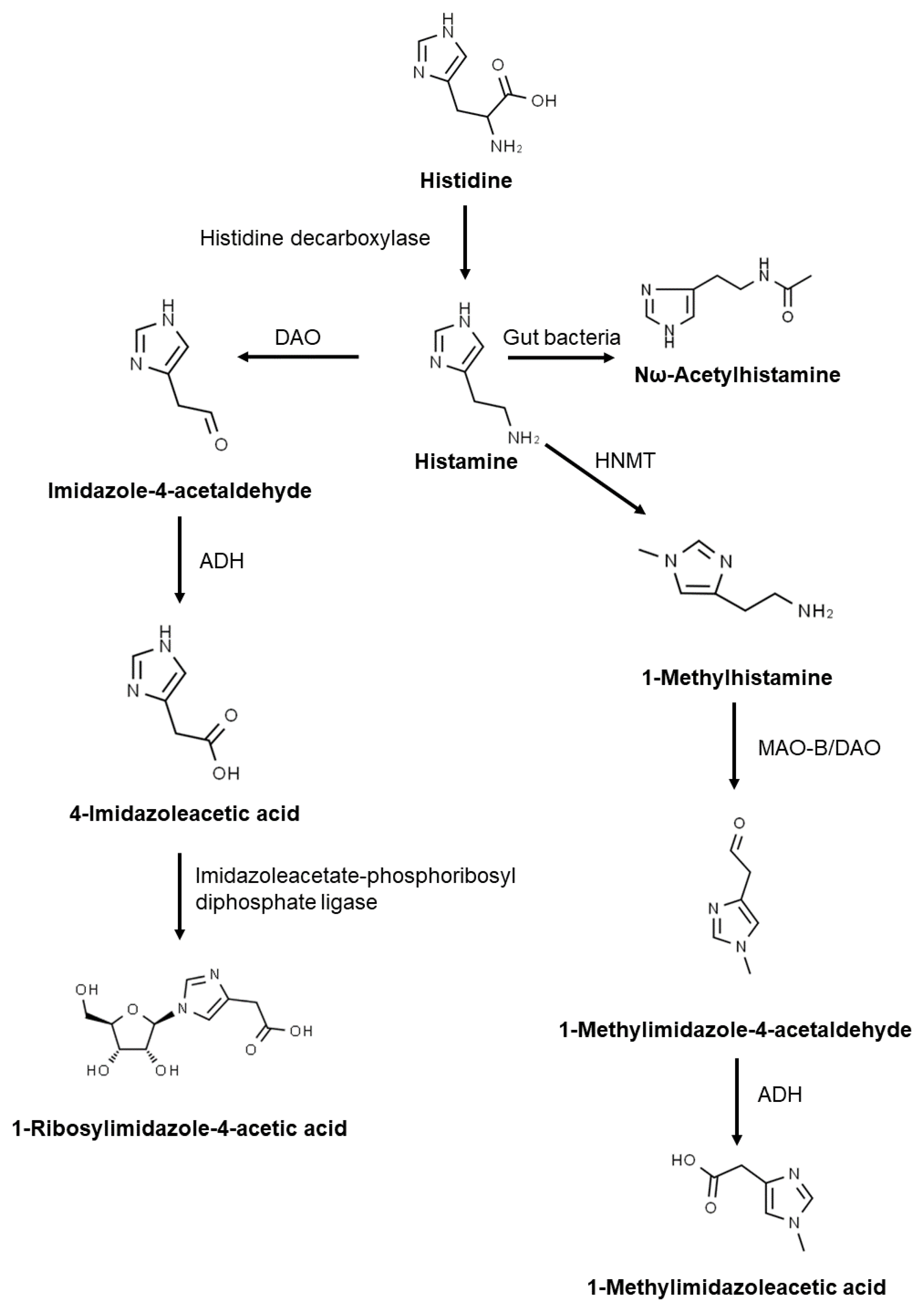
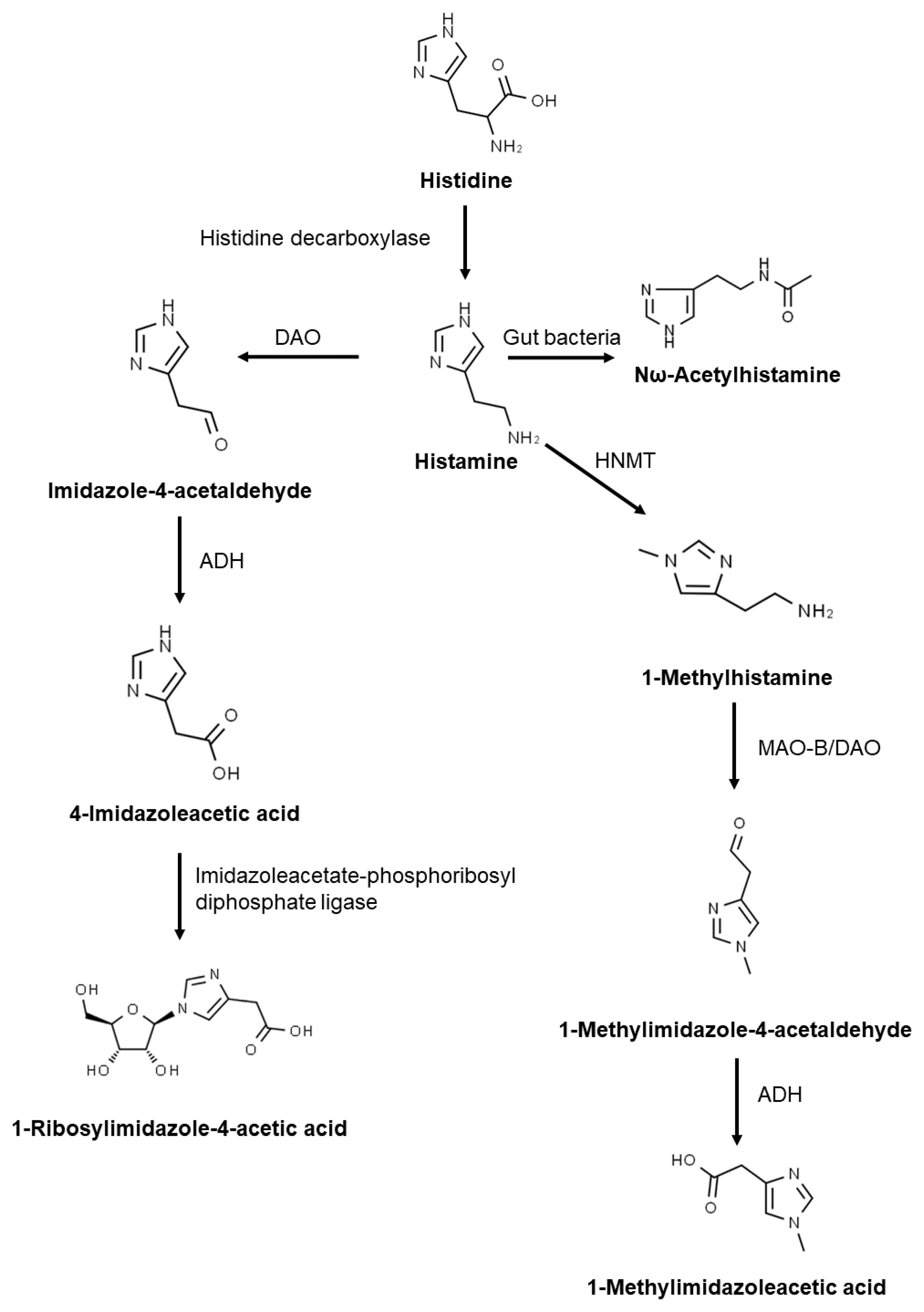
2. Histamine Metabolism
3. Histamine Content in Foods
4. Histamine Intolerance or Histamine Intoxication?
