
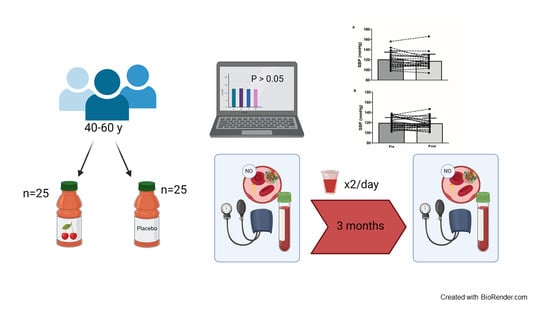
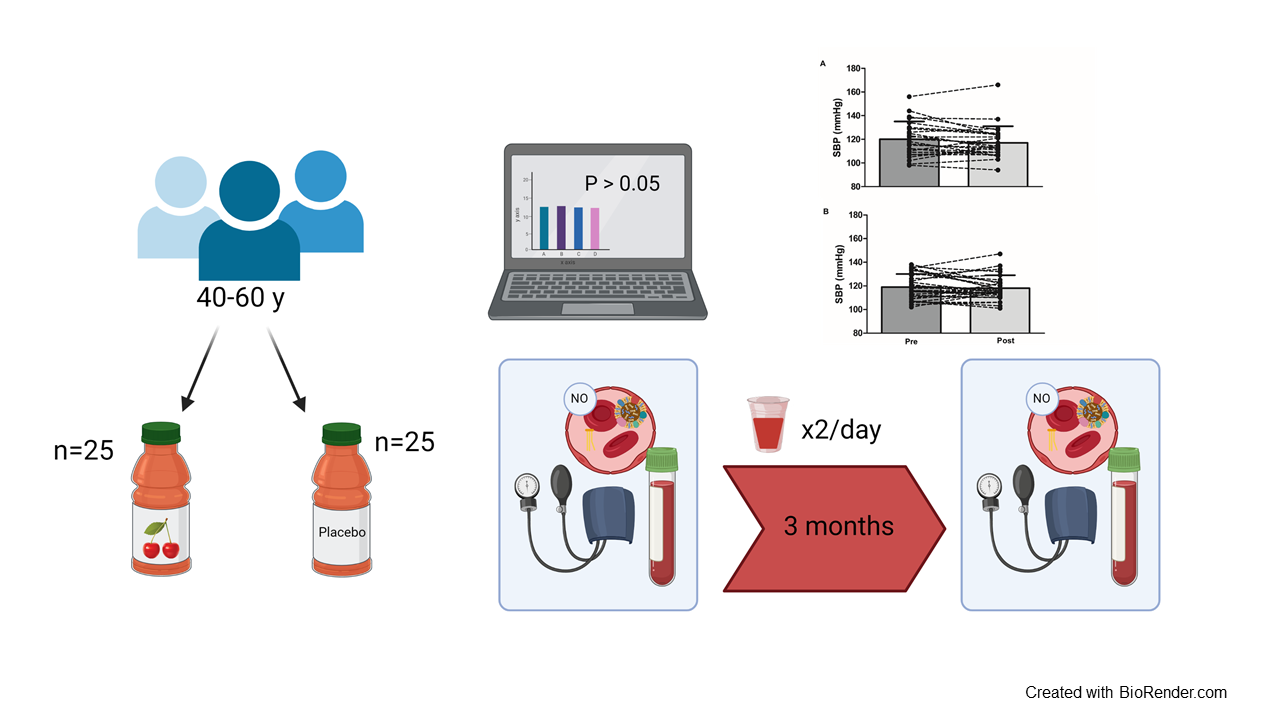
The Influence of Tart Cherry (Prunus cerasus, cv Montmorency) Concentrate Supplementation for 3 Months on Cardiometabolic Risk Factors in Middle-Aged Adults: A Randomised, Placebo-Controlled Trial




Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Dietary Intervention
2.4. Anthropometry and Aerobic Capacity
2.5. Vascular Function
2.6. Haematological Samples
2.7. Power Calculation and Statistical Analysis
3. Results
3.1. Physical Activity, Diet, and Body Composition
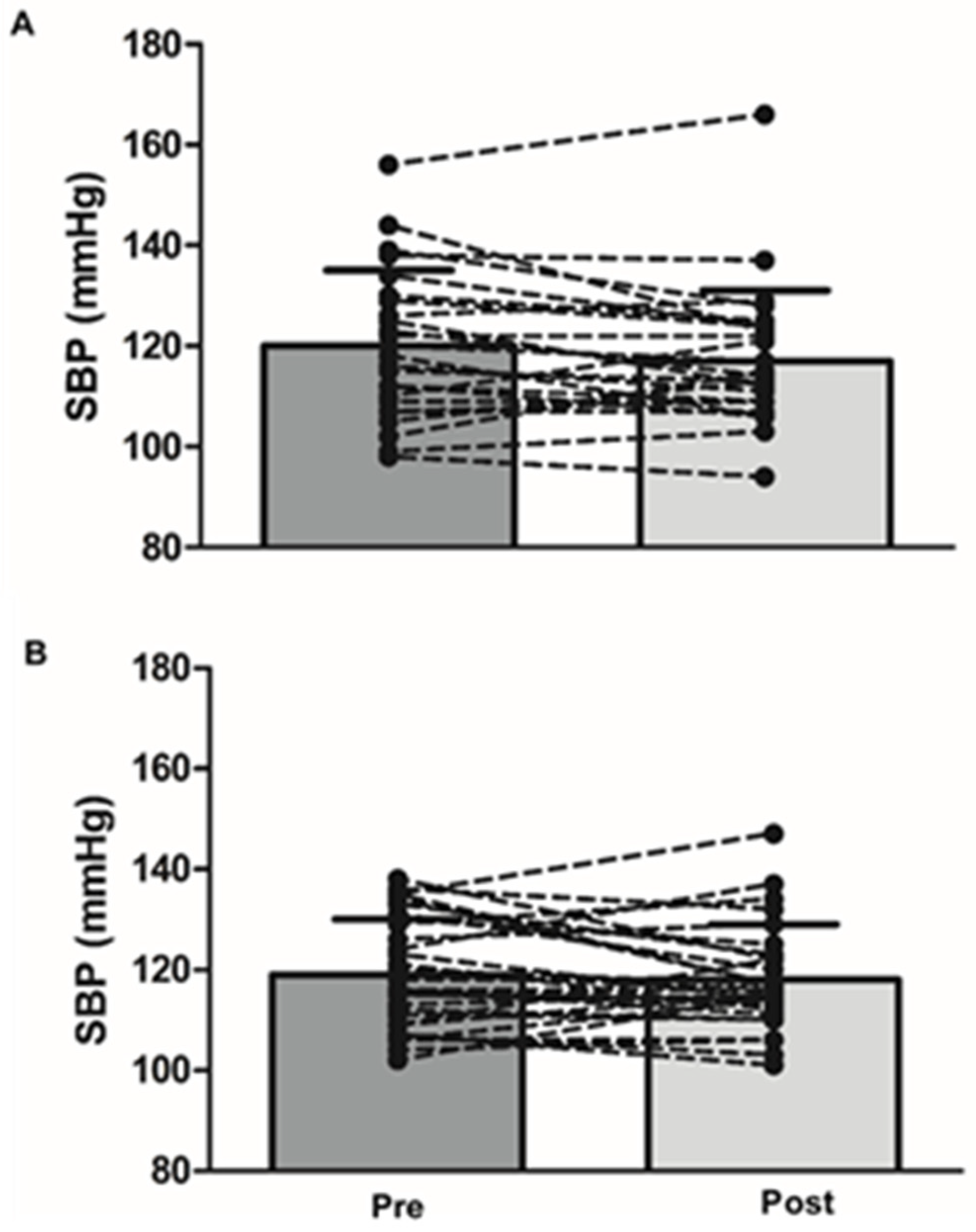
3.2. Influence of MC on Vascular Function
3.3. Influence of MC on Metabolic Health Indices
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. World Health Statistics 2019: Monitoring Health for the SDGs Sustainable Development Goals; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Danaei, G.; Lu, Y.; Singh, G.; Stevens, G.; Cowan, M.; Farzadfar, F.; Lin, J.; Finucane, M.; Rao, M.; Khang, Y. Cardiovascular disease, chronic kidney disease, and diabetes mortality burden of cardiometabolic risk factors from 1980 to 2010: A comparative risk assessment. Lancet 2014, 2, 634–647. [Google Scholar]
- Houston, M. The role of noninvasive cardiovascular testing, applied clinical nutrition and nutritional supplements in the prevention and treatment of coronary heart disease. Ther. Adv. Cardiovasc. Dis. 2018, 12, 85–108. [Google Scholar] [CrossRef]
- Seals, D.R.; Jablonski, K.L.; Donato, A.J. Aging and vascular endothelial function in humans. Clin. Sci. 2011, 120, 357–375. [Google Scholar] [CrossRef]
- Pandey, A.; Patel, M.R.; Willis, B.; Gao, A.; Leonard, D.; Das, S.R.; Defina, L.; Berry, J.D. Association between midlife cardiorespiratory fitness and risk of stroke: The Cooper Center Longitudinal Study. Stroke 2016, 47, 1720–1726. [Google Scholar] [CrossRef]
- Samieri, C.; Sun, Q.; Townsend, M.K.; Rimm, E.B.; Grodstein, F. Dietary flavonoid intake at midlife and healthy aging in women. Am. J. Clin. Nutr. 2014, 100, 1489–1497. [Google Scholar] [CrossRef]
- King, D.E.; Mainous, A.G., III; Geesey, M.E. Turning back the clock: Adopting a healthy lifestyle in middle age. Am. J. Med. 2007, 120, 598–603. [Google Scholar] [CrossRef]
- Allen, N.; Berry, J.D.; Ning, H.; Van Horn, L.; Dyer, A.; Lloyd-Jones, D.M. Impact of blood pressure and blood pressure change during middle age on the remaining lifetime risk for cardiovascular disease: The cardiovascular lifetime risk pooling project. Circulation 2012, 125, 37–44. [Google Scholar] [CrossRef]
- Odegaard, A.O.; Jacobs, D.R.; Sanchez, O.A.; Goff, D.C.; Reiner, A.P.; Gross, M.D. Oxidative stress, inflammation, endothelial dysfunction and incidence of type 2 diabetes. Cardiovasc. Diabetol. 2016, 15, 1–12. [Google Scholar] [CrossRef]
- Wallace, T.; Slavin, M.; Frankenfeld, C. Systematic Review of Anthocyanins and Markers of Cardiovascular Disease. Nutrients 2016, 8, 32. [Google Scholar] [CrossRef]
- Lynn, A.; Mathew, S.; Moore, C.T.; Russell, J.; Robinson, E.; Soumpasi, V.; Barker, M.E. Effect of a Tart Cherry Juice Supplement on Arterial Stiffness and Inflammation in Healthy Adults: A Randomised Controlled Trial. Plant Foods Hum. Nutr. 2014, 69, 122–127. [Google Scholar] [CrossRef]
