
Serum Selenium Level Predicts 10-Year Survival after Breast Cancer

 , , , , , , , , ,
, , , , , , , , , 

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Ethical Approval and Informed Consent
2.3. Analytical Procedures
2.4. Statistical Analysis
3. Results
3.1. General Characteristics of the Study Population
3.2. Serum Selenium Level—Subgroup Analysis
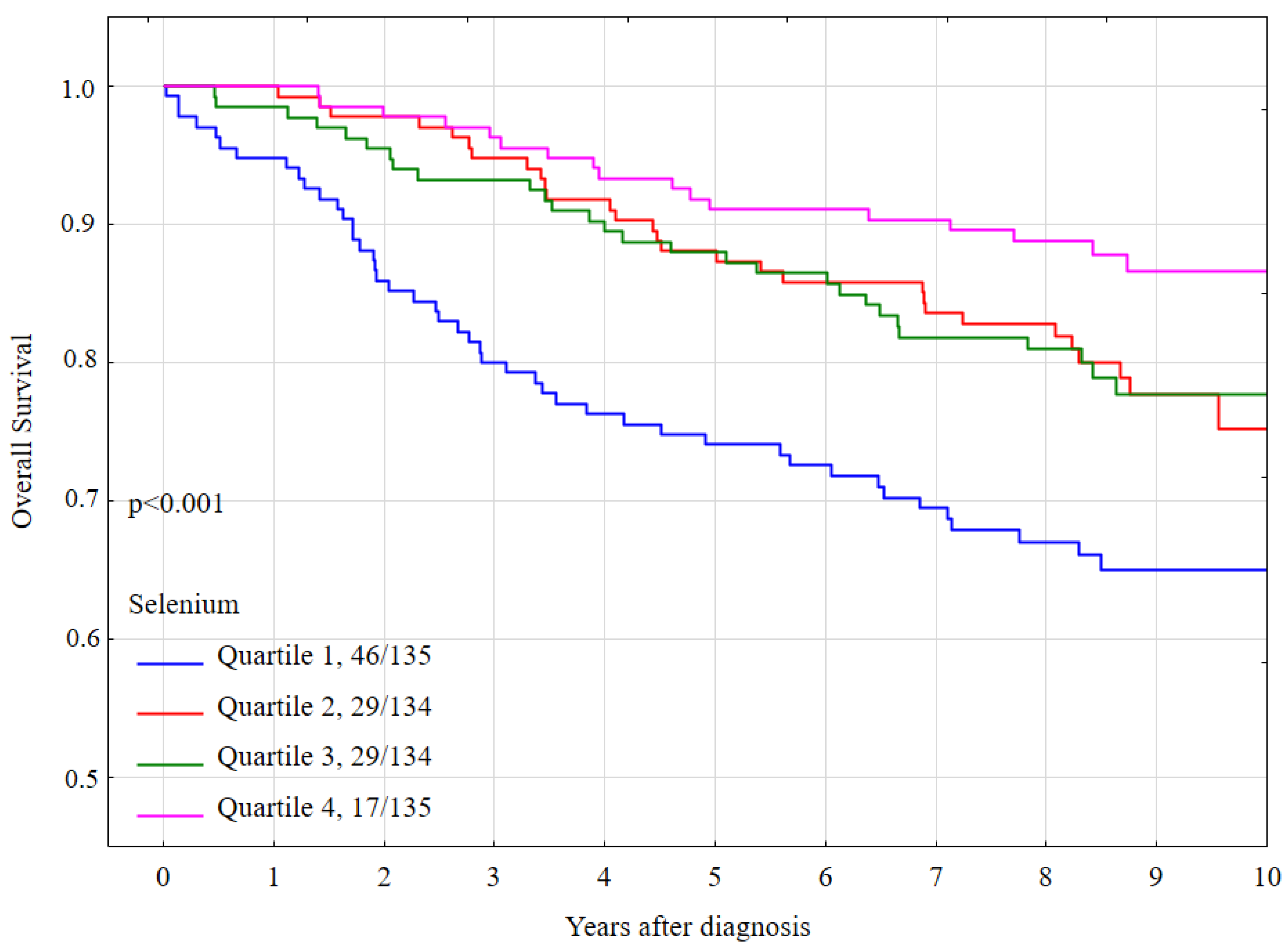
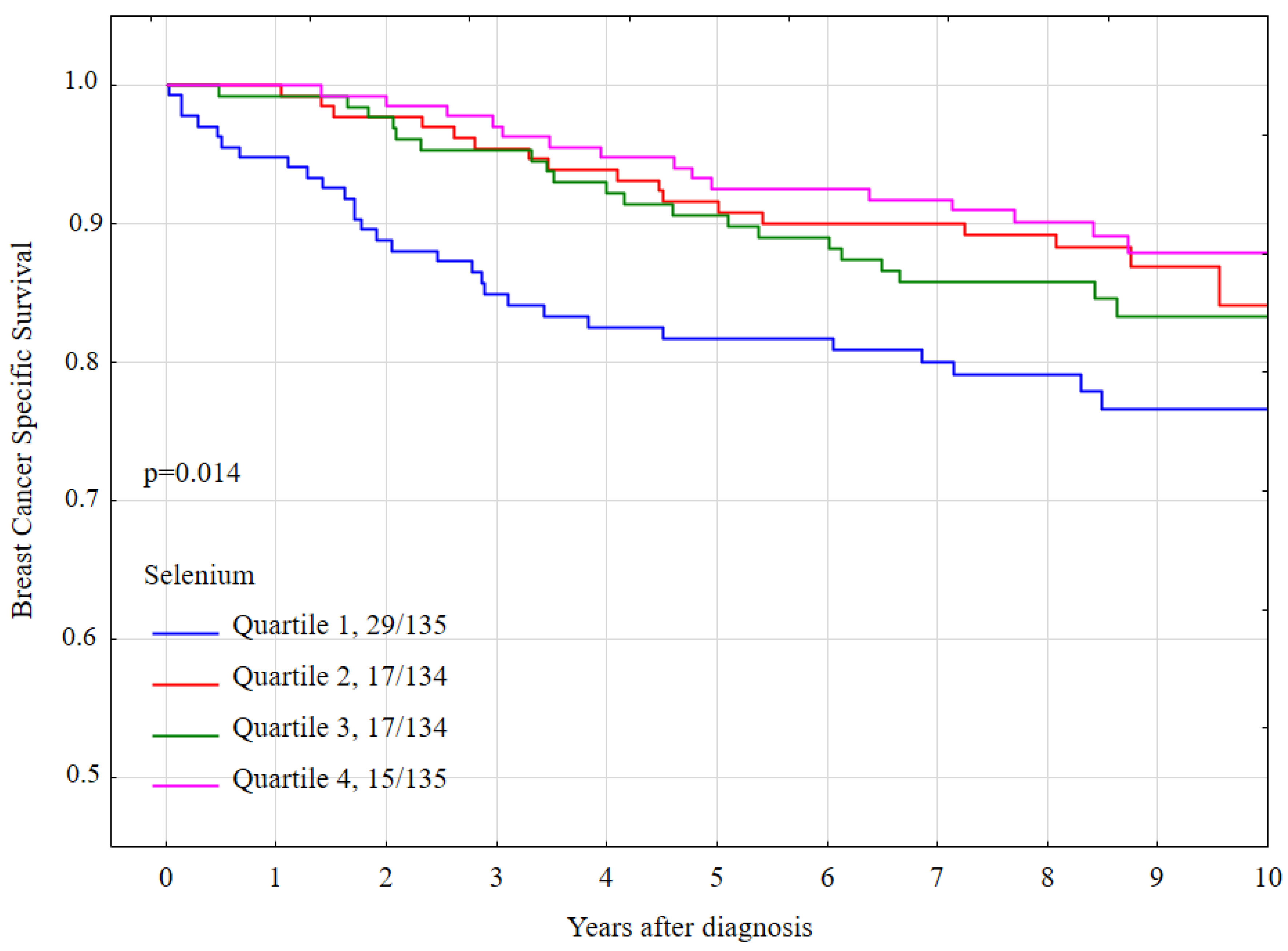
3.3. All-Cause Mortality, Breast Cancer-Specific Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Short, S.P.; Williams, C.S. Selenoproteins in Tumorigenesis and Cancer Progression. Adv. Cancer Res. 2017, 136, 49–83. [Google Scholar] [CrossRef]
- Rayman, M.P. Selenium in cancer prevention: A review of the evidence and mechanism of action. Proc. Nutr. Soc. 2005, 64, 527–542. [Google Scholar] [CrossRef] [PubMed]
- Rayman, M.P. Selenium and human health. Lancet 2012, 379, 1256–1268. [Google Scholar] [CrossRef]
- Davis, C.D.; Tsuji, P.A.; Milner, J.A. Selenoproteins and cancer prevention. Annu. Rev. Nutr. 2012, 32, 73–95. [Google Scholar] [CrossRef]
- Fernandes, A.P.; Gandin, V. Selenium compounds as therapeutic agents in cancer. Biochim. Biophys. Acta 2015, 1850, 1642–1660. [Google Scholar] [CrossRef] [PubMed]
- Navarro Silvera, S.A.; Rohan, T.E. Trace elements and cancer risk: A review of the epidemiologic evidence. Cancer Causes Control. 2007, 18, 7–27. [Google Scholar] [CrossRef]
- Vinceti, M.; Filippini, T.; Del Giovane, C.; Dennert, G.; Zwahlen, M.; Brinkman, M.; Zeegers, M.P.; Horneber, M.; D’Amico, R.; Crespi, C.M. Selenium for preventing cancer. Cochrane Database Syst. Rev. 2018, 1, CD005195. [Google Scholar] [CrossRef] [PubMed]
- Combs, G.F., Jr. Selenium in global food systems. Br. J. Nutr. 2001, 85, 517–547. [Google Scholar] [CrossRef] [PubMed]
- Rayman, M.P. The use of high-selenium yeast to raise selenium status: How does it measure up? Br. J. Nutr. 2004, 92, 557–573. [Google Scholar] [CrossRef] [PubMed]
