Abstract
Several brands of water enriched with O2 (O2-waters) are commercially available and are advertised as wellness and fitness waters with claims of physiological and psychological benefits, including improvement in exercise performance. However, these claims are based, at best, on anecdotal evidence or on a limited number of unreliable studies. The purpose of this double-blind randomized study was to compare the effect of two O2-waters (~110 mg O2·L−1) and a placebo (10 mg O2·L−1, i.e., close to the value at sea level, 9–12 mg O2·L−1) on the cardiopulmonary responses and on performance during high-intensity exercise. One of the two O2-waters and the placebo were prepared by injection of O2. The other O2-water was enriched by an electrolytic process. Twenty male subjects were randomly allocated to drink one of the three waters in a crossover study (2 L·day−1 × 2 days and 15 mL·kg−1 90 min before exercise). During each exercise trial, the subjects exercised at 95.9 ± 4.7% of maximal workload to volitional fatigue. Exercise time to exhaustion and the cardiopulmonary responses, arterial lactate concentration and pH were measured. Oxidative damage to proteins, lipids and DNA in blood was assessed at rest before exercise. Time to exhaustion (one-way ANOVA) and the responses to exercise (two-way ANOVA [Time; Waters] with repeated measurements) were not significantly different among the three waters. There was only a trend (p = 0.060) for a reduction in the time constant of the rapid component of VO2 kinetics with the water enriched in O2 by electrolysis. No difference in oxidative damage in blood was observed between the three waters. These results suggest that O2-water does not speed up cardiopulmonary response to exercise, does not increase performance and does not trigger oxidative stress measured at rest.
1. Introduction
At equilibrium with partial pressure at sea level (PO2 ~160 mmHg) and for temperature ranging between 10 and 25 °C, the amount of O2 dissolved in water ranges respectively between 12 and 9 mg·L−1 [1] (Box 1). However, several commercially available brands of water are purportedly enriched in O2 (O2-waters) at 7 and 40 times this basal value [2,3,4] and are advertised as wellness and fitness waters with a large range of physiological and psychological benefits. As discussed by several authors [2,3,5,6], these claims are based at best on anecdotal evidences or on a limited number of unreliable studies.
Box 1. Relationship between PO2 and temperature, and O2 content of water according to Henry’s law [1] expressed in various units: mol·L−1, mL·L−1, mg·L−1 and ppm, at sea level, 10 °C and dry air.
The amount of O2 dissolved in water (mol·L−1)
depends on the temperature (T in K = T[°C] + 273) and PO2
(in atmosphere: atm) and is described by Henry’s law where 769.23 and 1700
are Henry’s constants for O2:
O2
content (mol·L−1) = PO2 (atm)/{769.23 ×
exp [−1700 × (1/T − 1/298)}
For example, at sea level (PO2 = 160 mmHg or
0.21 atm in dry air) and 10 °C (283 K):
O2 content (mol.L−1) = 0.21
(atm)/{769.23 × exp [−1700 × (1/283 − 1/298)} = 0.000370 mol·L−1
Since the molar mass of O2 is 32 g and since 1
mol of O2 occupies 22.4 L, the conversion of this O2
content in various other units is as follows:
O2 content in mL·L−1 = O2
content in mol·L−1 × 22.4 × 1000 = 0.000370 × 22.4 × 1000 = 8.29
mL·L−1
O2
content in mg·L−1 = O2 content in mol·L−1 ×
32/1000 = 0.000370 × 32/1000 = 11.8 mg·L−1
Finally, since the molar mass of water is 18 g, there are
1000/18 = 55.5 mol of water·L−1. The O2 content in ppm,
thus is:
O2 content in ppm = O2
content in mol·L−1/H2O content in mol·L−1 =
(0.000370/55.5) × 106 = 6.67 ppm
Consumption of O2-waters is promoted in active subjects, and a dozen studies have been conducted to document their effects, if any, on the response to exercise and on performance (Table 1). However, in some of these studies, the characteristics of the water ingested, including the O2-content, were not precisely described, and the volume ingested was not indicated. In only two studies [2,7], the O2 content measured and/or reported appears reliable and in the range of values for which benefits are claimed by the manufacturers. In these two studies, O2-waters consumption did not improve maximal oxygen consumption (VO2max) [2,7] and in the study by Leibetseder et al. [7], the only significant difference when the O2-water was ingested was an increase in the ventilatory equivalent of oxygen (pulmonary ventilation/O2 consumption or VE/VO2) at sub-maximal exercise and in plasma lactate concentration at maximal exercise. As discussed by the authors, it is difficult to speculate about the physiological significance of these changes, their possible effects on performance and how they could be related to ingestion of the O2-water, but these findings suggest that O2-waters could modify the cardiopulmonary response to exercise.

