
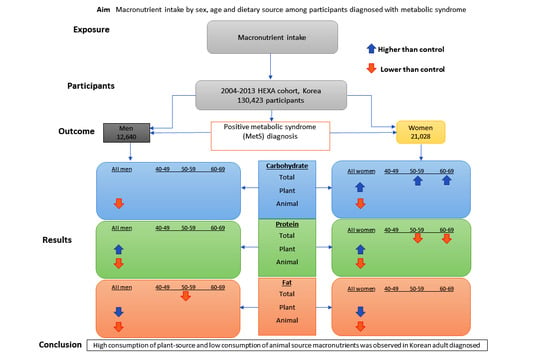
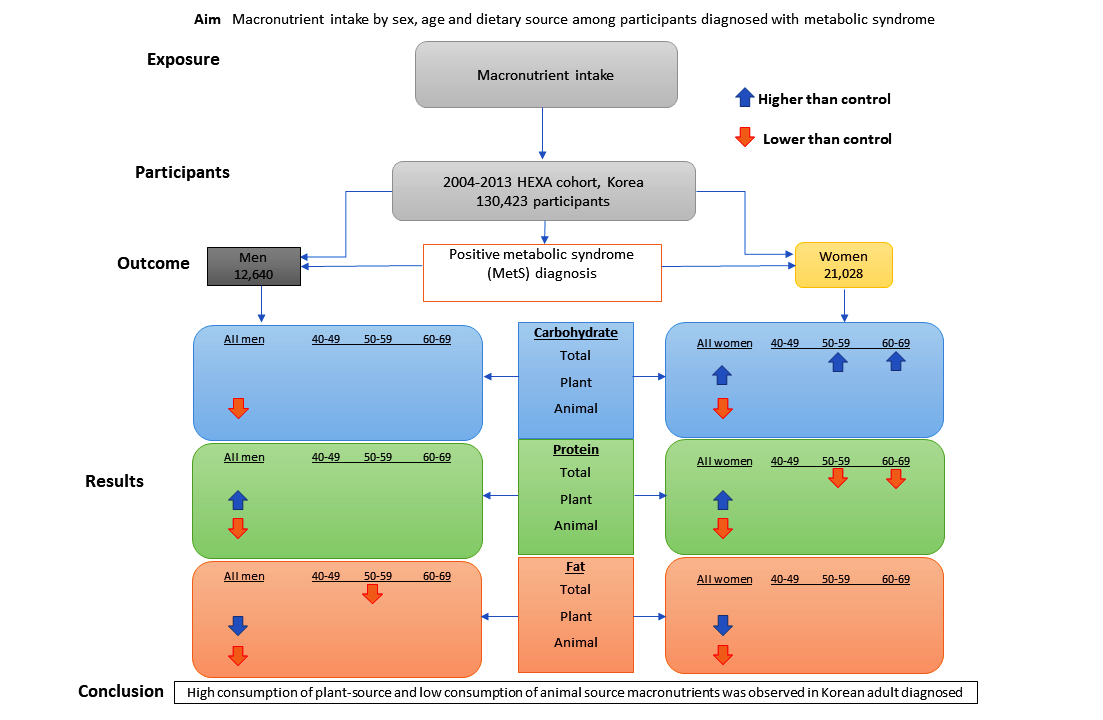
Macronutrient Intake in Adults Diagnosed with Metabolic Syndrome: Using the Health Examinee (HEXA) Cohort


Abstract
1. Introduction
2. Materials and Methods
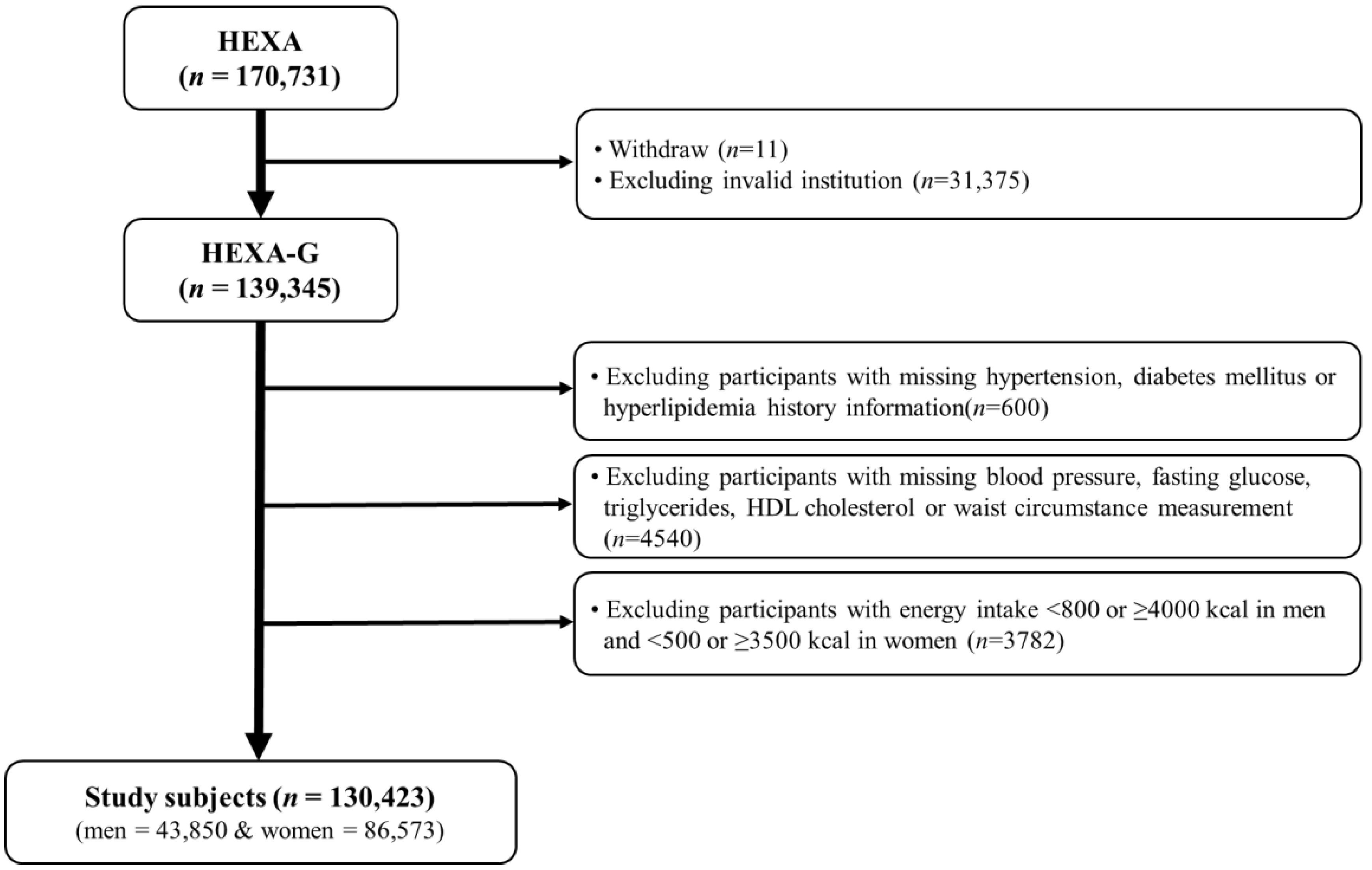
2.1. Study Population
2.2. Dietary Assessment
2.3. Definition of Metabolic Syndrome
2.4. Covariates
2.5. Statistical Analysis
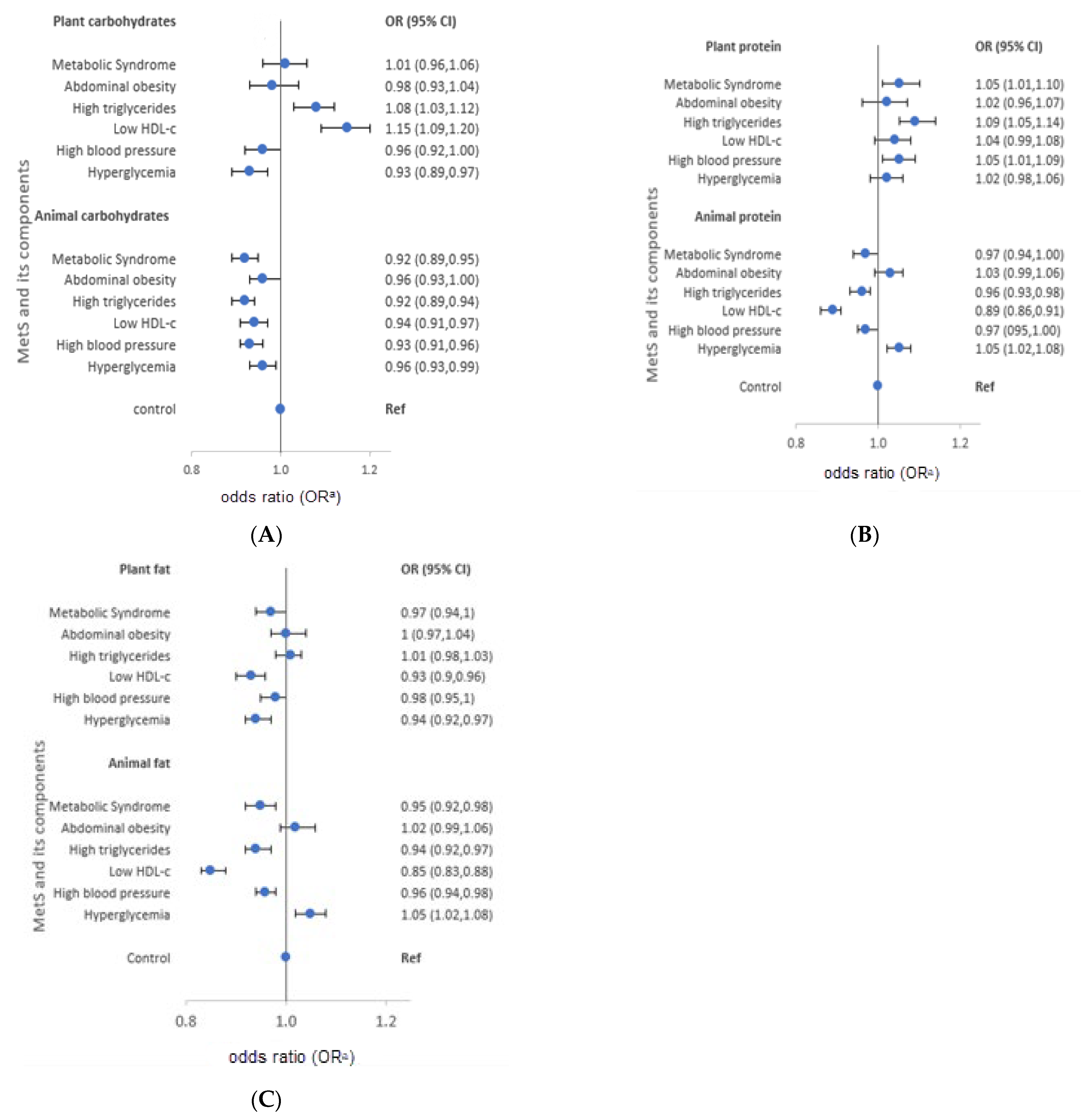
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kassi, E.; Pervanidou, P.; Kaltsas, G.; Chrousos, G. Metabolic syndrome: Definitions and controversies. BMC Med. 2011, 9, 48. [Google Scholar] [CrossRef]
- Ford, E.S.; Li, C.; Sattar, N. Metabolic syndrome and incident diabetes. Diabetes Care 2008, 31, 1898–1904. [Google Scholar] [CrossRef]
- Mottillo, S.; Filion, K.B.; Genest, J.; Joseph, L.; Pilote, L.; Poirier, P.; Rinfret, S.; Schiffrin, E.L.; Eisenberg, M.J. The metabolic syndrome and cardiovascular risk: A systematic review and meta-analysis. J. Am. Coll. Cardiol. 2010, 56, 1113–1132. [Google Scholar] [CrossRef]
- Seuring, T.; Archangelidi, O.; Suhrcke, M.; Archangelidi, O.; Suhrcke, M. The Economic Costs of Type 2 Diabetes: A Global Systematic Review. Pharmacoeconomics 2015, 33, 811–831. [Google Scholar] [CrossRef]
- Gheorghe, A.; Griffiths, U.; Murphy, A.; Legido-Quigley, H.; Lamptey, P.; Perel, P. The economic burden of cardiovascular disease and hypertension in low-and middle-income countries: A systematic review. BMC Public Health 2018, 18, 975. [Google Scholar] [CrossRef]
- Raposo, L.; Severo, M.; Barros, H.; Santos, A.C. The prevalence of the metabolic syndrome in Portugal: The PORMETS study. BMC Public Health 2017, 17, 1–9. [Google Scholar] [CrossRef]
- Aguilar, M.; Bhuket, T.; Torres, S.; Liu, B.; Wong, R.J. Prevalence of the metabolic syndrome in the United States, 2003–2012. JAMA 2015, 313, 1973–1974. [Google Scholar] [CrossRef]
