
Nationwide Representative Survey of Dietary Iodine Intake and Urinary Excretion in Postpartum Korean Women

 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Methods
2.2.1. Survey Questionnaire
2.2.2. Nutrient and Iodine Intake Assessments
2.2.3. Measurement of Urinary Iodine Concentration
2.2.4. Statistical Analysis
3. Results
3.1. General Characteristics of Participants
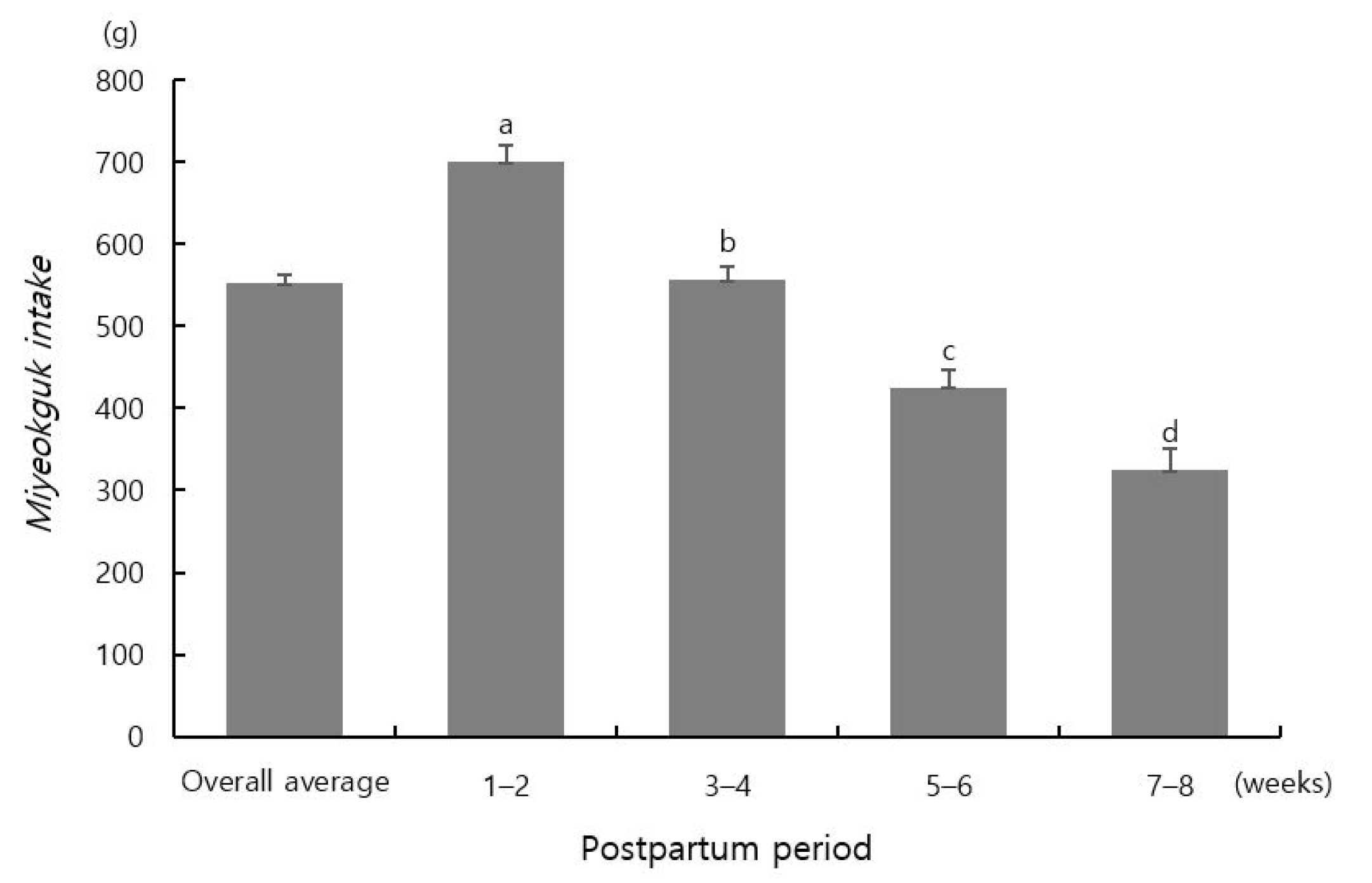
3.2. Miyeokguk Intake
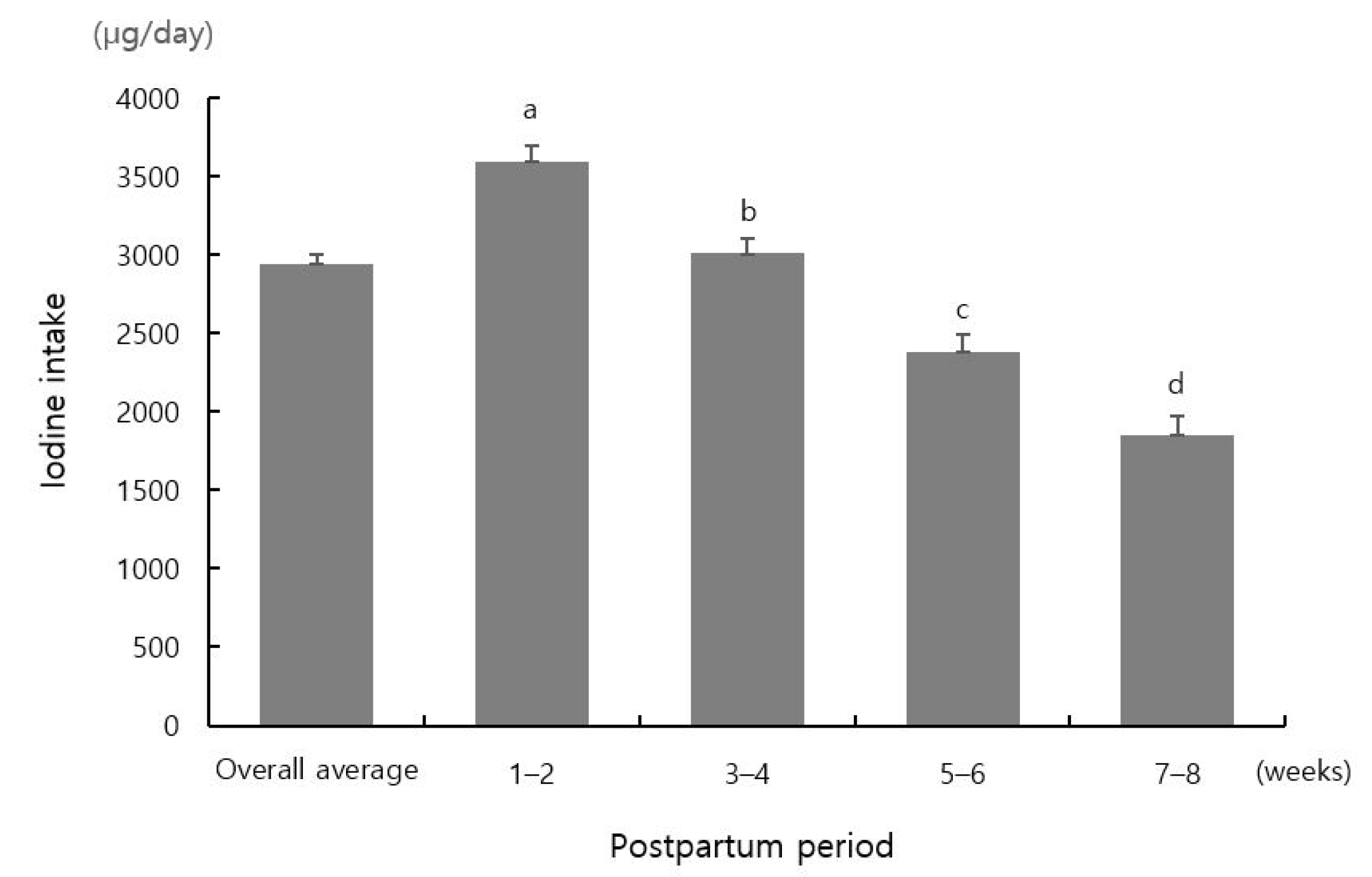
3.3. Nutrient and Iodine Intake
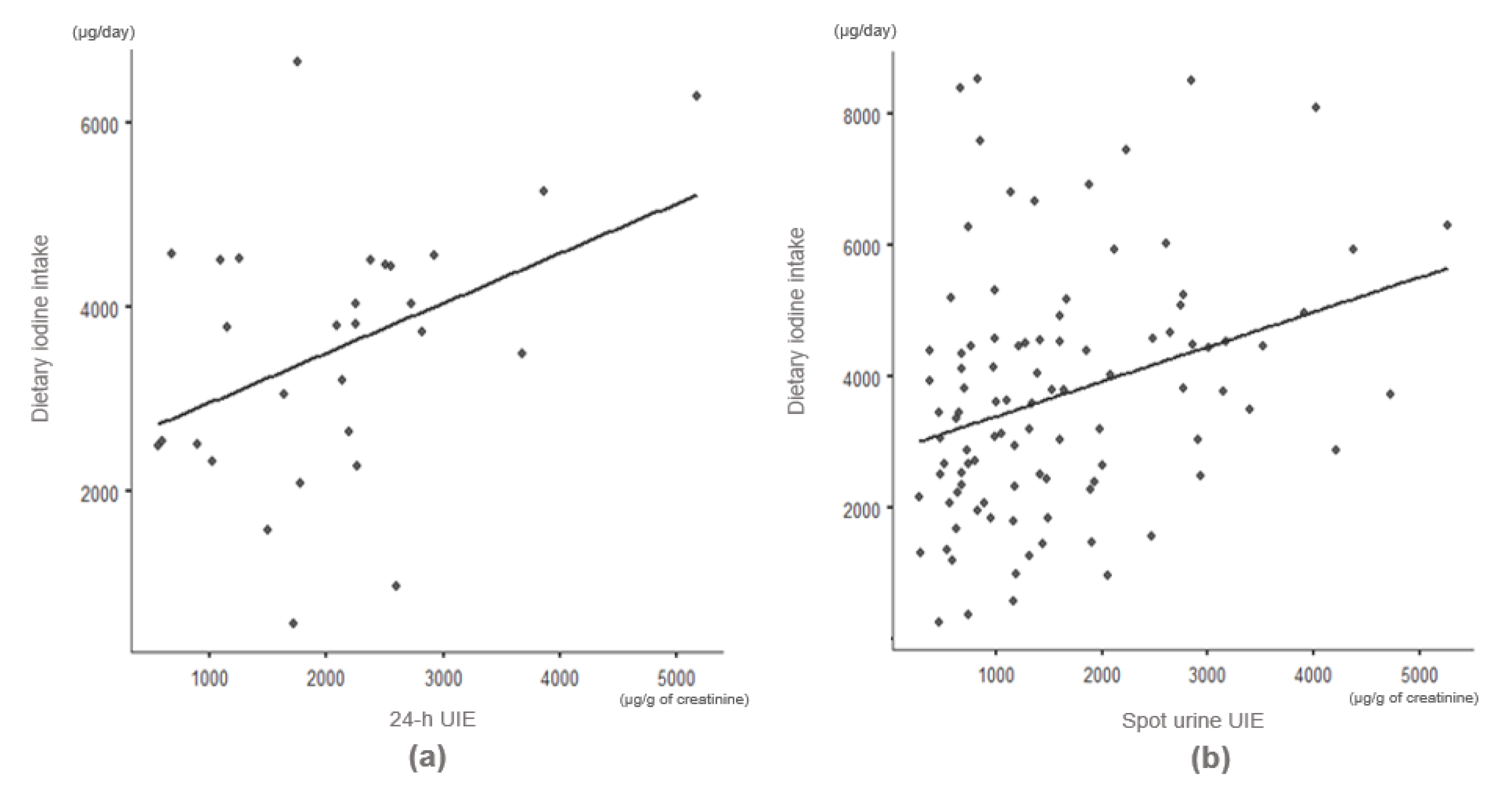
3.4. Relation between Dietary Iodine Intake and Urinary Iodine Excretion
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pérez-López, F.R. Iodine and thyroid hormones during pregnancy and postpartum. Gynecol. Endocrinol. 2007, 23, 414–428. [Google Scholar] [CrossRef] [PubMed]
- Wolmarans, D.W. Maintaining euthyroidism: Fundamentals of thyroid hormone physiology, iodine metabolism and hypothyroidism. S. Afr. Fam. Pract. 2017, 59, 11–21. [Google Scholar] [CrossRef]
- Teng, W.; Shan, Z.; Teng, X.; Guan, H.; Li, Y.; Teng, D.; Jin, Y.; Yu, X.; Fan, C.; Chong, W.; et al. Effect of iodine intake on thyroid diseases in China. N. Engl. J. Med. 2006, 354, 2783–2793. [Google Scholar]
