
Low-Carbohydrate Diet among Children with Type 1 Diabetes: A Multi-Center Study

 ,
,
Abstract
:1. Introduction
2. Research Design and Methods
2.1. Study Population Characteristic
2.2. Assessment of Dietary Habits
2.3. Clinical and Laboratory Data
2.4. Statistical Analysis
3. Results
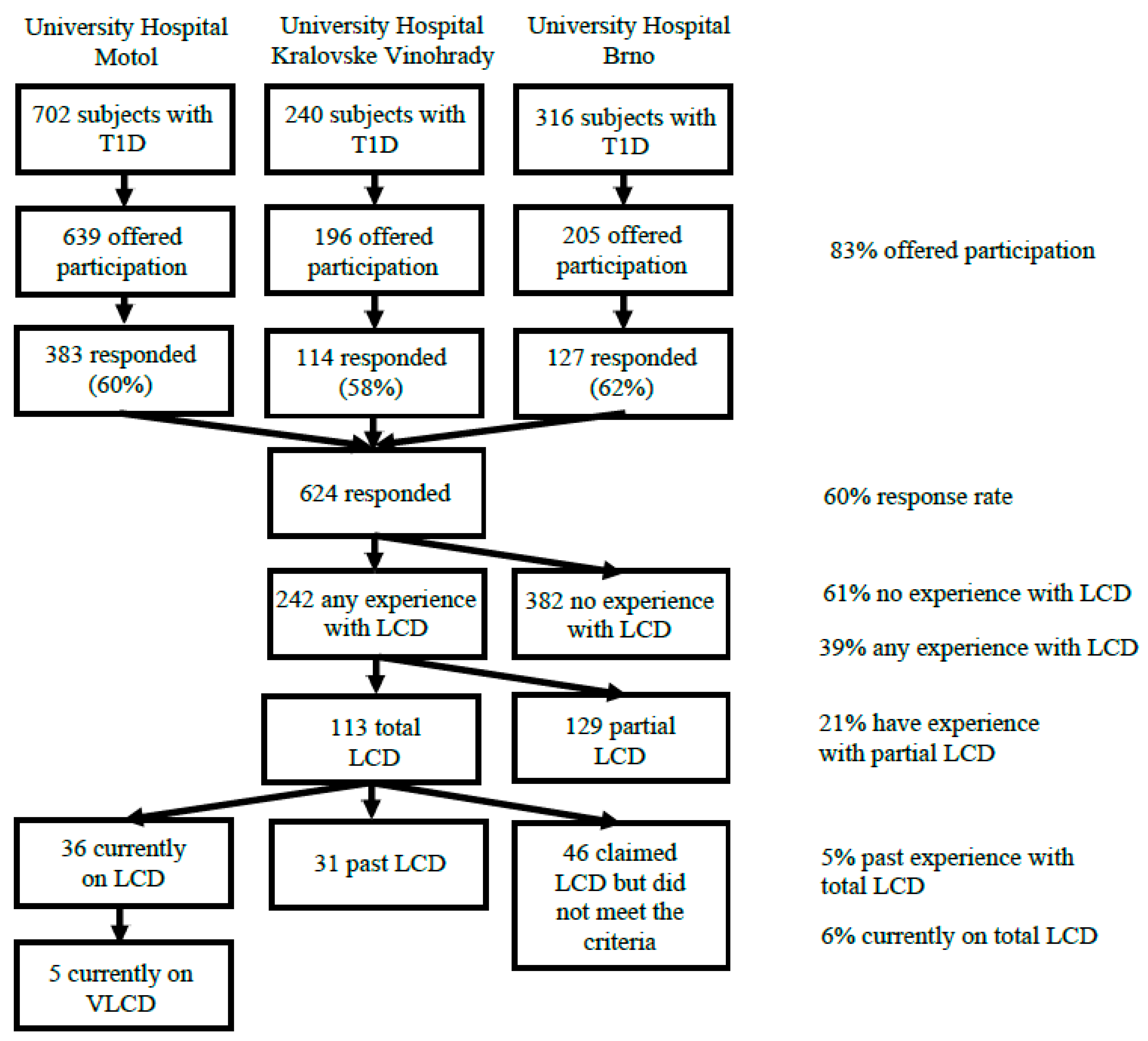
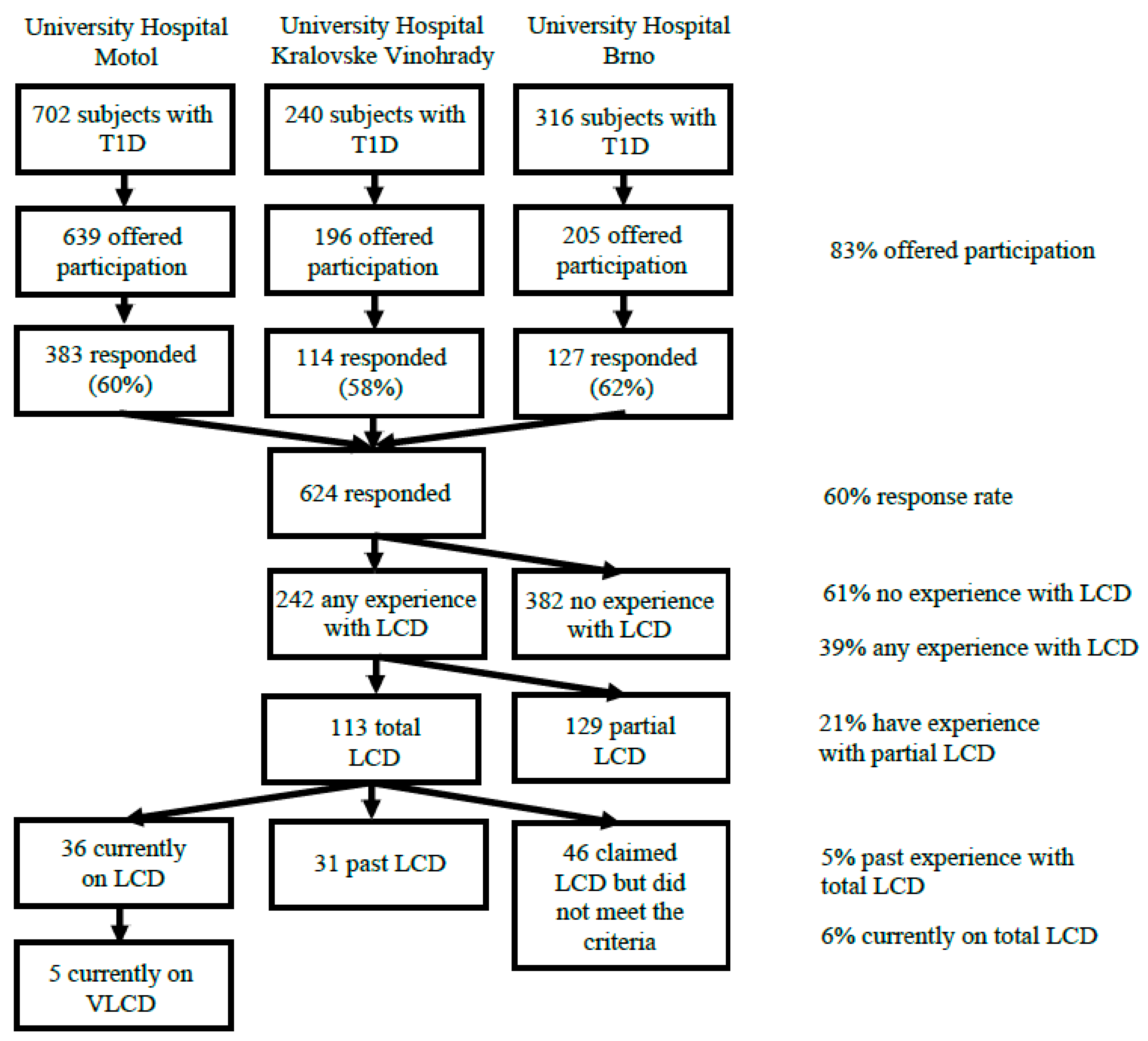
3.1. Frequency of the LCD among the Responders
3.2. Comparison of LCD Subjects to Their Non-LCD Matched Controls
3.3. Questions Specific for the LCD Group
3.4. Comparison of the VLCD Sub-Group to LCD Subjects
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CGM | continuous glucose monitoring |
| CV | glucose coefficient of variation |
| LCD | low-carbohydrate diet |
| SD | standard deviation of glycemia |
| SDS | standard deviation score |
| VLCD | very low-carbohydrate diet |
References
- Foster, N.C.; Beck, R.W.; Miller, K.M.; Clements, M.A.; Rickels, M.R.; DiMeglio, L.A.; Maahs, D.M.; Tamborlane, W.V.; Bergenstal, R.; Smith, E.; et al. State of Type 1 Diabetes Management and Outcomes from the T1D Exchange in 2016–2018. Diabetes Technol. Ther. 2019, 21, 66–72. [Google Scholar] [CrossRef]
- Bekiari, E.; Kitsios, K.; Thabit, H.; Tauschmann, M.; Athanasiadou, E.; Karagiannis, T.; Haidich, A.B.; Hovorka, R.; Tsapas, A. Artificial pancreas treatment for outpatients with type 1 diabetes: Systematic review and meta-analysis. BMJ 2018, 361, k1310. [Google Scholar] [CrossRef] [Green Version]
- Sumnik, Z.; Pavlikova, M.; Pomahacova, R.; Venhacova, P.; Petruzelkova, L.; Skvor, J.; Neumann, D.; Vosahlo, J.; Konecna, P.; Cizek, J.; et al. Use of continuous glucose monitoring and its association with type 1 diabetes control in children over the first 3 years of reimbursement approval: Population data from the CENDA registry. Pediatr. Diabetes 2021, 22, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Boeder, S.; Edelman, S.V. Sodium-glucose co-transporter inhibitors as adjunctive treatment to insulin in type 1 diabetes: A review of randomized controlled trials. Diabetes Obes. Metab. 2019, 21 (Suppl. S2), 62–77. [Google Scholar] [CrossRef] [Green Version]