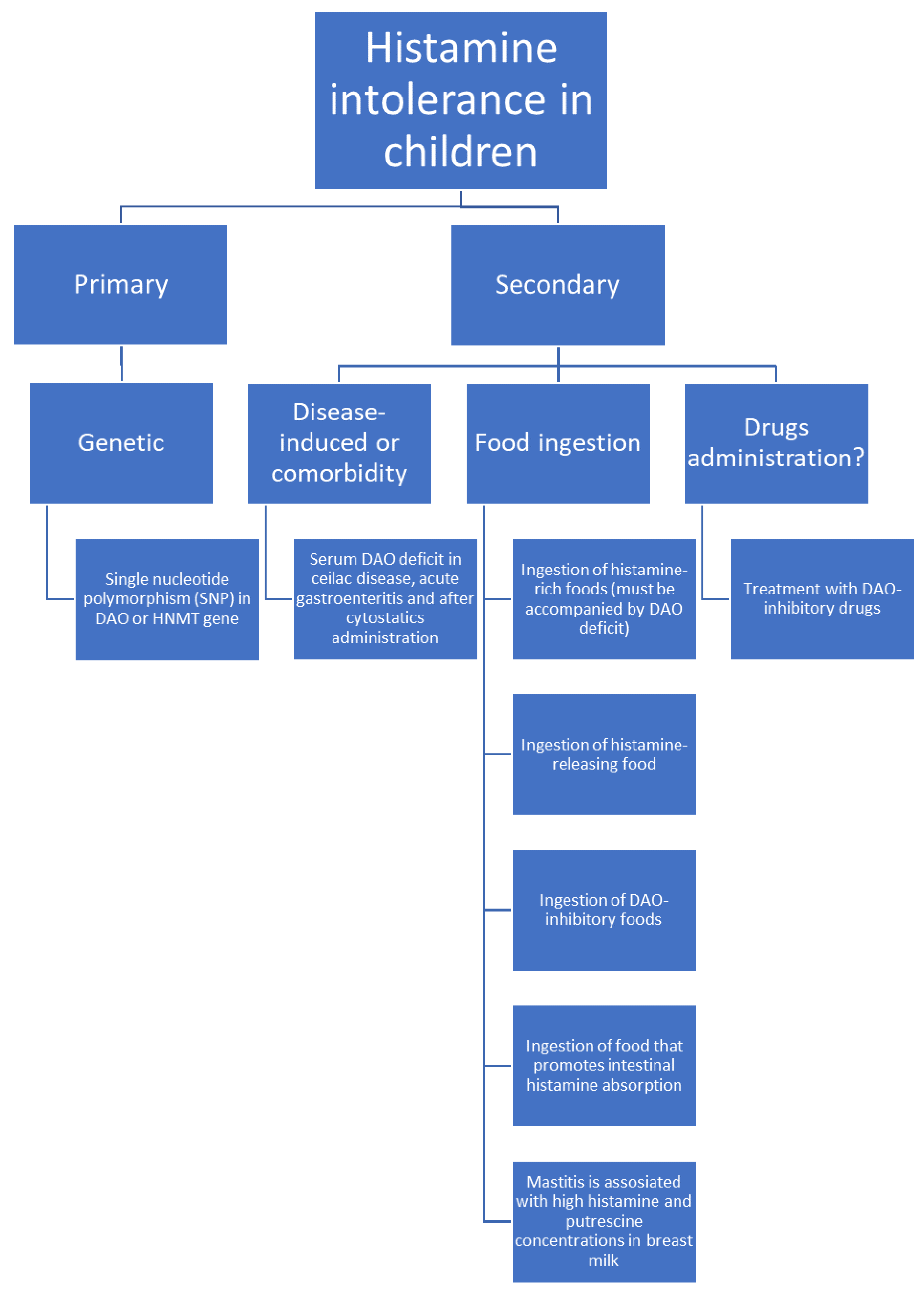
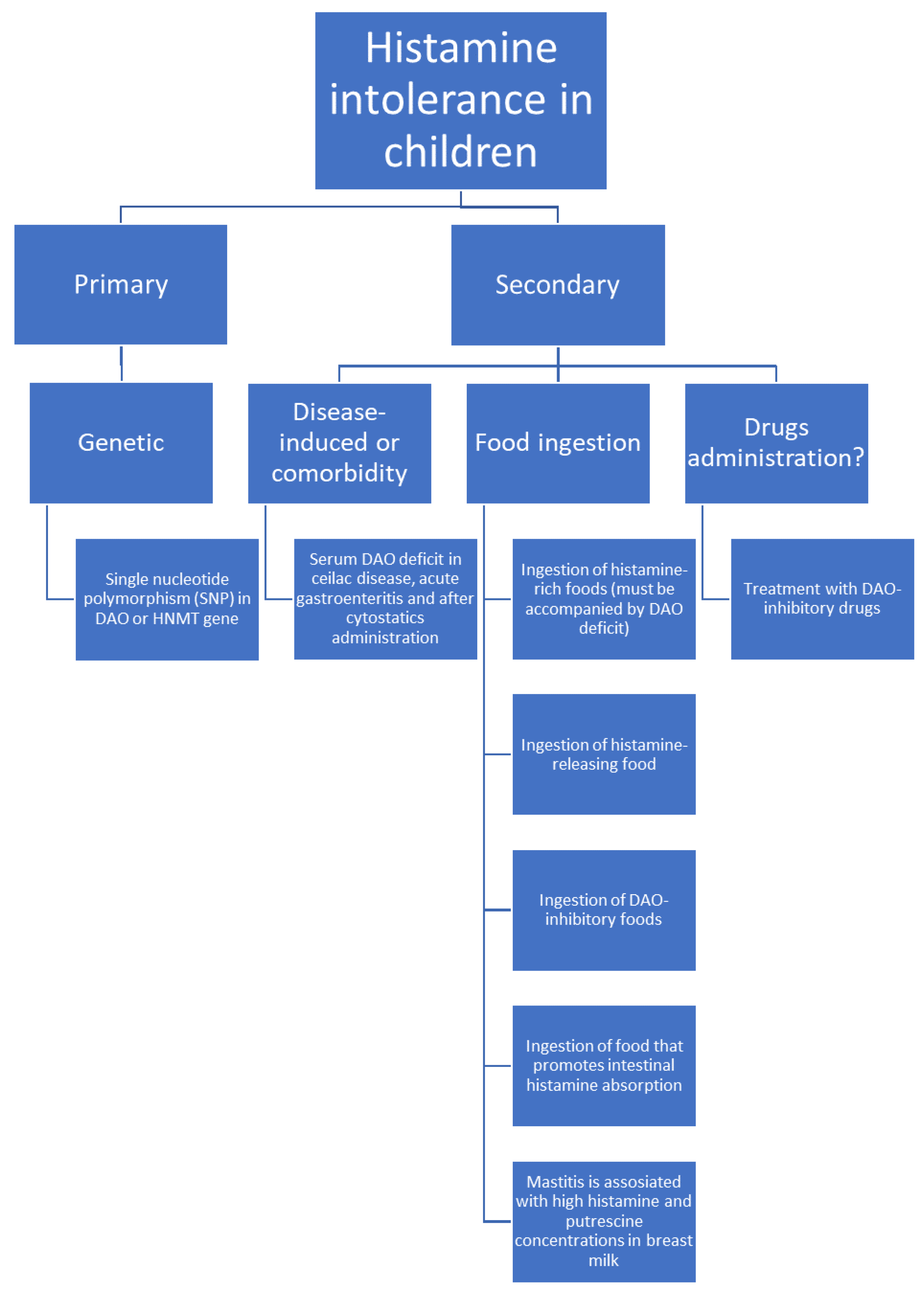
5. Primary (Genetic) Histamine Intolerance
6. Secondary Histamine Intolerance Aetiology
6.1. Disease-Induced Histamine Intolerance
- Are food intolerances (e.g., lactose or fructose malabsorption) and histamine intolerance frequently comorbid?