- Lee, S.E.; Han, K.; Kang, Y.M.; Kim, S.-O.; Cho, Y.K.; Ko, K.S.; Park, J.-Y.; Lee, K.-U. Trends in the prevalence of metabolic syndrome and its components in South Korea: Findings from the Korean National Health Insurance Service Database (2009–2013). PLoS ONE 2018, 13, e0194490. [Google Scholar] [CrossRef]
- Lim, S.; Shin, H.; Song, J.H.; Kwak, S.H.; Kang, S.M.; Yoon, J.W.; Choi, S.H.; Cho, S.I.; Park, K.S.; Lee, H.K.; et al. Increasing prevalence of metabolic syndrome in Korea: The Korean National Health and Nutrition Examination Survey for 1998–2007. Diabetes Care 2011, 34, 1323–1328. [Google Scholar] [CrossRef]
- Elder, S.J.; Lichtenstein, A.H.; Pittas, A.G.; Roberts, S.B.; Fuss, P.J.; Greenberg, A.S.; McCrory, M.A.; Bouchard, T.J.; Saltzman, E.; Neale, M.C. Genetic and environmental influences on factors associated with cardiovascular disease and the metabolic syndrome. J. Lipid Res. 2009, 50, 1917–1926. [Google Scholar] [CrossRef]
- Milovanovic, T.; Pantic, I.; Dragasevic, S.; Lugonja, S.; Dumic, I.; Rajilic-Stojanovic, M. The Interrelationship among Non-Alcoholic Fatty Liver Disease, Colonic Diverticulosis and Metabolic Syndrome. J. Gastrointest. Liver Dis. 2021, 30, 1–9. [Google Scholar] [CrossRef]
- de la Iglesia, R.; Loria-Kohen, V.; Zulet, M.A.; Martinez, J.A.; Reglero, G.; de Molina, A.R. Dietary strategies implicated in the prevention and treatment of metabolic syndrome. Int. J. Mol. Sci. 2016, 17, 1877. [Google Scholar] [CrossRef]
- Julibert, A.; Bibiloni, M.D.M.; Tur, J.A. Dietary fat intake and metabolic syndrome in adults: A systematic review. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 887–905. [Google Scholar] [CrossRef]
- Chalvon-Demersay, T.; Azzout-Marniche, D.; Arfsten, J.; Egli, L.; Gaudichon, C.; Karagounis, L.G.; Tomé, D. A systematic review of the effects of plant compared with animal protein sources on features of metabolic syndrome1-3. J. Nutr. 2017, 147, 281–292. [Google Scholar]
- Liu, Y.S.; Wu, Q.J.; Xia, Y.; Zhang, J.Y.; Jiang, Y.T.; Chang, Q.; Zhao, Y.H. Carbohydrate intake and risk of metabolic syndrome: A dose–response meta-analysis of observational studies. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 1288–1298. [Google Scholar] [CrossRef]