- Duffield-Lillico, A.J.; Reid, M.E.; Turnbull, B.W.; Combs, G.F., Jr.; Slate, E.H.; Fischbach, L.A.; Marshall, J.R.; Clark, L.C. Baseline characteristics and the effect of selenium supplementation on cancer incidence in a randomized clinical trial: A summary report of the Nutritional Prevention of Cancer Trial. Cancer Epidemiol. Biomark. Prev. 2002, 11, 630–639. [Google Scholar] [PubMed]
- Klein, E.A.; Thompson Jr, I.M.; Tangen, C.M.; Crowley, J.J.; Lucia, M.S.; Goodman, P.J.; Minasian, L.M.; Ford, L.G.; Parnes, H.L.; Gaziano, J.M.; et al. Vitamin E and the risk of prostate cancer: The Selenium and Vitamin E Cancer Prevention Trial (SELECT). JAMA 2011, 306, 1549–1556. [Google Scholar] [CrossRef] [PubMed]
- Marshall, J.R.; Tangen, C.M.; Sakr, W.A.; Wood, D.P., Jr.; Berry, D.L.; Klein, E.A.; Lippman, S.M.; Parnes, H.L.; Alberts, D.S.; Jarrard, D.F.; et al. Phase III trial of selenium to prevent prostate cancer in men with high-grade prostatic intraepithelial neoplasia: SWOG S9917. Cancer Prev. Res. 2011, 4, 1761–1769. [Google Scholar] [CrossRef] [PubMed]
- Algotar, A.M.; Stratton, M.S.; Ahmann, F.R.; Ranger-Moore, J.; Nagle, R.B.; Thompson, P.A.; Slate, E.; Hsu, C.H.; Dalkin, B.L.; Sindhwani, P.; et al. Phase 3 clinical trial investigating the effect of selenium supplementation in men at high-risk for prostate cancer. Prostate 2013, 73, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Karp, D.D.; Lee, S.J.; Keller, S.M.; Wright, G.S.; Aisner, S.; Belinsky, S.A.; Johnson, D.H.; Johnston, M.R.; Goodman, G.; Clamon, G.; et al. Randomized, double-blind, placebo-controlled, phase III chemoprevention trial of selenium supplementation in patients with resected stage I non-small-cell lung cancer: ECOG 5597. J. Clin. Oncol. 2013, 31, 4179–4187. [Google Scholar] [CrossRef] [PubMed]
- Jaworska, K.; Gupta, S.; Durda, K.; Muszyńska, M.; Sukiennicki, G.; Jaworowska, E.; Grodzki, T.; Sulikowski, M.; Woloszczyk, P.; Wójcik, J.; et al. A low selenium level is associated with lung and laryngeal cancers. PLoS ONE 2013, 8, e59051. [Google Scholar] [CrossRef]