- Could disaccharide malabsorption and histamine intolerance be caused by the same primary intestine-damaging disease?
- And, most importantly: is HIT heavily underdiagnosed?
6.2. Food Consumption
- Fish, sauerkraut, smoked meat products and some cheeses contain large amounts of histamine and may trigger HIT symptoms due to even slight overavailability of histamine [1,3,7,33,34,35]. Histamine’s presence in these foods is a result of histidine decarboxylation by microorganisms that exhibit histidine decarboxylase activity. This process occurs during food production [5]. To diagnose HIT, ingestion of histamine-rich food must be accompanied by a DAO deficit. Otherwise, histamine intoxication should be diagnosed.
- Some products can likely trigger histamine release. Examples are citrus fruits, papaya, strawberries, egg white, chocolate, some types of nuts, fish, and pork [1].
6.3. Breastfeeding
6.4. Drugs Administration
7. Epidemiology of Histamine Intolerance in the Paediatric Population
8. Histamine Intolerance Diagnosis in Children
9. Proposed Diagnostic Algorithm for Histamine Intolerance in Children
10. Symptoms of Histamine Intolerance
11. Major Criteria
12. Minor Criteria
13. Comorbidities
14. Treatment of Histamine Intolerance
15. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Maintz, L.; Novak, N. Histamine and histamine intolerance. Am. J. Clin. Nutr. 2007, 85, 1185–1196. [Google Scholar] [CrossRef]
- Kacik, J.; Wróblewska, B.; Lewicki, S.; Zdanowski, R.; Kalicki, B. Serum Diamine Oxidase in Pseudoallergy in the Pediatric Population. Adv. Exp. Med. Biol. 2017, 1039, 35–44. [Google Scholar] [CrossRef]
- Comas-Basté, O.; Sánchez-Pérez, S.; Veciana-Nogués, M.T.; Latorre-Moratalla, M.; Vidal-Carou, M.D.C. Histamine intoler-ance: The current state of the art. Biomolecules 2020, 10, 1181. [Google Scholar] [CrossRef]
- Moriguchi, T.; Takai, J. Histamine and histidine decarboxylase: Immunomodulatory functions and regulatory mechanisms. Genes Cells 2020, 25, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Schwelberger, H.G. Histamine intolerance: A metabolic disease? Inflamm. Res. 2009, 59, 219–221. [Google Scholar] [CrossRef] [PubMed]
- Nelis, M.; Decraecker, L.; Boeckxstaens, G.; Augustijns, P.; Cabooter, D. Development of a HILIC-MS/MS method for the quantification of histamine and its main metabolites in human urine samples. Talanta 2020, 220, 121328. [Google Scholar] [CrossRef] [PubMed]
- Rosell-Camps, A.; Zibetti, S.; Pérez-Esteban, G.; Vila-Vidal, M.; Ferrés-Ramis, L.; García-Teresa-García, E. Histamine intoler-ance as a cause of chronic digestive complaints in pediatric patients. Rev. Española Enferm. Dig. 2013, 105, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Doeun, D.; Davaatseren, M.; Chung, M.-S. Biogenic amines in foods. Food Sci. Biotechnol. 2017, 26, 1463–1474. [Google Scholar] [CrossRef]
- Sánchez-Pérez, S.; Comas-Basté, O.; Rabell-González, J.; Veciana-Nogués, M.T.; Latorre-Moratalla, M.L.; Vidal-Carou, M.C. Biogenic Amines in Plant-Origin Foods: Are they Frequently Underestimated in Low-Histamine Diets? Foods 2018, 7, 205. [Google Scholar] [CrossRef] [Green Version]
- Lieberman, P. The basics of histamine biology. Ann. Allergy Asthma Immunol. 2011, 106, S2–S5. [Google Scholar] [CrossRef]
- Colombo, F.M.; Cattaneo, P.; Confalonieri, E.; Bernardi, C. Histamine food poisonings: A systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 2018, 58, 1131–1151. [Google Scholar] [CrossRef] [Green Version]
- Mah, J.-H.; Park, Y.K.; Jin, Y.H.; Lee, J.-H.; Hwang, H.-J. Bacterial Production and Control of Biogenic Amines in Asian Fermented Soybean Foods. Foods 2019, 8, 85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaur, S.; Ali, A.; Siahbalaei, Y.; Ahmad, U.; Nargis, F.; Pandey, A.K.; Singh, B. Association of Diamine oxidase (DAO) vari-ants with the risk for migraine from North Indian population. Meta Gene 2020, 24, 100619. [Google Scholar] [CrossRef]
- Garcia-Martin, E.; García-Menaya, J.; Sanchez, B.; Martínez, C.; Rosendo, R.; Agúndez, J.A.G. Polymorphisms of histamine-metabolizing enzymes and clinical manifestations of asthma and allergic rhinitis. Clin. Exp. Allergy 2007, 37, 1175–1182. [Google Scholar] [CrossRef]