- Turton, J.L.; Raab, R.; Rooney, K.B. Low-carbohydrate diets for type 1 diabetes mellitus: A systematic review. PLoS ONE 2018, 13, e0194987. [Google Scholar] [CrossRef] [Green Version]
- Neuman, V.; Pruhova, S.; Kulich, M.; Kolouskova, S.; Vosahlo, J.; Romanova, M.; Petruzelkova, L.; Obermannova, B.; Funda, D.P.; Cinek, O.; et al. Gluten-free diet in children with recent-onset type 1 diabetes: A 12-month intervention trial. Diabetes Obes. Metab. 2020, 22, 866–872. [Google Scholar] [CrossRef] [PubMed]
- Smart, C.E.; Annan, F.; Higgins, L.A.; Jelleryd, E.; Lopez, M.; Acerini, C.L. ISPAD Clinical Practice Consensus Guidelines 2018: Nutritional management in children and adolescents with diabetes. Pediatr. Diabetes 2018, 19 (Suppl. S27), 136–154. [Google Scholar] [CrossRef]
- Seckold, R.; Fisher, E.; de Bock, M.; King, B.R.; Smart, C.E. The ups and downs of low-carbohydrate diets in the management of Type 1 diabetes: A review of clinical outcomes. Diabet. Med. 2019, 36, 326–334. [Google Scholar] [CrossRef] [PubMed]
- Sheard, N.F.; Clark, N.G.; Brand-Miller, J.C.; Franz, M.J.; Pi-Sunyer, F.X.; Mayer-Davis, E.; Kulkarni, K.; Geil, P. Dietary carbohydrate (amount and type) in the prevention and management of diabetes: A statement by the american diabetes association. Diabetes Care 2004, 27, 2266–2271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feinman, R.D.; Pogozelski, W.K.; Astrup, A.; Bernstein, R.K.; Fine, E.J.; Westman, E.C.; Accurso, A.; Frassetto, L.; Gower, B.A.; McFarlane, S.I.; et al. Dietary carbohydrate restriction as the first approach in diabetes management: Critical review and evidence base. Nutrition 2015, 31, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Bernstein, R.K. Dr. Bernstein’s Diabetes Solution: The Complete Guide to Achieving Normal Blood Sugars, 4th ed.; Little, Brown & Company: Boston, MA, USA, 2011. [Google Scholar]