Table 1.
Studies of the effects of O2-water ingestion on performance and on the response to exercise.
As already discussed [2,4,8], ingestion of water enriched in O2 is unlikely to directly modify oxygen consumption (VO2) at the mouth during exercise. In addition, in arterial blood, the amount of dissolved O2 is very small compared to the amount carried by hemoglobin, and in healthy subjects exercising at sea-level or a low altitude (<1000 m), arterial hemoglobin saturation remains close to normal values. It is, thus, very unlikely that increasing O2 delivery to the blood through the gut will markedly increase PO2 and O2 content in arterial blood and, thus, O2 delivery to any organ or tissue, including exercising muscles. However, we have previously studied the effects of a water enriched in O2, using an electrolytic process [9,10,11]. When compared to injection of O2, this process could generate water superstructures called clathrates, which could trap solutes, such as O2, and which can facilitate O2 diffusion along PO2 gradients [12,13,14]. This hypothesis is consistent with the higher tissue oxygenation observed in anaesthetized pigs [11] and the higher mitochondrial respiration observed at low PO2 in permeabilized rat muscle fibers [10] with water enriched by electrolysis vs. injection.
It have shown that the fast component of VO2 kinetics at the mouth in response to constant load exercise reflects O2 diffusion from the blood to muscle fibers [15]. Therefore, the aim of this study was to investigate the effect of O2-waters on the cardiopulmonary and acid–base responses during near maximal exercise continued to exhaustion. We hypothesized that the fast component of the kinetics of VO2 in response to high-intensity exercise could be faster following ingestion of the water enriched in O2 by electrolysis vs. injection or a control water with a low O2 content. A faster adjustment of VO2 at the onset of exercise could increase the time to exhaustion. Finally, it has been suggested that ingestion of O2-waters can be a safety issue because of production of reactive oxygen species (ROS) [5,6,16,17]. We, thus, also investigated the presence of ROS induces damages, including DNA damages, using the comet assay.
2. Methods
2.1. Subjects
Twenty active and healthy male subjects, recruited through advertisements in the hospital and university communities, volunteered for this study, which was approved by the local ethic committee (Comité de Protection des Personnes Est IV, Strasbourg, France: Eudract No.2008-A01051-54). Their age, height, body mass and percent body fat were respectively 22.8 ± 4.1 years, 178.7 ± 5.9 cm, 70.0 ± 5.7 kg and 13.0 ± 1.6% (mean ± SD). In accordance with the declaration of Helsinki, all participants signed an informed-consent form. The sample size was determined based on the significant difference in plasma lactate concentration at maximal exercise between the control and O2-water by Leibetseder et al. [7] (9.6 vs. 11.1 mmol·L−1 with SD = 1.6 mmol·L−1). These data indicated that 18 subjects were needed to detect a difference with an 80% power and p = 0.05 [25].
2.2. Study Design
The participants visited the laboratory on four separate occasions. All experimental conditions were conducted in a climate-controlled laboratory at Strasbourg Hospital. The first session was used to determine the VO2max and maximal power output by an incremental test to exhaustion. On the subsequent three visits separated by at least 5 days, the subjects performed an exercise trial to volitional fatigue. The study was randomized and double blind. The cardiopulmonary and acid–base response and time to exhaustion were measured.
2.3. Determination of VO2max and Pmax
VO2max and the corresponding workload (Pmax) were measured before the first experimental trial on cycle ergometer (Ergoline 900, Ergoline, Schiller, France), using an incremental test to volitional fatigue, as previously described [26]. The VO2 and carbon dioxide production (VCO2) were computed from breath-by-breath measurement of gas exchanges at the mouth (Sensor Medics, Yorba Linda, CA, USA) and the heart rate was measured from a 12-lead ECG (Cardiovit CS200, Schiller, Baar, Switzerland). The Pmax was considered to be the lowest workload, eliciting VO2max = 3.63 ± 0.39 L O2·min−1, reached at 276 ± 31 W, with heart rate (HR) = 187 ± 7 bpm and plasma lactate concentration = 12.4 ± 3.3 mmol·L−1.
