
Inflammation in Relation to Sarcopenia and Sarcopenic Obesity among Older Adults Living with Chronic Comorbidities: Results from the National Health and Nutrition Examination Survey 1999–2006

 , , ,
, , , 


Abstract
:1. Introduction
2. Methods
2.1. Data Source and Study Population
2.2. Inflammatory Biomarkers
2.3. Sarcopenia and Sarcopenic Obesity
2.4. Covariates
2.5. Statistical Analyses
3. Results
3.1. Characteristics of Participants
3.2. Association of Sarcopenia with Inflammatory Biomarkers
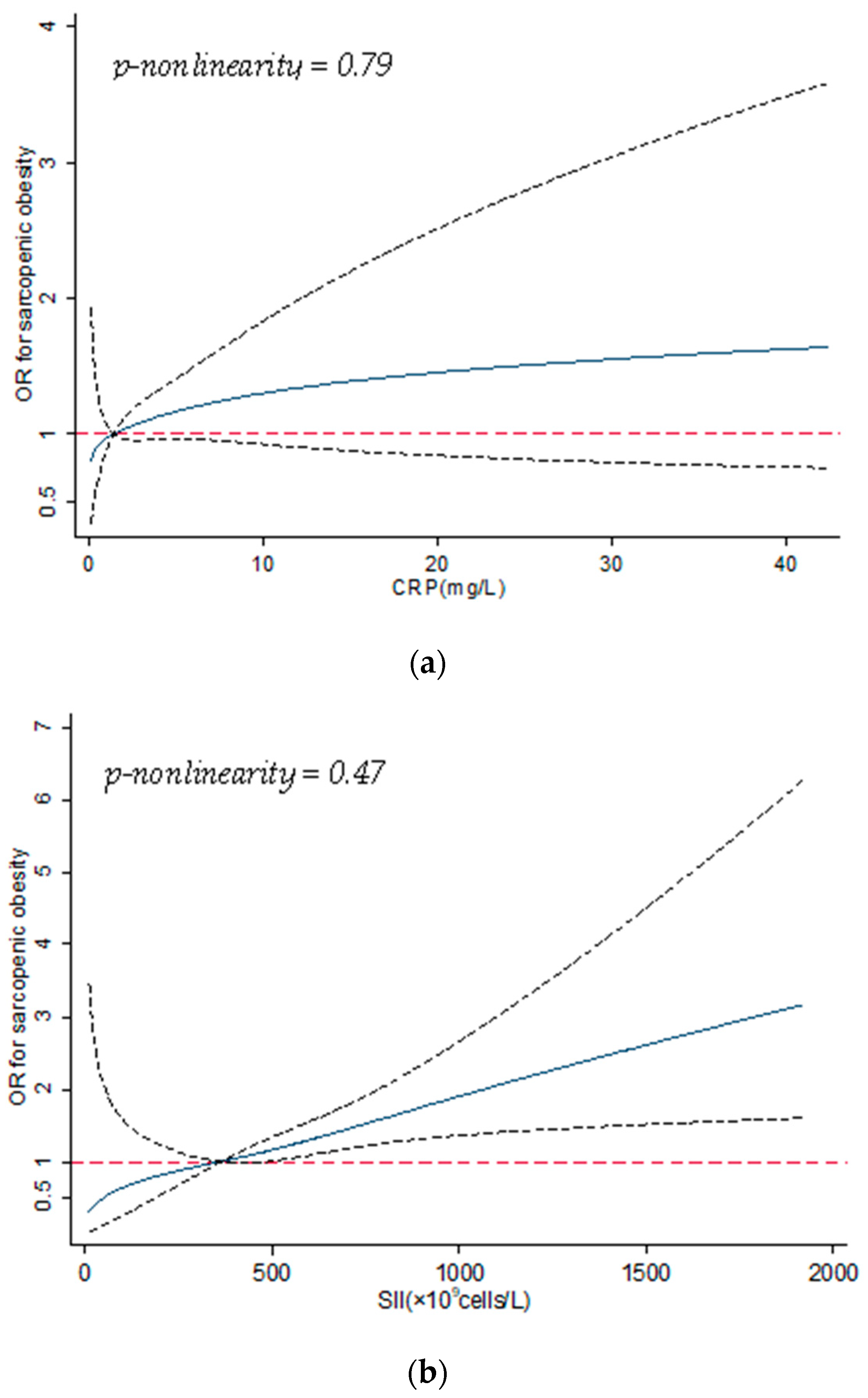
3.3. Association of Sarcopenic Obesity with Inflammatory Biomarkers
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Melton, L.J., 3rd; Khosla, S.; Crowson, C.S.; O’Connor, M.K.; O’Fallon, W.M.; Riggs, B.L. Epidemiology of sarcopenia. J Am. Geriatr. Soc. 2000, 48, 625–630. [Google Scholar] [PubMed]
- Choi, K.M. Sarcopenia and sarcopenic obesity. Korean J. Intern. Med. 2016, 31, 1054–1060. [Google Scholar] [PubMed] [Green Version]
- Wilkinson, D.; Piasecki, M.; Atherton, P.J. The age-related loss of skeletal muscle mass and function: Measurement and physiology of muscle fibre atrophy and muscle fibre loss in humans. Ageing Res. Rev. 2018, 47, 123–132. [Google Scholar] [CrossRef]
- Janssen, I.; Shepard, D.S.; Katzmarzyk, P.T.; Roubenoff, R. The Healthcare Costs of Sarcopenia in the United States. J. Am. Geriatr. Soc. 2003, 52, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E.; Anker, S.D.; Von Haehling, S. Prevalence, incidence, and clinical impact of sarcopenia: Facts, numbers, and epidemiology—Update 2014. J. Cachex Sarcopenia Muscle 2014, 5, 253–259. [Google Scholar] [CrossRef]
- Muscaritoli, M.; Anker, S.D.; Argilés, J.; Aversa, Z.; Bauer, J.M.; Biolo, G.; Boirief, Y.; Bosaeus, I.; Cederholm, T.; Costelli, P.; et al. Consensus definition of sarcopenia, cachexia and pre-cachexia: Joint document elaborated by Special Interest Groups (SIG) “cachex-ia-anorexia in chronic wasting diseases” and “nutrition in geriatrics”. Clin. Nutr. 2010, 29, 154–159. [Google Scholar] [CrossRef]
- Batsis, J.A.; Mackenzie, T.A.; Jones, J.D.; Lopez-Jimenez, F.; Bartels, S.J. Sarcopenia, sarcopenic obesity and inflammation: Results from the 1999–2004 National Health and Nutrition Examination Survey. Clin. Nutr. 2016, 35, 1472–1483. [Google Scholar] [CrossRef]
- Zhang, X.-M.; Chen, D.; Xie, X.-H.; Zhang, J.-E.; Zeng, Y.; Cheng, A.S.K. Sarcopenia as a predictor of mortality among the critically ill in an intensive care unit: A systematic review and meta-analysis. BMC Geriatr. 2021, 21, 339. [Google Scholar] [CrossRef]
- Abramowitz, M.K.; Hall, C.B.; Amodu, A.; Sharma, D.; Androga, L.; Hawkins, M. Muscle mass, BMI, and mortality among adults in the United States: A population-based cohort study. PLoS ONE 2018, 13, e0194697. [Google Scholar]
- Du, K.; Goates, S.; Arensberg, M.B.; Pereira, S.; Gaillard, T. Prevalence of Sarcopenia and Sarcopenic Obesity Vary with Race/Ethnicity and Advancing Age. Divers. Equal. Health Care 2018, 15, 175–183. [Google Scholar] [CrossRef]
- Pacifico, J.; Geerlings, M.A.J.; Reijnierse, E.M.; Phassouliotis, C.; Lim, W.K.; Maier, A.B. Prevalence of sarcopenia as a comorbid disease: A systematic review and meta-analysis. Exp. Gerontol. 2020, 131, 110801. [Google Scholar] [CrossRef] [PubMed]
- Majno, G.; Joris, I. Cells, Tissues and Disease; Oxford University Press: New York, NY, USA; Oxford, UK, 2004. [Google Scholar]