- Lener, M.R.; Gupta, S.; Scott, R.J.; Tootsi, M.; Kulp, M.; Tammesoo, M.L.; Viitak, A.; Metspalu, A.; Serrano-Fernández, P.; Kładny, J.; et al. Can selenium levels act as a marker of colorectal cancer risk? BMC Cancer 2013, 13, 214. [Google Scholar] [CrossRef]
- Sandsveden, M.; Nilsson, E.; Borgquist, S.; Rosendahl, A.H.; Manjer, J. Prediagnostic serum selenium levels in relation to breast cancer survival and tumor characteristics. Int. J. Cancer 2020, 6. [Google Scholar] [CrossRef]
- Jablońska, E.; Gromadzińska, J.; Sobala, W.; Reszka, E.; Wasowicz, W. Lung cancer risk associated with selenium status is modified in smoking individuals by Sep15 polymorphism. Eur. J. Nutr. 2008, 47, 47–54. [Google Scholar] [CrossRef]
- Laclaustra, M.; Stranges, S.; Navas-Acien, A.; Ordovas, J.M.; Guallar, E. Serum selenium and serum lipids in US adults: National Health and Nutrition Examination Survey (NHANES) 2003–2004. Atherosclerosis 2010, 210, 643–648. [Google Scholar] [CrossRef]
- Lubiński, J.; Marciniak, W.; Muszyńska, M.; Huzarski, T.; Gronwald, J.; Cybulski, C.; Jakubowska, A.; Dębniak, T.; Falco, M.; Kładny, J.; et al. Serum selenium levels predict survival after breast cancer. Breast Cancer Res. Treat. 2017, 167, 591–598. [Google Scholar] [CrossRef]
- Pietrzak, S.; Wójcik, J.; Scott, R.J.; Kashyap, A.; Grodzki, T.; Baszuk, P.; Bielewicz, M.; Marciniak, W.; Wójcik, N.; Dębniak, T.; et al. Influence of the selenium level on overall survival in lung cancer. J. Trace. Elem. Med. Biol. 2019, 56, 46–51. [Google Scholar] [CrossRef]
- Lubiński, J.; Marciniak, W.; Muszyńska, M.; Jaworowska, E.; Sulikowski, M.; Jakubowska, A.; Kaczmarek, K.; Sukiennicki, G.; Falco, M.; Baszuk, P.; et al. Serum selenium levels and the risk of progression of laryngeal cancer. PLoS ONE 2018, 13, e0184873. [Google Scholar] [CrossRef] [PubMed]
