
Pronounced Trace Element Variation in Follicular Fluids of Subfertile Women Undergoing Assisted Reproduction


 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
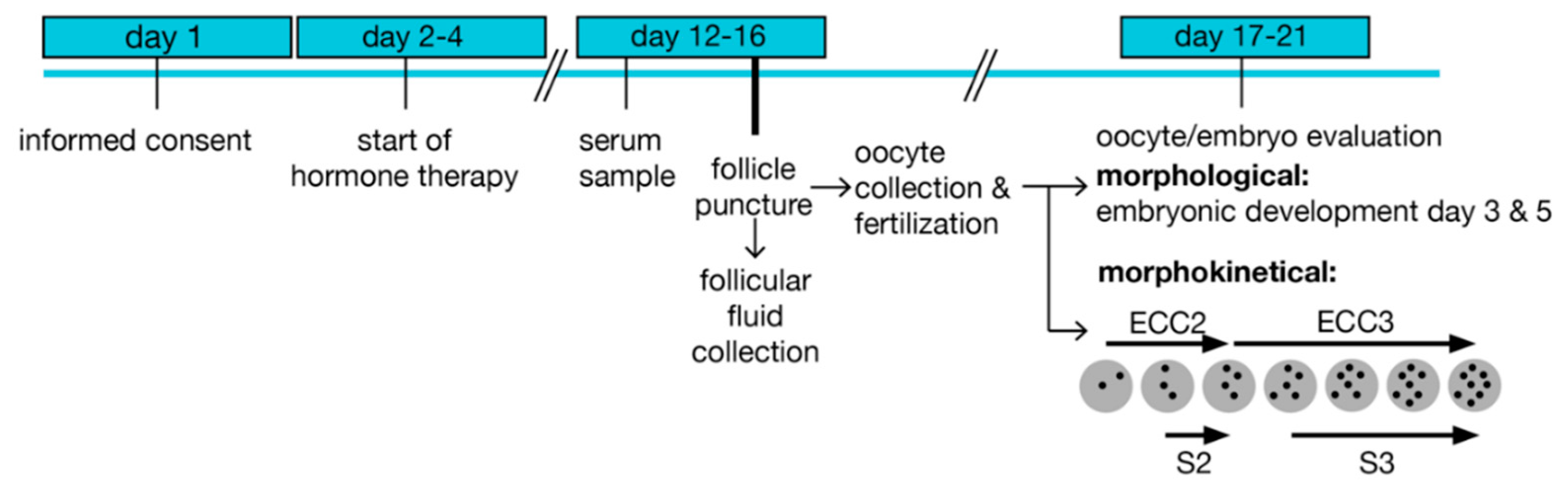
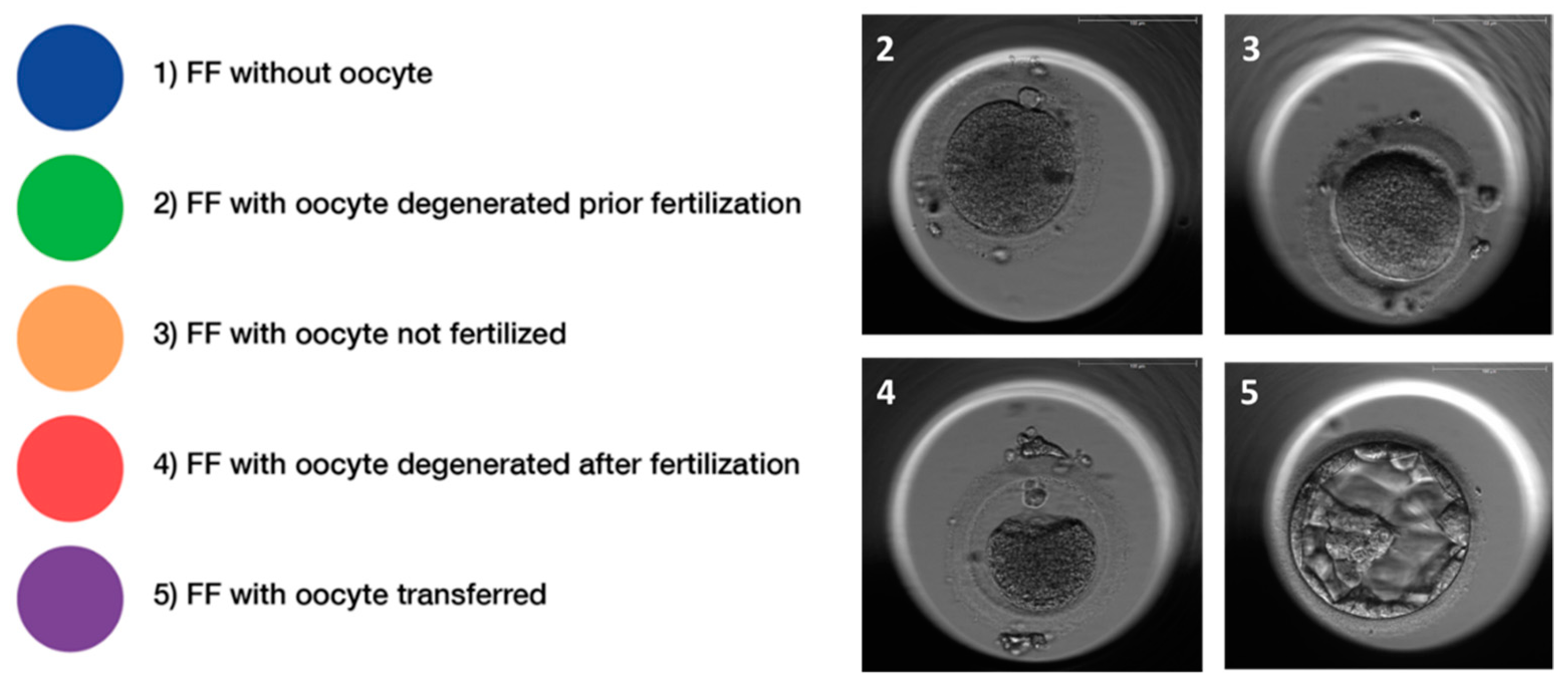
2.2. Sample Preparation and Characterization of Oocytes
2.3. Trace Element (TE) Analysis in Serum and FF Samples
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
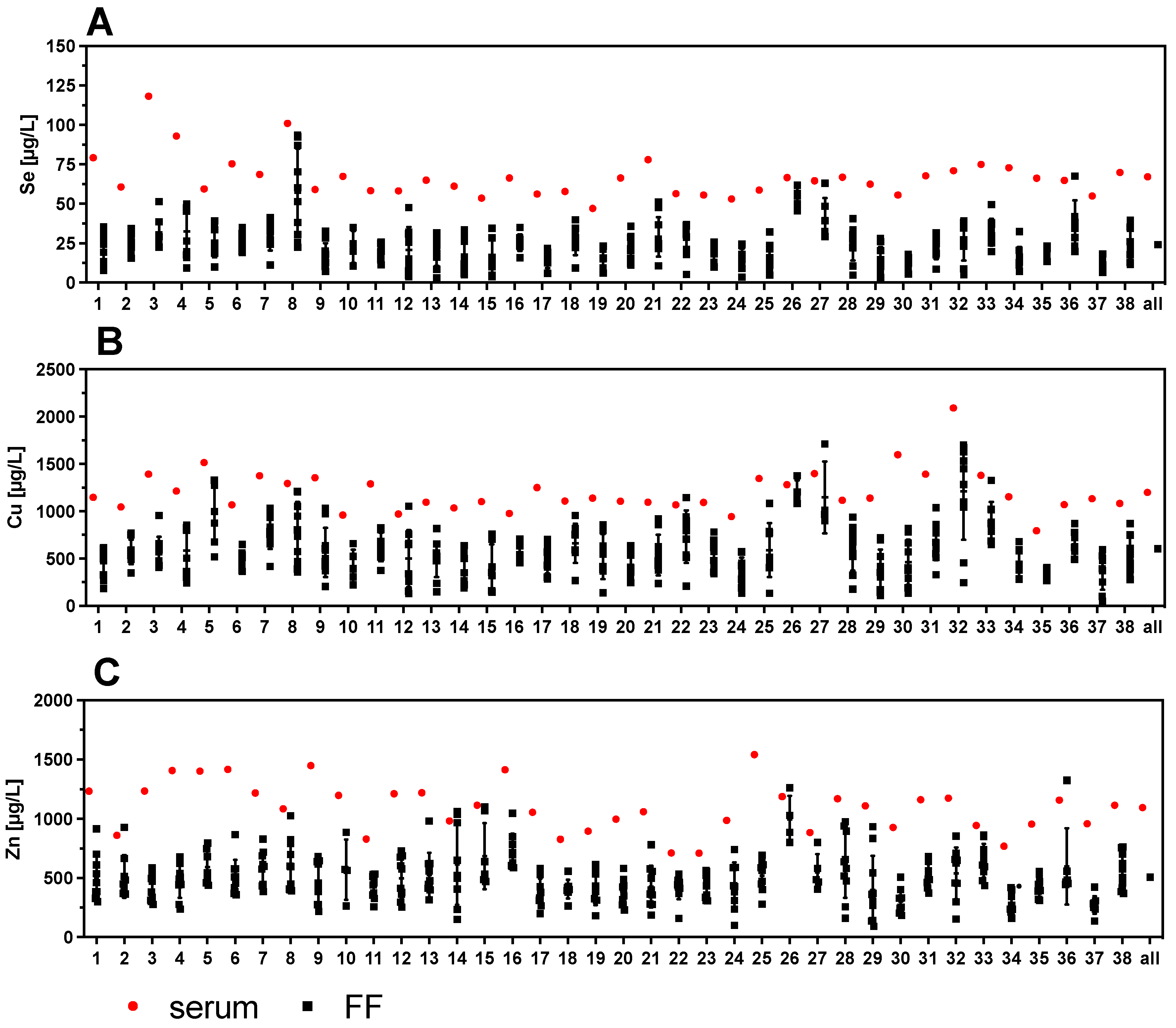
3.2. Trace Element Status in Serum and Follicular Fluids (FF)
3.3. Strong Variability of Trace Element Status in Follicular Fluids versus Corresponding Serum
3.4. Protein Biomarkers of Se Status in Follicular Fluids and Corresponding Serum Samples
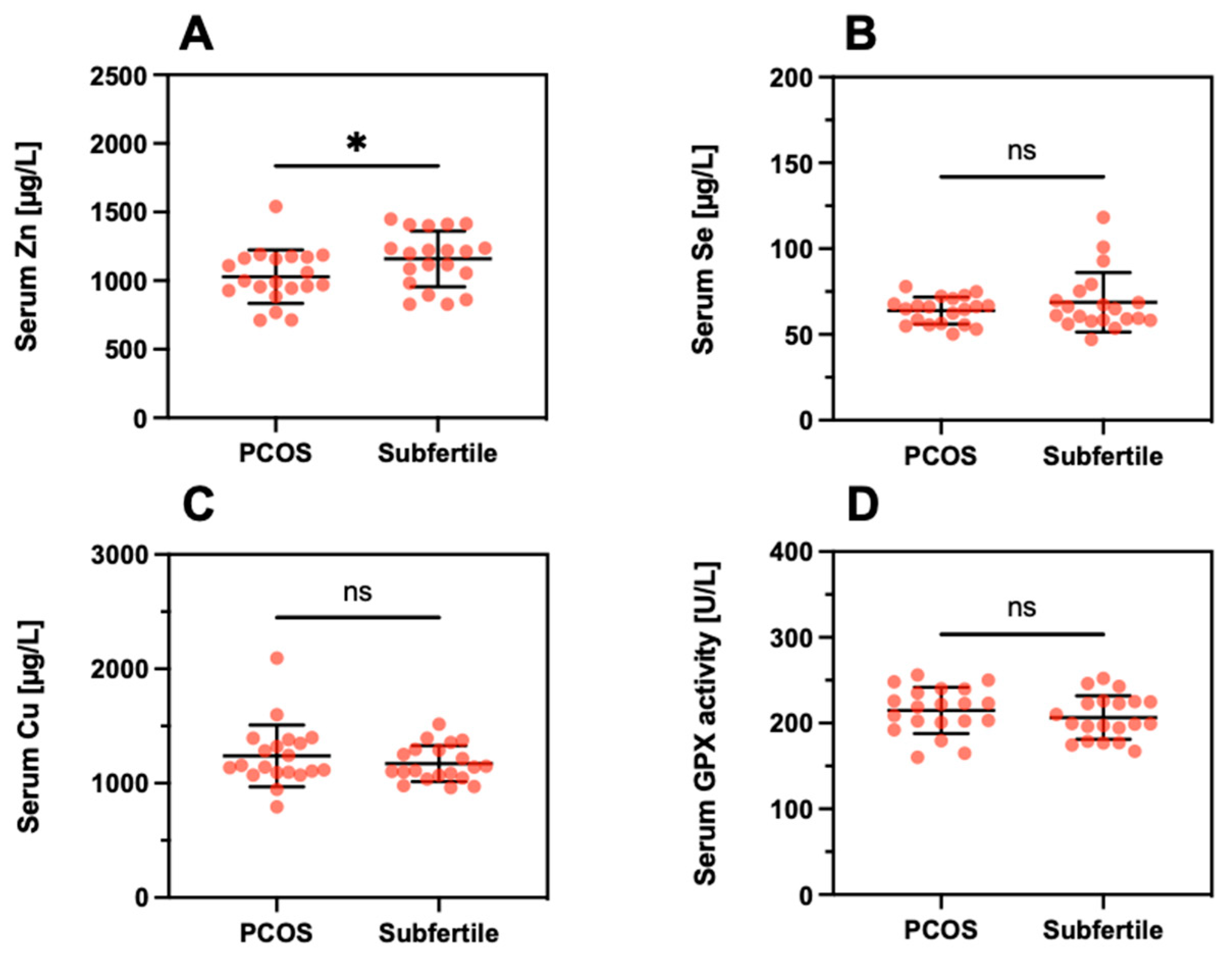
3.5. Trace Element Status in Patients in Relation to a Diagnosis of PCOS
3.6. Trace Element Status in Relation to Morphokinetic Variables
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Boivin, J.; Bunting, L.; Collins, J.A.; Nygren, K.G. International estimates of infertility prevalence and treatment-seeking: Potential need and demand for infertility medical care. Hum. Reprod. 2007, 22, 1506–1512. [Google Scholar] [CrossRef] [Green Version]
- Farquhar, C.M.; Bhattacharya, S.; Repping, S.; Mastenbroek, S.; Kamath, M.S.; Marjoribanks, J.; Boivin, J. Female subfertility. Nat. Rev. Dis. Primers 2019, 5, 7. [Google Scholar] [CrossRef] [PubMed]
- Costello, M.F.; Misso, M.L.; Balen, A.; Boyle, J.; Devoto, L.; Garad, R.M.; Hart, R.; Johnson, L.; Jordan, C.; Legro, R.S.; et al. A brief update on the evidence supporting the treatment of infertility in polycystic ovary syndrome. Aust. N. Z. J. Obstet. Gynaecol. 2019, 59, 867–873. [Google Scholar] [CrossRef]
- Patel, S. Polycystic ovary syndrome (PCOS), an inflammatory, systemic, lifestyle endocrinopathy. J. Steroid Biochem. Mol. Biol. 2018, 182, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Legro, R.S.; Dodson, W.C.; Kunselman, A.R.; Stetter, C.M.; Kris-Etherton, P.M.; Williams, N.I.; Gnatuk, C.L.; Estes, S.J.; Allison, K.C.; Sarwer, D.B.; et al. Benefit of delayed fertility therapy with preconception weight loss over immediate therapy in obese women with PCOS. J. Clin. Endocrinol. Metab. 2016, 101, 2658–2666. [Google Scholar] [CrossRef]
- Drakopoulos, P.; Bardhi, E.; Boudry, L.; Vaiarelli, A.; Makrigiannakis, A.; Esteves, S.C.; Tournaye, H.; Blockeel, C. Update on the management of poor ovarian response in IVF: The shift from Bologna criteria to the Poseidon concept. Adv. Reprod. Health 2020, 14, 1–11. [Google Scholar] [CrossRef]