- Krebs, J.D.; Parry Strong, A.; Cresswell, P.; Reynolds, A.N.; Hanna, A.; Haeusler, S. A randomised trial of the feasibility of a low carbohydrate diet vs standard carbohydrate counting in adults with type 1 diabetes taking body weight into account. Asia Pac. J. Clin. Nutr. 2016, 25, 78–84. [Google Scholar] [CrossRef]
- Ranjan, A.; Schmidt, S.; Damm-Frydenberg, C.; Holst, J.J.; Madsbad, S.; Norgaard, K. Short-term effects of a low carbohydrate diet on glycaemic variables and cardiovascular risk markers in patients with type 1 diabetes: A randomized open-label crossover trial. Diabetes Obes. Metab. 2017, 19, 1479–1484. [Google Scholar] [CrossRef]
- Schmidt, S.; Christensen, M.B.; Serifovski, N.; Damm-Frydenberg, C.; Jensen, J.B.; Floyel, T.; Storling, J.; Ranjan, A.; Norgaard, K. Low versus high carbohydrate diet in type 1 diabetes: A 12-week randomized open-label crossover study. Diabetes Obes. Metab. 2019, 21, 1680–1688. [Google Scholar] [CrossRef] [PubMed]
- Lennerz, B.S.; Barton, A.; Bernstein, R.K.; Dikeman, R.D.; Diulus, C.; Hallberg, S.; Rhodes, E.T.; Ebbeling, C.B.; Westman, E.C.; Yancy, W.S., Jr.; et al. Management of Type 1 Diabetes with a Very Low-Carbohydrate Diet. Pediatrics 2018, 141, e20173349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayer-Davis, E.J.; Laffel, L.M.; Buse, J.B. Management of Type 1 Diabetes with a Very Low-Carbohydrate Diet: A Word of Caution. Pediatrics 2018, 142, e20181536B. [Google Scholar] [CrossRef] [PubMed]
- de Bock, M.; Lobley, K.; Anderson, D.; Davis, E.; Donaghue, K.; Pappas, M.; Siafarikas, A.; Cho, Y.H.; Jones, T.; Smart, C. Endocrine and metabolic consequences due to restrictive carbohydrate diets in children with type 1 diabetes: An illustrative case series. Pediatr. Diabetes 2018, 19, 129–137. [Google Scholar] [CrossRef] [Green Version]
- Groleau, V.; Schall, J.I.; Stallings, V.A.; Bergqvist, C.A. Long-term impact of the ketogenic diet on growth and resting energy expenditure in children with intractable epilepsy. Dev. Med. Child Neurol. 2014, 56, 898–904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vining, E.P.; Pyzik, P.; McGrogan, J.; Hladky, H.; Anand, A.; Kriegler, S.; Freeman, J.M. Growth of children on the ketogenic diet. Dev. Med. Child Neurol. 2002, 44, 796–802. [Google Scholar] [CrossRef]