- Harris, H.R.; Bergkvist, L.; Wolk, A. Selenium intake and breast cancer mortality in a cohort of Swedish women. Breast Cancer Res. Treat. 2012, 134, 1269–1277. [Google Scholar] [CrossRef]
- Holmes, M.D.; Stampfer, M.J.; Colditz, G.A.; Rosner, B.; Hunter, D.J.; Willett, W.C. Dietary factors and the survival of women with breast carcinoma. Cancer 1999, 86, 826–835. [Google Scholar] [CrossRef]
- Saquib, J.; Rock, C.L.; Natarajan, L.; Saquib, N.; Newman, V.A.; Patterson, R.E.; Thomson, C.A.; Al-Delaimy, W.K.; Pierce, J.P. Dietary intake, supplement use, and survival among women diagnosed with early-stage breast cancer. Nutr. Cancer 2011, 63, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Steinbrenner, H.; Speckmann, B.; Sies, H. Toward understanding success and failures in the use of selenium for cancer prevention. Antioxid Redox Signal 2013, 19, 181–191. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Risk Factor | n | % | Mean Selenium Level | pa | |
|---|---|---|---|---|---|
| All | 538 | 100 | 86.2 | ||
| Age | |||||
| 26–50 | 132 | 24.5 | 85.1 | <0.001 b | |
| 51–60 | 186 | 34.6 | 88.4 | ||
| 61–70 | 146 | 27.1 | 87.6 | ||
| ≥71 | 74 | 13.8 | 80.0 | ||
| BRCA1 mutation | |||||
| Yes | 62 | 11.5 | 86.5 | 0.86 | |
| No | 476 | 88.5 | 86.2 | ||
| Lymph node status | |||||
| Positive | 193 | 35.9 | 86.1 | 0.77 | |
| Negative | 327 | 60.8 | 86.4 | ||
| Missing | 18 | 3.3 | 84.0 | ||
| ER status | |||||
| Positive | 372 | 69.1 | 85.6 | 0.06 | |
| Negative | 148 | 27.5 | 88.3 | ||
| Missing | 18 | 3.4 | 81.9 | ||
| Tumor size [cm] | |||||
| 0–1.9 | 307 | 57.1 | 87.2 | 0.13 | |
| 2.0–4.9 | 188 | 34.9 | 86.1 | ||
| ≥5.0 | 12 | 2.2 | 79.0 | ||
| Missing | 31 | 5.8 | 80.0 | ||
| Radiotherapy | |||||
| Yes | 308 | 57.3 | 87.0 | 0.26 | |
| No | 190 | 35.3 | 85.5 | ||
| Missing | 40 | 7.4 | 83.7 | ||
| Chemotherapy | |||||
| Yes | 282 | 52.4 | 86.4 | 0.80 | |
| No | 227 | 42.2 | 86.1 | ||
| Missing | 29 | 5.4 | 84.6 | ||
| Type of surgery | |||||
| Lumpectomy | 162 | 30.1 | 88.0 | 0.12 | |
| Mastectomy | 352 | 65.4 | 85.9 | ||
| Missing | 24 | 4.5 | 78.6 | ||