- Kumar, V.; Cotran, R.S.; Robbins, S.L. Robbins Basic Pathology; Saunders: Philadelphia, PA, USA, 2003. [Google Scholar]
- Dalle, S.; Rossmeislova, L.; Koppo, K. The Role of Inflammation in Age-Related Sarcopenia. Front. Physiol. 2017, 8, 1045. [Google Scholar] [CrossRef] [Green Version]
- Ferrucci, L.; Fabbri, E. Inflammageing: Chronic inflammation in ageing, cardiovascular disease, and frailty. Nat. Rev. Cardiol. 2018, 15, 505–522. [Google Scholar] [CrossRef] [PubMed]
- Ishihara, H.; Kondo, T.; Omae, K.; Takagi, T.; Iizuka, J.; Kobayashi, H.; Tanabe, K. Sarcopenia and the Modified Glasgow Prognostic Score are Significant Predictors of Survival among Patients with Metastatic Renal Cell Carcinoma Who are Receiving First-Line Sunitinib Treatment. Target. Oncol. 2016, 11, 605–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujikawa, H.; Araki, T.; Okita, Y.; Kondo, S.; Kawamura, M.; Hiro, J.; Toiyama, Y.; Kobayashi, M.; Tanaka, K.; Inoue, Y.; et al. Impact of sarcopenia on surgical site infection after restorative proctocolectomy for ulcerative colitis. Surg. Today 2017, 47, 92–98. [Google Scholar] [CrossRef]
- El Maghraoui, A.; Ebo’o, F.B.; Sadni, S.; Majjad, A.; Hamza, T.; Mounach, A. Is there a relation between pre-sarcopenia, sarcopenia, cachexia and osteoporosis in patients with ankylosing spondylitis? BMC Musculoskelet. Disord. 2016, 17, 268. [Google Scholar]
- Kim, T.N.; Park, M.S.; Lim, K.I.; Choi, H.Y.; Yang, S.J.; Yoo, H.J.; Kang, H.J.; Song, W.; Choi, H.; Baik, S.H.; et al. Relationships between sarcopenic obesity and insulin resistance, inflammation, and vitamin D status: The Korean Sarcopenic Obesity Study. Clin. Endocrinol. 2013, 78, 525–532. [Google Scholar] [CrossRef]
- Kim, T.N.; Won, J.C.; Kim, Y.J.; Lee, E.J.; Kim, M.-K.; Park, M.S.; Lee, S.K.; Kim, J.M.; Ko, K.S.; Rhee, B.D. Serum adipocyte fatty acid-binding protein levels are independently associated with sarcopenic obesity. Diabetes Res. Clin. Pract. 2013, 101, 210–217. [Google Scholar] [CrossRef]
- Abete, I.; Konieczna, J.; Zulet, M.A.; Galmés-Panades, A.M.; Ibero-Baraibar, I.; Babio, N.; Estruch, R.; Vidal, J.; Toledo, E.; Razquin, C.; et al. Association of lifestyle factors and inflammation with sarcopenic obesity: Data from the PREDIMED-Plus trial. J. Cachexia Sarcopenia Muscle 2019, 10, 974–984. [Google Scholar] [CrossRef] [Green Version]
- Pepys, M.B.; Hirschfield, G.M. C-reactive protein: A critical update. J. Clin. Investig. 2003, 111, 1805–1812. [Google Scholar] [CrossRef]
- Yang, Y.; Wu, C.; Hsu, P.; Chen, S.; Huang, S.; Chan, W.L.; Lin, S.; Chou, C.; Chen, J.; Pan, J.; et al. Systemic immune-inflammation index (SII) predicted clinical outcome in patients with coronary artery disease. Eur. J. Clin. Investig. 2020, 50, e13230. [Google Scholar] [CrossRef]
- Yan, Q.; Ertao, Z.; Zhimei, Z.; Weigang, D.; Jianjun, P.; Jianhui, C.; Chuangqi, C. Systemic immune-inflammation index (SII): A More Promising Inflammation-Based Prognostic Marker for Patients with synchronic colorectal peritoneal carcinomatosis. J. Cancer 2020, 11, 5264–5272. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Yang, X.-R.; Xu, Y.; Sun, Y.-F.; Sun, C.; Guo, W.; Zhang, X.; Wang, W.-M.; Qiu, S.-J.; Zhou, J.; et al. Systemic Immune-Inflammation Index Predicts Prognosis of Patients after Curative Resection for Hepatocellular Carcinoma. Clin. Cancer Res. 2014, 20, 6212–6222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, T.L.; Wilson, K.E.; Heymsfield, S.B. Dual Energy X-Ray Absorptiometry Body Composition Reference Values from NHANES. PLoS ONE 2009, 4, e7038. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.-S.; Lee, Y.; Chung, Y.-S.; Lee, D.-J.; Joo, N.-S.; Hong, D.; Song, G.E.; Kim, H.-J.; Choi, Y.J.; Kim, K.-M. Prevalence of Sarcopenia and Sarcopenic Obesity in the Korean Population Based on the Fourth Korean National Health and Nutritional Examination Surveys. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2012, 67, 1107–1113. [Google Scholar] [CrossRef]
- Woolcott, O.O.; Bergman, R.N. Defining cutoffs to diagnose obesity using the relative fat mass (RFM): Association with mortality in NHANES 1999–2014. Int. J. Obes. 2020, 44, 1301–1310. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.-P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [Green Version]
- Woolcott, O.O.; Bergman, R.N. Relative fat mass (RFM) as a new estimator of whole-body fat percentage—A cross-sectional study in American adult individuals. Sci. Rep. 2018, 8, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Nykänen, T.; Pihlainen, K.; Santtila, M.; Vasankari, T.; Fogelholm, M.; Kyröläinen, H. Diet Macronutrient Composition, Physical Activity, and Body Composition in Soldiers During 6 Months Deployment. Mil. Med. 2018, 184, e231–e237. [Google Scholar] [CrossRef] [Green Version]
- Geng, J.; Deng, L.; Qiu, S.; Bian, H.; Cai, B.; Jin, K.; Zheng, X.; Li, J.; Liao, X.; Li, Y.; et al. Dietary inflammatory potential and risk of sarcopenia: Data from national health and nutrition examination surveys. Aging 2021, 13, 1913–1928. [Google Scholar] [CrossRef]
- Woolcott, O.O.; Bergman, R.N. Relative Fat Mass as an estimator of whole-body fat percentage among children and adolescents: A cross-sectional study using NHANES. Sci. Rep. 2019, 9, 15279. [Google Scholar] [CrossRef] [Green Version]
- Farmer, H.R.; Wray, L.A.; Haas, S.A. Race, Gender, and Socioeconomic Variations in C-Reactive Protein Using the Health and Retirement Study. J. Gerontol. Ser. B 2021, 76, 583–595. [Google Scholar] [CrossRef]
- Lim, J.P.; Leung, B.P.; Ding, Y.Y.; Tay, L.; Ismail, N.H.; Yeo, A.; Yew, S. Monocyte chemoattractant protein-1: A proinflammatory cytokine elevated in sarcopenic obesity. Clin. Interv. Aging 2015, 10, 605–609. [Google Scholar] [CrossRef] [Green Version]
- Zhao, W.Y.; Zhang, Y.; Hou, L.S.; Xia, X.; Ge, M.L.; Liu, X.L.; Yue, J.; Dong, B. The association between systemic inflam-matory markers and sarcopenia: Results from the West China Health and Aging Trend Study (WCHAT). Arch. Gerontol. Geriatr. 2021, 92, 104262. [Google Scholar]
- Schaap, L.A.; Pluijm, S.M.; Deeg, D.J.; Visser, M. Inflammatory Markers and Loss of Muscle Mass (Sarcopenia) and Strength. Am. J. Med. 2006, 119, 526.e9–526.e17. [Google Scholar] [CrossRef]
- Bano, G.; Trevisan, C.; Carraro, S.; Solmi, M.; Luchini, C.; Stubbs, B.; Manzato, E.; Sergi, G.; Veronese, N. Inflammation and sarcopenia: A systematic review and meta-analysis. Maturitas 2017, 96, 10–15. [Google Scholar] [CrossRef]
- Yang, C.W.; Li, C.I.; Li, T.C.; Liu, C.S.; Lin, C.H.; Lin, W.Y.; Lin, C.-C. Association of Sarcopenic Obesity with Higher Serum High-Sensitivity C-Reactive Protein Levels in Chinese Older Males—A Community-Based Study (Taichung Community Health Study-Elderly, TCHS-E). PLoS ONE 2015, 10, e0132908. [Google Scholar]