- Julibert, A.; Bibiloni, M.D.M.; Mateos, D.; Angullo, E.; Tur, J.A. Dietary fat intake and metabolic syndrome in older adults. Nutrients 2019, 11, 1901. [Google Scholar] [CrossRef]
- Ha, K.; Kim, K.; Chun, O.K.; Joung, H.; Song, Y. Differential association of dietary carbohydrate intake with metabolic syndrome in the US and Korean adults: Data from the 2007–2012 NHANES and KNHANES. Eur. J. Clin. Nutr. 2018, 72, 848–860. [Google Scholar] [CrossRef]
- Chung, S.; Chung, M.Y.; Choi, H.K.; Park, J.H.; Hwang, J.T.; Joung, H. Animal protein intake is positively associated with metabolic syndrome risk factors in middle-aged korean men. Nutrients 2020, 12, 3415. [Google Scholar] [CrossRef]
- Song, S.J.; Lee, J.E.; Song, W.O.; Paik, H.Y.; Song, Y.J. Carbohydrate intake and refined-grain consumption are associated with metabolic syndrome in the korean adult population. J. Acad. Nutr. Diet. 2014, 114, 54–62. [Google Scholar] [CrossRef]
- Kang, D.; Kim, D.H.; Kim, D.H.; Lee, D.H.; Lee, D.H.; Lee, H.J.; Lee, J.K.; Lee, J.T.; Lee, K.H.; Yoon, K.Y.; et al. The health examinees (HEXA) study: Rationale, study design and baseline characteristics. Asian Pac. J. Cancer Prev. 2015, 16, 1591–1597. [Google Scholar]
- Kim, Y.; Han, B.-G. Cohort Profile: The Korean Genome and Epidemiology Study (KoGES) Consortium. Int. J. Epidemiol. 2017, 46, e20. [Google Scholar] [CrossRef]
- Shin, S.; Lee, H.-W.; Kim, C.; Lim, J.; Lee, J.; Lee, S.-A.; Kang, D. Egg Consumption and Risk of Metabolic Syndrome in Korean Adults: Results from the Health Examinees Study. Nutrients 2017, 9, 687. [Google Scholar] [CrossRef]
- Ahn, Y.; Kwon, E.; Shim, J.E.; Park, M.K.; Joo, Y.; Kimm, K.; Park, C.; Kim, D.H. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur. J. Clin. Nutr. 2007, 61, 1435–1441. [Google Scholar] [CrossRef]
- Rural Development Administration. National Institute of Agricultural Sciences. Korean Food Composition Table. 9th Revision. 2016. Available online: http://koreanfood.rda.go.kr/eng/fctFoodSrchEng/engMain (accessed on 7 May 2021).