- Laurberg, P.; Cerqueira, C.; Ovesen, L.; Rasmussen, L.B.; Perrild, H.; Andersen, S.; Pedersen, I.B.; Carlé, A. Iodine intake as a determinant of thyroid disorders in populations. Best Pract. Res. Clin. Endocrinol. Metab. 2010, 24, 13–27. [Google Scholar] [CrossRef]
- Squatrito, S.; Delange, F.; Trimarchi, F.; Lisi, E.; Vigneri, R. Endemic cretinism in Sicily. J. Endocrinol. Investig. 1981, 4, 295–302. [Google Scholar]
- Yordam, N.; Özön, A.; Alikaşifoğlu, A.; Özgen, A.; Ceren, N.; Zafer, Y.; Şimşek, E. Iodine deficiency in Turkey. Eur. J. Pediatrics 1999, 158, 501–505. [Google Scholar] [CrossRef] [PubMed]
- Skeaff, S.A. Iodine deficiency in pregnancy: The effect on neurodevelopment in the child. Nutrients 2011, 3, 265–273. [Google Scholar] [PubMed]
- Choue, R.; Yim, J.; Cho, Y.; Lee, W. The effects of dietary iodine intake on the postpartum thyrioditis (PPT) manifestation. Korean J. Nutr. 1997, 30, 1195–1202. [Google Scholar]
- Pennington, J. A review of iodine toxicity reports. J. Am. Diet. Assoc. 1990, 90, 1571–1581. [Google Scholar]