- Saket, Z.; Källén, K.; Lundin, K.; Magnusson, Å.; Bergh, C. Cumulative live birth rate after IVF: Trend over time and the impact of blastocyst culture and vitrification. Hum. Reprod. Open 2021, 2021, hoab021. [Google Scholar] [CrossRef]
- Yang, R.; Niu, Z.R.; Chen, L.X.; Liu, P.; Li, R.; Qiao, J. Analysis of related factors affecting cumulative live birth rates of the first ovarian hyperstimulation in vitro fertilization or intracytoplasmic sperm injection cycle: A population-based study from 17,978 women in China. Chin. Med. J. 2021, 134, 1405–1415. [Google Scholar] [CrossRef]
- Gardner, D.K.; Balaban, B. Assessment of human embryo development using morphological criteria in an era of time-lapse, algorithms and ‘OMICS’: Is looking good still important? Mol. Hum. Reprod. 2016, 22, 704–718. [Google Scholar] [CrossRef]
- Meseguer, M.; Herrero, J.; Tejera, A.; Hilligsøe, K.M.; Ramsing, N.B.; Remohí, J. The use of morphokinetics as a predictor of embryo implantation. Hum. Reprod. 2011, 26, 2658–2671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, M.H.; Wei, S.Y.; Hu, J.Y.; Yuan, J.; Liu, F.H. Does time-lapse imaging have favorable results for embryo incubation and selection compared with conventional methods in clinical in vitro fertilization? A meta-analysis and systematic review of randomized controlled trials. PLoS ONE 2017, 12, e0178720. [Google Scholar] [CrossRef]
- Zakerkish, F.; Brannstrom, M.; Carlsohn, E.; Sihlbom, C.; van der Post, S.; Thoroddsen, A. Proteomic analysis of follicular fluid during human ovulation. Acta Obstet. Gynecol. Scand. 2020, 99, 917–924. [Google Scholar] [CrossRef] [PubMed]
- Dumesic, D.A.; Meldrum, D.R.; Katz-Jaffe, M.G.; Krisher, R.L.; Schoolcraft, W.B. Oocyte environment: Follicular fluid and cumulus cells are critical for oocyte health. Fertil. Steril. 2015, 103, 303–316. [Google Scholar] [CrossRef] [PubMed]
- Springman, S.A.; Drewnoski, M.E.; Funston, R.N. Effects of hydroxy trace mineral supplementation on gain and reproductive performance in beef heifers. Livest. Sci. 2021, 245, 104425. [Google Scholar] [CrossRef]
- Hostetler, C.E.; Kincaid, R.L.; Mirando, M.A. The role of essential trace elements in embryonic and fetal development in livestock. Vet. J. 2003, 166, 125–139. [Google Scholar] [CrossRef]
- Capone, K.; Sentongo, T. The ABCs of nutrient deficiencies and toxicities. Pediatr. Ann. 2019, 48, e434–e440. [Google Scholar] [CrossRef]
- Mirnamniha, M.; Faroughi, F.; Tahmasbpoura, E.; Ebrahimi, P.; Harchegani, A.B. An overview on role of some trace elements in human reproductive health, sperm function and fertilization process. Rev. Environ. Health 2019, 34, 339–348. [Google Scholar] [CrossRef]