2.4. O2-Waters Ingested
The waters ingested were prepared from demineralized water, which was remineralized with Na+, SO42− and PO42−. The control water was enriched in O2 by injection (10 mg·L−1, i.e., close to the value at equilibrium with atmospheric O2 at sea level at the temperature of ingestion (5–10 °C)). The two other waters were enriched at ~110 mg·L−1 by injection or electrolysis, as previously described [11]. Their O2 content was found to be 116 and 109 mg·L−1, respectively, for the water enriched in O2 by electrolysis and injection. A very good stability of O2 was found in the two O2-waters. Upon opening and keeping the bottle unagitated at 20 °C, the half-life of the decrease in O2 content was about six days.
2.5. Exercises with Control and O2-Waters
The subjects took part in three similar exercise trials by 5- to 7-day intervals. For two days before each trial, the subjects ingested 2 L·day−1 of the assigned water (~500 mL every 4 h during the wake-up period). The waters were kept in a refrigerator (~5 °C) and were consumed within ~15 min, following removal of the cap. The subjects also ingested 15 mL·kg−1 of the same water 90 min before the beginning of the exercise trial. Over the two-day period preceding each exercise trial, the subjects refrained from exercising and were fed a standardized diet (35 kcal·kg−1·day−1 with 15, 35 and 50% energy from protein, fat and carbohydrate).
During each exercise trial, following a 20-min warm-up and a 5-min rest period, the subjects exercised at Pmax to volitional fatigue. Breath-by-breath gas exchanges were measured for the computation of ventilation (VE), breathing frequency (fR), tidal volume (VT), VO2, VCO2/VO2 (RER) and VE/VO2. The HR was monitored from a 3-lead ECG (Nihon Kohden TEC-5500, Tokyo, Japan), and cardiac output (Qc) was continuously monitored by impedancemetry (Physioflow, Manatec, France). The stroke volume and arterio-venous difference in O2 were computed. Finally, 100 µL blood samples were withdrawn from the arterialized earlobe at rest before exercise and every minute during the exercise period for the measurement of plasma lactate concentration and pH, arterial oxygen and carbon dioxide pressure (PaO2 and PaCO2) and arterial oxygen saturation (SaO2) (Bayer, Bayer series 800, Bayer France; Instrumentation Laboratory, Company, Bedford, MA, USA). PO2 measured in blood sampled at the arterialized earlobe was corrected, as previously suggested [27] (PaO2 [in mmHg] = 1.1 × earlobe PO2 − 3).
2.6. VO2 Kinetics
The time course of the VO2 response at the onset of exercise was described by using a three-component model [28]. Due to methodological considerations, the cardiodynamic phase was excluded by removing the data points in the first 20 s from the analysis [29]. We used a mathematical model with two exponential functions [30]. The parameters of the model were determined using an iterative procedure which minimizes the sum of the mean squares of the differences between VO2 estimates and the corresponding actual values as previously described [31]. The amplitude of the slow component was computed as suggested by Borrani et al. [32]. Aberrant breaths were excluded from the analysis, as previously described [33]. Less than 1% of the data points were excluded.
2.7. ROS Generation and Damages
Blood samples (6 mL) were taken at rest before exercise in an antecubital vein, following ingestion of the waters. These samples were assessed for estimating oxidative stress on lipid species (blood malondialdehyde (MDA) concentration [34]), protein species (preserved thiol groups [34]) and on endogenous antioxidant defenses (reduced and oxidized glutathione [35]; and on DNA [36]).
2.8. Statistical Analyses
Data are reported as mean ± standard deviation (SD). The normality of distribution was verified by using the Shapiro–Wilk test. Comparisons were made by using ANOVA for repeated measurements (one- or two-way [Time; Water], depending on the variable; see results) and Tukey HSD at p < 0.05 (SAS Software version 9.1, SAS Institute, Cary, NC, USA). The effect of time was tested by comparing the values observed before exercise to those observed at min 5:00 and the end of the exercise period, except for RER, for which the comparison was made between the final value and the peak value observed at min 3:30. A two-sided level of 5% for the type 1 error was applied. A significance level between 5 and 10% was considered as a trend.