- Tan, L.; Sang, Z.; Shen, J.; Liu, H.; Chen, W.; Zhao, N.; Wei, W.; Zhang, G.; Zhang, W. Prevalence of thyroid dysfunction with adequate and excessive iodine intake in Hebei Province, People’s Republic of China. Public Health Nutr. 2015, 18, 1692–1697. [Google Scholar] [CrossRef]
- Guan, H.; Ji, M.; Bao, R.; Yu, H.; Wang, Y.; Hou, P.; Zhang, Y.; Shan, Z.; Teng, W.; Xing, M. Association of high iodine intake with the T1799A BRAF mutation in papillary thyroid cancer. J. Clin. Endocrinol. Metab. 2009, 94, 1612–1617. [Google Scholar] [CrossRef]
- Jorgensen, A.; O’Leary, P.; James, I.; Skeaff, S.; Sherriff, J. Assessment of breast milk iodine concentrations in lactating women in Western Australia. Nutrients 2016, 8, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Mulrine, H.M.; Skeaff, S.A.; Ferguson, E.L.; Gray, A.R.; Valeix, P. Breast-milk iodine concentration declines over the first 6 mo postpartum in iodine-deficient women. Am. J. Clin. Nutr. 2010, 92, 849–856. [Google Scholar] [CrossRef]
- Ko, Y.M.; Kwon, Y.S.; Park, Y.K. An iodine database establishment and iodine intake in Korean adults: Based on the 1998~2014 Korea National Health and Nutrition Examination Survey. J. Nutr. Health 2017, 50, 624–644. [Google Scholar] [CrossRef]
- Seo, K. Almanac of Seasonal Customs of China; National Folk Museum of Korea: Seoul, Korea, 2006. [Google Scholar]