- Ranjan, A.; Schmidt, S.; Damm-Frydenberg, C.; Steineck, I.; Clausen, T.R.; Holst, J.J.; Madsbad, S.; Norgaard, K. Low-Carbohydrate Diet Impairs the Effect of Glucagon in the Treatment of Insulin-Induced Mild Hypoglycemia: A Randomized Crossover Study. Diabetes Care 2017, 40, 132–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faith, M.S.; Scanlon, K.S.; Birch, L.L.; Francis, L.A.; Sherry, B. Parent-child feeding strategies and their relationships to child eating and weight status. Obes. Res. 2004, 12, 1711–1722. [Google Scholar] [CrossRef]
- Laffel, L.M.; Connell, A.; Vangsness, L.; Goebel-Fabbri, A.; Mansfield, A.; Anderson, B.J. General quality of life in youth with type 1 diabetes: Relationship to patient management and diabetes-specific family conflict. Diabetes Care 2003, 26, 3067–3073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, S.; Emborg, C.; Molbak, A.G. Mortality in concurrent type 1 diabetes and anorexia nervosa. Diabetes Care 2002, 25, 309–312. [Google Scholar] [CrossRef] [Green Version]
- Goebel-Fabbri, A.E. Diabetes and eating disorders. J. Diabetes Sci. Technol. 2008, 2, 530–532. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. 2. Classification and diagnosis of diabetes. Diabetes Care 2015, 38, S8–S16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association. Nutrition Recommendations and Interventions for Diabetes: A position statement of the American Diabetes Association. Diabetes Care 2007, 31, S61–S78. [Google Scholar] [CrossRef] [Green Version]
- Sumnik, Z.; Venhacova, J.; Skvor, J.; Pomahacova, R.; Konecna, P.; Neumann, D.; Vosahlo, J.; Strnadel, J.; Cizek, J.; Obermannova, B.; et al. Five years of improving diabetes control in Czech children after the establishment of the population-based childhood diabetes register CENDA. Pediatr. Diabetes 2020, 21, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Kobzova, J.; Vignerova, J.; Blaha, P.; Krejcovsky, L.; Riedlova, J. The 6th nationwide anthropological survey of children and adolescents in the Czech Republic in 2001. Cent. Eur. J. Public Health 2004, 12, 126–130. [Google Scholar]