- Meza-Velázquez, R.; López-Márquez, F.; Espinosa-Padilla, S.; Rivera-Guillen, M.; Gutíerrez-Díaz, N.; Pérez-Armendáriz, L.; Rosales-González, M. Association between two polymorphisms of histamine-metabolising enzymes and the severity of allergic rhinitis in a group of Mexican children. Allergol. Immunopathol. 2016, 44, 433–438. [Google Scholar] [CrossRef]
- Kennedy, M.J.; Loehle, J.A.; Griffin, A.R.; Doll, M.A.; Kearns, G.L.; Sullivan, J.E.; Hein, D.W. Association of the HistamineN-Methyltransferase C314T (Thr105Ile) Polymorphism with Atopic Dermatitis in Caucasian Children. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2008, 28, 1495–1501. [Google Scholar] [CrossRef] [Green Version]
- Deindl, P.; Peri-Jerkan, S.; Deichmann, K.; Niggemann, B.; Lau, S.; Sommerfeld, C.; Sengler, C.; Müller, S.; Wahn, U.; Nickel, R.; et al. No association of histamine- N-methyltransferase polymorphism with asthma or bronchial hyperresponsiveness in two German pediatric populations. Pediatr. Allergy Immunol. 2005, 16, 40–42. [Google Scholar] [CrossRef] [PubMed]
- Szczepankiewicz, A.; Breborowicz, A.; Sobkowiak, P.; Popiel, A. Polymorphisms of two histamine-metabolizing enzymes genes and childhood allergic asthma: A case control study. Clin. Mol. Allergy 2010, 8, 14. [Google Scholar] [CrossRef] [Green Version]
- Anvari, S.; Vyhlidal, C.A.; Dai, H.; Jones, B.L. Genetic Variation along the Histamine Pathway in Children with Allergic versus Nonallergic Asthma. Am. J. Respir. Cell Mol. Biol. 2015, 53, 802–809. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, Y.; Mizote, H.; Asakawa, T.; Kobayashi, H.; Otani, M.; Tanikawa, K.; Nakamizo, H.; Kawaguchi, C.; Asagiri, K.; Aki-yoshi, K.; et al. Clinical Significance of Plasma Diamine Oxidase Activity in Pediatric Patients: Influence of Nutritional Thera-py and Chemotherapy. Kurume Med. J. 2003, 50, 131–137. [Google Scholar] [CrossRef] [Green Version]
- Forget, P.; Grandfils, C.; Van Cutsem, J.L.; Dandrifosse, G. Diamine Oxidase in Serum and Small Intestinal Biopsy Tissue in Childhood Celiac Disease. J. Pediatr. Gastroenterol. Nutr. 1986, 5, 379–383. [Google Scholar] [CrossRef]
- Forget, P.; Saye, Z.; Van Cutsem, J.L.; Dandrifosse, G. Serum Diamine Oxidase Activity in Acute Gastroenteritis in Children. Pediatr. Res. 1985, 19, 26–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toporowska-Kowalska, E.; Wasowska-Królikowska, K.; Bodalski, J.; Fogel, A.; Kozłowski, W. Diamine oxidase plasma activity and jejunal mucosa integrity in children with protracted diarrhoea. Rocz. Akad. Med. Bialymst. 1995, 40, 499–503. [Google Scholar] [PubMed]
- Caffarelli, C.; Paravati, F.; El Hachem, M.; Duse, M.; Bergamini, M.; Simeone, G.; Barbagallo, M.; Bernardini, R.; Bottau, P.; Bugliaro, F.; et al. Management of chronic urticaria in children: A clinical guideline. Ital. J. Pediatr. 2019, 45, 1–25. [Google Scholar] [CrossRef] [Green Version]
- Kelly, D. Viral Hepatitis in Children. Adv. Exp. Med. Biol. 2004, 549, 83–90. [Google Scholar] [PubMed]
- Rosen, M.J.; Dhawan, A.; Saeed, S.A. Inflammatory Bowel Disease in Children and Adolescents. JAMA Pediatr. 2015, 169, 1053–1060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibranji, A.; Nikolla, E.; Loloci, G.; Mingomataj, E. A case report on transitory histamine intolerance from strawberry intake in a 15 month old child with acute gastroenteritis. Clin. Transl. Allergy 2015, 5, P61. [Google Scholar] [CrossRef] [Green Version]
- Misselwitz, B.; Butter, M.; Verbeke, K.; Fox, M.R. Update on lactose malabsorption and intolerance: Pathogenesis, diagnosis and clinical management. Gut 2019, 68, 2080–2091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Storhaug, C.L.; Fosse, S.K.; Fadnes, L.T. Country, regional, and global estimates for lactose malabsorption in adults: A system-atic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2017, 2, 738–746. [Google Scholar] [CrossRef] [Green Version]