- Martin, K.R.; Burrell, L.; Bopp, J. Authentic tart cherry juice reduces markers of inflammation in overweight and obese subjects: A randomized, crossover pilot study. Food Funct. 2018, 9, 5290–5300. [Google Scholar] [CrossRef]
- Keane, K.M.; George, T.W.; Constantinou, C.L.; Brown, M.A.; Clifford, T.; Howatson, G. Effects of Montmorency tart cherry (Prunus Cerasus L.) consumption on vascular function in men with early hypertension. Am. J. Clin. Nutr. 2016, 103, 1531–1539. [Google Scholar] [CrossRef]
- Chai, S.C.; Davis, K.; Wright, R.S.; Kuczmarski, M.F.; Zhang, Z. Impact of tart cherry juice on systolic blood pressure and low-density lipoprotein cholesterol in older adults: A randomized controlled trial. Food Funct. 2018, 9, 3185–3194. [Google Scholar] [CrossRef]
- Desai, T.; Roberts, M.; Bottoms, L. Effects of Montmorency tart cherry supplementation on cardio-metabolic markers in metabolic syndrome participants: A pilot study. J. Funct. Foods 2019, 57, 286–298. [Google Scholar] [CrossRef]
- Kirakosyan, A.; Seymour, E.; Llanes, D.E.U.; Kaufman, P.B.; Bolling, S.F. Chemical profile and antioxidant capacities of tart cherry products. Food Chem. 2009, 115, 20–25. [Google Scholar] [CrossRef]
- Kimble, R.; Keane, K.M.; Lodge, J.K.; Howatson, G. Dietary intake of anthocyanins and risk of cardiovascular disease: A systematic review and meta-analysis of prospective cohort studies. Crit. Rev. Food Sci. Nutr. 2018, 59, 3032–3043. [Google Scholar] [CrossRef]
- Tresserra-Rimbau, A.; Rimm, E.B.; Medina-Remón, A.; Martínez-González, M.A.; de la Torre, R.; Corella, D.; Salas-Salvadó, J.; Gómez-Gracia, E.; Lapetra, J.; Arós, F.; et al. Inverse association between habitual polyphenol intake and incidence of cardiovascular events in the PREDIMED study. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 639–647. [Google Scholar] [CrossRef]
- Adriouch, S.; Lampuré, A.; Nechba, A.; Baudry, J.; Assmann, K.; Kesse-Guyot, E.; Hercberg, S.; Scalbert, A.; Touvier, M.; Fezeu, L. Prospective Association between Total and Specific Dietary Polyphenol Intakes and Cardiovascular Disease Risk in the Nutrinet-Santé French Cohort. Nutrients 2018, 10, 1587. [Google Scholar] [CrossRef]
- Igwe, E.; Charlton, K.; Probst, Y. Usual dietary anthocyanin intake, sources and their association with blood pressure in a representative sample of Australian adults. J. Hum. Nutr. Diet. 2019, 32, 578–590. [Google Scholar] [CrossRef]
- Keane, K.M.; Bell, P.G.; Lodge, J.K.; Constantinou, C.L.; Jenkinson, S.E.; Bass, R.; Howatson, G. Phytochemical uptake following human consumption of Montmorency tart cherry (L. Prunus cerasus) and influence of phenolic acids on vascular smooth muscle cells in vitro. Eur. J. Nutr. 2016, 55, 1695–1705. [Google Scholar] [CrossRef]
- Edwards, M.; Czank, C.; Woodward, G.M.; Cassidy, A.; Kay, C.D. Phenolic Metabolites of Anthocyanins Modulate Mechanisms of Endothelial Function. J. Agric. Food Chem. 2015, 63, 2423–2431. [Google Scholar] [CrossRef]
- Rodriguez-Mateos, A.; Istas, G.; Boschek, L.; Feliciano, R.P.; Mills, C.E.; Boby, C.; Gomez-Alonso, S.; Milenkovic, D.; Heiss, C. Circulating Anthocyanin Metabolites Mediate Vascular Benefits of Blueberries: Insights From Randomized Controlled Trials, Metabolomics, and Nutrigenomics. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2019, 74, 967–976. [Google Scholar] [CrossRef]