- Flynn, J.T.; Kaelber, D.C.; Baker-Smith, C.M.; Blowey, D.; Carroll, A.E.; Daniels, S.R.; de Ferranti, S.D.; Dionne, J.M.; Falkner, B.; Flinn, S.K.; et al. Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents. Pediatrics 2017, 140, e20171904. [Google Scholar] [CrossRef] [Green Version]
- Battelino, T.; Danne, T.; Bergenstal, R.M.; Amiel, S.A.; Beck, R.; Biester, T.; Bosi, E.; Buckingham, B.A.; Cefalu, W.T.; Close, K.L.; et al. Clinical Targets for Continuous Glucose Monitoring Data Interpretation: Recommendations From the International Consensus on Time in Range. Diabetes Care 2019, 42, 1593–1603. [Google Scholar] [CrossRef] [Green Version]
- Ahola, A.J.; Forsblom, C.; Harjutsalo, V.; Groop, P.H.; FinnDiane Study, G. Dietary carbohydrate intake and cardio-metabolic risk factors in type 1 diabetes. Diabetes Res. Clin. Pract. 2019, 155, 107818. [Google Scholar] [CrossRef] [Green Version]
- Raitakari, O.T.; Porkka, K.V.; Ronnemaa, T.; Knip, M.; Uhari, M.; Akerblom, H.K.; Viikari, J.S. The role of insulin in clustering of serum lipids and blood pressure in children and adolescents. The Cardiovascular Risk in Young Finns Study. Diabetologia 1995, 38, 1042–1050. [Google Scholar] [CrossRef]
- Park, S.K.; Jung, J.Y.; Choi, W.J.; Kim, Y.H.; Kim, H.S.; Ham, W.T.; Shin, H.; Ryoo, J.H. Elevated fasting serum insulin level predicts future development of hypertension. Int. J. Cardiol. 2014, 172, 450–455. [Google Scholar] [CrossRef] [PubMed]
- Leow, Z.Z.X.; Guelfi, K.J.; Davis, E.A.; Jones, T.W.; Fournier, P.A. The glycaemic benefits of a very-low-carbohydrate ketogenic diet in adults with Type 1 diabetes mellitus may be opposed by increased hypoglycaemia risk and dyslipidaemia. Diabet. Med. 2018, 35, 1258–1263. [Google Scholar] [CrossRef] [PubMed]
- Czech Statistical Office. Regional GDP Per Capita for the Regions of the Czech Republic. Available online: https://www.czso.cz/csu/xb/regionalni_hdp (accessed on 25 May 2021).