- Enko, D.; Meinitzer, A.; Mangge, H.; Kriegshäuser, G.; Halwachs-Baumann, G.; Reininghaus, E.Z.; Bengesser, S.A.; Schnedl, W.J. Concomitant Prevalence of Low Serum Diamine Oxidase Activity and Carbohydrate Malabsorption. Can. J. Gastroenterol. Hepatol. 2016, 2016, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Forget, P.; Grandfils, C.; Van Cutsem, J.L.; Dandrifosse, G. Diamine Oxidase and Disaccharidase Activities in Small Intestinal Biopsies of Children. Pediatr. Res. 1984, 18, 647–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schnedl, W.J.; Meier-Allard, N.; Lackner, S.; Enko, D.; Mangge, H.; Holasek, S.J. Increasing Expiratory Hydrogen in Lactose Intolerance Is Associated with Additional Food Intolerance/Malabsorption. Nutrients 2020, 12, 3690. [Google Scholar] [CrossRef] [PubMed]
- Amon, U.; Bangha, E.; Kuster, T.; Menne, A.; Vollrath, I.B.; Gibbs, B.F. Enteral histaminosis: Clinical implications. Inflamm. Res. 1999, 48, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Bodmer, S.; Imark, C.; Kneubühl, M. Biogenic amines in foods: Histamine and food processing. Inflamm. Res. 1999, 48, 296–300. [Google Scholar] [CrossRef] [PubMed]
- Missbichler, A.; Mayer, I.; Pongracz, C.; Gabor, F.; Komericki, P. 19 Supplementation of enteric coated diamine oxidase im-proves intestinal degradation of food-borne biogenic amines in case of histamine intolerance. Clin. Nutr. Suppl. 2010, 5, 11. [Google Scholar] [CrossRef]
- del Rio, B.; Redruello, B.; Linares, D.M.; Ladero, V.; Ruas-Madiedo, P.; Fernandez, M.; Martin, M.C.; Alvarez, M.A. The bio-genic amines putrescine and cadaverine show in vitro cytotoxicity at concentrations that can be found in foods. Sci. Rep. 2019, 9, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Muñoz-Esparza, N.C.; Latorre-Moratalla, M.L.; Comas-Basté, O.; Toro-Funes, N.; Veciana-Nogués, M.T.; Vidal-Carou, M.C. Polyamines in Food. Front. Nutr. 2019, 6, 108. [Google Scholar] [CrossRef]
- Centers of Disease Control of Prevention. Available online: https://www.cdc.gov/nutrition/infantandtoddlernutrition/breastfeeding/recommendations-benefits.html (accessed on 20 December 2020).
- Pérez, M.; Ladero, V.; Redruello, B.; Del Rio, B.; Fernández, L.; Rodriguez, J.M.; Martín, M.C.; Fernández, M.; Alvarez, M.A. Mastitis Modifies the Biogenic Amines Profile in Human Milk, with Significant Changes in the Presence of Histamine, Putrescine and Spermine. PLoS ONE 2016, 11, e0162426. [Google Scholar] [CrossRef]
- Pediatric Care Online. Available online: https://pediatriccare.solutions.aap.org/drug-lookup.aspx (accessed on 20 December 2020).
- WHO Expert Committee on the Selection and Use of Essential Medicines. WHO Model List of Essential Medicines for Children; 1st List; World Health Organization: Geneva, Switzerland, 2007; p. 32. [Google Scholar]
- Hoffmann, K.M.; Gruber, E.; Deutschmann, A.; Jahnel, J.; Hauer, A.C. Histamine intolerance in children with chronic ab-dominal pain. Arch. Dis. Child. 2013, 98, 832–833. [Google Scholar] [CrossRef]
- Schnedl, W.J.; Lackner, S.; Enko, D.; Schenk, M.; Holasek, S.J.; Mangge, H. Evaluation of symptoms and symptom combina-tions in histamine intolerance. Intest. Res. 2019, 17, 427–433. [Google Scholar] [CrossRef] [Green Version]
- Manzotti, G.; Breda, D.; Di Gioacchino, M.; Burastero, S.E. Serum diamine oxidase activity in patients with histamine intoler-ance. Int. J. Immunopathol. Pharmacol. 2016, 29, 105–111. [Google Scholar] [CrossRef] [Green Version]
- Pinzer, T.C.; Tietz, E.; Waldmann, E.; Schink, M.; Neurath, M.F.; Zopf, Y. Circadian profiling reveals higher histamine plasma levels and lower diamine oxidase serum activities in 24% of patients with suspected histamine intolerance compared to food allergy and controls. Eur. J. Allergy Clin. Immunol. 2017, 73, 949–957. [Google Scholar] [CrossRef] [Green Version]
- Komericki, P.; Klein, G.; Reider, N.; Hawranek, T.; Strimitzer, T.; Lang, R.; Kranzelbinder, B.; Aberer, W. Histamine intoler-ance: Lack of reproducibility of single symptoms by oral provocation with histamine: A randomised, double-blind, placebo-controlled cross-over study. Wien. Klin. Wochenschr. 2011, 123, 15–20. [Google Scholar] [CrossRef]