- Chung, H.Y.; Cesari, M.; Anton, S.; Marzetti, E.; Giovannini, S.; Seo, A.Y.; Carter, C.; Yu, B.P.; Leeuwenburg, C. Molecular inflammation: Un-derpinnings of aging and age-related diseases. Ageing Res. Rev. 2009, 8, 18–30. [Google Scholar] [CrossRef] [Green Version]
- Phillips, T.; Leeuwenburgh, C. Muscle fiber specific apoptosis and TNF-alpha signaling in sarcopenia are attenuated by life-long calorie restriction. FASEB J. 2005, 19, 668–670. [Google Scholar]
- Fry, C.S.; Rasmussen, B.B. Skeletal muscle protein balance and metabolism in the elderly. Curr. Aging Sci. 2011, 4, 260–268. [Google Scholar] [CrossRef] [Green Version]
- Schrager, M.A.; Metter, E.J.; Simonsick, E.; Ble, A.; Bandinelli, S.; Lauretani, F.; Ferrucci, L. Sarcopenic obesity and inflammation in the InCHIANTI study. J. Appl. Physiol. 2007, 102, 919–925. [Google Scholar] [CrossRef]
- Petermann-Rocha, F.; Yang, S.; Gray, S.R.; Pell, J.P.; Celis-Morales, C.; Ho, F.K. Sarcopenic obesity and its as-sociation with respiratory disease incidence and mortality. Clin. Nutr. 2020, 39, 3461–3466. [Google Scholar]
- Chen, F.; Xu, S.; Wang, Y.; Chen, F.; Cao, L.; Liu, T.; Huang, T.; Wei, Q.; Ma, G.; Zhao, Y.; et al. Risk Factors for Sarcopenia in the Elderly with Type 2 Diabetes Mellitus and the Effect of Metformin. J. Diabetes Res. 2020, 2020, 3950404. [Google Scholar] [CrossRef]
- Bagheri, A.; Soltani, S.; Hashemi, R.; Heshmat, R.; Motlagh, A.D.; Esmaillzadeh, A. Inflammatory potential of the diet and risk of sarcopenia and its components. Nutr. J. 2020, 19, 1–8. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variables | Overall | CRP (mg/L) | p-Value | SII (×109 cells/L) | p-Value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n (%) | 2483 (100) | <1.2 | 1.2–2.5 | 2.6–5.2 | ≥5.3 | <365.7 | 365.7–503.6 | 503.7–704.0 | ≥704.1 | ||
| 599 (24.1) | 636 (25.6) | 619 (24.9) | 629 (25.4) | 620 (25.0) | 623 (25.1) | 619 (24.9) | 621 (25.0) | ||||
| Age (years) | |||||||||||
| 60–69 | 1319 (53.1) | 319 (53.3) | 315 (49.5) | 324 (52.3) | 361 (57.4) | 0.19 | 357 (57.6) | 366 (58.8) | 293 (47.4) | 303 (48.8) | <0.01 |
| 70–79 | 756 (30.5) | 183 (30.5) | 204 (32.1) | 190 (30.7) | 179 (28.5) | 181 (29.2) | 178 (28.5) | 202 (32.6) | 195 (31.4) | ||
| ≥80 | 408 (16.4) | 97 (16.2) | 117 (18.4) | 105 (17.0) | 89 (14.1) | 82 (13.2) | 79 (12.7) | 124 (20.0) | 123 (19.8) | ||
| Sex | |||||||||||
| Female | 1292 (52.0) | 247 (41.2) | 304 (47.8) | 349 (56.4) | 392 (62.3) | <0.01 | 320 (51.6) | 315 (50.6) | 347 (56.1) | 310 (49.9) | 0.13 |
| Male | 1191 (48.0) | 352 (58.8) | 332 (52.2) | 270 (43.6) | 237 (37.7) | 300 (48.4) | 308 (49.4) | 272 (43.9) | 311 (50.1) | ||
| Race | |||||||||||
| White | 1408 (56.7) | 345 (57.6) | 400 (62.9) | 343 (55.4) | 320 (50.9) | <0.01 | 272 (43.9) | 346 (55.5) | 379 (61.2) | 411 (66.2) | <0.01 |
| Black | 400 (16.1) | 82 (13.7) | 81 (13.7) | 98 (15.3) | 139 (22.1) | 170 (27.4) | 86 (13.8) | 78 (12.6) | 66 (10.6) | ||
| Other | 675 (27.2) | 172 (28.7) | 155 (24.4) | 178 (28.8) | 170 (27.0) | 178 (28.7) | 191 (30.7) | 162 (26.2) | 144 (23.2) | ||
| Education | |||||||||||
| High school or less | 1555 (62.6) | 343 (57.3) | 381 (59.9) | 410 (66.2) | 421 (66.9) | <0.01 | 396 (63.9) | 396 (63.5) | 393 (63.5) | 370 (59.6) | 0.76 |
| Attended college | 504 (20.3) | 117 (19.5) | 129 (20.3) | 121 (19.6) | 137 (21.8) | 123 (19.8) | 122 (19.6) | 123 (19.9) | 136 (21.9) | ||