- Milosavljevic, D.; Mandic, M.L.; Banjari, I. Nutritional knowledge and dietary habits survey in high school population. Coll. Antropol. 2015, 39, 101–107. [Google Scholar] [PubMed]
- Ahola, A.J.; Forsblom, C.; Groop, P.H. Adherence to special diets and its association with meeting the nutrient recommendations in individuals with type 1 diabetes. Acta Diabetol. 2018, 55, 843–851. [Google Scholar] [CrossRef] [Green Version]
- Caccavale, L.J.; Nansel, T.R.; Quick, V.; Lipsky, L.M.; Laffel, L.M.; Mehta, S.N. Associations of disordered eating behavior with the family diabetes environment in adolescents with Type 1 diabetes. J. Dev. Behav. Pediatr. 2015, 36, 8–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Low-Carbohydrate Diet | Non-LCD Diet | p-Value | |
|---|---|---|---|
| Subjects | N = 36 | N = 36 | |
| Demographics | |||
| Age at survey collection (years) | 11.9 (6.1) | 11.8 (5.6) | 0.03 * (0.06) |
| Sex | F = 25 (69.4%) M = 11 (30.6%) | F = 25 (69.4%) M = 11 (30.6%) | - |
| Age at T1D onset (years) | 8.0 (7.1) | 8.4 (5.6) | 0.11 (0.21) |
| T1D duration (years) | 3.2 (2.7) | 3.7 (3.5) | 0.74 (0.87) |
| Anthropometric data | |||
| Body height (cm) | 0.54 (0.57) | ||
| Body height SDS | −0.4 (1.4) | 0.3 (1.2) | 0.35 (0.42) |
| Body weight (kg) | 0.62 (0.66) | ||
| Body weight SDS | 0.5 (1.2) | 0.4 (1.0) | 0.68 (0.72) |
| Body mass index SDS | 0.5 (1.3) | 0.5 (0.9) | 0.62 (0.68) |
| Systolic arterial blood pressure (centile) | 43 (63.0) | 73.5 (40.8) | 0.03 * (0.008 **) |
| Diastolic arterial blood pressure (centile) | 61 (32.5) | 76.5 (39.8) | 0.17 (0.08) |
| LCD data | |||
| Daily carbohydrate intake (g) | 96.5 (42) | 170 (39.8) | <0.001 *** (<0.001 ***) |
| Age at LCD start (years) | 11.2 | - | - |
| LCD duration (years) | 1.1 | - | - |
| LCD type | LCD = 31 (86.1%) VLCD = 5 (13.8%) | - | - |
| Treatment and T1D control | |||
| Treatment type | MDI = 27 (75%) CSII = 9 (25%) | MDI = 27 (75%) CSII = 9 (25%) | - |
| Bolus insulin (units daily) | 10.0 (10.4) | 21.5 (16.8) | <0.001 *** (<0.001 ***) |
| Basal insulin (units daily) | 12.0 (12.7) | 13.5 (11.6) | 0.76 (0.60) |
| Total insulin daily dose (units/kg/day) | 0.6 (0.3) | 0.8 (0.3) | <0.001 *** (<0.001 ***) |
| Last HbA1c (mmol/mol) | 45.0 (9.5) | 49.5 (15.2) | 0.11 (0.26) |
| Last HbA1c (%) | 6.3 (3.0) | 6.7 (3.6) | 0.11 (0.26) |
| Average HbA1c during the last year (mmol/mol) | 47.9 (10.3) | 50.9 (10.6) | 0.05 (0.11) |
| Average HbA1c during the last year (%) | 6.5 (3.1) | 6.8 (3.1) | 0.05 (0.11) |
| CGM data | |||