- Kirakosyan, A.; Seymour, E.M.; Noon, K.R.; Llanes, D.E.U.; Kaufman, P.B.; Warber, S.L.; Bolling, S.F. Interactions of antioxidants isolated from tart cherry (Prunus cerasus) fruits. Food Chem. 2010, 122, 78–83. [Google Scholar] [CrossRef]
- Lear, R.; O’Leary, M.; O’Brien Andersen, L.; Holt, C.C.; Stensvold, C.R.; van der Giezen, M.; Bowtell, J.L. Tart Cherry Concentrate Does Not Alter the Gut Microbiome, Glycaemic Control or Systemic Inflammation in a Middle-Aged Population. Nutrients 2019, 11, 1063. [Google Scholar] [CrossRef] [PubMed]
- Aboo-Bakkar, Z.; Fulford, J.; Gates, P.E.; Jackman, S.R.; Jones, A.M.; Bond, B.; Bowtell, J.L. Montmorency cherry supplementation attenuates vascular dysfunction induced by prolonged forearm occlusion in overweight, middle-aged men. J. Appl. Physiol. 2018, 126, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.A.; Navaei, N.; Pourafshar, S.; Jaime, S.J.; Akhavan, N.S.; Alvarez-Alvarado, S.; Proaño, G.V.; Litwin, N.S.; Clark, E.A.; Foley, E.M.; et al. Effects of Montmorency Tart Cherry Juice Consumption on Cardiometabolic Biomarkers in Adults with Metabolic Syndrome: A Randomized Controlled Pilot Trial. J. Med. Food 2020, 23, 1238–1247. [Google Scholar] [CrossRef] [PubMed]
- Ekoé, J.-M.; Punthakee, Z.; Ransom, T.; Prebtani, A.P.; Goldenberg, R. Screening for Type 1 and Type 2 Diabetes. Can. J. Diabetes 2013, 37, S12–S15. [Google Scholar] [CrossRef][Green Version]
- Lindström, J.; Tuomilehto, J. The Diabetes Risk Score: A practical tool to predict type 2 diabetes risk. Diabetes Care 2003, 26, 725–731. [Google Scholar] [CrossRef]
- Keane, K.M.; Haskell-Ramsay, C.F.; Veasey, R.C.; Howatson, G. Montmorency Tart cherries (Prunus cerasus L.) modulate vascular function acutely, in the absence of improvement in cognitive performance. Br. J. Nutr. 2016, 116, 1935–1944. [Google Scholar] [CrossRef]
- Neveu, V.; Perez-Jimenez, J.; Vos, F.; Crespy, V.; Du Chaffaut, L.; Mennen, L.; Knox, C.; Eisner, R.; Cruz, J.; Wishart, D.; et al. Phenol-Explorer: An online comprehensive database on polyphenol contents in foods. Database 2010, 2010, bap024. [Google Scholar] [CrossRef]
- Losso, J.N.; Finley, J.W.; Karki, N.; Liu, A.G.; Prudente, A.; Tipton, R.; Yu, Y.; Greenway, F.L. Pilot Study of the Tart Cherry Juice for the Treatment of Insomnia and Investigation of Mechanisms. Am. J. Ther. 2017, 25, e194–e201. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E.; Kosinski, M. Interpreting SF&-36 summary health measures: A response. Qual. Life Res. 2001, 10, 405–413. [Google Scholar] [CrossRef]
- Noonan, V.; Dean, E. Submaximal Exercise Testing: Clinical Application and Interpretation. Phys. Ther. 2000, 80, 782–807. [Google Scholar] [CrossRef]
- Astrand, I. Aerobic Work Capacity in Men and Women: With Special Reference to Age; Norstedt: Stockholm, Sweden, 1960. [Google Scholar]
- Kimble, R.; Keane, K.; Lodge, J.; Howatson, G. Methodological Considerations for a Vascular Function Test Battery. Int. J. Sports Med. 2019, 40, 601–608. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, E.; Asmar, R.; Beilin, L.; Imai, Y.; Mallion, J.-M.; Mancia, G.; Mengden, T.; Myers, M.; Padfield, P.; Palatini, P.; et al. European Society of Hypertension recommendations for conventional, ambulatory and home blood pressure measurement. J. Hypertens. 2003, 21, 821–848. [Google Scholar] [CrossRef]