| Graduated from college | 423 (17.1) | 139 (23.2) | 126 (19.8) | 88 (14.2) | 71 (11.3) | 101 (16.3) | 105 (16.9) | 103 (16.6) | 115 (18.5) | ||
| Marital status | |||||||||||
| Not married | 896 (36.1) | 198 (33.1) | 203 (31.9) | 227 (36.7) | 268 (42.6) | <0.01 | 221 (35.7) | 205 (32.9) | 224 (36.2) | 246 (39.6) | 0.11 |
| Married or living with partner | 1587 (63.9) | 401 (66.9) | 433 (68.1) | 392 (63.3) | 361 (57.4) | 399 (64.4) | 418 (67.1) | 395 (63.8) | 375 (60.4) | ||
| Smoking status | |||||||||||
| Never | 1161 (46.8) | 304 (50.8) | 279 (43.8) | 283 (45.7) | 295 (46.9) | 0.02 | 311 (50.1) | 304 (48.8) | 269 (43.5) | 277 (44.6) | 0.06 |
| Current | 310 (12.5) | 51 (8.5) | 82 (12.8) | 86 (13.9) | 91 (14.5) | 70 (11.3) | 63 (10.1) | 86 (13.9) | 91 (14.6) | ||
| Former | 1012 (40.8) | 244 (40.7) | 275 (43.2) | 250 (40.4) | 243 (38.6) | 239 (38.6) | 256 (41.1) | 264 (42.6) | 253 (40.7) | ||
| RFM | |||||||||||
| Low | 218 (8.8) | 91 (15.1) | 57 (8.9) | 35 (5.7) | 35 (5.6) | <0.01 | 58 (9.3) | 50 (8.0) | 52 (8.4) | 58 (9.3) | 0.39 |
| Moderate | 672 (27.1) | 227 (37.9) | 188 (29.6) | 141 (22.9) | 116 (18.4) | 190 (30.7) | 170 (27.3) | 154 (24.9) | 158 (25.4) | ||
| High | 1126 (45.4) | 228 (38.1) | 305 (48.0) | 304 (49.1) | 289 (45.9) | 270 (43.5) | 280 (45.0) | 286 (46.2) | 290 (46.7) | ||
| Very high | 467 (18.8) | 53 (8.9) | 86 (13.5) | 139 (22.4) | 189 (30.1) | 102 (16.5) | 123 (19.7) | 127 (20.5) | 115 (18.5) | ||
| Regular physical activity | |||||||||||
| No | 1207 (48.6) | 255 (42.6) | 286 (45.0) | 307 (49.6) | 359 (57.1) | <0.01 | 287 (46.3) | 297 (47.7) | 309 (49.9) | 314 (50.6) | 0.40 |
| Yes | 1276 (51.4) | 344 (57.4) | 350 (55.0) | 312 (50.4) | 270 (42.9) | 333 (53.7) | 326 (52.3) | 310 (50.1) | 307 (49.4) | ||
| Alcohol drinking | |||||||||||
| No | 960 (38.6) | 219 (36.5) | 227 (35.7) | 245 (39.6) | 269 (42.8) | 0.02 | 266 (42.9) | 248 (39.8) | 218 (35.2) | 228 (36.7) | <0.01 |
| ≤1 drink/day | 593 (23.9) | 162 (27.1) | 168 (26.4) | 141 (22.8) | 122 (19.4) | 122 (19.7) | 141 (22.6) | 190 (30.7) | 140 (22.5) | ||
| >1 drink/day | 930 (37.5) | 218 (36.4) | 241 (37.9) | 233 (37.6) | 238 (37.8) | 232 (37.4) | 234 (37.6) | 211 (34.1) | 253 (40.8) | ||
| Carbohydrate intake (g/day) | |||||||||||
| <153.9 | 621 (25.0) | 111 (18.5) | 152 (26.3) | 156 (25.2) | 202 (32.1) | <0.01 | 162 (26.1) | 158 (25.5) | 142 (22.9) | 159 (25.6) | 0.65 |
| 153.9–205.8 | 593 (23.9) | 143 (23.3) | 148 (23.3) | 157 (25.3) | 145 (23.1) | 141 (22.7) | 160 (25.7) | 147 (23.8) | 145 (23.4) | ||
| 205.9–268.9 | 643 (25.9) | 155 (25.9) | 173 (27.2) | 160 (25.9) | 155 (24.6) | 159 (25.7) | 156 (25.0) | 178 (28.8) | 150 (24.1) | ||
| ≥269.0 | 626 (25.2) | 190 (31.7) | 163 (25.6) | 146 (23.6) | 127 (20.2) | 158 (25.5) | 149 (23.9) | 152 (24.6) | 167 (26.9) | ||
| Total fat intake (g/day) | |||||||||||
| <42.2 | 624 (25.1) | 134 (22.4) | 153 (24.1) | 157 (25.4) | 180 (28.6) | 0.19 | 162 (26.1) | 161 (25.8) | 149 (24.1) | 152 (24.5) | 0.83 |
| 42.2–60.1 | 614 (24.7) | 156 (26.0) | 143 (22.5) | 155 (25.0) | 160 (25.5) | 152 (24.5) | 164 (26.3) | 152 (24.6) | 146 (23.5) | ||
| 60.2–82.9 | 631 (25.4) | 151 (25.2) | 170 (26.7) | 155 (25.0) | 155 (24.6) | 158 (25.5) | 142 (22.8) | 160 (25.8) | 171 (27.5) | ||
| ≥83.0 | 614 (24.7) | 158 (26.4) | 170 (26.7) | 152 (24.6) | 134 (21.3) | 148 (23.9) | 156 (25.1) | 158 (25.5) | 152 (24.5) | ||
| Protein intake (g/day) | |||||||||||