3. Results
Figure 1 and Figure 2 show the kinetics of VE, VO2, VE/VO2, lactate concentration and of the circulatory adjustments in response to exercise, respectively. Table 2 shows the values of PaO2, PaCO2, SaO2 and pH observed at rest before exercise, at min 5 during the exercise and at the end of exercise.
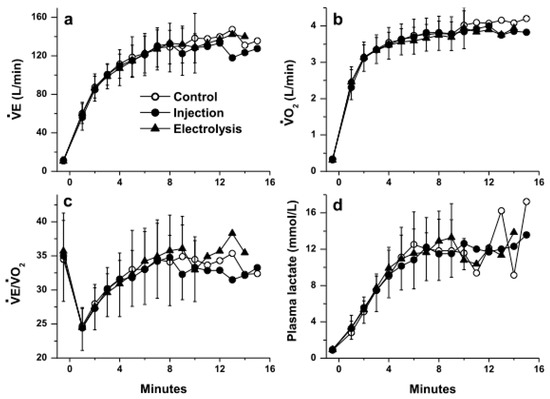
Figure 1.
Pulmonary responses during exercise: (a) pulmonary ventilation (VE), (b) oxygen uptake (VO2), (c) ventilatory equivalent of oxygen and (d) plasma lactate concentration with the three waters (mean ± SD; SD not shown past min 10 because n < 5; no significant difference was observed between the three waters, p > 0.05).
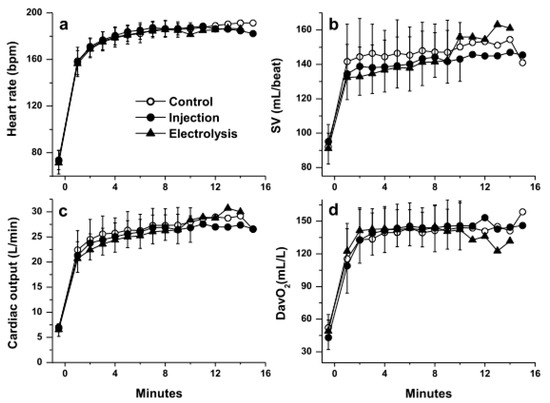
Figure 2.
Circulatory responses during exercise: (a) heart rate, (b) stroke volume (SV), (c) cardiac output and (d) arterio-venous difference in O2 (DavO2) with the three waters (mean ± SD; SD not shown past min 10 because n < 5; no significant difference was observed between the three waters, p > 0.05).
Table 2.
Blood gases and pH.
As expected, in response to high-intensity exercise continued to volitional fatigue, following an early response observed between min 0 and min ~5, some variables levelled off (VT [data not shown], VE/VO2, plasma lactate concentration, pH and PaO2), while others significantly drifted upwards (fR and RER [data not shown], and VCO2, VE, VO2, HR and Qc) or downwards (PaCO2 and SaO2) (Figure 1 and Figure 2). No significant difference was observed between the three waters for any of the variables measures at any time points.
No significant difference was observed for any of the parameters of the VO2 kinetics between the three waters. However, there was a trend for the time constant of the fast component of the kinetics of VO2 (τ1) to be different with the three waters (p = 0.060) due to the large difference between the values computed with the control water and the water enriched in O2 by electrolysis (Tukey HSD, p = 0.0513; the corresponding p-values for the comparison between the control water and the water enriched by injection, and between the two waters enriched in O2 were much larger, at 0.668 and 0.272, respectively) (Table 3).
Table 3.
Pulmonary VO2 kinetics responses.
No significant difference was observed between exercise time to exhaustion with ingestion of the three waters (in min:s: 10:28 ± 3:52, 9:28 ± 3:42, and 9:54 ± 3:38 with control water and the waters enriched in O2 by injection and the electrolytic process), and the values in the three trials were closely correlated (injection vs. control: Pearson r = 0.825; electrolysis vs. control: Pearson r = 0.847; electrolysis vs. injection: Pearson r = 0.875; p < 0.001 for the three correlation coefficients).
No significant difference was observed between the three waters for any of the indices of ROS generation and damages at rest before exercise (Table 4).
Table 4.
Indices of ROS and damages in venous blood samples taken at rest.