- Pickering, T.G.; Hall, J.E.; Appel, L.J.; Falkner, B.E.; Graves, J.; Hill, M.N.; Jones, D.W.; Kurtz, T.; Sheps, S.G.; Roccella, E.J. Recommendations for blood pressure measurement in humans and experimental animals: Part 1: Blood pressure measurement in humans: A statement for professionals from the Subcommittee of Professional and Public Education of the American Heart Association Council on High Blood Pressure Research. Circulation 2005, 111, 697–716. [Google Scholar]
- Pauca, A.L.; O’Rourke, M.F.; Kon, N.D. Prospective Evaluation of a Method for Estimating Ascending Aortic Pressure From the Radial Artery Pressure Waveform. Hypertension 2001, 38, 932–937. [Google Scholar] [CrossRef]
- Wilkinson, I.B.; Maccallum, H.; Flint, L.; Cockcroft, J.R.; Newby, D.E.; Webb, D.J. The influence of heart rate on augmentation index and central arterial pressure in humans. J. Physiol. 2000, 525, 263–270. [Google Scholar] [CrossRef]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the Concentration of Low-Density Lipoprotein Cholesterol in Plasma, Without Use of the Preparative Ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Matthews, D.; Hosker, J.; Rudenski, A.; Naylor, B.; Treacher, D.; Turner, R. Homeostasis model assessment: Insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Makai, P.; IntHout, J.; Deinum, J.; Jenniskens, K.; Van Der Wilt, G.J. A Network Meta-Analysis of Clinical Management Strategies for Treatment-Resistant Hypertension: Making Optimal Use of the Evidence. J. Gen. Intern. Med. 2017, 32, 921–930. [Google Scholar] [CrossRef]
- Vickers, A.J.; Altman, D.G. Analysing controlled trials with baseline and follow up measurements. BMJ 2001, 323, 1123–1124. [Google Scholar] [CrossRef] [PubMed]
- Seymour, E.M.; Warber, S.M.; Kirakosyan, A.; Noon, K.R.; Gillespie, B.; Uhley, V.E.; Wunder, J.; Urcuyo, D.E.; Kaufman, P.B.; Bolling, S.F. Anthocyanin pharmacokinetics and dose-dependent plasma antioxidant pharmacodynamics following whole tart cherry intake in healthy humans. J. Funct. Foods 2014, 11, 509–516. [Google Scholar] [CrossRef]
- Desai, T.; Roberts, M.; Bottoms, L. Effects of short-term continuous Montmorency tart cherry juice supplementation in participants with metabolic syndrome. Eur. J. Nutr. 2020, 1–17. [Google Scholar] [CrossRef]
- LaRochelle, P.; Du Souich, P.; Hamet, P.; Larocque, P.; Armstrong, J. Prazosin plasma concentration and blood pressure reduction. Hypertension 1982, 4, 93–101. [Google Scholar] [CrossRef]
- Kent, K.; Charlton, K.; Roodenrys, S.; Batterham, M.; Potter, J.; Traynor, V.; Gilbert, H.; Morgan, O.; Richards, R. Consumption of anthocyanin-rich cherry juice for 12 weeks improves memory and cognition in older adults with mild-to-moderate dementia. Eur. J. Nutr. 2017, 56, 333–341. [Google Scholar] [CrossRef]
- Istas, G.; Wood, E.; Le Sayec, M.; Rawlings, C.; Yoon, J.; Dandavate, V.; Cera, D.; Rampelli, S.; Costabile, A.; Fromentin, E.; et al. Effects of aronia berry (poly)phenols on vascular function and gut microbiota: A double-blind randomized controlled trial in adult men. Am. J. Clin. Nutr. 2019, 110, 316–329. [Google Scholar] [CrossRef] [PubMed]