| < 48.3 | 617 (24.9) | 115 (19.2) | 154 (24.2) | 165 (26.6) | 183 (29.1) | <0.01 | 142 (22.9) | 161 (25.8) | 152 (24.6) | 162 (26.1) | 0.78 |
| 48.3–65.4 | 615 (24.8) | 143 (23.9) | 139 (21.9) | 160 (25.9) | 173 (27.5) | 150 (24.2) | 146 (23.4) | 157 (25.4) | 162 (26.1) | ||
| 65.5–85.1 | 630 (25.3) | 166 (27.7) | 165 (25.9) | 157 (25.4) | 142 (22.6) | 158 (25.5) | 163 (26.2) | 162 (26.2) | 147 (23.6) | ||
| ≥85.2 | 621 (25.0) | 175 (29.2) | 178 (28.0) | 137 (22.1) | 131 (20.8) | 170 (27.4) | 153 (24.6) | 148 (23.9) | 150 (24.2) | ||
| Energy intake (kcal/day) | |||||||||||
| < 1259.0 | 622 (25.1) | 116 (19.4) | 161 (25.3) | 159 (25.7) | 186 (29.6) | <0.01 | 154 (24.8) | 174 (27.9) | 146 (23.6) | 148 (23.8) | 0.84 |
| 1259.0–1654.3 | 592 (23.8) | 145 (24.2) | 130 (20.4) | 158 (25.5) | 159 (25.3) | 149 (24.0) | 140 (22.5) | 146 (23.6) | 157 (25.3) | ||
| 1654.4–2133.7 | 641 (25.8) | 163 (27.2) | 174 (27.4) | 151 (24.4) | 153 (24.3) | 163 (26.2) | 154 (24.7) | 167 (26.9) | 157 (25.3) | ||
| ≥2133.8 | 628 (25.3) | 175 (29.2) | 171 (26.9) | 151 (24.4) | 131 (20.8) | 154 (24.8) | 155 (24.9) | 160 (25.9) | 159 (25.6) | ||
| Multimorbidity * | |||||||||||
| No | 894 (36.0) | 247 (41.2) | 217 (34.1) | 226 (36.5) | 204 (32.4) | <0.01 | 238 (38.4) | 260 (41.7) | 202 (32.6) | 194 (31.2) | <0.01 |
| Yes | 1589 (64.0) | 352 (58.8) | 419 (65.9) | 393 (63.5) | 425 (67.6) | 382 (61.6) | 363 (58.3) | 417 (67.4) | 427 (68.8) | ||
| Respiratory disease § | |||||||||||
| No | 2219 (89.4) | 559 (93.3) | 572 (89.9) | 543 (87.7) | 545 (86.6) | <0.01 | 569 (91.8) | 572 (91.8) | 548 (88.5) | 530 (85.4) | <0.01 |
| Yes | 264 (10.6) | 40 (6.7) | 64 (10.1) | 76 (12.3) | 84 (13.4) | 51 (8.2) | 51 (8.2) | 71 (11.5) | 91 (14.6) | ||
| Hypertension | |||||||||||
| No | 906 (36.5) | 245 (40.9) | 237 (37.3) | 219 (35.4) | 205 (32.6) | 0.02 | 234 (37.7) | 239 (38.4) | 233 (37.6) | 200 (32.2) | 0.09 |
| Yes | 1577 (63.5) | 354 (59.1) | 399 (62.7) | 400 (64.6) | 424 (67.4) | 386 (62.3) | 384 (61.6) | 386 (62.4) | 421 (67.8) | ||
| CVD † | |||||||||||
| No | 1932 (77.8) | 454 (75.8) | 488 (76.7) | 512 (82.7) | 478 (76.0) | <0.01 | 493 (79.5) | 494 (79.3) | 479 (77.4) | 466 (75.0) | 0.19 |
| Yes | 551 (22.2) | 145 (24.2) | 148 (23.3) | 107 (17.3) | 151 (24.0) | 127 (20.5) | 129 (20.7) | 140 (22.6) | 155 (25.0) | ||
| Diabetes | |||||||||||
| No | 1949 (78.5) | 466 (77.8) | 513 (80.7) | 474 (76.6) | 496 (78.9) | 0.34 | 483 (77.9) | 478 (76.7) | 500 (80.8) | 488 (78.6) | 0.36 |
| Yes | 534 (21.5) | 133 (22.2) | 123 (19.3) | 145 (23.4) | 133 (21.1) | 137 (22.1) | 145 (23.3) | 119 (19.2) | 133 (21.4) | ||
| Chronic kidney disease | |||||||||||
| No | 2387 (96.1) | 586 (97.8) | 612 (96.2) | 597 (96.5) | 592 (94.1) | <0.01 | 598 (96.5) | 606 (97.3) | 596 (96.3) | 587 (94.5) | 0.08 |
| Yes | 96 (3.9) | 13 (2.2) | 24 (3.8) | 22 (3.5) | 37 (5.9) | 22 (3.5) | 17 (2.7) | 23 (3.7) | 34 (5.5) | ||
| Arthritis | |||||||||||
| No | 1159 (46.7) | 318 (53.1) | 283 (44.5) | 290 (46.9) | 268 (42.6) | <0.01 | 306 (49.4) | 301 (48.3) | 265 (43.8) | 287 (46.2) | 0.10 |
| Yes | 1324 (53.3) | 281 (46.9) | 353 (55.5) | 329 (53.1) | 361 (57.4) | 314 (50.6) | 322 (51.7) | 354 (57.2) | 334 (53.8) | ||
| Osteoporosis | |||||||||||
| No | 2,163 (87.1) | 526 (87.2) | 551 (86.6) | 535 (86.4) | 551 (87.6) | 0.85 | 552 (89.0) | 548 (88.0) | 526 (85.0) | 537 (86.5) | 0.16 |
| Yes | 320 (12.9) | 73 (12.8) | 85 (13.4) | 84 (13.6) | 78 (12.4) | 68 (11.0) | 75 (12.0) | 93 (15.0) | 84 (13.5) | ||