- Buhling, K.J.; Grajecki, D. The effect of micronutrient supplements on female fertility. Curr. Opin. Obstet. Gynecol. 2013, 25, 173–180. [Google Scholar] [CrossRef]
- Roychoudhury, S.; Nath, S.; Massanyi, P.; Stawarz, R.; Kacaniova, M.; Kolesarova, A. Copper-induced changes in reproductive functions: In vivo and in vitro effects. Physiol. Res. 2016, 65, 11–22. [Google Scholar] [CrossRef]
- Mintziori, G.; Mousiolis, A.; Duntas, L.H.; Goulis, D.G. Evidence for a manifold role of selenium in infertility. Horm. Int. J. Endocrinol. 2020, 19, 55–59. [Google Scholar] [CrossRef]
- Mistry, H.D.; Broughton Pipkin, F.; Redman, C.W.; Poston, L. Selenium in reproductive health. Am. J. Obstet. Gynecol. 2012, 206, 21–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allouche-Fitoussi, D.; Breitbart, H. The role of zinc in male fertility. Int. J. Mol. Sci. 2020, 21, 7796. [Google Scholar] [CrossRef] [PubMed]
- Vickram, S.; Rohini, K.; Srinivasan, S.; Nancy Veenakumari, D.; Archana, K.; Anbarasu, K.; Jeyanthi, P.; Thanigaivel, S.; Gulothungan, G.; Rajendiran, N.; et al. Role of Zinc (Zn) in human reproduction: A journey from initial spermatogenesis to childbirth. Int. J. Mol. Sci. 2021, 22, 2188. [Google Scholar] [CrossRef] [PubMed]
- Ursini, F.; Heim, S.; Kiess, M.; Maiorino, M.; Roveri, A.; Wissing, J.; Flohe, L. Dual function of the selenoprotein PHGPx during sperm maturation. Science 1999, 285, 1393–1396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Renko, K.; Werner, M.; Renner-Muller, I.; Cooper, T.G.; Yeung, C.H.; Hollenbach, B.; Scharpf, M.; Kohrle, J.; Schomburg, L.; Schweizer, U. Hepatic selenoprotein P (SePP) expression restores selenium transport and prevents infertility and motor-incoordination in Sepp-knockout mice. Biochem. J. 2008, 409, 741–749. [Google Scholar] [CrossRef] [Green Version]
- Olson, G.E.; Winfrey, V.P.; NagDas, S.K.; Hill, K.E.; Burk, R.F. Apolipoprotein E receptor-2 (ApoER2) mediates selenium uptake from selenoprotein P by the mouse testis. J. Biol. Chem. 2007, 282, 12290–12297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michaelis, M.; Gralla, O.; Behrends, T.; Scharpf, M.; Endermann, T.; Rijntjes, E.; Pietschmann, N.; Hollenbach, B.; Schomburg, L. Selenoprotein P in seminal fluid is a novel biomarker of sperm quality. Biochem. Biophys. Res. Commun. 2014, 443, 905–910. [Google Scholar] [CrossRef] [PubMed]
- Schenk, M.; Huppertz, B.; Obermayer-Pietsch, B.; Kastelic, D.; Hormann-Kropfl, M.; Weiss, G. Biobanking of different body fluids within the frame of IVF-a standard operating procedure to improve reproductive biology research. J. Assist. Reprod. Genet. 2017, 34, 283–290. [Google Scholar] [CrossRef] [Green Version]