- Rosado, J.L. Lactose intolerance. Gac. Med. Mex. 2016, 152, 67–73. [Google Scholar] [PubMed]
- Reese, I.; Ballmer-Weber, B.; Beyer, K.; Fuchs, T.; Kleine-Tebbe, J.; Klimek, L.; Lepp, U.; Niggemann, B.; Saloga, J.; Schäfer, C.; et al. Leitlinie zum Vorgehen bei Verdacht auf Unverträglichkeit gegenüber oral aufgenommenem Histamin. Allergo J. 2017, 26, 51–61. [Google Scholar] [CrossRef]
- Kofler, L.; Ulmer, H.; Kofler, H. Histamine 50-Skin-Prick Test: A Tool to Diagnose Histamine Intolerance. ISRN Allergy 2011, 2011, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, A.; Buczyłko, K.; Zielińska-Bliźniewska, H.; Wagner, W. Impaired resolution of wheals in the skin prick test and low diamine oxidase blood level in allergic patients. Adv. Dermatol. Allergol. 2019, 36, 538–543. [Google Scholar] [CrossRef] [Green Version]
- Comas-Basté, O.; Latorre-Moratalla, M.; Bernacchia, R.; Veciana-Nogués, M.; Vidal-Carou, M. New approach for the diagnosis of histamine intolerance based on the determination of histamine and methylhistamine in urine. J. Pharm. Biomed. Anal. 2017, 145, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Raithel, M.; Ulrich, P.; Keymling, J.; Hahn, E.G. Analysis and topographical distribution of gut diamine oxidase activity in patients with food allergy. Ann. N. Y. Acad. Sci. 1998, 859, 258–261. [Google Scholar] [CrossRef] [PubMed]
- Kuefner, M.A.; Schwelberger, H.G.; Hahn, E.G.; Raithel, M. Decreased Histamine Catabolism in the Colonic Mucosa of Patients with Colonic Adenoma. Dig. Dis. Sci. 2007, 53, 436–442. [Google Scholar] [CrossRef]
- Kuefner, M.A.; Schwelberger, H.G.; Weidenhiller, M.; Hahn, E.G.; Raithel, M. Both catabolic pathways of histamine via his-tamine-N-melhyl-transferase and diamine oxidase are diminished in the colonic mucosa of patients with food allergy. Inflamm. Res. 2004, 53, S31–S32. [Google Scholar] [PubMed]
- Raithel, M.; Küfner, M.; Ulrich, P.; Hahn, E.G. The involvement of the histamine degradation pathway by diamine oxidase in manifest gastrointestinal allergies. Inflamm. Res. 1999, 48, 75–76. [Google Scholar] [CrossRef] [PubMed]
- Lessof, M.H.; Gant, V.; Hinuma, K.; Murphy, G.M.; Dowling, R.H. Recurrent urticaria and reduced diamine oxidase activity. Clin. Exp. Allergy 1990, 20, 373–376. [Google Scholar] [CrossRef] [PubMed]
- Schnedl, W.J.; Schenk, M.; Lackner, S.; Enko, D.; Mangge, H.; Forster, F. Diamine oxidase supplementation improves symp-toms in patients with histamine intolerance. Food Sci. Biotechnol. 2019, 28, 1779–1784. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Food | Histamine Content: Mean [mg/kg] | Histamine Content: Range [mg/kg] |
|---|---|---|
| Water | - | - |
| Coffee | - | - |
| Tea | - | - |
| Bread | ND | - |
| Cereals | ND | - |
| Oats | ND | - |
| Pasta | ND | - |
| Rice | ND | - |
| Yoghurt | ND | - |
| Asparagus | 0.34 | ND–1.42 |
| Beans | ND | - |
| Broccoli | ND | - |
| Carrot | ND | - |
| Cauliflower | ND | - |
| Courgette | ND | - |
| Cucumber | ND | - |
| Lettuce | ND | - |
| Mushroom | ND | - |
| Onion | ND | - |
| Potatoes | ND | - |
| Pumpkin | 0.28 | ND–1.90 |
| Apple | ND | - |
| Banana | ND | - |
| Cherry | ND | - |
| Peach | ND | - |
| Pineapple | ND | - |
| Plum | ND | - |
| Grapefruit juice | 0.31 | ND–1.74 |
| Orange juice | 0.46 | ND–1.32 |
| Pineapple juice | 2.44 | ND–4.61 |
| Herbs and spices | ND | - |
| Pepper | ND | - |
| Vegetable oil | - | - |
| Vinegar | - | - |
| Olives | - | - |
| Fresh meat | ND | - |
| Cooked meat | 0.3 | ND–4.8 |
| Poultry | 3 | - |
| Mozzarella | ND | - |
| Cream cheese | 3 | - |
| Food | Histamine Content: Mean [mg/kg] | Histamine Content: Range [mg/kg] |
|---|---|---|
| Cod (fresh) | - | 2–77 |
| Tuna (frozen) | ND | - |
| Tuna (smoked or salted) | ND | - |
| Tuna (canned) | 0.33 | 1–402 |
| Mackerel (frozen) | - | 1–20 |
| Mackerel (smoked or salted) | - | 1–1788 |
| Mackerel (canned) | - | ND–210 |
| Herring (frozen) | - | od 1 do 4 |
| Herring (smoked or salted) | - | 5–121 |
| Herring (canned) | - | 1–479 |
| Sardine (frozen) | ND | - |
| Sardine (smoked or salted) | - | 14–150 |