4. Discussion
The results from the present experiment indicate that ingestion of waters enriched in O2 by injection or electrolysis at ~11 times the level in the control water did not modify the cardiopulmonary response to high-intensity exercise, the response of plasma lactate concentration and pH, or the response of arterial blood gases. No significant difference was observed between the three waters for the parameters of the kinetics of VO2; however, there was a trend for the fast component to be slightly faster with the water enriched in O2 by the electrolytic process. Finally, ingestion of waters enriched in O2 does not increase time to exhaustion at high exercise intensity, but it also has no adverse effect on the production of ROS and associated damages to lipids, proteins or DNA measured at rest.
These observations are difficult to compare with data in the literature; however, a dozen studies have described the effect of O2-water consumption on the response to exercise (Table 1). In only two of these studies [2,7], the O2 content, which was reported or was computed from the PO2 reported (see Box 1), was higher than the minimal value for which benefits have been claimed in terms of physiological response and performance (about >7 times the value in tap water) and were credible. In three of the ten other studies listed in Table 1, the O2 content of the water ingested was simply not reported [18,20,23]. In four other studies [8,17,21,24], there was no evidence that the O2 content was actually measured, and the values reported are much too high to be credible: the O2 content reported would require PO2 in excess of ~900 to ~10,000 atmospheres. Finally, in the three studies listed, in which the O2 content in commercially available O2-waters was actually measured [4,19,37], its value was found to be much lower than advertised by the manufacturer and similar to or only slightly above the value at equilibrium at sea level (see Box 1). It is also worth mentioning that, in only one of the five brands of O2-waters analyzed by Hampson et al. [2], the PO2 corresponded to an O2 content higher than ~4× the content at equilibrium at sea level. Taken together, results from 10 of the 12 studies available in the literature do not allow us to conclude about putative effects of O2-waters on the response to exercise and on performance, because the O2-content cannot be ascertained, is incredibly high, or is much too low.
As already discussed by several authors [3,4,7], when compared to the VO2 at rest and even more during exercise, the amount of O2 which could be supplied to the blood in the gut by O2-waters is extremely small, and unlikely to directly increase aerobic energy production at rest and even less during exercise. In addition, as observed by Fleming et al. [8], a putative increase in VO2 in peripheral tissues because of an additional supply of O2 from ingested O2-water will not be detected from VO2 measurement at the mouth which only tracks pulmonary gas exchanges. It is, thus, not surprising that, in previous studies [2,7], as well as in the present experiment, for a given workload, the VO2 was similar between the three waters. The only previous significant differences reported were a slightly higher VE/VO2 at submaximal workload and a higher plasma lactate concentration at maximal exercise [7]. However, the differences were low, and the authors questioned their physiological significance. In the present experiment, O2-waters with an O2 content well above the range of values for which manufacturers claim benefits in terms of physiological response and performance did not have any effect on any of the variables measured. Taken together, these data question the interest to use O2-water as an ergogenic aid to improve aerobic performance.
There was, however, a trend for the water enriched in O2 by electrolysis to speed up the kinetic of VO2 in response to high-intensity exercise when compared with the control water. Since the fast component of the kinetics of VO2 reflects O2 diffusion from the blood to muscle fibers [15], this observation is consistent with our previous study showing a lower apparent Km of the mitochondria for O2 in a solution enriched in O2 by electrolysis, without any change in the Km for ADP in rat permeabilized muscle fibers [10]. The faster diffusion of O2 to the mitochondria, as well as the trend to faster adjustment of VO2 at the onset of exercise observed in the present experiment, in turn, is consistent with the hypothesis that the electrolytic process could generate supramolecular water structures, similar to clathrates [12,13,14], which can trap O2 molecules and could modify the local pressure/content relationship for O2.