| Cancer | |||||||||||
| No | 1989 (80.1) | 470 (78.5) | 502 (78.9) | 499 (80.6) | 518 (82.4) | 0.30 | 515 (83.1) | 505 (81.1) | 482 (77.9) | 487 (78.4) | 0.08 |
| Yes | 494 (19.9) | 129 (21.5) | 134 (21.1) | 120 (19.4) | 111 (17.6) | 105 (16.9) | 118 (18.9) | 137 (22.1) | 134 (21.6) | ||
| Varibales | No. Sarcopenia /Overall | Prevalence (%) and 95% CI | cOR and 95% CI (n = 2483) | aOR and 95% CI † (n = 2483) | aOR and 95% CI § (n = 2483) |
|---|---|---|---|---|---|
| CRP (mg/L) | |||||
| <1.2 | 161/599 | 26.9 (23.5, 30.6) | REF | REF | REF |
| 1.2–2.6 | 151/636 | 23.7 (20.6, 27.2) | 0.85 (0.66 1.10) | 1.02 (0.75, 1.38) | 0.89 (0.61, 1.33) |
| 2.7–5.2 | 141/619 | 22.8 (19.6, 26.3) | 0.80 (0.62, 1.04) | 1.28 (0.93, 1.76) | 1.05 (0.76, 1.46) |
| ≥5.3 | 121/629 | 19.2 (16.3, 22.5) | 0.65 (0.49, 0.87) | 1.29 (0.93, 1.80) | 1.44 (0.95, 2.16) |
| p-trend < 0.01 | p-trend = 0.06 | p-trend = 0.07 | |||
| SII(×109 cells/L) | |||||
| <365.7 | 118/620 | 19.0 (16.1, 22.3) | REF | REF | REF |
| 365.7–503.6 | 109/623 | 17.5 (14.7, 20.7) | 0.90 (0.68, 1.20) | 0.89 (0.64, 1.24) | 0.90 (0.59, 1.37) |
| 503.7–704.0 | 156/619 | 25.2 (21.9, 28.8) | 1.43 (1.09, 1.88) | 1.45 (1.05, 2.01) | 1.36 (0.84, 2.18) |
| ≥704.1 | 191/621 | 30.8 (27.2, 34.5) | 1.89 (1.45, 2.46) | 1.90 (1.38, 2.62) | 2.27 (1.63, 3.15) |
| p-trend < 0.01 | p-trend < 0.01 | p-trend < 0.01 | |||
| Variables | CRP (mg/L) | p-Trend | SII (×109 cells/L) | p-Trend | ||||
|---|---|---|---|---|---|---|---|---|
| aOR and 95% CI | aOR and 95% CI | |||||||
| 1.2–2.5 vs. < 1.2 | 2.6–5.2 vs. <1.2 | ≥5.3 vs. <1.2 | 365.7–503.6 vs. <365.7 | 503.7–704.0 vs. < 365.7 | ≥704.1 vs. <365.7 | |||
| Age (year) | ||||||||
| <70 (n = 1319) | 0.91 (0.57, 1.47) | 1.07 (0.66, 1.76) | 1.7 (0.70, 1.94) | 0.48 | 0.79 (0.48, 1.32) | 1.72 (1.04, 2.85) | 1.65 (1.00, 2.72) | <0.01 |
| ≥70 (n = 1164) | 1.21 (0.81, 1.82) | 1.57 (1.03, 2.39) | 1.46 (0.94, 2.27) | 0.04 | 0.98 (0.62, 1.55) | 1.41 (0.91, 2.17) | 2.24 (1.45, 3.46) | <0.01 |
| p-interaction = 0.74 | p-interaction = 0.28 | |||||||
| Sex | ||||||||
| Female (n = 1292) | 0.91 (0.57, 1.45) | 1.21 (0.76, 1.95) | 1.00 (0.62, 1.62) | 0.71 | 0.74 (0.44, 1.22) | 1.45 (0.91, 2.30) | 1.66 (1.04, 267) | <0.01 |
| Male (n = 1191) | 1.22 (0.73, 1.69) | 1.29 (0.82, 2.00) | 1.40 (0.86, 2.26) | 0.13 | 1.10 (0.69, 1.76) | 1.35 (0.84, 2.16) | 2.14 (1.36, 3.37) | <0.01 |
| p-interaction = 0.63 | p-interaction = 0.63 | |||||||
| Multimorbidity | ||||||||
| No (n = 894) | 1.04 (0.61, 1.75) | 1.48 (0.86, 2.53) | 0.97 (0.54, 1.74) | 0.66 | 1.40 (0.81, 2.39) | 1.84 (1.04, 3.27) | 2.72 (1.53, 4.84) | <0.01 |
| Yes (n = 1589) | 1.00 (0.68, 1.48) | 1.24 (0.89, 1.87) | 1.56 (1.03, 2.36) | 0.02 | 0.64 (0.40, 1.01) | 1.29 (0.85, 1.94) | 1.66 (1.11, 2.46) | <0.01 |
| p-interaction = 0.32 | p-interaction = 0.28 |
| Variables | No. Sarcopenic Obesity/ Overall | Prevalence (%) and 95% CI | cOR and 95% CI (n = 2483) | aOR and 95% CI † (n = 2483) | aOR and 95% CI § (n = 2483) |
|---|---|---|---|---|---|
| CRP (mg/L) | |||||
| <1.2 | 35/599 | 5.8 (4.2, 8.0) | REF | REF | REF |
| 1.2–2.5 | 53/636 | 8.3 (6.4, 10.8) | 1.46 (0.94, 2.27) | 1.43 (0.91, 2.26) | 1.37 (0.72, 2.61) |
| 2.6–5.2 | 52/619 | 8.4 (6.5, 10.9) | 1.28 (0.95, 2.30) | 1.44 (0.91, 2.28) | 1.30 (0.68, 2.48) |
| ≥5.3 | 50/629 | 7.9 (6.0, 10.3) | 1.39 (0.89, 2.17) | 1.46 (0.92, 2.33) | 1.61 (0.86, 3.03) |
| p-trend = 0.19 | p-trend = 0.15 | p-trend = 0.19 | |||