- Moon, S.; Kim, J. Iodine content of human milk and dietary iodine intake of Korean lactating mothers. Int. J. Food Sci. Nutr. 1999, 50, 165–171. [Google Scholar] [PubMed]
- Rhee, S.S.; Braverman, L.E.; Pino, S.; He, X.; Pearce, E.N. High iodine content of Korean seaweed soup: A health risk for lactating women and their infants? Thyroid 2011, 21, 927–928. [Google Scholar] [CrossRef] [PubMed]
- Andersson, M.; De Benoist, B.; Delange, F.; Zupan, J. Prevention and control of iodine deficiency in pregnant and lactating women and in children less than 2-years-old: Conclusions and recommendations of the Technical Consultation. Public Health Nutr. 2007, 10, 1606–1611. [Google Scholar]
- New South Wales Government. Warning to Pregnant and Breastfeeding Women: Seaweed Soup. Northern Sydney Local Health District 2012. Available online: https://www.mhcs.health.nsw.gov.au/publications/9120 (accessed on 1 August 2020).
- Chung, H.R.; Shin, C.H.; Yang, S.W.; Choi, C.W.; Kim, B.I. Subclinical hypothyroidism in Korean preterm infants associated with high levels of iodine in breast milk. J. Clin. Endocrinol. Metab. 2009, 94, 4444–4447. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Korean Statistical Information Service. National Vital Statistics Reports 2017; National Statistical Information Service: Daejeon, Korea, 2018.