Finally, it has been suggested that administering O2 internally by ingesting O2-waters, which increases PO2 in the portal vein in rats [38], can be a safety issue because of possible damage to the liver and generation of oxygen radicals [16]. Previous studies showed that acute ingestion of O2-waters (300 mL with O2 content ranging from 30 to ~200 mg·L−1) transiently increased blood ascorbyl radical concentration [5,6]. This effect was attenuated following chronic ingestion (0.9 to 1.5 L·day−1 for 21 to 28 days). Moreover, ingestion of an O2-water for eight days significantly increased serum lipid peroxide concentration and urine alkenyl excretion [17]. However, as already discussed, the actual O2 content in the water ingested in this study cannot be ascertained. In the present experiment, ingestion of O2-water did not result in ROS-induced damage at rest. In addition, the comet assay, which is very sensitive to detect oxidative DNA damages, did not show any genotoxicity of the O2-waters administered. A similar result was reported 30 and 60 min following ingestion of 500 mL of O2-waters with 70 mg O2·L−1 [39]. Taken together, these results suggest that consumption of waters enriched in O2 does not induce oxidative stress at rest in healthy subjects.
5. Conclusions
In response to high-intensity exercise, results from the present study did not show any beneficial effects of water enriched in O2 by injection or electrolysis on exercise time to exhaustion, on the cardiopulmonary response and on arterial lactate concentration and pH.
Author Contributions
Conceptualization and methodology, F.P. and R.R.; investigation, F.N.D., F.P., A.C., E.L., S.D., B.G. and R.R.; formal analysis, F.N.D., F.P., A.C. and R.R.; data curation, F.N.D., F.P., A.C. and R.R.; resources, A.C., E.L., S.D. and B.G.; validation, F.N.D., F.P. and A.C.; visualization, F.N.D., F.P. and A.C.; writing review and editing, F.N.D., F.P., A.C., E.L., S.D., B.G. and R.R.; supervision, F.P., B.G. and R.R.; project administration, R.R.; funding acquisition, F.P. and R.R. All authors have read and agreed to the published version of the manuscript.
Funding
The study was financed by an unrestricted grant from Danone Research (Palaiseau, France).
Institutional Review Board Statement
All procedures were performed by following the Code of Ethics of the World Medical Association (Declaration of Helsinki). The protocol was approved by the local ethic committee (Comité de Protection des Personnes Est IV, Strasbourg, France, Eudract No. 2008-A01051-54 on 14 October 2008).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors thank the University of Lille which paid the publication costs.
Conflicts of Interest
F. Péronnet and R. Richard are occasional consultants for Danone Research. Frédéric N. Daussin, Antoine Charton, Evelyne Lonsdorfer, Stéphane Doutreleau and Bernard Geny do not have any competing interest to declare.
References
- Sander, R. Compilation of Henry’s law constants (version 4.0) for water as solvent. Atmos. Chem. Phys. 2015, 15, 4399–4981. [Google Scholar] [CrossRef]
- Hampson, N.B.; Pollock, N.W.; Piantadosi, C.A. Oxygenated Water and Athletic Performance. JAMA J. Am. Med. Assoc. 2003, 290, 2408–2409. [Google Scholar] [CrossRef]
- Piantadosi, C.A. “Oxygenated” water and athletic performance. Br. J. Sports Med. 2006, 40, 740–741. [Google Scholar] [CrossRef] [PubMed]
- Willmert, N.; Porcari, J.P.; Foster, C.; Doberstein, S.; Brice, G. The effects of oxygenated water on exercise physiology during incremental exercise and recovery. J. Exerc. Physiol. 2002, 5, 16–21. [Google Scholar]
- Gruber, R.; Axmann, S.; Schoenberg, M.H. The influence of oxygenated water on the immune status, liver enzymes, and the generation of oxygen radicals: A prospective, randomised, blinded clinical study. Clin. Nutr. 2005, 24, 407–414. [Google Scholar] [CrossRef]