| CGM use | Yes = 35 (97.2%) No = 1 (2.8%) | Yes = 34 (94.4%) No = 2 (5.6%) | 0.75 (0.75) |
| Time in range 3.9–10.0 mmol/L (%) | 74.0 (14.5) | 66.5 (16.4) | 0.02 * (0.05) |
| Time below 3.9 mmol/L (%) | 8.0 (8.0) | 5.0 (6.0) | 0.05 (0.25) |
| Time below 3.0 mmol/L (%) | 2.0 (3.0) | 1.0 (4.5) | 0.78 (0.89) |
| Time above 10.0 mmol/L (%) | 17.0 (15.9) | 20.0 (9.0) | 0.04 * (0.20) |
| Time above 13.9 mmol/L (%) | 2.0 (4.0) | 3.0 (5.0) | 0.04 * (0.07) |
| Average glycemia (mmol/L) | 7.0 (1.2) | 7.9 (2.1) | 0.02 * (0.05) |
| Standard deviation of glycemia | 2.6 (1.0) | 3.2 (0.8) | 0.03 * (0.07) |
| Coefficient of variation (%) | 37.4 (8.0) | 39.5 (11.8) | 0.60 (0.80) |
| Lipid spectrum | |||
| Total cholesterol (mmol/L) | 4.8 (0.8) | 4.7 (1.4) | 0.55 (0.83) |
| Triglycerides (mmol/L) | 0.9 (0.5) | 0.9 (0.6) | 0.29 (0.08) |
| HDL cholesterol (mmol/L) | 1.5 (0.5) | 1.7 (0.4) | 0.23 (0.46) |
| LDL cholesterol (mmol/L) | 2.6 (0.9) | 2.7 (1.1) | 0.57 (0.98) |
| Question | Answer | N | % |
|---|---|---|---|
| Who initiated carbohydrate restriction? | The child/adolescent with T1D | 18/67 | 26.8 |
| The parent/caregiver | 42/67 | 62.7 | |
| The diabetologist | 6/67 | 8.9 | |
| No answer | 1/67 | 1.5 | |
| Did you consult your intention to reduce carbohydrate intake with your diabetologist? | No | 26/67 | 38.8 |
| Yes, he/she supported us | 18/67 | 26.9 | |
| Yes, he did not support us nor discouraged us but explained the risks and benefits | 17/67 | 25.4 | |
| Yes, he/she discouraged us | 4/67 | 6.0 | |
| What was the reason for carbohydrate restriction? * | Better T1D control | 46/67 | 68.7 |
| Lower insulin dose | 20/67 | 29.9 | |
| Reduction of body weight | 12/67 | 17.9 | |
| Healthy lifestyle | 40/67 | 59.7 | |
| What were your sources of information on carbohydrate restriction? * | Internet | 42/67 | 62.7 |
| Books | 23/67 | 34.3 | |
| Other families with T1D children | 27/67 | 40.3 | |
| Diabetologist | 16/67 | 23.9 | |
| Have you noticed any changes after the initiation of carbohydrate restriction? If so, which? * | No | 9/67 | 13.4 |
| Better T1D control | 32/67 | 47.8 | |
| Lower insulin dose | 40/67 | 59.7 | |
| Body weight reduction | 21/67 | 31.3 | |
| Increased fatigue | 7/67 | 10.4 | |
| More frequent hypoglycemia | 12/67 | 17.9 | |
| School-related conflict | 4/67 | 6.0 | |
| Conflicts with diabetologist | 1/67 | 1.5 | |
| Family conflict | 7/67 | 10.4 | |
| Increased costs for meal preparation | 13/67 | 19.4 | |
| Increased time for meal preparation | 15/67 | 22.4 | |
| Hunger | 1/67 | 1.5 | |
