
Assessing the Effectiveness of Front of Pack Labels: Findings from an Online Randomised-Controlled Experiment in a Representative British Sample

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
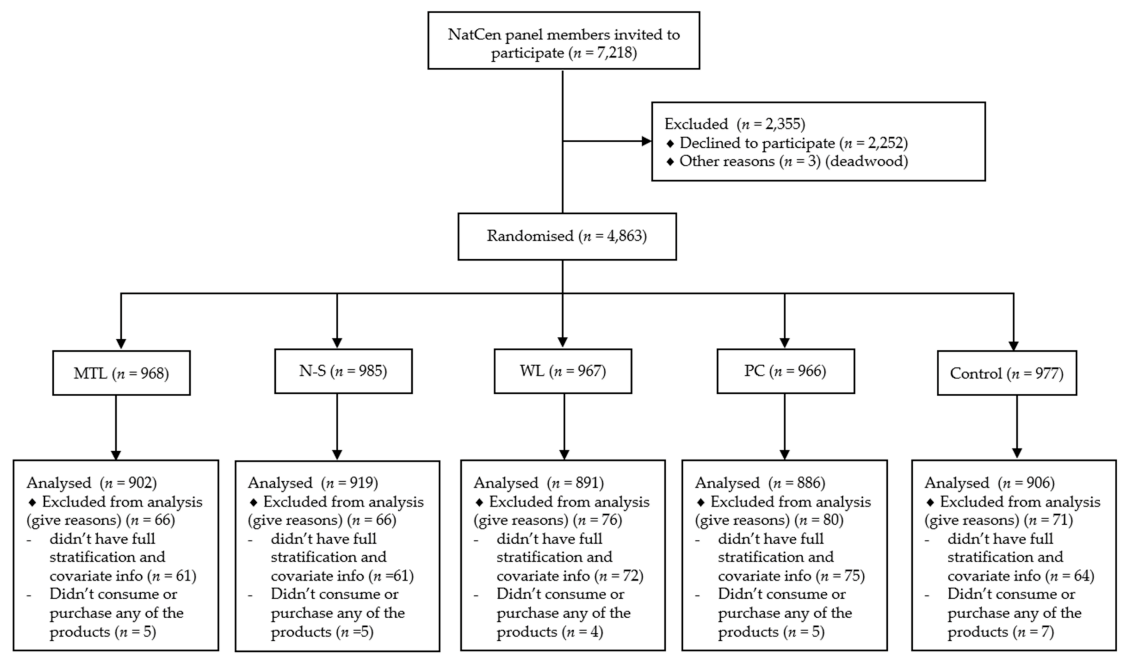
2.1. Study Design and Participants
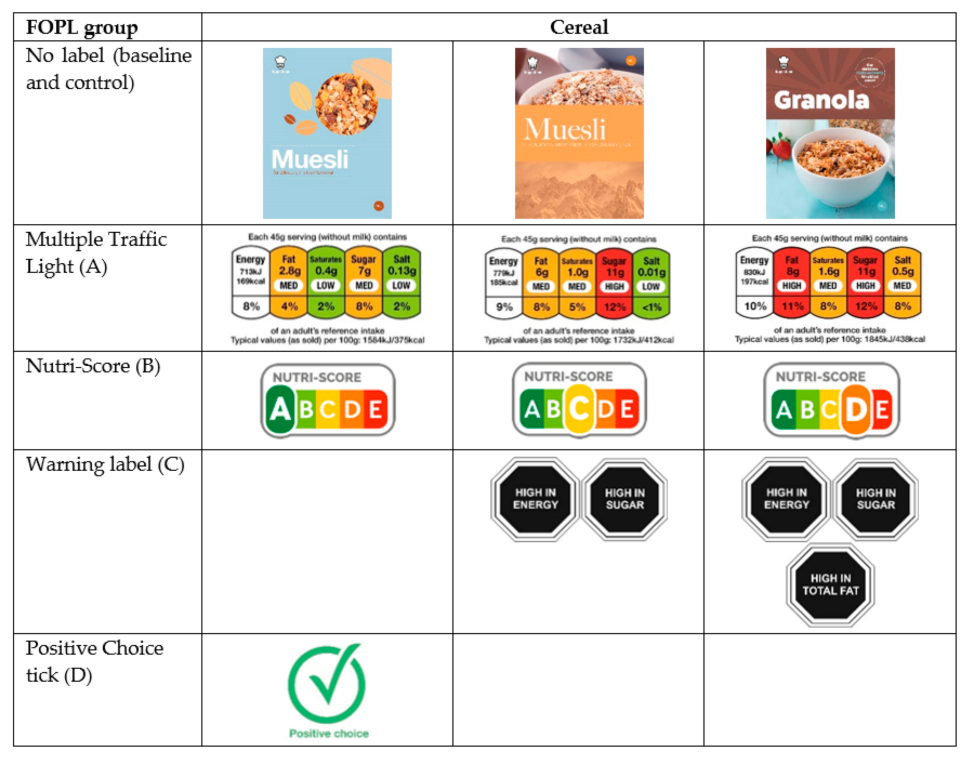
2.2. Materials
2.3. Randomisation
2.4. Procedure
2.5. Measures
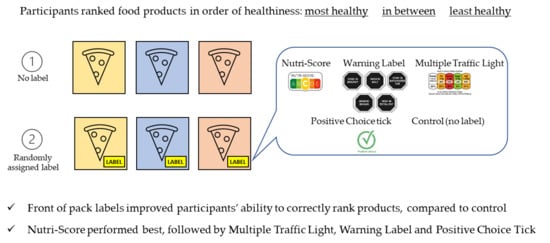
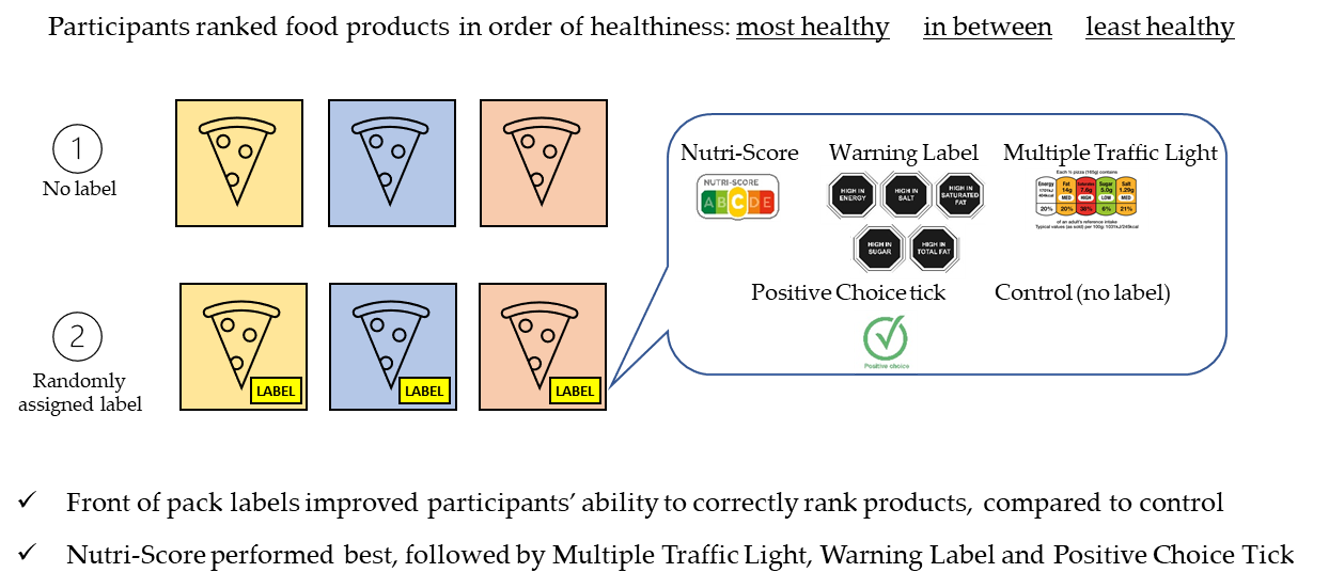
2.5.1. Primary Outcome
- ranking of healthiness of products (correct for all products = 1, any incorrect = 0) at baseline and follow-up;
- change in ranking from baseline to follow-up (improved = +1; no change = 0; worsened = −1);
- change in global food score, with change for each of the five food categories, i.e., excluding the drink (see Section 2.6), summed to give an overall score (range +5, all categories improved, to −5, all categories worsened).