- Schoenberg, M.H.; Hierl, T.C.; Zhao, J.; Wohlgemuth, N.; Nilsson, U.A. The generation of oxygen radicals after drinking of oxygenated water. Eur. J. Med. Res. 2002, 7, 109–116. [Google Scholar]
- Leibetseder, V.; Strauss-Blasche, G.; Marktl, W.; Ekmekcioglu, C. Does Oxygenated Water Support Aerobic Performance and Lactate Kinetics? Int. J. Sports Med. 2006, 27, 232–235. [Google Scholar] [CrossRef] [PubMed]
- Fleming, N.; Vaughan, J.; Feeback, M. Ingestion of oxygenated water enhances lactate clearance kinetics in trained runners. J. Int. Soc. Sports Nutr. 2017, 14, 9. [Google Scholar] [CrossRef] [PubMed]
- Lascoste, C.; Brunner, S.; Jimenez, L.; Klein, A. Method for Enriching Water with Oxygen by an Electrolytic Process, Oxygen Enriched Water or Beverage and Uses Thereof. U.S. Patent US008709231B2, 29 April 2014. [Google Scholar]
- Zoll, J.; Bouitbir, J.; Sirvent, P.; Klein, A.; Charton, A.; Jimenez, L.; Péronnet, F.R.; Geny, B.; Richard, R. Apparent Km of mitochondria for oxygen computed from Vmax measured in permeabilized muscle fibers is lower in water enriched in oxygen by electrolysis than injection. Drug Des. Dev. Ther. 2015, 9, 3589–3597. [Google Scholar]
- Charton, A.; Péronnet, F.; Doutreleau, S.; Lonsdorfer, E.; Klein, A.; Jimenez, L.; Geny, B.; Diemunsch, P.; Richard, R. Effect of administration of water enriched in O2 by injection or electrolysis on transcutaneous oxygen pressure in anesthetized pigs. Drug Des. Dev. Ther. 2014, 8, 1161–1167. [Google Scholar] [CrossRef][Green Version]
- Chaplin, M.F. A proposal for the structuring of water. Biophys. Chem. 2000, 83, 211–221. [Google Scholar] [CrossRef]
- Ozeki, S.; Otsuka, I. Transient oxygen clathrate-like hydrate and water networks induced by magnetic fields. J. Phys. Chem. B 2006, 110, 20067–20072. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.-F.; Chin, C.-C.; Liu, B.-M.; Chen, Y.-C.; Lin, C.-H.; Chang, K.-D.; Lee, Y.-H. Self-assembly formation of the magic ion of (H2O)20O+: Observation of nanoscale cages of oxygenated water clusters induced from iron nanoparticles. Rapid Commun. Mass Spectrom. RCM 2011, 25, 410–414. [Google Scholar] [CrossRef]
- Wasserman, K. Coupling of external to cellular respiration during exercise: The wisdom of the body revisited. Am. J. Physiol. Endocrinol. Metab. 1994, 266, E519–E539. [Google Scholar] [CrossRef] [PubMed]
- Arnaud, M.J. Letter to the Editor - Does oxygenated water support aerobic performance and lactate kinetics? Int. J. Sports Med. 2006, 27, 759–760. [Google Scholar] [CrossRef]
- Askew, E.W.; Pfeiffer, J.M.; Roberts, D.E.; Reading, J.E.; Ensign, W.Y. Does “activated stabilized oxygen” dissolved in drinking water improve aerobic metabolism at moderate altitude? Wilderness Environ. Med. 2001, 12, 49. [Google Scholar]
- Duncan, J. Fluid Replacement During Exercise: Psychological, Physiologic and Biochemical Benefits of Oxygenated Enhanced Water; Texas Woman’s University. Center for Research on Women’s Health: Denton, TX, USA, 1997. [Google Scholar]
- Fuller, P.J. The Effects of Activated Stabilized Oxygen on Aerobic Endurance in Division II Collegiate Male Soccer Players. Master’s Thesis, Humboldt State University, Arcata, CA, USA, 2010. [Google Scholar]
- Jenkins, A.; Moreland, M.; Waddell, T.B.; Fernhall, B. Effect of oxygenized water on percent oxygen saturation and performance during exercise. Med. Sci. Sports Exerc. 2001, 33, S167. [Google Scholar] [CrossRef]
- McNaughton, L.R.; Kenney, S.; Siegler, J.; Midgley, A.W.; Lovell, R.J.; Bentley, D.J. The effect of superoxygenated water on blood gases, lactate, and aerobic cycling performance. Int. J. Sports Physiol. Perform. 2007, 2, 377–385. [Google Scholar] [CrossRef]
- Mielke, M. Oxygenated Water and Exercise Performance; Florida Atlantic University: Boca Raton, FL, USA, 2004. [Google Scholar]