- Korean Center for Disease Control and Prevention. Korean Genome and Epidemiology Study. Manual of Korean Genome and Epidemiology Study-Food Frequency Questionnaire. 2019. Available online: https://www.kdca.go.kr/contents.es?mid=a40504100200 (accessed on 9 December 2021).
- National Cholesterol Education Program (NCEP). Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, evaluation, and treatment of High Blood cholesterol in adults (adult Treatment Panel III) Final Report. Circulation 2002, 106, 3143–3421. [Google Scholar]
- Alberti, K.G.M.M.; Zimmet, P.; Shaw, J. Metabolic syndrome-A new world-wide definition. A consensus statement from the International Diabetes Federation. Diabet. Med. 2006, 23, 469–480. [Google Scholar] [CrossRef]
- Sanders, A.E.; Slade, G.D.; Beck, J.D.; Ágústsdóttir, H. Secondhand smoke and periodontal disease: Atherosclerosis Risk in Communities study. Am. J. Public Health 2011, 101 (Suppl. 1), S339–S346. [Google Scholar] [CrossRef]
- Yang, J.J.; Song, M.; Yoon, H.-S.; Lee, H.-W.; Lee, Y.; Lee, S.-A.; Choi, J.-Y.; Lee, J.-K.; Kang, D.; Wei, Q.-Y. What Are the Major Determinants in the Success of Smoking Cessation: Results from the Health Examinees Study. PLoS ONE 2015, 10, e0143303. [Google Scholar] [CrossRef]
- Delavar, M.A.; Lye, M.-S.; Lin Khor, G.; Tajuddin, S.; Syed, B.; Hanachi, P. Dietary patterns and the metabolic syndrome in middle aged women, Babol, Iran. Asia Pac. J. Clin. Nutr. 2009, 18, 285–292. [Google Scholar]
- Cabello-Saavedra, E.; Bes-Rastrollo, M.; Alfredo Martinez, J.; Diez-Espino, J.; Buil-Cosiales, P.; Serrano-Martinez, M.; Serrano-Martinez, M.; Martinez-Gonzalez, A. Macronutrient Intake and Metabolic Syndrome in Subjects at High Cardiovascular Risk. Ann. Nutr. Metab. 2010, 56, 152–159. [Google Scholar] [CrossRef]
- Moon, H.-K.; Kong, J.-E. Assessment of Nutrient Intake for Middle Aged with and without Metabolic Syndrome Using 2005 and 2007 Korean National Health and Nutrition Survey. J. Nutr. 2010, 43, 69–78. [Google Scholar] [CrossRef][Green Version]
- Vasbinder, A.; Tinker, L.F.; Neuhouser, M.L.; Pettinger, M.; Hale, L.; Di, C.; Zaslavsky, O.; Hayman, L.L.; Lin, X.; Eaton, C.; et al. Risk of metabolic syndrome and metabolic phenotypes in relation to biomarker-calibrated estimates of energy and protein intakes: An investigation from the Women’s Health Initiative. Am. J. Clin. Nutr. 2021, 113, 706–715. [Google Scholar] [CrossRef]
- Nabuco, H.C.G.; Tomeleri, C.M.; Sugihara Junior, P.; dos Reis Fernandes, R.; Cavalcante, E.F.; Antunes, M.; Burini, R.C.; Venturini, D.; Barbosa, D.S.; Silva, A.M. Lower protein and higher carbohydrate intake are related with altering metabolic syndrome components in elderly women: A cross-sectional study. Exp. Gerontol. 2018, 103, 132–137. [Google Scholar] [CrossRef]
- Skilton, M.R.; Laville, M.; Cust, A.E.; Moulin, P.; Bonnet, F. The association between dietary macronutrient intake and the prevalence of the metabolic syndrome. Br. J. Nutr. 2021, 100, 400–407. [Google Scholar] [CrossRef]
- Murakami, K.; Livingstone, M.B.E. Prevalence and characteristics of misreporting of energy intake in US adults: NHANES 2003-2012. Br. J. Nutr. 2015, 114, 1294–1303. [Google Scholar] [CrossRef]
- Gemming, L.; Jiang, Y.; Swinburn, B.; Utter, J.; Mhurchu, C. Under-reporting remains a key limitation of self-reported dietary intake: An analysis of the 2008/09 New Zealand Adult Nutrition Survey. Eur. J. Clin. Nutr. 2014, 68, 259–264. [Google Scholar] [CrossRef]
- Kye, S.; Kwon, S.-O.; Lee, S.-Y.; Lee, J.; Kim, B.H.; Suh, H.-J.; Moon, H.-K. Under-reporting of Energy Intake from 24-hour Dietary Recalls in the Korean National Health and Nutrition Examination Survey. Osong Public Health Res. Perspect. 2014, 5, 85–91. [Google Scholar] [CrossRef]
- Hoyas, I.; Leon-Sanz, M. Nutritional Challenges in Metabolic Syndrome. J. Clin. Med. 2019, 8, 1301. [Google Scholar] [CrossRef]
- Jung, W.S.; Park, H.Y.; Kim, S.W.; Lim, K. Sex-specific energy intakes and physical activity levels according to the presence of metabolic syndrome in korean elderly people: Korean national health and nutrition examination survey 2016–2018. Int. J. Environ. Res. Public Health 2020, 17, 5416. [Google Scholar] [CrossRef]