- Lerchbaum, E.; Theiler-Schwetz, V.; Kollmann, M.; Wolfler, M.; Pilz, S.; Obermayer-Pietsch, B.; Trummer, C. Effects of vitamin D supplementation on surrogate markers of fertility in pcos women: A randomized controlled trial. Nutrients 2021, 13, 547. [Google Scholar] [CrossRef]
- Azziz, R.; Carmina, E.; Chen, Z.J.; Dunaif, A.; Laven, J.S.E.; Legro, R.S.; Lizneva, D.; Natterson-Horowtiz, B.; Teede, H.J.; Yildiz, B.O. Polycystic ovary syndrome. Nat. Rev. Dis. Primers 2016, 2, 16057. [Google Scholar] [CrossRef]
- Gardner, D.K.; Lane, M.; Stevens, J.; Schlenker, T.; Schoolcraft, W.B. Blastocyst score affects implantation and pregnancy outcome: Towards a single blastocyst transfer. Fertil. Steril. 2019, 112, E81–E84. [Google Scholar] [CrossRef] [PubMed]
- Schenk, M.; Kröpfl, J.M.; Hörmann-Kröpfl, M.; Weiss, G. Endometriosis accelerates synchronization of early embryo cell divisions but does not change morphokinetic dynamics in endometriosis patients. PLoS ONE 2019, 14, e0220529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciray, H.N.; Campbell, A.; Agerholm, I.E.; Aguilar, J.; Chamayou, S.; Esbert, M.; Sayed, S.; Time-Lapse User, G. Proposed guidelines on the nomenclature and annotation of dynamic human embryo monitoring by a time-lapse user group. Hum. Reprod. 2014, 29, 2650–2660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoeflich, J.; Hollenbach, B.; Behrends, T.; Hoeg, A.; Stosnach, H.; Schomburg, L. The choice of biomarkers determines the selenium status in young German vegans and vegetarians. Br. J. Nutr. 2010, 104, 1601–1604. [Google Scholar] [CrossRef]
- Moghaddam, A.; Heller, R.A.; Sun, Q.; Seelig, J.; Cherkezov, A.; Seibert, L.; Hackler, J.; Seemann, P.; Diegmann, J.; Pilz, M.; et al. Selenium deficiency is associated with mortality risk from COVID-19. Nutrients 2020, 12, 2098. [Google Scholar] [CrossRef]
- Flohe, L.; Gunzler, W.A. Assays of glutathione peroxidase. Methods Enzymol. 1984, 105, 114–121. [Google Scholar] [CrossRef]
- Schomburg, L.; Schweizer, U.; Holtmann, B.; Flohe, L.; Sendtner, M.; Kohrle, J. Gene disruption discloses role of selenoprotein P in selenium delivery to target tissues. Biochem. J. 2003, 370, 397–402. [Google Scholar] [CrossRef] [Green Version]
- Hybsier, S.; Schulz, T.; Wu, Z.; Demuth, I.; Minich, W.B.; Renko, K.; Rijntjes, E.; Kohrle, J.; Strasburger, C.J.; Steinhagen-Thiessen, E.; et al. Sex-specific and inter-individual differences in biomarkers of selenium status identified by a calibrated ELISA for selenoprotein P. Redox Biol. 2017, 11, 403–414. [Google Scholar] [CrossRef]
- Combs, G.F., Jr. Biomarkers of selenium status. Nutrients 2015, 7, 2209–2236. [Google Scholar] [CrossRef] [Green Version]