| Did you/your child find low-carbohydrate meals tasty? | Yes, or mostly yes | 29/67 | 43.3 |
| Depending on the meal | 26/67 | 38.8 | |
| No, or mostly no | 11/67 | 16.4 | |
| Did you/your child with T1D have severe hypoglycemia requiring hospitalization during the time you reduced carbohydrates? | Yes | 2/67 | 3.0 |
| No | 65/67 | 97.0 | |
| Did you/your child with T1D have diabetic ketoacidosis requiring hospitalization during the time you reduced carbohydrates? | Yes | 0/67 | 0.0 |
| No | 67/67 | 100.0 | |
| Would you recommend carbohydrate restriction to other children/adolescents with T1D? | Yes | 49/67 | 73.1 |
| No | 18/67 | 26.9 | |
| Who initiated the termination of carbohydrate restriction? † | The child/adolescents with T1D | 14/31 | 45.2 |
| The parent/caregiver | 14/31 | 45.2 | |
| The diabetologist | 3/31 | 9.7 | |
| What were the reasons for the termination of carbohydrate restriction? *,† | It did not fulfill our expectations | 13/31 | 41.9 |
| Non-adherence on the side of child/adolescent with T1D | 16/31 | 51.6 | |
| Side-effects (fatigue, frequent hypoglycemia) | 7/31 | 22.6 | |
| Financial costs | 2/31 | 6.5 | |
| Time consumption | 4/31 | 12.9 | |
| School-related conflict | 2/31 | 6.5 | |
| Family conflict | 1/31 | 3.2 | |
| No answer | 2/31 | 6.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neuman, V.; Plachy, L.; Pruhova, S.; Kolouskova, S.; Petruzelkova, L.; Obermannova, B.; Vyzralkova, J.; Konecna, P.; Vosahlo, J.; Romanova, M.; et al. Low-Carbohydrate Diet among Children with Type 1 Diabetes: A Multi-Center Study. Nutrients 2021, 13, 3903. https://doi.org/10.3390/nu13113903
Neuman V, Plachy L, Pruhova S, Kolouskova S, Petruzelkova L, Obermannova B, Vyzralkova J, Konecna P, Vosahlo J, Romanova M, et al. Low-Carbohydrate Diet among Children with Type 1 Diabetes: A Multi-Center Study. Nutrients. 2021; 13(11):3903. https://doi.org/10.3390/nu13113903
Chicago/Turabian StyleNeuman, Vit, Lukas Plachy, Stepanka Pruhova, Stanislava Kolouskova, Lenka Petruzelkova, Barbora Obermannova, Jana Vyzralkova, Petra Konecna, Jan Vosahlo, Martina Romanova, and et al. 2021. "Low-Carbohydrate Diet among Children with Type 1 Diabetes: A Multi-Center Study" Nutrients 13, no. 11: 3903. https://doi.org/10.3390/nu13113903
APA StyleNeuman, V., Plachy, L., Pruhova, S., Kolouskova, S., Petruzelkova, L., Obermannova, B., Vyzralkova, J., Konecna, P., Vosahlo, J., Romanova, M., Pavlikova, M., & Sumnik, Z. (2021). Low-Carbohydrate Diet among Children with Type 1 Diabetes: A Multi-Center Study. Nutrients, 13(11), 3903. https://doi.org/10.3390/nu13113903