- Park, H.S.; Kim, S.M.; Lee, J.S.; Lee, J.; Han, J.H.; Yoon, D.K.; Baik, S.H.; Choi, D.S.; Choi, K.M. Prevalence and trends of metabolic syndrome in Korea: Korean National Health and Nutrition Survey 1998–2001. Diabetes Obes. Metab. 2007, 9, 50–58. [Google Scholar] [CrossRef]
- Jeppesen, J.; Schaaf, P.; Jones, C.; Zhou, M.Y.; Chen, Y.D.; Reaven, G.M. Effects of low-fat, high-carbohydrate diets on risk factors for ischemic heart disease in postmenopausal women. Am. J. Clin. Nutr. 1997, 65, 1027–1033. [Google Scholar] [CrossRef]
- Lee, Y.J.; Song, S.J.; Song, Y.J. High-carbohydrate diets and food patterns and their associations with metabolic disease in the Korean population. Yonsei Med. J. 2018, 59, 834–842. [Google Scholar] [CrossRef] [PubMed]
- Oh, H.Y.; Kim, M.K.; Lee, M.; Kim, Y.O. Macronutrient Composition and Sodium Intake of Diet Are Associated with Risk of Metabolic Syndrome and Hypertension in Korean Women. PLoS ONE 2013, 8, e78088. [Google Scholar]
- Kim, K.; Yun, S.H.; Choi, B.Y.; Kim, M.K. Cross-sectional relationship between dietary carbohydrate, glycaemic index, glycaemic load and risk of the metabolic syndrome in a Korean population. Br. J. Nutr. 2008, 100, 576–584. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.; Lee, K.; Lee, J.; Kim, J. Grain Subtype and the Combination of Grains Consumed Are Associated with the Risk of Metabolic Syndrome: Analysis of a Community-Based Prospective Cohort. J. Nutr. 2020, 150, 118–127. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Sasaki, S.; Takahashi, Y.; Okubo, H.; Hosoi, Y.; Horiguchi, H.; Oguma, E.; Kayama, F. Dietary glycemic index and load in relation to metabolic risk factors in Japanese female farmers with traditional dietary habits. Am. J. Clin. Nutr. 2006, 83, 1161–1169. [Google Scholar] [CrossRef]
- Augustin, L.S.A.; Kendall, C.W.C.; Jenkins, D.J.A.; Willett, W.C.; Astrup, A.; Barclay, A.W.; Björck, I.; Brand-Miller, J.C.; Brighenti, F.; Buyken, A.E.; et al. Glycemic index, glycemic load and glycemic response: An International Scientific Consensus Summit from the International Carbohydrate Quality Consortium (ICQC). Nutr. Metab. Cardiovasc. Dis. 2015, 25, 795–815. [Google Scholar] [CrossRef]
- Yun, S.; Kim, H.J.; Oh, K. Trends in energy intake among Korean adults, 1998-2015: Results from the Korea National Health and Nutrition Examination Survey. Nutr. Res. Pract. 2017, 11, 147–154. [Google Scholar] [CrossRef]
- Park, S.; Ahn, J.; Lee, B.K. Very-low-fat diets may be associated with increased risk of metabolic syndrome in the adult population. Clin. Nutr. 2016, 35, 1159–1167. [Google Scholar] [CrossRef]
- Jun, S.; Ha, K.; Chung, S.; Joung, H. Meat and milk intake in the rice-based Korean diet: Impact on cancer and metabolic syndrome. Proc. Nutr. Soc. 2016, 75, 374–384. [Google Scholar] [CrossRef]
- Kim, J. Dairy food consumption is inversely associated with the risk of the metabolic syndrome in Korean adults. J. Hum. Nutr. Diet. 2013, 26, 171–179. [Google Scholar] [CrossRef]
- Kwon, H.T.; Lee, C.M.; Park, J.H.; Ko, J.A.; Seong, E.J.; Park, M.S.; Cho, B.L. Milk intake and its association with metabolic syndrome in Korean: Analysis of the third Korea national health and nutrition examination survey (KNHANES III). J. Korean Med. Sci. 2010, 25, 1473–1479. [Google Scholar] [CrossRef]
- Shin, H.; Yoon, Y.S.; Lee, Y.; Kim, C.I.L.; Oh, S.W. Dairy product intake is inversely associated with metabolic syndrome in Korean adults: Anseong and ansan cohort of the Korean genome and epidemiology study. J. Korean Med. Sci. 2013, 28, 1482–1488. [Google Scholar] [CrossRef]
- Otsuka, R.; Imai, T.; Kato, Y.; Ando, F.; Shimokata, H. Relationship between number of metabolic syndrome components and dietary factors in middle-aged and elderly Japanese subjects. Hypertens. Res. 2010, 33, 548–554. [Google Scholar] [CrossRef]
- Ministry of Health and Welfare, Centers for Disease Control and Prevention. Korea health statistics 2019. Korean National Health and Nutrition Examination Survey (KNHANES VIII-1). 2019. Available online: https://knhanes.kdca.go.kr/knhanes/sub04/sub04_04_01.do (accessed on 12 December 2021).