2.5.2. Other Secondary Outcomes
2.5.3. Participant Characteristics
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abarca-Gómez, L.; Abdeen, Z.A.; Hamid, Z.A.; Abu-Rmeileh, N.M.; Acosta-Cazares, B.; Acuin, C.; Adams, R.J.; Aekplakorn, W.; Afsana, K.; Aguilar-Salinas, C.A.; et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128.9 million, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef]
- Goiana-da-Silva, F.; Cruz-e-Silva, D.; Miraldo, M.; Calhau, C.; Bento, A.; Cruz, D.; Almeida, F.; Darzi, A.; Araújo, F. Front-of-pack labelling policies and the need for guidance. Lancet Public Health 2019, 4, e15. [Google Scholar] [CrossRef]
- Kelly, B.; Jewell, J. What is the Evidence on the Policy Specifications, Development Processes and Effectiveness of Existing Front-of-Pack Food Labelling Policies in the WHO European Region? Available online: https://www.euro.who.int/__data/assets/pdf_file/0007/384460/Web-WHO-HEN-Report-61-on-FOPL.pdf (accessed on 5 February 2021).
- Van der Bend, D.L.M.; Lissner, L. Differences and Similarities between Front-of-Pack Nutrition Labels in Europe: A Comparison of Functional and Visual Aspects. Nutrients 2019, 11, 626. [Google Scholar] [CrossRef] [PubMed]
- Crockett, R.A.; King, S.E.; Marteau, T.M.; Prevost, A.T.; Bignardi, G.; Roberts, N.W.; Stubbs, B.; Hollands, G.J.; Jebb, S.A. Nutritional labelling for healthier food or non-alcoholic drink purchasing and consumption. Cochrane Database Syst. Rev. 2018, 2, CD009315. [Google Scholar] [CrossRef] [PubMed]
- Grunert, K.G.; Wills, J.M. A review of European research on consumer response to nutrition information on food labels. J. Public Health 2007, 15, 385–399. [Google Scholar] [CrossRef]
- Van Kleef, E.; Dagevos, H. The growing role of front-of-pack nutrition profile labeling: A consumer perspective on key issues and controversies. Crit. Rev. Food Sci. Nutr. 2015, 55, 291–303. [Google Scholar] [CrossRef] [PubMed]
- Hersey, J.C.; Wohlgenant, K.C.; Arsenault, J.E.; Kosa, K.M.; Muth, M.K. Effects of front-of-package and shelf nutrition labeling systems on consumers. Nutr. Rev. 2013, 71, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Ikonen, I.; Sotgiu, F.; Aydinli, A.; Verlegh, P.W.J. Consumer effects of front-of-package nutrition labeling: An interdisciplinary meta-analysis. J. Acad. Mark. Sci. 2020, 48, 360–383. [Google Scholar] [CrossRef]
- Talati, Z.; Pettigrew, S.; Neal, B.; Dixon, H.; Hughes, C.; Kelly, B.; Miller, C. Consumers’ responses to health claims in the context of other on-pack nutrition information: A systematic review. Nutr. Rev. 2017, 75, 260–273. [Google Scholar] [CrossRef]
- Temple, N.J. Front-of-package food labels: A narrative review. Appetite 2020, 144, 104485. [Google Scholar] [CrossRef]
- Cecchini, M.; Warin, L. Impact of food labelling systems on food choices and eating behaviours: A systematic review and meta-analysis of randomized studies. Obes. Rev. 2016, 17, 201–210. [Google Scholar] [CrossRef]
- Croker, H.; Packer, J.; Russell, S.J.; Stansfield, C.; Viner, R.M. Front of pack nutritional labelling schemes: A systematic review and meta-analysis of recent evidence relating to objectively measured consumption and purchasing. J. Hum. Nutr. Diet. 2020, 33, 518–537. [Google Scholar] [CrossRef]
- Becker, M.W.; Bello, N.M.; Sundar, R.P.; Peltier, C.; Bix, L. Front of pack labels enhance attention to nutrition information in novel and commercial brands. Food Policy 2015, 56, 76–86. [Google Scholar] [CrossRef]
- Egnell, M.; Talati, Z.; Hercberg, S.; Pettigrew, S.; Julia, C. Objective Understanding of Front-of-Package Nutrition Labels: An International Comparative Experimental Study across 12 Countries. Nutrients 2018, 10, 1542. [Google Scholar] [CrossRef] [PubMed]