- Schomburg, L. The other view: The trace element selenium as a micronutrient in thyroid disease, diabetes, and beyond. Hormones 2020, 19, 15–24. [Google Scholar] [CrossRef]
- Demircan, K.; Bengtsson, Y.; Sun, Q.; Brange, A.; Vallon-Christersson, J.; Rijntjes, E.; Malmberg, M.; Saal, L.H.; Ryden, L.; Borg, A.; et al. Serum selenium, selenoprotein P and glutathione peroxidase 3 as predictors of mortality and recurrence following breast cancer diagnosis: A multicentre cohort study. Redox Biol. 2021, 47, 102145. [Google Scholar] [CrossRef] [PubMed]
- Nasiadek, M.; Stragierowicz, J.; Klimczak, M.; Kilanowicz, A. The Role of Zinc in Selected Female Reproductive System Disorders. Nutrients 2020, 12, 2464. [Google Scholar] [CrossRef]
- Tolunay, H.E.; Sukur, Y.E.; Ozkavukcu, S.; Seval, M.M.; Ates, C.; Turksoy, V.A.; Ecemis, T.; Atabekoglu, C.S.; Ozmen, B.; Berker, B.; et al. Heavy metal and trace element concentrations in blood and follicular fluid affect ART outcome. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 198, 73–77. [Google Scholar] [CrossRef]
- Wu, S.; Wang, M.; Deng, Y.; Qiu, J.; Zhang, X.; Tan, J. Associations of toxic and essential trace elements in serum, follicular fluid, and seminal plasma with In vitro fertilization outcomes. Ecotoxicol. Environ. Saf. 2020, 204, 110965. [Google Scholar] [CrossRef] [PubMed]
- Paszkowski, T.; Traub, A.I.; Robinson, S.Y.; McMaster, D. Selenium dependent glutathione peroxidase activity in human follicular fluid. Clin. Chim. Acta 1995, 236, 173–180. [Google Scholar] [CrossRef]
- Stoffaneller, R.; Morse, N.L. A review of dietary selenium intake and selenium status in Europe and the Middle East. Nutrients 2015, 7, 1494–1537. [Google Scholar] [CrossRef]
- Hurst, R.; Armah, C.N.; Dainty, J.R.; Hart, D.J.; Teucher, B.; Goldson, A.J.; Broadley, M.R.; Motley, A.K.; Fairweather-Tait, S.J. Establishing optimal selenium status: Results of a randomized, double-blind, placebo-controlled trial. Am. J. Clin. Nutr. 2010, 91, 923–931. [Google Scholar] [CrossRef] [Green Version]
- Xia, Y.; Hill, K.E.; Li, P.; Xu, J.; Zhou, D.; Motley, A.K.; Wang, L.; Byrne, D.W.; Burk, R.F. Optimization of selenoprotein P and other plasma selenium biomarkers for the assessment of the selenium nutritional requirement: A placebo-controlled, double-blind study of selenomethionine supplementation in selenium-deficient Chinese subjects. Am. J. Clin. Nutr. 2010, 92, 525–531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laclaustra, M.; Stranges, S.; Navas-Acien, A.; Ordovas, J.M.; Guallar, E. Serum selenium and serum lipids in US adults: National Health and Nutrition Examination Survey (NHANES) 2003–2004. Atherosclerosis 2010, 210, 643–648. [Google Scholar] [CrossRef] [Green Version]