- Park, K.S.; Yang, J.Y.; Kim, S.H.; Lee, J.Y. Study of International Standards for Iodine in Seaweed; Nov. Report No. 15162seafood661; National Institute of Food and Drug Safety: Cheongju, Korea, 2015.
- Kang, T.S.; Lee, J.H.; Leem, D.; Seo, I.W.; Lee, Y.J.; Yoon, T.H.; Lee, J.H.; Lee, Y.J.; Kim, Y.J.; Kim, S.G. Monitoring of Iodine in Foods for Estimation of Dietary Intake; National Institute of Food and Drug Safety: Cheongju, Korea, 2012.
- Rural Development Administration. Korean Food Composition Table, 9.1th ed.; Rural Development Administration: Jeonju, Korea, 2019.
- Ministry of Health and Welfare. Year Book on Postpartum Care Center 2019; Ministry of Health and Welfare: Sejong, Korea, 2019.
- Leung, A.M.; Pearce, E.N.; Braverman, L.E. Iodine nutrition in pregnancy and lactation. Endocrinol. Metab. Clin. 2011, 40, 765–777. [Google Scholar] [CrossRef]
- Ministry of Health and Welfare, The Korean Nutrition Society. Dietary Reference Intakes for Koreans 2020; Ministry of Health and Welfare: Sejong, Korea, 2020.