| SII (×109 cells/L) | |||||
| <365.7 | 31/620 | 5.0 (3.5, 7.0) | REF | REF | REF |
| 365.7–503.6 | 33/623 | 5.3 (3.8, 7.4) | 1.06 (0.64 1.76) | 0.97 (0.57, 1.62) | 0.99 (0.52, 1.85) |
| 503.7–704.0 | 57/619 | 9.2 (7.1, 11.8) | 1.92 (1.23, 3.03) | 1.58 (0.99, 2.54) | 1.34 (0.71, 2.52) |
| ≥704.1 | 69/621 | 11.1 (8.9, 13.8) | 2.38 (1.53, 3.69) | 1.94 (1.23, 3.07) | 2.32 (1.32, 4.05) |
| p-trend < 0.01 | p-trend < 0.01 | p-trend < 0.01 |
| Variables | CRP (mg/L) | p-Trend | SII (×109 cells/L) | p-Trend | ||||
|---|---|---|---|---|---|---|---|---|
| aOR and 95% CI | aOR and 95% CI | |||||||
| 1.2–2.5 vs. <1.2 | 2.6–5.2 vs. <1.2 | ≥ 5.3 vs. <1.2 | 365.7–503.6 vs. <365.7 | 503.7–704.0 vs. <365.7 | ≥704.1 vs. <365.7 | |||
| Age (year) | ||||||||
| <70 (n = 1319) | 1.15 (0.51, 2.61) | 1.31 (0.60, 2.88) | 1.43 (0.65, 3.13) | 0.34 | 0.59 (0.24, 1.44) | 2.01 (0.95,4.25) | 1.46 (0.66, 3.20) | 0.06 |
| ≥70(n = 1164) | 1.62 (0.93, 2.83) | 1.48 (0.84, 2.62) | 1.36 (0.75, 2.45) | 0.43 | 1.29 (0.67, 2.48) | 1.46 (0.79, 2.69) | 2.41 (1.35, 4.30) | <0.01 |
| p-interaction = 0.78 | p-interaction = 0.08 | |||||||
| Sex | ||||||||
| Female (n = 1292) | 1.66 (0.85, 3.27) | 1.37 (0.70, 2.69) | 1.27 (0.65, 2.49) | 0.78 | 0.92 (0.43, 1.96) | 1.85 (0.94, 3.61) | 2.45 (1.27, 4.74) | <0.01 |
| Male (n = 1191) | 1.30 (0.69, 2.45) | 1.58 (0.82, 3.03) | 1.62 (0.82, 3.18) | 0.13 | 1.01 (0.49, 2.11) | 1.46 (0.73, 2.92) | 1.78 (0.92, 3.44) | 0.04 |
| p-interaction = 0.69 | p-interaction = 0.96 | |||||||
| Multimorbidity | ||||||||
| No (n = 894) | 0.96 (0.38, 2.39) | 1.63 (0.71, 3.74) | 1.30 (0.53, 3.20) | 0.34 | 1.52 (0.56, 4.08) | 2.58 (0.98, 6.78) | 2.54 (0.97, 6.63) | 0.03 |
| Yes (n = 1589) | 1.68 (0.97, 2.88) | 1.52 (0.86, 2.68) | 1.61 (0.91, 2.83) | 0.18 | 0.80 (0.43, 1.51) | 1.34 (0.77, 2.32) | 1.83 (1.07, 3.11) | <0.01 |
| p-interaction = 0.67 | p-interaction = 0.76 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karanth, S.D.; Washington, C.; Cheng, T.-Y.D.; Zhou, D.; Leeuwenburgh, C.; Braithwaite, D.; Zhang, D. Inflammation in Relation to Sarcopenia and Sarcopenic Obesity among Older Adults Living with Chronic Comorbidities: Results from the National Health and Nutrition Examination Survey 1999–2006. Nutrients 2021, 13, 3957. https://doi.org/10.3390/nu13113957
Karanth SD, Washington C, Cheng T-YD, Zhou D, Leeuwenburgh C, Braithwaite D, Zhang D. Inflammation in Relation to Sarcopenia and Sarcopenic Obesity among Older Adults Living with Chronic Comorbidities: Results from the National Health and Nutrition Examination Survey 1999–2006. Nutrients. 2021; 13(11):3957. https://doi.org/10.3390/nu13113957
Chicago/Turabian StyleKaranth, Shama D., Caretia Washington, Ting-Yuan D. Cheng, Daohong Zhou, Christiaan Leeuwenburgh, Dejana Braithwaite, and Dongyu Zhang. 2021. "Inflammation in Relation to Sarcopenia and Sarcopenic Obesity among Older Adults Living with Chronic Comorbidities: Results from the National Health and Nutrition Examination Survey 1999–2006" Nutrients 13, no. 11: 3957. https://doi.org/10.3390/nu13113957
APA StyleKaranth, S. D., Washington, C., Cheng, T.-Y. D., Zhou, D., Leeuwenburgh, C., Braithwaite, D., & Zhang, D. (2021). Inflammation in Relation to Sarcopenia and Sarcopenic Obesity among Older Adults Living with Chronic Comorbidities: Results from the National Health and Nutrition Examination Survey 1999–2006. Nutrients, 13(11), 3957. https://doi.org/10.3390/nu13113957