- Krga, I.; Milenkovic, D.; Morand, C.; Monfoulet, L.-E. An update on the role of nutrigenomic modulations in mediating the cardiovascular protective effect of fruit polyphenols. Food Funct. 2016, 7, 3656–3676. [Google Scholar] [CrossRef] [PubMed]
- Crispi, S.; Filosa, S.; Di Meo, F. Polyphenols-gut microbiota interplay and brain neuromodulation. Neural Regen. Res. 2018, 13, 2055–2059. [Google Scholar] [CrossRef]
- Barrera-Reyes, P.K.; De Lara, J.C.-F.; González-Soto, M.; Tejero, M.E. Effects of Cocoa-Derived Polyphenols on Cognitive Function in Humans. Systematic Review and Analysis of Methodological Aspects. Plant Foods Hum. Nutr. 2020, 75, 1–11. [Google Scholar] [CrossRef]
- Mariat, D.; Firmesse, O.; Levenez, F.; Guimaraes, V.; Sokol, H.; Dore, J.; Corthier, G.; Furet, J. The Firmicutes/Bacteroidetes ratio of the human microbiota changes with age. BMC Microbiol. 2009, 9, 123. [Google Scholar] [CrossRef]
- De La Cuesta-Zuluaga, J.; Kelley, S.T.; Chen, Y.; Escobar, J.S.; Mueller, N.T.; Ley, R.E.; McDonald, D.; Huang, S.; Swafford, A.D.; Knight, R.; et al. Age- and Sex-Dependent Patterns of Gut Microbial Diversity in Human Adults. Msystems 2019, 4, e00261-19. [Google Scholar] [CrossRef]
- Vendrame, S.; Klimis-Zacas, D. Potential Factors Influencing the Effects of Anthocyanins on Blood Pressure Regulation in Humans: A Review. Nutrients 2019, 11, 1431. [Google Scholar] [CrossRef]
- Desai, T.; Bottoms, L.; Roberts, M. The effects of Montmorency tart cherry juice supplementation and FATMAX exercise on fat oxidation rates and cardio-metabolic markers in healthy humans. Graefe’s Arch. Clin. Exp. Ophthalmol. 2018, 118, 2523–2539. [Google Scholar] [CrossRef]
- Mattace-Raso, F.U.; van der Cammen, T.J.; Hofman, A.; van Popele, N.M.; Bos, M.L.; Schalekamp, M.A.; Asmar, R.; Reneman, R.S.; Hoeks, A.P.; Breteler, M.M. Arterial stiffness and risk of coronary heart disease and stroke: The Rotterdam Study. Circulation 2006, 113, 657–663. [Google Scholar] [CrossRef]
- Osborne, B.; Cooper, V. Health Survey for England 2017 Adult Health Related Behaviours. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/health-survey-for-england/2017 (accessed on 15 March 2019).
- Dohadwala, M.M.; Holbrook, M.; Hamburg, N.M.; Shenouda, S.M.; Chung, W.B.; Titas, M.; Kluge, M.A.; Wang, N.; Palmisano, J.; Milbury, P.E.; et al. Effects of cranberry juice consumption on vascular function in patients with coronary artery disease. Am. J. Clin. Nutr. 2011, 93, 934–940. [Google Scholar] [CrossRef]
- Zhu, Y.; Xia, M.; Yang, Y.; Liu, F.; Li, Z.; Hao, Y.; Mi, M.; Jin, T.; Ling, W. Purified anthocyanin supplementation improves endothelial function via NO-cGMP activation in hypercholesterolemic individuals. Clin. Chem. 2011, 57, 1524–1533. [Google Scholar] [CrossRef]
- Chou, E.J.; Keevil, J.G.; Aeschlimann, S.; Wiebe, D.A.; Folts, J.D.; Stein, J.H. Effect of ingestion of purple grape juice on endothelial function in patients with coronary heart disease. Am. J. Cardiol. 2001, 88, 553–555. [Google Scholar] [CrossRef]
- Ataie-Jafari, A.; Hosseini, S.; Karimi, F.; Pajouhi, M. Effects of sour cherry juice on blood glucose and some cardiovascular risk factors improvements in diabetic women: A pilot study. Nutr. Food Sci. 2008, 38, 355–360. [Google Scholar] [CrossRef]