- Egnell, M.; Talati, Z.; Galan, P.; Andreeva, V.A.; Vandevijvere, S.; Gombaud, M.; Dréano-Trécant, L.; Hercberg, S.; Pettigrew, S.; Julia, C. Objective understanding of the Nutri-score front-of-pack label by European consumers and its effect on food choices: An online experimental study. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 146. [Google Scholar] [CrossRef]
- Vanderlee, L.; Franco-Arellano, B.; Ahmed, M.; Oh, A.; Lou, W.; L’Abbé, M.R. The efficacy of ‘high in’ warning labels, health star and traffic light front-of-package labelling: An online randomised control trial. Public Health Nutr. 2020, 24, 62–74. [Google Scholar] [CrossRef] [PubMed]
- Grunert, K.G.; Wills, J.M.; Fernández-Celemín, L. Nutrition knowledge, and use and understanding of nutrition information on food labels among consumers in the UK. Appetite 2010, 55, 177–189. [Google Scholar] [CrossRef] [PubMed]
- Lima, M.; Ares, G.; Deliza, R. How do front of pack nutrition labels affect healthfulness perception of foods targeted at children? Insights from Brazilian children and parents. Food Qual. Prefer. 2018, 64, 111–119. [Google Scholar] [CrossRef]
- WHO. Regional Office for Europe. European Food and Nutrition Action Plan 2015–2020. Available online: https://www.euro.who.int/__data/assets/pdf_file/0008/253727/64wd14e_FoodNutAP_140426.pdf (accessed on 5 February 2021).
- Jones, A.; Neal, B.; Reeve, B.; Ni Mhurchu, C.; Thow, A.M. Front-of-pack nutrition labelling to promote healthier diets: Current practice and opportunities to strengthen regulation worldwide. BMJ Glob. Health 2019, 4, e001882. [Google Scholar] [CrossRef] [PubMed]
- Department of Health. Front of Pack Nutrition Labelling: Joint Response to Consultation. Available online: http://www.foodstandards.gov.scot/downloads/Front_of_pack_nutrition_labelling_joint_responses.pdf (accessed on 5 February 2021).
- Department of Health and Social Care. Tackling Obesity: Empowering Adults and Children to Live Healthier Lives. Available online: https://www.gov.uk/government/publications/tackling-obesity-government-strategy/tackling-obesity-empowering-adults-and-children-to-live-healthier-lives (accessed on 5 February 2021).
- Experimental Study Examining the Impact of Front of Pack Labelling Skills on Knowledge. Available online: https://osf.io/k9v2p/ (accessed on 20 November 2020).
- Jessop, C. The NatCen Panel: Developing an open probability-based mixed-mode panel in Great Britain. Soc. Res. Pract. 2018, 6, 2–14. [Google Scholar]
- Department of Health. Nutrient Profiling Technical Guidance. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/216094/dh_123492.pdf (accessed on 5 February 2021).
- Santé Publique France. Nutri-Score: Charte Graphique. Available online: https://partage.santepubliquefrance.fr/public/folder/MMGg-LaV6UiJ0BAm1Bb5PA/Pack_logo_hzt (accessed on 5 February 2021).
- UK Government. Guide to Creating a Front of Pack (FoP) Nutrition Label for Pre-Packed Products Sold through Retail Outlets. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/566251/FoP_Nutrition_labelling_UK_guidance.pdf (accessed on 5 February 2021).
- Republica de Chile Ministerio de Salud. Reglamento Sanitario de los Alimentos [Food Sanitary Regulation]. Available online: https://dipol.minsal.cl/wp-content/uploads/2019/06/DECRETO_977_96_2019-2.pdf (accessed on 5 February 2021). (In Spanish).
- Department of Health and Social Care. Building on the Success of Front-of-Pack Nutrition Labelling in the UK: A Public Consultation. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/905096/front-of-pack-labelling-consultation-document-english.pdf (accessed on 5 February 2021).