| Tamoxifen | |||||
| Yes | 363 | 67.5 | 86.0 | 0.42 | |
| No | 157 | 29.2 | 87.1 | ||
| Missing | 18 | 3.3 | 81.9 | ||
| Vital status | |||||
| Alive | 417 | 77.5 | 87.5 | ||
| Dead | 121 | 22.5 | 81.8 | <0.001 | |
| Dead of breast cancer | 81 | 66.9 | 83.6 | 0.03 | |
| Dead of other cancers | 10 | 8.3 | 71.0 | <0.001 | |
| Dead of any cancers | 91 | 74.4 | 82.2 | 0.002 | |
| Smoking | |||||
| Yes, current | 115 | 21.4 | 86.7 | 0.59 | |
| Yes, past | 139 | 25.8 | 86.8 | ||
| Never | 271 | 50.4 | 85.5 | ||
| Missing | 13 | 2.4 | 90.5 | ||
| Selenium Quartile * | Overall Survival (OS) | Breast Cancer Specific Survival | ||
|---|---|---|---|---|
| 10-Year (%) | Log-Rank Test | 10-Year (%) | Log-Rank Test | |
| All group | 76.2 | p | 83.1 | p |
| Quartile 1 | 65.1 | <0.001 a | 76.7 | 0.014 b |
| Quartile 2 | 75.1 | 84.2 | ||
| Quartile 3 | 77.7 | 83.4 | ||
| Quartile 4 | 86.7 | 87.9 | ||
| Risk Factor | All-Cause Mortality | Breast Cancer-Specific Mortality | |||||
|---|---|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | ||||
| Age | |||||||
| ≤50 | 1.00 | Reference | 1.00 | Reference | |||
| 51–60 | 1.23 | (0.73–2.08) | 0.44 | 1.17 | (0.65–2.09) | 0.60 | |
| 61–70 | 1.08 | (0.62–1.90) | 0.79 | 0.83 | (0.43–1.62) | 0.59 | |
| ≥71 | 2.98 | (1.73–5.12) | <0.001 | 1.86 | (0.95–3.65) | 0.07 | |
| BRCA1 mutation | |||||||
| No | 1.00 | Reference | 1.00 | Reference | |||
| Yes | 0.84 | (0.45–1.57) | 0.59 | 0.89 | (0.43–1.85) | 0.75 | |
| Lymph node status | |||||||
| Negative | 1.00 | Reference | 1.00 | Reference | |||
| Positive | 2.80 | (1.91–4.11) | <0.001 | 3.44 | (2.14–5.52) | <0.001 | |
| ER status | |||||||
| Negative | 1.00 | Reference | 1.00 | Reference | |||
| Positive | 0.93 | (0.61–1.40) | 0.72 | 0.64 | (0.40–1.02) | 0.06 | |
| Tumor size [cm] | |||||||
| 0–1.9 | 1.00 | Reference | 1.00 | Reference | |||
| 2.0–4.9 | 2.20 | (1.46–3.32) | <0.001 | 2.42 | (1.44–4.05) | <0.001 | |
| ≥5.0 | 6.00 | (2.67–3.35) | <0.001 | 6.91 | (2.63–18.1) | <0.001 | |