- Martin, K.R.; Coles, K.M. Consumption of 100% Tart Cherry Juice Reduces Serum Urate in Overweight and Obese Adults. Curr. Dev. Nutr. 2019, 3, nzz011. [Google Scholar] [CrossRef]
- Schumacher, H.R.; Pullman-Mooar, S.; Gupta, S.R.; Dinnella, J.E.; Kim, R.; McHugh, M.P. Randomized double-blind crossover study of the efficacy of a tart cherry juice blend in treatment of osteoarthritis (OA) of the knee. Osteoarthr. Cartil. 2013, 21, 1035–1041. [Google Scholar] [CrossRef]
- Vendrame, S.; Del Bo’, C.; Ciappellano, S.; Riso, P.; Klimis-Zacas, D. Berry Fruit Consumption and Metabolic Syndrome. Antioxidants 2016, 5, 34. [Google Scholar] [CrossRef] [PubMed]
- Wedick, N.M.; Pan, A.; Cassidy, A.; Rimm, E.B.; Sampson, L.; Rosner, B.; Willett, W.; Hu, F.B.; Sun, Q.; Van Dam, R.M. Dietary flavonoid intakes and risk of type 2 diabetes in US men and women. Am. J. Clin. Nutr. 2012, 95, 925–933. [Google Scholar] [CrossRef] [PubMed]
- Jennings, A.; Welch, A.A.; Spector, T.; MacGregor, A.; Cassidy, A. Intakes of Anthocyanins and Flavones Are Associated with Biomarkers of Insulin Resistance and Inflammation in Women. J. Nutr. 2014, 144, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Olendzki, B.C.; Li, W.; Hafner, A.R.; Chiriboga, D.; Hebert, J.R.; Campbell, M.; Sarnie, M.; Ockene, I.S. Seasonal variation in food intake, physical activity, and body weight in a predominantly overweight population. Eur. J. Clin. Nutr. 2006, 60, 519–528. [Google Scholar] [CrossRef] [PubMed]
- DiMeglio, D.P.; Mattes, R.D. Liquid versus solid carbohydrate: Effects on food intake and body weight. Int. J. Obes. 2000, 24, 794–800. [Google Scholar] [CrossRef] [PubMed]
- Dodier, T.; Anderson, K.L.; Bothwell, J.; Hermann, J.; Lucas, E.A.; Smith, B.J.U.S. Montmorency Tart Cherry Juice Decreases Bone Resorption in Women Aged 65–80 Years. Nutrients 2021, 13, 544. [Google Scholar] [CrossRef]
- Johnson, S.A.; Figueroa, A.; Navaei, N.; Wong, A.; Kalfon, R.; Ormsbee, L.T.; Feresin, R.G.; Elam, M.L.; Hooshmand, S.; Payton, M.E.; et al. Daily Blueberry Consumption Improves Blood Pressure and Arterial Stiffness in Postmenopausal Women with Pre- and Stage 1-Hypertension: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. J. Acad. Nutr. Diet. 2015, 115, 369–377. [Google Scholar] [CrossRef]
- Sabou, V.R.; O’Leary, M.F.; Liu, Y.; Brown, P.N.; Murch, S.; Bowtell, J.L. Review of Analytical Methods and Reporting of the Polyphenol Content of Tart Cherry Supplements in Human Supplementation Studies Investigating Health and Exercise Performance Effects: Recommendations for Good Practice. Front. Nutr. 2021, 8. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
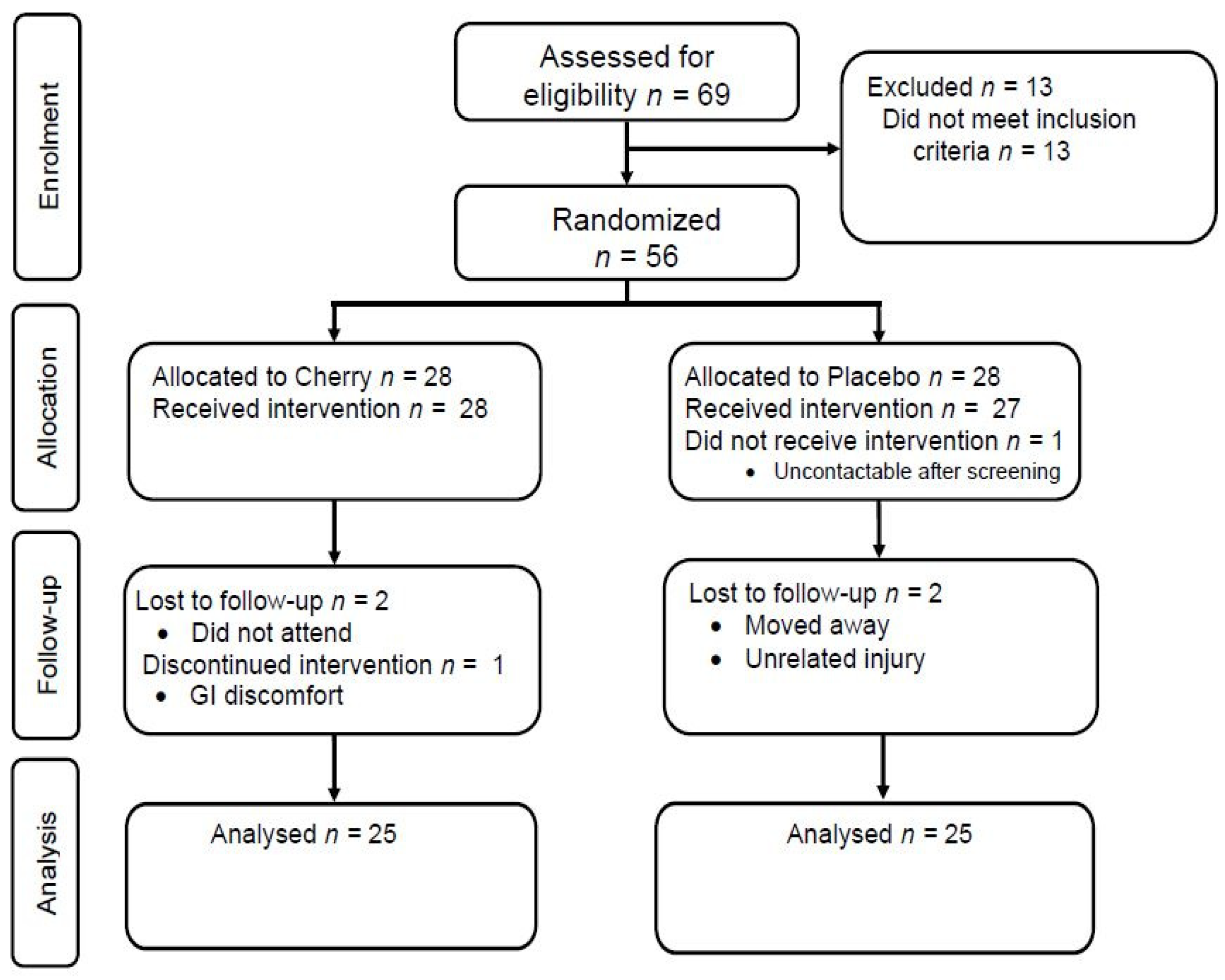
| Characteristic | All (n = 56) | Cherry (n = 28) | Placebo (n = 28) | p-Value |
|---|---|---|---|---|
| Age (y) | 48 ± 6 | 49 ± 6 | 47 ± 6 | 0.160 |
| Sex (m/f) | 37/19 | 19/9 | 18/10 | 0.778 |
| Stature (cm) | 173.1 ± 8.8 | 173.7 ± 8.9 | 172.4 ± 9.0 | 0.494 |
| Body Mass (kg) | 81.8 ± 12.9 | 81.7 ± 14.0 | 82.0 ± 11.9 | 0.793 |
| BMI (kg/m2) | 27.3 ± 3.7 | 27.0 ± 3.8 | 27.4 ± 3.7 | 0.569 |
| Ethnicity (n; %) | 0.368 | |||
| White | 54 (96.4) | 27 (96.4) | 27 (96.4) | |
| Education (n; %) | 0.798 | |||
| Less Than High School | − | − | − | |
| High School or Equivalent | 24 (43) | 11 (39) | 13 (46) | |