- Schomburg, L. Selenium Deficiency Due to Diet, Pregnancy, Severe Illness, or COVID-19-A Preventable Trigger for Autoimmune Disease. Int. J. Mol. Sci. 2021, 22, 8532. [Google Scholar] [CrossRef]
- Butts, C.D.; Bloom, M.S.; McGough, A.; Lenhart, N.; Wong, R.; Mok-Lin, E.; Parsons, P.J.; Galusha, A.L.; Yucel, R.M.; Feingold, B.J.; et al. Variability of essential and non-essential trace elements in the follicular fluid of women undergoing in vitro fertilization (IVF). Ecotoxicol. Environ. Saf. 2021, 209, 111733. [Google Scholar] [CrossRef]
- Silberstein, T.; Saphier, O.; Paz-Tal, O.; Gonzalez, L.; Keefe, D.L.; Trimarchi, J.R. Trace element concentrations in follicular fluid of small follicles differ from those in blood serum, and may represent long-term exposure. Fertil. Steril. 2009, 91, 1771–1774. [Google Scholar] [CrossRef]
- Sun, Y.; Wang, W.; Guo, Y.; Zheng, B.; Li, H.; Chen, J.; Zhang, W. High copper levels in follicular fluid affect follicle development in polycystic ovary syndrome patients: Population-based and in vitro studies. Toxicol. Appl. Pharmacol. 2019, 365, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Shoukir, Y.; Campana, A.; Farley, T.; Sakkas, D. Early cleavage of in-vitro fertilized human embryos to the 2-cell stage: A novel indicator of embryo quality and viability. Hum. Reprod. 1997, 12, 1531–1536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lundin, K.; Bergh, C.; Hardarson, T. Early embryo cleavage is a strong indicator of embryo quality in human IVF. Hum. Reprod. 2001, 16, 2652–2657. [Google Scholar] [CrossRef]
- Ciray, H.N.; Karagenç, L.; Ulug, U.; Bener, F.; Bahçeci, M. Early cleavage morphology affects the quality and implantation potential of day 3 embryos. Fertil. Steril. 2006, 85, 358–365. [Google Scholar] [CrossRef]
- Lemmen, J.G.; Agerholm, I.; Ziebe, S. Kinetic markers of human embryo quality using time-lapse recordings of IVF/ICSI-fertilized oocytes. Reprod. Biomed. Online 2008, 17, 385–391. [Google Scholar] [CrossRef]
- Mio, Y.; Maeda, K. Time-lapse cinematography of dynamic changes occurring during in vitro development of human embryos. Am. J. Obstet. Gynecol. 2008, 199, 660.e1–660.e5. [Google Scholar] [CrossRef]
- Desai, N.; Ploskonka, S.; Goodman, L.R.; Austin, C.; Goldberg, J.; Falcone, T. Analysis of embryo morphokinetics, multinucleation and cleavage anomalies using continuous time-lapse monitoring in blastocyst transfer cycles. Reprod. Biol. Endocrinol. 2014, 12, 54. [Google Scholar] [CrossRef]