- Kim, H.; Lee, H.N.; Ha, J. Association high-iodine-containing seaweed soup consumption after birth and subclinical hypothyroidism in Korean women: Korea National Health and Nutrition Examination Survey IV (2013–2015). Int. J. Thyroidol. 2019, 12, 105–112. [Google Scholar] [CrossRef]
- Katagiri, R.; Asakura, K.; Uechi, K.; Masayasu, S.; Sasaki, S. Iodine Excretion in 24-hour Urine Collection and Its Dietary Determinants in Healthy Japanese Adults. J. Epidemiol. 2016, 26, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.B.; Yim, C.H.; Park, K.S.; Moon, B.S.; Lee, J.H.; Jun, H.W.; Jin, H.J.; Kim, S.Y.; Cho, B.Y.; Lee, H.G. The incidence of postpartum thyroiditis and effect of high iodine intake on it in Korean women. J. Korean Soc. Endocrinol. 1998, 13, 339–350. [Google Scholar]
- Wolff, J.; Chaikoff, I.L. Plasma inorganic iodide as a homeostatic regulator of thyroid function. J. Biol. Chem. 1948, 174, 555–564. [Google Scholar] [CrossRef]
- Eng, P.H.; Cardona, G.R.; Fang, S.L.; Previti, M.; Alex, S.; Carrasco, N.; Chin, W.W.; Braverman, L.E. Escape from the acute Wolff-Chaikoff effect is associated with a decrease in thyroid sodium/iodide symporter messenger ribonucleic acid and protein. Endocrinology 1999, 140, 3404–3410. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.M.; Braverman, L.E. Consequences of excess iodine. Nat. Rev. Endocrinol. 2014, 10, 136–142. [Google Scholar] [CrossRef]
- Jahreis, G.; Hausmann, W.; Kiessling, G.; Franke, K.; Leiterer, M. Bioavailability of iodine from normal diets rich in dairy products-results of balance studies in women. Exp. Clin. Endocrinol. Diabetes 2001, 109, 163–167. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 1054) | 1–2 Weeks (n = 368) | 3–4 Weeks (n = 351) | 5–6 Weeks (n = 201) | 7–8 Weeks (n = 134) | |
|---|---|---|---|---|---|
| Seoul | 549 (52.2) (1) | 205 (55.7) | 174 (49.6) | 102 (50.7) | 68 (50.7) |
| Yeongnam | 255 (24.1) | 95 (25.8) | 84 (23.9) | 40 (19.9) | 36 (26.9) |
| Chungcheong | 121 (11.5) | 37 (10.1) | 42 (12.0) | 32 (15.9) | 10 (7.5) |
| Gangwon | 31 (2.9) | 6 (1.6) | 12 (3.4) | 6 (3.0) | 7 (5.2) |
| Honam | 98 (9.3) | 25 (6.8) | 39 (11.1) | 21 (10.4) | 13 (9.7) |
| Variables | Total (n = 1054) | 1–2 Weeks (n = 368) | 3–4 Weeks (n = 351) | 5–6 Weeks (n = 201) | 7–8 Weeks (n = 134) | p |
|---|---|---|---|---|---|---|
| Age (years) | 32.5 ± 0.1 (1) | 32.4 ± 0.2 | 32.5 ± 0.2 | 32.2 ± 0.3 | 33.0 ± 0.3 | 0.231 |
| Anthropometric data | ||||||
| Height (cm) | 161.9 ± 0.2 | 162.1 ± 0.3 | 161.9 ± 0.3 | 161.7 ± 0.4 | 161.5 ± 0.4 | 0.617 |
| Weight (kg) | 63.3 ± 0.3 | 63.6 ± 0.5 | 63.6 ± 0.5 | 62.6 ± 0.7 | 62.5 ± 0.8 | 0.447 |