| Bachelor’s Degree | 19 (34) | 9 (32) | 10 (36) | |
| Postgraduate Degree | 13 (23) | 8 (29) | 5 (18) | |
| Medication (n; %) | 17 (30) | 10 (36) | 7 (25) | 0.771 |
| Cherry | Placebo | ANOVA | |||
|---|---|---|---|---|---|
| Treatment | Time | Interaction | |||
| METs (min/week) | |||||
| Baseline | 2462 ± 2038 | 1953 ± 1527 | 0.267 | 0.959 | 0.961 |
| 3 months | 2464 ± 2336 | 1978 ± 1217 | |||
| Sitting time (h) | |||||
| Baseline | 6.6 ± 3.1 | 6.7 ± 3.0 | 0.856 | 0.852 | 0.486 |
| 3 months | 6.7 ± 2.8 | 6.3 ± 3.0 | |||
| V̇O2 max (mL·kg−1·min−1) | |||||
| Baseline | 35.9 ± 11.1 | 37.3 ± 7.5 | 0.319 | 0.187 | 0.386 |
| 3 months | 33.7 ± 9.6 | 37.1 ± 6.2 | |||
| Energy (Kcal) | |||||
| Baseline | 1921 ± 340 | 1896 ± 439 | 0.997 | 0.212 | 0.673 |
| 3 months | 1977 ± 439 | 2001 ± 423 | |||
| Carbohydrates (g) | |||||
| Baseline | 208.8 ± 38.6 | 196.1 ± 47.3 | 0.671 | <0.001 | 0.350 |
| 3 months | 237.3 ± 70.0 # | 239.6 ± 66.7 # | |||
| Fat (g) | |||||
| Baseline | 76.5 ± 18.5 | 78.4 ± 24.2 | 0.681 | 0.231 | 0.999 |
| 3 months | 72.1 ± 18.1 | 74.1 ± 21.2 | |||
| Saturated fat (g) | |||||
| Baseline | 28.2 ± 8.6 | 27.5 ± 8.0 | 0.849 | 0.224 | 0.836 |
| 3 months | 25.8 ± 8.3 | 25.7 ± 10.6 | |||
| Protein (g) | |||||
| Baseline | 80.2 ± 21.9 | 92.3 ± 16.9 * | 0.193 | 0.051 | 0.006 |
| 3 months | 80.3 ± 15.7 | 78.5 ± 19.3 # | |||
| Body mass (kg) | |||||
| Baseline | 82.8 ± 13.9 | 82.4 ± 12.3 | 0.968 | 0.007 | 0.048 |
| 3 months | 83.4 ± 14.2 | 84.1 ± 13.2 # | |||
| BMI (kg/m2) | |||||
| Baseline | 27.3 ± 3.8 | 27.5 ± 3.8 | 0.757 | 0.001 | 0.057 |
| 3 months | 27.5 ± 3.8 | 28.1 ± 4.0 # | |||
| Body fat (%) | |||||
| Baseline | 37.1 ± 7.9 | 36.1 ± 6.8 | 0.642 | 0.031 | 0.862 |
| 3 months | 37.7 ± 6.8 # | 36.7 ± 6.8 | |||
| Fat mass (kg) | |||||
| Baseline | 30.2 ± 9.1 | 29.6 ± 7.1 | 0.856 | 0.007 | 0.691 |
| 3 months | 31.1 ± 9.5 # | 30.7 ± 7.5 # | |||
| Lean mass (kg) | |||||
| Baseline | 48.1 ± 9.4 | 49.8 ± 8.5 | 0.360 | 0.248 | 0.199 |
| 3 months | 48.1 ± 8.5 | 50.4 ± 9.2 | |||
| Android/gynoid ratio | |||||
| Baseline | 1.09 ± 0.17 | 1.13 ± 0.18 | 0.394 | 0.403 | 0.529 |
| 3 months | 1.08 ± 0.17 | 1.13 ± 0.18 | |||
| Cherry Juice | Placebo | ANCOVA Adjusted for Baseline | Adjusted for Baseline, Sex and Medication | |||||
|---|---|---|---|---|---|---|---|---|
| Difference (95% CI) | F | p-Value | Difference (95% CI) | F | p-Value | |||
| SBP (mmHg) | ||||||||
| Baseline | 120 ± 15 | 119 ± 11 | −0.5 (−4.9, 3.8) | 0.056 | 0.814 | −0.6 (−5.1, 3.9) | 0.079 | 0.780 |
| 3 months | 117 ± 14 | 118 ± 11 | ||||||
| DBP (mmHg) | ||||||||
| Baseline | 73 ± 10 | 73 ± 8 | −0.4 (−3.0, 2.3) | 0.086 | 0.770 | −0.5 (−3.1, 2.2) | 0.127 | 0.723 |
| 3 months | 73 ± 9 | 73 ± 8 | ||||||
| HR (BPM) | ||||||||
| Baseline | 59 ± 11 | 59 ± 10 | −0.3 (−3.7, 3.1) | 0.033 | 0.858 | −0.2 (−3.6, 3.2) | 0.014 | 0.908 |
| 3 months | 59 ± 12 | 59 ± 10 | ||||||
| PWV (m/s) | ||||||||
| Baseline | 6.7 ± 1.0 | 6.4 ± 0.8 | 0.3 (−0.3, 0.8) | 1.051 | 0.312 | 0.2 (−0.2, 0.7) | 0.967 | 0.332 |
| 3 months | 6.8 ± 1.3 | 6.2 ± 0.8 | ||||||
| AIx (%) | ||||||||
| Baseline | 22.1 ± 8.9 | 17.8 ± 11.4 | 0.3 (−3.6, 4.2) | 0.021 | 0.886 | 0.3 (−3.6, 4.2) | 0.022 | 0.884 |
| 3 months | 20.4 ± 9.6 | 17.0 ± 10.0 | ||||||
| AIx@75 (%) | ||||||||