- Wahlich, C.; Gardner, B.; McGowan, L. How, when and why do young women use nutrition information on food labels? A qualitative analysis. Psychol. Health 2013, 28, 202–216. [Google Scholar] [CrossRef] [PubMed]
- Cowburn, G.; Stockley, L. Consumer understanding and use of nutrition labelling: A systematic review. Public Health Nutr. 2005, 8, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Office for National Statistics; National Records of Scotland; Northern Ireland Statistics and Research Agency. 2011 Census Aggregate Data. Available online: https://discover.ukdataservice.ac.uk/doi/2011-census-aggregate (accessed on 5 February 2021).




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n (%) | |
|---|---|
| Sex | |
| Female | 2570 (57.1) |
| Male | 1934 (42.9) |
| Age * | |
| 18–29 | 278 (6.2) |
| 30–39 | 639 (14.2) |
| 40–49 | 878 (19.5) |
| 50–59 | 962 (21.4) |
| 60–69 | 924 (20.5) |
| 70+ | 820 (18.2) |
| Ethnicity | |
| White British | 3954 (87.8) |
| White other | 257 (5.7) |
| Mixed or multiple ethnic groups | 54 (1.2) |
| Asian or Asian British | 152 (3.4) |
| Black or Black British | 71 (1.6) |
| Other | 16 (0.4) |
| Education | |
| Degree or equivalent | 2182 (48.5) |
| A-levels or vocational level 3 or equivalent | 874 (19.4) |
| Other qualifications below A-levels or equivalent | 781 (17.3) |
| Other qualification | 269 (6.0) |
| No qualifications | 398 (8.8) |
| Children in household | |
| Yes | 1373 (30.4) |
| No | 3131 (69.6) |
| Shopping responsibility | |
| Yes—some or all | 4316 (95.8) |
| No—someone else does | 188 (4.2) |
| Current label use | |
| Very often | 934 (20.7) |
| Quite often | 1536 (34.1) |
| Occasionally | 1316 (29.2) |
| Rarely | 558 (12.4) |
| Never | 160 (3.6) |
| Reported consuming or buying product in past 12 months | |
| Pizza | 3361 (74.6) |
| Drink | 1630 (36.2) |
| Cake | 3163 (70.2) |
| Crisps | 3723 (82.7) |
| Yoghurt | 3779 (83.9) |
| Breakfast cereal | 3802 (84.4) |
| Reported Seeing FOPLs * (n = 3598) | ||||||
| Overall | MTL | N-S | WL | PC | Control * | |
| Yes | 2679 (74.4) | 693 (76.8) | 803 (87.4) | 695 (78.0) | 488 (55.1) | n/a |
| No/not sure | 919 (25.6) | 209 (23.2) | 116 (12.6) | 196 (22.0) | 398 (44.9) | n/a |
| Reported having enough information to rank (n = 4504) (Yes response) | ||||||
| Overall | MTL | N-S | WL | PC | Control | |
| Pizza | 1351 (40.2) | 550 (85.0) | 405 (59.0) † | 243 (35.2) † | 67 (10.0) | 86 (12.8) |
| Drink | 611 (37.5) | 276 (82.1) | 180 (55.6) | 111 (33.0) | 22 (6.9) ^ | 22 (7.0) † |
| Cake | 1362 (43.1) | 546 (83.9) † | 379 (59.9) | 279 (43.9) | 70 (11.4) | 88 (14.0) |
| Crisps | 1651 (44.4) | 647 (87.6) | 472 (61.1) | 317 (42.1) | 93 (13.2) | 122 (16.2) |
| Yoghurt | 1494 (39.5) | 647 (85.7) | 444 (57.5) | 231 (30.9) † | 86 (11.6) † | 86 (11.3) |