| Radiotherapy | |||||||
| No | 1.00 | Reference | 1.00 | Reference | |||
| Yes | 0.85 | (0.57–1.25) | 0.40 | 1.03 | (0.63–1.67) | 0.91 | |
| Chemotherapy | |||||||
| No | 1.00 | Reference | 1.00 | Reference | |||
| Yes | 1.46 | (0.98–2.17) | 0.06 | 2.37 | (1.40–4.00) | 0.001 | |
| Type of surgery | |||||||
| Mastectomy | 1.00 | Reference | 1.00 | Reference | |||
| Lumpectomy | 0.42 | (0.25–0.70) | <0.001 | 0.34 | (0.17–0.67) | 0.002 | |
| Tamoxifen | |||||||
| No | 1.00 | Reference | 1.00 | Reference | |||
| Yes | 0.98 | (0.65–1.47) | 0.92 | 0.67 | (0.42–1.06) | 0.09 | |
| Smoking | |||||||
| Never | 1.00 | Reference | 1.00 | Reference | |||
| Yes, current | 0.96 | (0.61–1.52) | 0.88 | 0.76 | (0.42–1.39) | 0.37 | |
| Yes, past | 0.82 | (0.52–1.28) | 0.37 | 0.92 | (0.55–1.54) | 0.74 | |
| Selenium quartile * | |||||||
| Quartile 4 | 1.00 | Reference | 1.00 | Reference | |||
| Quartile 1 | 3.26 | (1.87–5.69) | <0.001 | 2.31 | (1.24–4.31) | 0.008 | |
| Quartile 2 | 1.78 | (0.98–3.23) | 0.06 | 1.19 | (0.59–2.38) | 0.62 | |
| Quartile 3 | 1.77 | (0.97–3.24) | 0.06 | 1.45 | (0.74–2.83) | 0.28 | |
| Risk Factor | All-Cause Mortality | Breast Cancer-Specific Mortality | |||||
|---|---|---|---|---|---|---|---|
| HR (95% CI) | pa | HR (95% CI) | pb | ||||
| Age | |||||||
| ≤50 | 1.00 | Reference | 1.00 | Reference | |||
| 51–60 | 1.38 | (0.74–2.54) | 0.31 | 1.34 | (0.65–2.77) | 0.42 | |
| 61–70 | 1.58 | (0.82–3.01) | 0.17 | 1.51 | (0.69–3.36) | 0.30 | |
| ≥71 | 2.60 | (1.28–5.28) | 0.008 | 2.03 | (0.80–5.15) | 0.13 | |
| Lymph node status | |||||||
| Negative | 1.00 | Reference | 1.00 | Reference | |||
| Positive | 1.97 | (1.23–3.16) | 0.005 | 2.14 | (1.16–3.94) | 0.01 | |
| ER status | |||||||
| Negative | - | 1.00 | Reference | ||||
| Positive | 0.86 | (0.28–2.65) | 0.79 | ||||
| Tumor size [cm] | |||||||
| 0–1.9 | 1.00 | Reference | 1.00 | Reference | |||
| 2.0–4.9 | 1.66 | (1.05–2.63) | 0.03 | 2.04 | (1.14–3.67) | 0.02 | |
| ≥5.0 | 3.71 | (1.52–9.07) | 0.004 | 6.00 | (2.00–17.97) | 0.001 | |