| Baseline | 13.4 ± 8.1 | 9.6 ± 12.9 | 0.02 (−3.6, 3.6) | <0.001 | 0.991 | −0.06 (−3.6, 3.5) | 0.001 | 0.937 |
| 3 months | 12.3 ± 9.2 | 9.3 ± 11.0 | ||||||
| FMD (%) | ||||||||
| Baseline | 8.3 ± 3.5 | 9.3 ± 3.5 | 1.1 (−1.1, 3.3) | 0.972 | 0.330 | 1.2 (−1.0, 3.3) | 1.256 | 0.269 |
| 3 months | 9.7 ± 3.5 | 9.0 ± 4.0 | ||||||
| Cherry (n = 19) | Placebo (n = 21) | ANCOVA Adjusted for Baseline | |||
|---|---|---|---|---|---|
| Difference (95% CI) | F | p-Value | |||
| Insulin (pmol/L) | |||||
| Baseline | 20.3 ± 15.4 | 19.6 ± 10.2 | −0.01 (−0.18, 0.15) | 0.020 | 0.888 |
| 3 months | 17.8 ± 10.0 | 19.0 ± 13.0 | |||
| Glucose (mmol/L) | |||||
| Baseline | 5.4 ± 0.5 | 5.5 ± 0.5 | −0.01 (−0.21, 0.18) | 0.016 | 0.899 |
| 3 months | 5.4 ± 0.5 | 5.4 ± 0.3 | |||
| HOMA-IR | |||||
| Baseline | 0.7 ± 0.6 | 0.7 ± 0.4 | 0.04 (−0.13, 0.21) | 0.239 | 0.629 |
| 3 months | 0.7 ± 0.4 | 0.7 ± 0.5 | |||
| hs-CRP (mg/L) | |||||
| Baseline | 1.6 ± 2.3 | 1.2 ± 1.2 | −0.003 (−0.14, 0.14) | 0.111 | 0.741 |
| 3 months | 1.4 ± 1.7 | 1.2 ± 1.0 | |||
| Triglycerides (mmol/L) | |||||
| Baseline | 1.2 ± 0.6 | 1.2 ± 0.7 | −0.06 (−0.29, 0.18) | 0.241 | 0.627 |
| 3 months | 1.2 ± 0.7 | 1.3 ± 0.7 | |||
| Cholesterol (mmol/L) | |||||
| Baseline | 5.3 ± 1.2 | 5.0 ± 1.0 | −0.15 (−0.51, 0.21) | 0.728 | 0.399 |
| 3 months | 5.2 ± 1.1 | 5.1 ± 0.9 | |||
| LDL Cholesterol (mmol/L) | |||||
| Baseline | 3.2 ± 1.0 | 3.0 ± 1.0 | −0.09 (−0.38, 0.20) | 0.411 | 0.525 |
| 3 months | 3.1 ± 1.0 | 3.1 ± 1.0 | |||
| HDL Cholesterol (mmol/L) | |||||
| Baseline | 1.6 ± 0.3 | 1.5 ± 0.4 | −0.02 (−0.15, 0.12) | 0.061 | 0.806 |
| 3 months | 1.5 ± 0.4 | 1.5 ± 0.4 | |||
| Non-HDL Cholesterol (mmol/L) | |||||
| Baseline | 3.7 ± 1.2 | 3.5 ± 1.2 | −0.17 (−0.49, 0.16) | 1.08 | 0.305 |
| 3 months | 3.7 ± 1.1 | 3.6 ± 1.1 | |||
| Total/HDL Cholesterol Ratio | |||||
| Baseline | 3.5 ± 1.0 | 3.7 ± 1.3 | −0.076, −0.41, 0.26) | 0.209 | 0.650 |
| 3 months | 3.6 ± 1.2 | 3.8 ± 1.4 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kimble, R.; Keane, K.M.; Lodge, J.K.; Howatson, G. The Influence of Tart Cherry (Prunus cerasus, cv Montmorency) Concentrate Supplementation for 3 Months on Cardiometabolic Risk Factors in Middle-Aged Adults: A Randomised, Placebo-Controlled Trial. Nutrients 2021, 13, 1417. https://doi.org/10.3390/nu13051417
Kimble R, Keane KM, Lodge JK, Howatson G. The Influence of Tart Cherry (Prunus cerasus, cv Montmorency) Concentrate Supplementation for 3 Months on Cardiometabolic Risk Factors in Middle-Aged Adults: A Randomised, Placebo-Controlled Trial. Nutrients. 2021; 13(5):1417. https://doi.org/10.3390/nu13051417
Chicago/Turabian StyleKimble, Rachel, Karen M. Keane, John K. Lodge, and Glyn Howatson. 2021. "The Influence of Tart Cherry (Prunus cerasus, cv Montmorency) Concentrate Supplementation for 3 Months on Cardiometabolic Risk Factors in Middle-Aged Adults: A Randomised, Placebo-Controlled Trial" Nutrients 13, no. 5: 1417. https://doi.org/10.3390/nu13051417
APA StyleKimble, R., Keane, K. M., Lodge, J. K., & Howatson, G. (2021). The Influence of Tart Cherry (Prunus cerasus, cv Montmorency) Concentrate Supplementation for 3 Months on Cardiometabolic Risk Factors in Middle-Aged Adults: A Randomised, Placebo-Controlled Trial. Nutrients, 13(5), 1417. https://doi.org/10.3390/nu13051417