| Sardine (canned) | - | 3–2000 |
| Shellfish/Shrimp paste | 328 | - |
| Fish sauce | 574.7 | - |
| Parma ham | 1100 | - |
| Sobrassada/Soppresata | 21.9 | - |
| Saucisson | 71 | - |
| Salami | - | 1–654 |
| Fermented ham | - | 38–271 |
| Fermented sousage | 21.9 | ND–650 |
| Parmesan (cheese) | 40.64 | 10–581 |
| Blue cheese | 376.6 | - |
| Gouda (cheese) | - | 10–900 |
| Emmental (cheese) | - | 5–2500 |
| Roquefort (cheese) | 9.9 | - |
| Camembert (cheese) | - | 0–1000 |
| Cheddar (cheese) | - | 0–2100 |
| Sauerkraut/fermented cabbage | 37 | 0–229 |
| Soy derivatives | 307 | ND–307 |
| Chocolate | 0.58 | - |
| Vanilla | - | - |
| Citrus | - | - |
| Kiwi | ND | - |
| Nuts | 0.45 | ND–11.86 |
| Strawberry (dry) | - | - |
| Pineapple (dry) | - | - |
| Papaya (dry) | - | - |
| Spinach | 31.77 | 9.46–69.71 |
| Tomato (fresh and sauce) | 22 | ND–22 |
| Eggplant | 39.42 | 4.17–100.6 |
| Eggs | - | - |
| Type of Drug/Substance | Example |
|---|---|
| Contrast media | - |
| Muscle relaxants | Pancurorium, alcuronium, D-tubocurarine |
| Anaesthetics | Thiopental |
| Analgesics | Morphine, pethidine, NSAIDs, ASA, metamizole |
| Local anaesthetics | Prilocaine |
| Cardiotonics | Dobutamine, dopamine |
| Antihypertensives | Verapamil, alprenolol, dihydrazine |
| Antiarrhythmics | Propafenone |
| Diuretics | Amiloride |
| Antibiotics | Cefuroxime, isoniazid, pentamidine, clavulanate, chloroquine |
| Mucolytics | Ambroxol, acetylcysteine |
| Bronchodilators | Aminophylline |
| Cytostatics | Cyclophosphamide |
| Antidepressants | Amitriptyline |
| Prokinetics | Metoclopramide |
| Antihistamines | Cimetidine |
| Clinical Outcome | Number of Patients | |
|---|---|---|
| Rosell-Camps et al. [7] | Hoffman et al. [42] | |
| Abdominal pain | 16 (100%) | 31 (100%) |
| DAO deficit | 14 (87.5%) | 31 (100%) |
| Males | 11 (68.8%) | 17 (54.8%) |
| DAO deficit and positive response to histamine-reduced diet | 14 (100%) | 16 (43.2%) |
| High serum histamine level | 1 out of 8 measured (12.5%) | 22 (71.0%) |
| High urine histamine level | 1 out of 8 measured (12.5%) | 13 (41.2%) |
| Must-Have Criteria |
| Presenting ≥ 3 symptoms of histamine intolerance in total or ≥2 gastrointestinal symptoms |
| ≥2 Major criteria |
| Positive histamine oral provocation test |
| OR |
| positive 50-skin-prick test when other possible pathologies giving positive result are excluded |
| serum DAO deficit (≤10 IU/mL) |
| OR |
| symptoms improvement after DAO supplementation (4–8 weeks) |
| OR |
| symptoms improvement after DAO inhibitory drugs dismission |
| OR |
| identification of single nucleotide polymorphism responsible for DAO/HNMT deficit |
| OR |
| decreased DAO activity in colon biopsy |
| Symptoms improvement after histamine-reduced diet (4–8 weeks) |
| Additional criteria that increase the probability of histamine intolerance diagnosis |
| Correlation between specific food |
| consumption and symptomatology based on a diet diary |
| High concentration biomarkers of histamine metabolism in urine, blood or stool samples |
| Exclusion of mastocytosis (tryptase) |
| Exclusion of food allergies (skin prick test) |
| Exclusion or confirmation of other underlying diseases relevant to presented symptoms |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nazar, W.; Plata-Nazar, K.; Sznurkowska, K.; Szlagatys-Sidorkiewicz, A. Histamine Intolerance in Children: A Narrative Review. Nutrients 2021, 13, 1486. https://doi.org/10.3390/nu13051486
Nazar W, Plata-Nazar K, Sznurkowska K, Szlagatys-Sidorkiewicz A. Histamine Intolerance in Children: A Narrative Review. Nutrients. 2021; 13(5):1486. https://doi.org/10.3390/nu13051486
Chicago/Turabian StyleNazar, Wojciech, Katarzyna Plata-Nazar, Katarzyna Sznurkowska, and Agnieszka Szlagatys-Sidorkiewicz. 2021. "Histamine Intolerance in Children: A Narrative Review" Nutrients 13, no. 5: 1486. https://doi.org/10.3390/nu13051486
APA StyleNazar, W., Plata-Nazar, K., Sznurkowska, K., & Szlagatys-Sidorkiewicz, A. (2021). Histamine Intolerance in Children: A Narrative Review. Nutrients, 13(5), 1486. https://doi.org/10.3390/nu13051486