| Breakfast cereal | 1533 (40.3) | 649 (85.7) | 455 (60.3) ^ | 253 (33.5) † | 87 (11.5) | 89 (11.4) † |
| MTL vs. Control RR (95%CI) | N-S vs. Control RR (95%CI) | WL vs. Control RR (95%CI) | PC vs. Control RR (95%CI) | N-S vs. MTL RR (95%CI) | |
|---|---|---|---|---|---|
| Pizza | 1.23 (1.11, 1.36) p < 0.001 | 1.29 (1.18, 1.41) p < 0.001 | 1.20 (1.09, 1.32) p < 0.001 | 0.98 (0.90, 1.07) 0.69 | 1.05 (0.95, 1.16) p = 0.32 |
| Drink | 1.29 (1.13, 1.46) p < 0.001 | 1.61 (1.41, 1.84) p < 0.001 | 1.16 (1.03, 1.30) p = 0.01 | 1.18 (1.04, 1.33) p < 0.01 | 1.25 (1.08, 1.46) p < 0.01 |
| Cake | 1.47 (1.32, 1.63) p < 0.001 | 1.42 (1.29, 1.57) p < 0.001 | 1.38 (1.25, 1.52) p < 0.001 | 1.04 † (0.96, 1.12) 0.38 | 0.97 (0.87, 1.08) p = 0.55 |
| Crisps | 1.45 (1.32, 1.59) p < 0.001 | 1.48 (1.35, 1.62) p < 0.001 | 1.26 (1.16, 1.37) p < 0.001 | 1.03 † (0.95, 1.11) 0.50 | 1.02 (0.92, 1.14) p = 0.70 |
| Yoghurt | 5.72 (4.30, 7.59) p < 0.001 | 6.86 (4.90, 9.60) p < 0.001 | 4.22 (3.02, 5.90) p < 0.001 | 1.73 (1.25, 2.38) p < 0.01 | 1.20 (0.83, 1.74) p = 0.34 |
| Breakfast cereal | 2.48 (2.09, 2.96) p < 0.001 | 2.61 (2.18, 3.12) p < 0.001 | 2.35 (1.93, 2.88) p < 0.001 | 1.14 (0.95, 1.36) p = 0.15 | 1.05 (0.87, 1.27) p = 0.60 |
| MTL vs. Control RR (95%CI) | N-S vs. Control RR (95%CI) | WL vs. Control RR (95%CI) | PC vs. Control RR (95%CI) | N-S vs. MTL RR (95%CI) | |
|---|---|---|---|---|---|
| Pizza | 2.66 (1.72, 4.11) p < 0.001 | 2.70 (1.76, 4.15) p < 0.001 | 2.36 (1.51, 3.67) p < 0.001 | 0.90 (0.56, 1.46) 0.67 | 1.02 (0.78, 1.33) p = 0.90 |
| Drink | 4.27 (2.36, 7.74) p < 0.001 | 6.10 (3.43, 10.84) p < 0.001 | 2.95 (1.61, 5.41) p < 0.001 | 2.37 (1.17, 4.77) p < 0.001 | 1.43 (1.04, 1.96) p = 0.03 |
| Cake | 6.89 (3.80, 12.50) p < 0.001 | 6.21 (3.46, 11.14) p < 0.001 | 5.60 (3.11, 10.10) p < 0.001 | 0.91 † (0.41, 2.02) 0.82 | 0.90 (0.70, 1.15) p = 0.40 |
| Crisps | 5.28 (3.59, 7.76) p < 0.001 | 5.83 (3.97, 8.56) p < 0.001 | 3.69 (2.46, 5.53) p < 0.001 | 1.40 † (0.82, 2.40) 0.22 | 1.10 (0.90, 1.35) p = 0.34 |
| Yoghurt | 22.36 (13.77, 36.31) p < 0.001 | 22.80 (14.04, 37.04) p < 0.001 | 15.81 (9.69, 25.81) p < 0.001 | 2.92 (1.65, 5.16) p < 0.001 | 1.02 (0.93, 1.12) p = 0.68 |
| Breakfast cereal | 7.03 (4.96, 9.98) p < 0.001 | 7.75 (5.47, 10.97) p < 0.001 | 6.43 (4.51, 9.17) p < 0.001 | 1.95 (1.29, 2.95) p < 0.01 | 1.10 (0.97, 1.25) p = 0.13 |
| MTL vs. Control RR (95%CI) | N-S vs. Control RR (95%CI) | WL vs. Control RR (95%CI) | PC vs. Control RR (95%CI) | N-S vs. MTL RR (95%CI) | |
|---|---|---|---|---|---|
| Score (−5, +5) Regression (coefficients) | 1.7 (1.6, 1.9) p < 0.001 | 2.1 (1.9, 2.2) p < 0.001 | 1.4 (1.3, 1.6) p < 0.001 | 0.1 (−0.02, 0.3) 0.09 | 0.3 (0.2, 0.5) p < 0.001 |
| Education | FOPL Group | ||||
|---|---|---|---|---|---|