| Chemotherapy | |||||||
| No | 1.00 | Reference | 1.00 | Reference | |||
| Yes | 1.35 | (0.79–2.33) | 0.27 | 1.86 | (0.86–4.01) | 0.11 | |
| Type of surgery | |||||||
| Mastectomy | 1.00 | Reference | 1.00 | Reference | |||
| Lumpectomy | 0.76 | (0.43–1.34) | 0.34 | 0.79 | (0.37–1.68) | 0.55 | |
| Tamoxifen | |||||||
| No | - | 1.00 | Reference | ||||
| Yes | 0.76 | (0.26–2.24) | 0.62 | ||||
| Selenium quartile * | |||||||
| Quartile 4 | 1.00 | Reference | 1.00 | Reference | |||
| Quartile 1 | 2.35 | (1.21–4.55) | 0.01 | 1.56 | (0.72–3.40) | 0.26 | |
| Quartile 2 | 1.52 | (0.76–3.02) | 0.23 | 0.99 | (0.46–2.16) | 0.99 | |
| Quartile 3 | 1.95 | (1.01–3.76) | 0.047 | 1.35 | (0.63–2.87) | 0.43 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szwiec, M.; Marciniak, W.; Derkacz, R.; Huzarski, T.; Gronwald, J.; Cybulski, C.; Dębniak, T.; Jakubowska, A.; Lener, M.; Falco, M.; et al. Serum Selenium Level Predicts 10-Year Survival after Breast Cancer. Nutrients 2021, 13, 953. https://doi.org/10.3390/nu13030953
Szwiec M, Marciniak W, Derkacz R, Huzarski T, Gronwald J, Cybulski C, Dębniak T, Jakubowska A, Lener M, Falco M, et al. Serum Selenium Level Predicts 10-Year Survival after Breast Cancer. Nutrients. 2021; 13(3):953. https://doi.org/10.3390/nu13030953
Chicago/Turabian StyleSzwiec, Marek, Wojciech Marciniak, Róża Derkacz, Tomasz Huzarski, Jacek Gronwald, Cezary Cybulski, Tadeusz Dębniak, Anna Jakubowska, Marcin Lener, Michał Falco, and et al. 2021. "Serum Selenium Level Predicts 10-Year Survival after Breast Cancer" Nutrients 13, no. 3: 953. https://doi.org/10.3390/nu13030953
APA StyleSzwiec, M., Marciniak, W., Derkacz, R., Huzarski, T., Gronwald, J., Cybulski, C., Dębniak, T., Jakubowska, A., Lener, M., Falco, M., Kładny, J., Baszuk, P., Duszyński, J., Kotsopoulos, J., Narod, S. A., & Lubiński, J. (2021). Serum Selenium Level Predicts 10-Year Survival after Breast Cancer. Nutrients, 13(3), 953. https://doi.org/10.3390/nu13030953