| Gestation period (weeks) | 38.7 ± 0.1 | 38.9 ± 0.1 | 38.6 ± 0.1 | 38.6 ± 0.1 | 38.1 ± 0.2 | <0.01 |
| Delivery type | 0.142 | |||||
| Normal delivery | 532(50.5) (2) | 199 (54.1) | 164 (46.7) | 107 (53.2) | 62 (46.3) | |
| Caesarean section | 522 (49.5) | 169 (45.9) | 187 (53.3) | 94 (46.8) | 72 (53.7) | |
| Feeding type | <0.01 | |||||
| Breastfeeding | 202 (19.2) | 36 (9.8) | 91 (25.9) | 46 (22.9) | 29 (21.6) | |
| Mixed feeding | 762 (72.3) | 322 (87.5) | 234 (66.7) | 129 (64.2) | 77 (57.5) | |
| Formula feeding | 90 (8.5) | 10 (2.7) | 26 (7.4) | 26 (12.9) | 28 (20.9) | |
| Alcohol drinking | <0.01 | |||||
| Yes | 49 (4.6) | 5 (1.4) | 15 (4.3) | 15 (7.5) | 14 (10.4) | |
| No | 1005 (95.4) | 363 (98.6) | 336 (95.7) | 186 (92.5) | 120 (89.6) | |
| Smoking | 0.169 | |||||
| Current smoking | 1 (0.1) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.7) | |
| Past smoking | 151 (14.3) | 45 (12.2) | 53 (15.1) | 31 (15.4) | 22 (16.4) | |
| Non-smoking | 902 (85.6) | 323 (87.8) | 298 (84.9) | 170 (84.6) | 111 (82.8) | |
| Regular physical exercise | <0.05 | |||||
| Yes | 214 (20.3) | 94 (25.5) | 57 (16.2) | 40 (19.9) | 23 (17.2) | |
| No | 840 (79.7) | 274 (74.5) | 294 (83.8) | 161 (80.1) | 111 (82.8) | |
| Monthly income (US $) | 0.115 | |||||
| <2000 | 75 (7.1) | 26 (7.1) | 29 (8.3) | 14 (7.0) | 6 (4.5) | |
| 2000–4000 | 597 (56.6) | 192 (52.2) | 208 (59.3) | 114 (56.7) | 83 (61.9) | |
| 4000–6000 | 255 (24.2) | 93 (25.3) | 80 (22.8) | 51 (25.4) | 31 (23.1) | |
| >6000 | 127 (12.0) | 57 (15.5) | 34 (9.7) | 22 (10.9) | 14 (10.4) | |
| Chronic disease | 0.633 | |||||
| Yes | 67 (6.4) | 20 (5.4) | 26 (7.4) | 11 (5.5) | 10 (7.5) | |
| No | 987 (93.6) | 348 (94.6) | 325 (92.6) | 19 (94.5) | 124 (92.5) | |
| Dietary supplement | 0.535 | |||||
| Yes | 861 (81.7) | 297 (80.7) | 295 (84.0) | 163 (81.1) | 106 (79.1) | |
| - Without iodine | 754 (87.6) | 260 (87.5) | 256 (86.8) | 141 (86.5) | 97 (91.5) | |
| - Containing iodine | 107 (12.4) | 37 (12.5) | 39 (13.2) | 22 (13.5) | 9 (8.5) | |
| No | 193 (18.3) | 71 (19.3) | 56 (16.0) | 38 (18.9) | 28 (20.9) | |
| Total | 1–2 Weeks | 3–4 Weeks | 5–6 Weeks | 7–8 Weeks | p | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (n = 1054) | (n = 368) | (n = 351) | (n = 201) | (n = 134) | ||||||||||||
| Energy (kcal) | 2074.8 | ± | 18.9 (1) | 2403.8 | ± | 30.8 | 2003.3 | ± | 28.7 | 1776.7 | ± | 35.6 | 1805.8 | ± | 51.8 | <0.01 |
| Carbohydrate (g) | 273.1 | ± | 2.4 | 305.2 | ± | 4.0 | 266.8 | ± | 3.8 | 242.7 | ± | 4.8 | 246.7 | ± | 6.8 | <0.01 |
| Protein (g) | 88.6 | ± | 0.9 | 104.0 | ± | 1.4 | 85.3 | ± | 1.3 | 75.9 | ± | 1.8 | 73.7 | ± | 2.5 | <0.01 |