- Park, H.A. Adequacy of protein intake among Korean Elderly: An analysis of the 2013-2014 Korea National Health and Nutrition Examination Survey Data. Korean J. Fam. Med. 2018, 39, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Kyung Paik, J.; Park, M.; Shin, J.E.; Jang, S.Y.; Shin, J.Y. Dietary protein to carbohydrate ratio and incidence of metabolic syndrome in Korean adults based on a long-term prospective community-based cohort. Nutrients 2020, 12, 1–13. [Google Scholar]
- Tinker, L.F.; Sarto, G.E.; Howard, B.V.; Huang, Y.; Neuhouser, M.L.; Mossavar-Rahmani, Y.; Beasley, J.M.; Margolis, K.L.; Eaton, C.B.; Phillips, L.S.; et al. Biomarker-calibrated dietary energy and protein intake associations with diabetes risk among postmenopausal women from the Women’s Health Initiative. Am. J. Clin. Nutr. 2011, 94, 1600–1606. [Google Scholar] [CrossRef]
- Van Nielen, M.; Feskens, E.J.M.; Mensink, M.; Sluijs, I.; Molina, E.; Amiano, P.; Ardanaz, E.; Balkau, B.; Beulens, J.W.J.; Boeing, H.; et al. Dietary protein intake and incidence of type 2 diabetes in Europe: The EPIC-InterAct case-cohort study. Diabetes Care 2014, 37, 1854–1862. [Google Scholar] [CrossRef] [PubMed]
- Appel, L.J.; Sacks, F.M.; Carey, V.J.; Obarzanek, E.; Swain, J.F.; Miller, E.R.; Conlin, P.R.; Erlinger, T.P.; Rosner, B.A.; Laranjo, N.M.; et al. Effects of protein, monounsaturated fat, and carbohydrate intake on blood pressure and serum lipids: Results of the OmniHeart randomized trial. J. Am. Med. Assoc. 2005, 294, 2455–2464. [Google Scholar] [CrossRef]
- Oh, C.; No, J. Does Protein Intake Affect Metabolic Risk Factors among Older Adults in Korea? J. Obes. Metab. Syndr. 2017, 26, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Shang, X.; Scott, D.; Hodge, A.; English, D.R.; Giles, G.G.; Ebeling, P.R.; Sanders, K.M. Dietary protein from different food sources, incident metabolic syndrome and changes in its components: An 11-year longitudinal study in healthy community-dwelling adults. Clin. Nutr. 2017, 36, 1540–1548. [Google Scholar] [CrossRef]
- Liu, R.; Dang, S.; Yan, H.; Wang, D.; Zhao, Y.; Li, Q.; Liu, X. Association between dietary protein intake and the risk of hypertension: A cross-sectional study from rural western China. Hypertens. Res. 2013, 36, 972–979. [Google Scholar] [CrossRef]
- Hajihashemi, P.; Hassannejad, R.; Haghighatdoost, F.; Mohammadifard, N.; Sadeghi, M.; Roohafza, H.; Sajjadi, F.; Sarrafzadegan, N.l. The long-term association of different dietary protein sources with metabolic syndrome. Sci. Rep. 2021, 11, 1–8. [Google Scholar] [CrossRef]
- Hruby, A.; Jacques, P.F. Dietary protein and changes in markers of cardiometabolic health across 20 years of follow-up in middle-aged Americans. Public Health Nutr. 2018, 21, 2998–3010. [Google Scholar] [CrossRef]
- Buendia, J.R.; Bradlee, M.L.; Singer, M.R.; Moore, L.L. Diets Higher in Protein Predict Lower High Blood Pressure Risk in Framingham Offspring Study Adults. Am. J. Hypertens. 2015, 28, 372. [Google Scholar] [CrossRef]
- Aggarwal, A.; Drewnowski, A. Plant- and animal-protein diets in relation to sociodemographic drivers, quality, and cost: Findings from the Seattle Obesity Study. Am. J. Clin. Nutr. 2019, 110, 451–460. [Google Scholar] [CrossRef]
- Dietary Guidelines for Americans 2015–2020. U.S. Department of Health and Human Services and, U.S. Department of Agriculture. 2015–2020. Dietary Guidelines for Americans. 8th Edition. 2015. Available online: https://health.gov/dietaryguidelines/2015/ (accessed on 25 November 2021).
- Lee, M.-J.; Popkin, B.M.; Kim, S. The unique aspects of the nutrition transition in South Korea: The retention of healthful elements in their traditional diet. Public Health Nutr. 2002, 5, 197–203. [Google Scholar] [CrossRef]
- Ervin, R.B.; Wright, J.D.; Wang, C.-Y.; Kennedy-Stephenson, J. Dietary Intake of Fats and Fatty Acids for the United States Population: 1999–2000; National Center for Health Statistics: Bethesda, MD, USA, 2004.
- Baek, Y.; Hwang, J.-Y.; Kim, K.; Moon, H.-K.; Kweon, S.; Yang, J.; Oh, K.; Shim, J.E. Dietary intake of fats and fatty acids in the Korean population: Korea National Health and Nutrition Examination Survey, 2013. Nutr. Res. Pract. 2015, 9, 650–657. [Google Scholar] [CrossRef]