- Wissing, M.L.; Bjerge, M.R.; Olesen, A.I.; Hoest, T.; Mikkelsen, A.L. Impact of PCOS on early embryo cleavage kinetics. Reprod. Biomed. Online 2014, 28, 508–514. [Google Scholar] [CrossRef] [Green Version]
- Garner, T.B.; Hester, J.M.; Carothers, A.; Diaz, F.J. Role of zinc in female reproduction. Biol. Reprod. 2021, 104, 976–994. [Google Scholar] [CrossRef] [PubMed]
- Grieger, J.A.; Grzeskowiak, L.E.; Wilson, R.L.; Bianco-Miotto, T.; Leemaqz, S.Y.; Jankovic-Karasoulos, T.; Perkins, A.V.; Norman, R.J.; Dekker, G.A.; Roberts, C.T. Maternal selenium, copper and zinc concentrations in early pregnancy, and the association with fertility. Nutrients 2019, 11, 1609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torshizi, F.F.; Chamani, M.; Khodaei, H.R.; Sadeghi, A.A.; Hejazi, S.H.; Heravi, R.M. The effects of zinc methionine on reproductive and thyroid hormones in rats with polycystic ovarian syndrome. Adv. Biomed. Res. India 2020, 9, 57. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subfertile | PCOS | ||||
|---|---|---|---|---|---|
| Parameter | Mean ± SD | n | Mean ± SD | n | p-Value * |
| Age (year) | 35 ± 3 | 20 | 29 ± 4 | 20 | <0.0001 |
| BMI (kg/m2) | 22 ± 3 | 20 | 23 ± 3 | 20 | n.s. |
| Smoker/non-smoker | - | 2/18 | - | 4/16 | |
| Hormonal status | |||||
| FSH (mIU/mL) | 6.4 ± 1.6 | 19 | 6.6 ± 2.0 | 19 | n.s. |
| AMH (ng/mL) | 3.5 ± 2.2 | 19 | 8.2 ± 4.6 | 17 | 0.0004 |
| E2 (pg/mL) | 38.0 ± 15.1 | 19 | 38.3 ± 15.5 | 19 | n.s. |
| Newborn height and weight | |||||
| Newborn height (cm) | 48 ± 4 | 7 | 50 ± 5 | 5 | n.s. |
| Newborn weight (g) | 2994 ± 863 | 7 | 3001 ± 809 | 5 | n.s. |
| ICSI/IVF/missing data | 19/1/0 | 15/3/2 | |||
| Subfertile | PCOS | |||||
|---|---|---|---|---|---|---|
| Group | Mean ± SD | n | Mean ± SD | n | p-Value | |
| 1 | Se (µg/L) | 23 ± 10 | 17 | 19 ± 11 | 13 | n.s. |
| Cu (µg/L) | 555 ± 191 | 17 | 518 ± 267 | 13 | n.s. | |
| Zn (µg/L) | 474 ± 118 | 17 | 402 ± 164 | 13 | n.s. | |
| GPX3 (U/L) | 96 ± 33 | 17 | 96 ± 49 | 13 | n.s. | |
| 2 | Se (µg/L) | 31 ± 26 | 8 | 24 ± 11 | 10 | n.s. |
| Cu (µg/L) | 683 ± 289 | 8 | 682 ± 381 | 10 | n.s. | |
| Zn (µg/L) | 569 ± 144 | 8 | 572 ± 231 | 10 | n.s. | |
| GPX3 (U/L) | 103 ± 25 | 8 | 102 ± 42 | 10 | n.s. | |
| 3 | Se (µg/L) | 24 ± 14 | 10 | 22 ± 5 | 5 | n.s. |
| Cu (µg/L) | 516 ± 185 | 10 | 479 ± 179 | 5 | n.s. | |
| Zn (µg/L) | 571 ± 111 | 10 | 419 ± 142 | 5 | 0.039 | |
| GPX3 (U/L) | 86 ± 35 | 10 | 75 ± 12 | 5 | n.s. | |
| 4 | Se (µg/L) | 26 ± 11 | 16 | 24 ± 11 | 17 | n.s. |
| Cu (µg/L) | 619 ± 176 | 16 | 652 ± 276 | 17 | n.s. | |
| Zn (µg/L) | 536 ± 170 | 16 | 467 ± 174 | 17 | n.s. | |
| GPX3 (U/L) | 111 ± 36 | 16 | 103 ± 40 | 17 | n.s. | |