- Wing-Gaia, S.L.; Subudhi, A.W.; Askew, E.W. Effects of purified oxygenated water on exercise performance during acute hypoxic exposure. Int. J. Sport Nutr. Exerc. Metab. 2005, 15, 680–688. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Chunran, L.; Ling, W. A preliminary study of hyperoxic solution taken orally on fatigue induced by exercise and its mechanism. Med. J. Chin. Peoples Lib. Army 2005, 6. [Google Scholar]
- Whitley, E.; Ball, J. Statistics review 4: Sample size calculations. Crit. Care 2002, 6, 335. [Google Scholar] [CrossRef] [PubMed]
- Jones, N.L.; Summers, E.; Killian, K.J. Influence of age and stature on exercise capacity during incremental cycle ergometry in men and women. Am. Rev. Respir. Dis. 1989, 140, 1373–1380. [Google Scholar] [CrossRef] [PubMed]
- Aguilaniu, B.; Maitre, J.; Diab, S.; Perrault, H.; Péronnet, F. Detection of disturbances in pulmonary gas exchanges during exercise from arterialized earlobe PO2. Respir. Physiol. Neurobiol. 2011, 177, 30–35. [Google Scholar] [CrossRef]
- Barstow, T.J.; Molé, P.A. Linear and nonlinear characteristics of oxygen uptake kinetics during heavy exercise. J. Appl. Physiol. 1991, 71, 2099–2106. [Google Scholar] [CrossRef] [PubMed]
- Whipp, B.J.; Ward, S.A.; Lamarra, N.; Davis, J.A.; Wasserman, K. Parameters of ventilatory and gas exchange dynamics during exercise. J. Appl. Physiol. 1982, 52, 1506–1513. [Google Scholar] [CrossRef] [PubMed]
- Daussin, F.N.; Zoll, J.; Dufour, S.P.; Ponsot, E.; Lonsdorfer-Wolf, E.; Doutreleau, S.; Mettauer, B.; Piquard, F.; Geny, B.; Richard, R. Effect of interval versus continuous training on cardiorespiratory and mitochondrial functions: Relationship to aerobic performance improvements in sedentary subjects. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2008, 295, R264–R272. [Google Scholar] [CrossRef]
- Efron, B.; Tibshirani, R.J. An Introduction to the Bootstrap; CRC Press LLC: Boca Raton, FL, USA, 1994. [Google Scholar]
- Borrani, F.; Candau, R.; Millet, G.Y.; Perrey, S.; Fuchslocher, J.; Rouillon, J.D. Is the VO2 slow component dependent on progressive recruitment of fast-twitch fibers in trained runners? J. Appl. Physiol. 2001, 90, 2212–2220. [Google Scholar] [CrossRef] [PubMed]
- Lamarra, N.; Whipp, B.J.; Ward, S.A.; Wasserman, K. Effect of interbreath fluctuations on characterizing exercise gas exchange kinetics. J. Appl. Physiol. 1987, 62, 2003–2012. [Google Scholar] [CrossRef] [PubMed]
- Richard, M.J.; Portal, B.; Meo, J.; Coudray, C.; Hadjian, A.; Favier, A. Malondialdehyde kit evaluated for determining plasma and lipoprotein fractions that react with thiobarbituric acid. Clin. Chem. 1992, 38, 704–709. [Google Scholar] [CrossRef] [PubMed]
- Akerboom, T.P.M.; Sies, H. Assay of glutathione, glutathione disulfide, and glutathione mixed disulfides in biological samples. Methods Enzymol. 1981, 77, 373–382. [Google Scholar] [PubMed]
- Hininger, I.; Chollat-Namy, A.; Sauvaigo, S.; Osman, M.; Faure, H.; Cadet, J.; Favier, A.; Roussel, A.-M. Assessment of DNA damage by comet assay on frozen total blood: Method and evaluation in smokers and non-smokers. Mutat. Res./Genet. Toxicol. Environ. Mutagenesis 2004, 558, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Mielke, M.; Kroy, J.O.; Torok, D.; Zoeller, R. Oxygenated Water Does Not Improve Endurance Exercise Performance. Med. Sci. Sports Exerc. 2005, 37, S42–S43. [Google Scholar] [CrossRef]
- Gelman, S.I. The effect of enteral oxygen administration on the hepatic circulation during halothane anaesthesia: Experimental investigations. Br. J. Anaesth. 1975, 47, 1253–1259. [Google Scholar] [CrossRef] [PubMed]
- Speit, G.; Schütz, P.; Trenz, K.; Rothfuss, A. Oxygenated water does not induce genotoxic effects in the comet assay. Toxicol. Lett. 2002, 133, 203–210. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).