| Fat (g) | 69.2 | ± | 0.8 | 84.7 | ± | 1.3 | 65.7 | ± | 1.3 | 55.1 | ± | 1.5 | 57.4 | ± | 2.2 | <0.01 |
| Fibre (g) | 37.8 | ± | 0.4 | 45.1 | ± | 0.7 | 37.3 | ± | 0.7 | 31.1 | ± | 0.9 | 28.6 | ± | 1.3 | <0.01 |
| Vitamin A (RE) | 579.2 | ± | 9.1 | 706.7 | ± | 14.8 | 537.5 | ± | 14.2 | 476.0 | ± | 19.1 | 492.7 | ± | 28.0 | <0.01 |
| Retinol (μg) | 146.7 | ± | 3.9 | 154.2 | ± | 5.2 | 137.4 | ± | 6.3 | 135.1 | ± | 9.3 | 167.6 | ± | 15.9 | 0.034 |
| Carotene (μg) | 5190.0 | ± | 95.1 | 6630.0 | ± | 154.5 | 4801.5 | ± | 151.1 | 4090.9 | ± | 186.7 | 3901.5 | ± | 272.1 | <0.01 |
| Vitamin C (mg) | 78.4 | ± | 1.4 | 97.7 | ± | 2.3 | 74.6 | ± | 2.2 | 63.7 | ± | 2.8 | 57.8 | ± | 3.2 | <0.01 |
| Vitamin B1 (mg) | 1.9 | ± | 0.02 | 2.1 | ± | 0.03 | 1.8 | ± | 0.03 | 1.6 | ± | 0.04 | 1.6 | ± | 0.06 | <0.01 |
| Vitamin B2 (mg) | 1.8 | ± | 0.02 | 2.2 | ± | 0.04 | 1.7 | ± | 0.03 | 1.6 | ± | 0.04 | 1.6 | ± | 0.06 | <0.01 |
| Niacin (mg) | 15.7 | ± | 0.2 | 18.7 | ± | 0.3 | 15.0 | ± | 0.3 | 13.3 | ± | 0.3 | 13.2 | ± | 0.5 | <0.01 |
| Calcium (mg) | 672.2 | ± | 8.5 | 756.5 | ± | 12.7 | 668.0 | ± | 15.2 | 597.8 | ± | 19.0 | 563.7 | ± | 23.0 | <0.01 |
| P (mg) | 1311.0 | ± | 13.5 | 1494.7 | ± | 20.3 | 1284.0 | ± | 23.8 | 1153.2 | ± | 27.1 | 113.7 | ± | 36.5 | <0.01 |
| Sodium (mg) | 6156.4 | ± | 68.2 | 7297.6 | ± | 96.0 | 6048.3 | ± | 110.8 | 5192.0 | ± | 148.2 | 4752.4 | ± | 182.0 | <0.01 |
| K (mg) | 3757.2 | ± | 40.6 | 4401.5 | ± | 61.0 | 3727.5 | ± | 63.8 | 3176.6 | ± | 83.1 | 2936.6 | ± | 115.2 | <0.01 |
| Fe (mg) | 19.7 | ± | 0.3 | 23.5 | ± | 0.4 | 18.9 | ± | 0.5 | 17.0 | ± | 0.5 | 15.6 | ± | 0.6 | <0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, D.-K.; Lee, H.; Lee, H.; Yoon, T.; Park, S.-J.; Lee, H.-J. Nationwide Representative Survey of Dietary Iodine Intake and Urinary Excretion in Postpartum Korean Women. Nutrients 2021, 13, 3955. https://doi.org/10.3390/nu13113955
Lee D-K, Lee H, Lee H, Yoon T, Park S-J, Lee H-J. Nationwide Representative Survey of Dietary Iodine Intake and Urinary Excretion in Postpartum Korean Women. Nutrients. 2021; 13(11):3955. https://doi.org/10.3390/nu13113955
Chicago/Turabian StyleLee, Do-Kyung, Hunjoo Lee, Hyeyoung Lee, Taehyung Yoon, Seon-Joo Park, and Hae-Jeung Lee. 2021. "Nationwide Representative Survey of Dietary Iodine Intake and Urinary Excretion in Postpartum Korean Women" Nutrients 13, no. 11: 3955. https://doi.org/10.3390/nu13113955
APA StyleLee, D.-K., Lee, H., Lee, H., Yoon, T., Park, S.-J., & Lee, H.-J. (2021). Nationwide Representative Survey of Dietary Iodine Intake and Urinary Excretion in Postpartum Korean Women. Nutrients, 13(11), 3955. https://doi.org/10.3390/nu13113955