| 5 | Se (µg/L) | 22 ± 11 | 13 | 27 ± 12 | 15 | n.s. |
| Cu (µg/L) | 507 ± 190 | 13 | 742 ± 318 | 15 | 0.028 | |
| Zn (µg/L) | 503 ± 167 | 13 | 591 ± 220 | 15 | n.s. | |
| GPX3 (U/L) | 97 ± 38 | 13 | 105 ± 38 | 15 | n.s. | |
| Δ (2–1) | Se (µg/L) | 9 ± 17 | 8 | 7 ± 9 | 6 | n.s. |
| Cu (µg/L) | 179 ± 283 | 8 | 236 ± 389 | 6 | n.s. | |
| Zn (µg/L) | 138 ± 120 | 8 | 270 ± 285 | 6 | n.s. | |
| GPX3 (U/L) | 21 ± 45 | 7 | 8 ± 25 | 5 | n.s. | |
| Δ (3–1) | Se (µg/L) | 2 ± 11 | 8 | 3 ± 7 | 4 | n.s. |
| Cu (µg/L) | 75 ± 189 | 8 | 28 ± 152 | 4 | n.s. | |
| Zn (µg/L) | 128 ± 167 | 8 | 31 ± 205 | 4 | n.s. | |
| GPX3 (U/L) | 0 ± 42 | 8 | −22 ± 13 | 3 | n.s. | |
| Δ (4–1) | Se (µg/L) | 2 ± 9 | 13 | 4 ± 9 | 13 | n.s. |
| Cu (µg/L) | 46 ± 190 | 13 | 132 ± 223 | 13 | n.s. | |
| Zn (µg/L) | 83 ± 161 | 13 | 49 ± 143 | 13 | n.s. | |
| GPX3 (U/L) | 9 ± 39 | 12 | 3 ± 26 | 11 | n.s. | |
| Δ (5–1) | Se (µg/L) | 1 ± 8 | 10 | 9 ± 12 | 11 | n.s. |
| Cu (µg/L) | 27 ± 141 | 10 | 274 ± 277 | 11 | 0.02 | |
| Zn (µg/L) | −28 ± 169 | 10 | 164 ± 215 | 11 | 0.036 | |
| GPX3 (U/L) | 3 ± 31 | 9 | 10 ± 42 | 9 | n.s. | |
| Group 4 | Group 5 | ||||
|---|---|---|---|---|---|
| Parameter | Mean ± SD | n | Mean ± SD | n | p-Value |
| ECC2 (h) | 13.6 ± 6.0 | 19 | 12.6 ± 1.5 | 19 | n.s. |
| ECC3 (h) | 22.7 ± 7.3 | 15 | 19.1 ± 3.5 | 15 | n.s. |
| S2 (h) | 5.2 ± 5.8 | 20 | 1.8 ± 2.6 | 20 | 0.023 |
| S3 (h) | 15.7 ± 9.1 | 15 | 8.7 ± 4.8 | 15 | 0.017 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schmalbrock, L.J.; Weiss, G.; Rijntjes, E.; Reinschissler, N.; Sun, Q.; Schenk, M.; Schomburg, L. Pronounced Trace Element Variation in Follicular Fluids of Subfertile Women Undergoing Assisted Reproduction. Nutrients 2021, 13, 4134. https://doi.org/10.3390/nu13114134
Schmalbrock LJ, Weiss G, Rijntjes E, Reinschissler N, Sun Q, Schenk M, Schomburg L. Pronounced Trace Element Variation in Follicular Fluids of Subfertile Women Undergoing Assisted Reproduction. Nutrients. 2021; 13(11):4134. https://doi.org/10.3390/nu13114134
Chicago/Turabian StyleSchmalbrock, Lilly Johanna, Gregor Weiss, Eddy Rijntjes, Nina Reinschissler, Qian Sun, Michael Schenk, and Lutz Schomburg. 2021. "Pronounced Trace Element Variation in Follicular Fluids of Subfertile Women Undergoing Assisted Reproduction" Nutrients 13, no. 11: 4134. https://doi.org/10.3390/nu13114134
APA StyleSchmalbrock, L. J., Weiss, G., Rijntjes, E., Reinschissler, N., Sun, Q., Schenk, M., & Schomburg, L. (2021). Pronounced Trace Element Variation in Follicular Fluids of Subfertile Women Undergoing Assisted Reproduction. Nutrients, 13(11), 4134. https://doi.org/10.3390/nu13114134