- Son, J.; Lee, Y.; Park, K. Effects of processed red meat consumption on the risk of type 2 diabetes and cardiovascular diseases among Korean adults: The Korean Genome and Epidemiology Study. Eur. J. Nutr. 2019, 58, 2477–2484. [Google Scholar] [CrossRef]
- Hekmatdoost, A.; Mirmiran, P.; Hosseini-Esfahani, F.; Azizi, F. Dietary fatty acid composition and metabolic syndrome in Tehranian adults. Nutrition 2011, 27, 1002–1007. [Google Scholar] [CrossRef]
- Um, Y.J.; Oh, S.W.; Lee, C.M.; Kwon, H.T.; Joh, H.K.; Kim, Y.J.; Kim, H.J.; Ahn, S.H. Dietary fat intake and the risk of metabolic syndrome in Korean adults. Korean J. Fam. Med. 2015, 36, 245–252. [Google Scholar] [CrossRef]
- Chowdhury, R.; Warnakula, S.; Kunutsor, S.; Crowe, F.; Ward, H.A.; Johnson, L.; Franco, O.H.; Butterworth, A.S.; Forouhi, N.G.; Thompson, S.G.; et al. Association of dietary, circulating, and supplement fatty acids with coronary risk: A systematic review and meta-analysis. Ann. Intern. Med. 2014, 160, 398–406. [Google Scholar] [CrossRef] [PubMed]
- McCaulley, M. Association of dietary, circulating, and supplement fatty acids with coronary risk. Annals of internal medicine. Am. Coll. Physicians 2014, 161, 456. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Men (n = 43,850) | Women (n = 86,573) | |||||
|---|---|---|---|---|---|---|
| MetS (n = 12,640) | Control (n = 31,210) | OR (95% CI) b | MetS (n = 21,028) | Control (n = 65,545) | OR (95% CI) b | |
| Age (years) a | 55 (48,61) | 53 (46,60) | 1.03 (1.03–1.04) | 57 (51,62) | 50 (45,56) | 1.07 (1.06–1.07) |
| Body mass index (kg/m2) a | 26.0 (24.5,27.7) | 23.7 (22.1,25.3) | 1.51 (1.49–1.53) | 25.4 (23.7,27.4) | 22.7 (21.2,24.5) | 1.40 (1.39–1.42) |
| Marital status | ||||||
| No | 5.7 | 5.8 | Ref. | 15.4 | 12.5 | Ref. |
| Yes | 94.3 | 94.2 | 0.94 (0.84–1.05) | 84.6 | 87.5 | 1.04 (0.98–1.10) |
| Education (%) | ||||||
| <12 years | 58.8 | 55.0 | Ref. | 86.8 | 72.3 | Ref. |
| ≥12 years | 41.2 | 45.0 | 0.89 (0.85–0.94) | 13.2 | 27.7 | 0.75 (0.71–0.79) |
| Family income (%) | ||||||
| <000 USD/month | 51.4 | 49.9 | Ref. | 68.3 | 52.1 | Ref. |
| ≥3000 USD/month | 48.6 | 50.1 | 0.95 (0.90–1.01) | 31.7 | 47.9 | 0.87 (0.83–0.91) |
| Occupied (%) | ||||||
| No | 20.9 | 17.8 | Ref. | 67.0 | 58.2 | Ref. |
| Yes | 79.1 | 82.2 | 1.20 (1.12–1.28) | 33.0 | 41.8 | 1.12 (1.08–1.17) |
| Current smoker (%) | ||||||
| No | 65.8 | 69.1 | Ref. | 97.6 | 97.7 | Ref. |
| Yes | 34.2 | 30.9 | 1.37 (1.30–1.45) | 2.4 | 2.3 | 1.34 (1.18–1.53) |
| Current drinker (%) | ||||||
| No | 26.1 | 27.6 | Ref. | 76.5 | 67.1 | Ref. |
| Yes | 73.9 | 72.5 | 1.09 (1.03–1.16) | 23.5 | 32.9 | 0.80 (0.76–0.84) |
| Regular exercise (%) | ||||||
| No | 44.7 | 42.1 | Ref. | 51.5 | 48.0 | Ref. |
| Yes | 55.3 | 57.9 | 0.85 (0.81–0.89) | 48.5 | 52.0 | 0.90 (0.86–0.94) |
| Energy (Kcal/day) | Carbohydrate (g/day) | Protein (g/day) | Fat (g/day) | |||||
|---|---|---|---|---|---|---|---|---|
| Case/Control a | OR (95% CI) b | Case/Control a | OR (95% CI) b | Case/Control a | OR (95% CI) b | Case/Control a | OR (95% CI) b | |
| Men | ||||||||
| MetS | 1789 (1525,2125)/ 1781 (1516,2117) | 0.95 (0.92–0.98) | 318 (277,370)/ 317 (276,368) | 0.97 (0.93–1.03) | 59.5 (47,75)/ 58.4 (47,74) | 0.98 (0.94–1.02) | 27.4 (19,38)/ 27.3 (19,38) | 0.93 (0.90–0.96) |
| Abdominal obesity | 1821 (1546,2171)/ 1769 (1508,2100) | 1.08 (1.05–1.12) | 321 (279,377)/ 316 (275,366) | 0.97 (0.91–1.03) | 60.7 (48,77)/ 57.8 (46,73) | 1.04 (0.99–1.10) | 28.4 (20,40)/ 26.9 (19,37) | 1.03 (0.99–1.07) |
| High triglycerides | 1791 (1526,2129)/ 1778 (1514,2113) | 0.97 (0.95–1.00) | 318 (277,371)/ 317 (276,368) | 1.05 (1.00–1.10) | 59.3 (47,74)/ 58.3 (47,74) | 0.98 (0.94–1.01) | 27.7 (19,38)/ 27.1 (19,38) | 0.94 (0.91–0.97) |
| Low HDL-c | 1778 (1512,2109)/ 1785 (1520,2122) | 0.94 (0.92–0.97) | 319 (278,370)/ 317 (276,369) | 1.14 (1.08–1.20) | 57.9 (46,73)/ 59.0 (47,74) | 0.87 (0.83–0.90) | 26.3 (18,37)/ 27.6 (19,39) | 0.81 (0.78–0.84) |
| High blood pressure | 1776 (1514,2109)/ 1791 (1526,2132) | 0.94 (0.92–0.97) | 316 (276,366)/ 319 (277,372) | 0.93 (0.89–0.97) | 58.6 (47,74)/ 58.8 (47,74) | 0.98 (0.95–1.02) | 26.9 (19,38)/ 27.8 (20,39) | 0.94 (0.92–0.97) |