| MTL | N-S | WL | PC | Control | |
| Pizza | |||||
| Higher | 427/460 (92.8%) | 462/493 (93.7%) | 411/479 (85.8%) | 358/478 (74.9%) | 333/474 (70.3%) |
| Lower | 155/187 (82.9%) | 178/193 (92.2%) | 152/211 (72.0%) | 133/190 (70.0%) | 123/196 (62.8%) |
| Drink | |||||
| Higher | 209/240 (87.1%) | 232/245 (94.7%) | 205/242 (84.7%) | 160/230 (69.6%) | 143/226 (63.3%) |
| Lower | 77/96 (80.2%) | 74/79 (93.7%) | 75/94 (79.8%) | 61/91 (67.0%) | 53/87 (60.9%) |
| Cake | |||||
| Higher | 406/439 (92.5%) | 426/451 (94.5%) | 383/437 (87.6%) | 302/434 (69.6%) | 303/429 (70.6%) |
| Lower | 187/212 (88.2%) | 164/182 (90.1%) | 164/198 (82.8%) | 109/183 (59.6%) | 114/198 (57.6%) |
| Crisps | |||||
| Higher | 468/500 (93.6%) | 503/533 (94.4%) | 442/520 (85.0%) | 312/477 (65.4%) | 325/526 (61.8%) |
| Lower | 207/239 (86.6%) | 220/239 (92.1%) | 187/233 (80.3%) | 152/230 (66.1%) | 134/226 (59.3%) |
| Yoghurt | |||||
| Higher | 452/521 (86.8%) | 481/545 (88.3%) | 327/515 (63.5%) | 86/520 (16.5%) | 75/532 (14.1%) |
| Lower | 190/234 (81.2%) | 179/227 (78.9%) | 131/232 (56.5%) | 31/224 (13.8%) | 26/229 (11.4%) |
| Breakfast cereal | |||||
| Higher | 460/503 (91.5%) | 477/512 (93.2%) | 380/510 (74.5%) | 224/512 (43.8%) | 191/532 (35.9%) |
| Lower | 198/254 (78.0%) | 187/243 (77.0%) | 166/246 (67.5%) | 75/243 (30.9%) | 76/247 (30.8%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Packer, J.; Russell, S.J.; Ridout, D.; Hope, S.; Conolly, A.; Jessop, C.; Robinson, O.J.; Stoffel, S.T.; Viner, R.M.; Croker, H. Assessing the Effectiveness of Front of Pack Labels: Findings from an Online Randomised-Controlled Experiment in a Representative British Sample. Nutrients 2021, 13, 900. https://doi.org/10.3390/nu13030900
Packer J, Russell SJ, Ridout D, Hope S, Conolly A, Jessop C, Robinson OJ, Stoffel ST, Viner RM, Croker H. Assessing the Effectiveness of Front of Pack Labels: Findings from an Online Randomised-Controlled Experiment in a Representative British Sample. Nutrients. 2021; 13(3):900. https://doi.org/10.3390/nu13030900
Chicago/Turabian StylePacker, Jessica, Simon J. Russell, Deborah Ridout, Steven Hope, Anne Conolly, Curtis Jessop, Oliver J. Robinson, Sandro T. Stoffel, Russell M. Viner, and Helen Croker. 2021. "Assessing the Effectiveness of Front of Pack Labels: Findings from an Online Randomised-Controlled Experiment in a Representative British Sample" Nutrients 13, no. 3: 900. https://doi.org/10.3390/nu13030900
APA StylePacker, J., Russell, S. J., Ridout, D., Hope, S., Conolly, A., Jessop, C., Robinson, O. J., Stoffel, S. T., Viner, R. M., & Croker, H. (2021). Assessing the Effectiveness of Front of Pack Labels: Findings from an Online Randomised-Controlled Experiment in a Representative British Sample. Nutrients, 13(3), 900. https://doi.org/10.3390/nu13030900