| Hyperglycemia | 1768 (1508,2100)/ 1791 (1524,2129) | 0.95 (0.93–0.98) | 315 (275,365)/ 319 (277,371) | 0.91 (0.87–0.95) | 58.8 (47,74)/ 58.7 (47,74) | 1.07 (1.04–1.11) | 26.9 (19,38)/ 27.5 (19,38) | 1.02 (0.99–1.05) |
| Women c | ||||||||
| MetS | 1617 (1351,1924)/ 1652 (1359,1976) | 0.97 (0.95–0.99) | 300 (251,347)/ 300 (244,351) | 1.14 (1.08–1.19) | 51.8 (41,66)/ 54.0 (42,69) | 0.90 (0.87–0.94) | 20.9 (14,30)/ 24.0 (17,34) | 0.80 (0.77–0.83) |
| Abdominal obesity | 1643 (1367,1957)/ 1643 (1349,1967) | 1.04 (1.02–1.06) | 302 (251,350)/ 299 (242,350) | 1.02 (0.98–1.07) | 53.2 (42,68)/ 53.6 (42,68) | 1.01 (0.98–1.05) | 22.3 (15,32)/ 23.8 (16,34) | 0.96 (0.93–0.99) |
| High triglycerides | 1624 (1346,1940)/ 1648 (1360,1971) | 0.99 (0.97–1.01) | 300 (248,349)/ 300 (245,350) | 1.11 (1.07–1.16) | 52.0 (41,66)/ 53.9 (42,68) | 0.90 (0.87–0.93) | 21.3 (14,31)/ 23.8 (16,34) | 0.84 (0.82–0.87) |
| Low HDL-c | 1629 (1356,1943)/ 1652 (1358,1976) | 0.97 (0.95–0.99) | 300 (249,349)/ 300 (244,351) | 1.17 (1.13–1.21) | 52.4 (41,67)/ 54.1 (42,69) | 0.91 (0.88–0.93) | 21.6 (15,31)/ 24.1 (17,34) | 0.79 (0.77–0.81) |
| High blood pressure | 1619 (1346,1928)/ 1658 (1364,1983) | 0.97 (0.96–0.99) | 299 (247,347)/ 301 (245,352) | 1.08 (1.04–1.12) | 52.3 (41,66)/ 54.2 (42,69) | 0.99 (0.97–1.02) | 21.6 (15,31)/ 24.2 (17,34) | 0.93 (0.90–0.95) |
| Hyperglycemia | 1616 (1338,1927)/ 1649 (1362,1972) | 0.96 (0.94–0.98) | 297 (245,345)/ 301 (246,352) | 0.93 (0.90–0.97) | 52.3 (41,67)/ 53.7 (42,68) | 1.04 (1.01–1.08) | 21.7 (15,32)/ 23.5 (16,34) | 0.99 (0.97–1.02) |
| Men | Women | |||||
|---|---|---|---|---|---|---|
| MetS a | Control a | OR (95% CI) b | MetS a | Control a | OR (95% CI) b | |
| Energy (kcal/day) | ||||||
| 40–49 | 1875 (1590,2241) | 1846 (1568,2217) | 0.96 (0.91–1.00) | 1699 (1404,2044) | 1703 (1393,2039) | 0.97 (0.93–1.02) |
| 50–59 | 1778 (1525,2111) | 1774 (1511,2096) | 0.94 (0.89–0.98) | 1632 (1367,1937) | 1635 (1342,1947) | 0.97 (0.94–1.00) |
| 60–69 | 1727 (1473,2032) | 1711 (1471,2013) | 0.97 (0.92–1.02) | 1564 (1310,1842) | 1571 (1308,1865) | 0.97 (0.92–1.01) |
| Carbohydrate (g/day) | ||||||
| 40–49 | 327 (280,386) | 324 (279,382) | 0.99 (0.91–1.08) | 307 (252,359) | 305 (246,358) | 1.05 (0.97–1.14) |
| 50–59 | 316 (277,368) | 317 (276,366) | 0.95 (0.88–1.04) | 302 (253,349) | 299 (243,349) | 1.14 (1.07–1.21) |
| 60–69 | 312 (274,359) | 311 (273,356) | 0.99 (0.89–1.09) | 295 (247,339) | 293 (242,338) | 1.17 (1.08–1.27) |
| Protein (g/day) | ||||||
| 40–49 | 63.1 (51,79) | 61.4 (49,78) | 1.00 (0.93–1.07) | 55.7 (44,71) | 56.1 (44,71) | 0.99 (0.93–1.06) |
| 50–59 | 59.3 (47,74) | 58.3 (46,73) | 0.96 (0.90–1.03) | 52.4 (42,67) | 53.3 (42,68) | 0.90 (0.86–0.95) |
| 60–69 | 56.4 (45,71) | 55.1 (44,70) | 0.97 (0.89–1.05) | 49.3 (39,62) | 50.0 (40,64) | 0.88 (0.82–0.94) |
| Fat (g/day) | ||||||
| 40–49 | 31.5 (23,43) | 30.7 (22,42) | 0.94 (0.89–1.00) | 25.3 (18,36) | 26.5 (19,37) | 0.87 (0.82–0.92) |
| 50–59 | 26.8 (19,37) | 26.8 (19,37) | 0.91 (0.86–0.97) | 21.2 (15,30) | 22.8 (16,32) | 0.81 (0.77–0.85) |
| 60–69 | 24.4 (17,35) | 23.9 (17,34) | 0.94 (0.87–1.00) | 18.4 (12,27) | 19.6 (14,29) | 0.78 (0.73–0.83) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, H.; Kityo, A.; Kim, Y.; Lee, S.-A. Macronutrient Intake in Adults Diagnosed with Metabolic Syndrome: Using the Health Examinee (HEXA) Cohort. Nutrients 2021, 13, 4457. https://doi.org/10.3390/nu13124457
Park H, Kityo A, Kim Y, Lee S-A. Macronutrient Intake in Adults Diagnosed with Metabolic Syndrome: Using the Health Examinee (HEXA) Cohort. Nutrients. 2021; 13(12):4457. https://doi.org/10.3390/nu13124457
Chicago/Turabian StylePark, Hyerim, Anthony Kityo, Yeonjin Kim, and Sang-Ah Lee. 2021. "Macronutrient Intake in Adults Diagnosed with Metabolic Syndrome: Using the Health Examinee (HEXA) Cohort" Nutrients 13, no. 12: 4457. https://doi.org/10.3390/nu13124457
APA StylePark, H., Kityo, A., Kim, Y., & Lee, S.-A. (2021). Macronutrient Intake in Adults Diagnosed with Metabolic Syndrome: Using the Health Examinee (HEXA) Cohort. Nutrients, 13(12), 4457. https://doi.org/10.3390/nu13124457