
Effectiveness of Intensive Cardiac Rehabilitation in High-Risk Patients with Cardiovascular Disease in Real-World Practice

 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Cardiometabolic Outcomes
2.3. Psychosocial Outcomes
2.4. Major Adverse Cardiac Events
2.5. Primary and Exploratory Study Outcomes
2.6. Statistical Analysis
3. Results
3.1. Baseline Clinical Characteristics
3.2. Cardiometabolic Outcomes
3.3. Psychosocial Outcomes
3.4. Major Adverse Cardiac Events
3.5. Primary and Exploratory Study Outcomes
3.6. Summary of Main Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. On behalf of the American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics—2020 Update: A Report from the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.S.; Ning, H.; Wilkins, J.T.; Allen, N.; Carnethon, M.; Berry, J.D.; Sweis, R.N.; Lloyd-Jones, D.M. Association of Body Mass Index with Lifetime Risk of Cardiovascular Disease and Compression of Morbidity. JAMA Cardiol. 2018, 3, 280–287. [Google Scholar] [CrossRef]
- Świątkiewicz, I.; Taub, P.R. The usefulness of C-reactive protein for the prediction of post-infarct left ventricular systolic dysfunction and heart failure. Kardiol. Pol. 2018, 76, 821–829. [Google Scholar] [CrossRef] [Green Version]
- Świątkiewicz, I.; Magielski, P.; Kubica, J.; Zadourian, A.; DeMaria, A.N.; Taub, P.R. Enhanced inflammation is a marker for risk of post-infarct ventricular dysfunction and heart failure. Int. J. Mol. Sci. 2020, 21, 807. [Google Scholar] [CrossRef] [Green Version]
- Pogosova, N.; Saner, H.; Pedersen, S.S.; Cupples, M.E.; McGee, H.; Höfer, S.; Doyle, F.; Schmid, J.P.; von Känel, R. Cardiac Rehabilitation Section of the European Association of Cardiovascular Prevention and Rehabilitation of the European Society of Cardiology. Psychosocial aspects in cardiac rehabilitation: From theory to practice. A position paper from the Cardiac Rehabilitation Section of the European Association of Cardiovascular Prevention and Rehabilitation of the European Society of Cardiology. Eur. J. Prev. Cardiol. 2015, 22, 290–306. [Google Scholar]
- Richards, S.H.; Anderson, L.; Jenkinson, C.E.; Whalley, B.; Rees, K.; Davies, P.; Bennett, P.; Liu, Z.; West, R.; Thompson, D.R.; et al. Psychological Interventions for Coronary Heart Disease. Cochrane Database Syst. Rev. 2017, 2017, CD002902. [Google Scholar] [CrossRef] [PubMed]
- Rao, A.; Zecchin, R.; Newton, P.J.; Phillips, J.L.; DiGiacomo, M.; Denniss, A.R.; Hickman, L.D. The prevalence and impact of depression and anxiety in cardiac rehabilitation: A longitudinal cohort study. Eur. J. Prev. Cardiol. 2020, 27, 478–489. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, S.; Hawken, S.; Ounpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef]
- Chow, C.K.; Jolly, S.; Rao-Melacini, P.; Fox, K.A.; Anand, S.S.; Yusuf, S. Association of Diet, Exercise, and Smoking Modification with Risk of Early Cardiovascular Events after Acute Coronary Syndromes. Circulation 2010, 121, 750–758. [Google Scholar] [CrossRef] [Green Version]
- Cholesterol Treatment Trialists’ (CTT) Collaborators. Efficacy and safety of more intensive lowering of LDL cholesterol: A meta-analysis of data from 170000 participants in 26 randomised trials. Lancet 2010, 376, 1670–1681. [Google Scholar] [CrossRef] [Green Version]
- Smith, S.C.; Benjamin, E.J.; Bonow, R.O.; Braun, L.T.; Creager, M.A.; Franklin, B.A.; Gibbons, R.J.; Grundy, S.M.; Hiratzka, L.F.; Jones, D.W.; et al. AHA/ACCF Secondary Prevention and Risk Reduction Therapy for Patients with Coronary and Other Atherosclerotic Vascular Disease: 2011 Update. Circulation 2011, 124, 2458–2473. [Google Scholar] [CrossRef] [Green Version]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; de Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 Guideline on the Management of Blood Cholesterol. A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 139, e1082–e1143. [Google Scholar] [PubMed]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Corrà, U.; Benzer, W.; Bjarnason-Wehrens, B.; Dendale, P.; Gaita, D.; McGee, H.; Mendes, M.; Niebauer, J.; Zwisler, A.D.; et al. Secondary prevention through cardiac rehabilitation: From knowledge to implementation. A position paper from the Cardiac Rehabilitation Section of the European Association of Cardiovascular Prevention and Rehabilitation. Eur. J. Cardiovasc. Prev. Rehabil. 2010, 17, 1–17. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [PubMed] [Green Version]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef] [PubMed]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef]
- Ambrosetti, M.; Abreu, A.; Corrà, U.; Davos, C.H.; Hansen, D.; Frederix, I.; Iliou, M.C.; Pedretti, R.F.; Schmid, J.P.; Vigorito, C.; et al. Secondary prevention through comprehensive cardiovascular rehabilitation: From knowledge to implementation. 2020 update. A position paper from the Secondary Prevention and Rehabilitation Section of the European Association of Preventive Cardiology. Eur. J. Prev. Cardiol. 2021, 28, 460–495. [Google Scholar] [CrossRef] [Green Version]
- Lo, H.C.; Pazargadi, A.; Świątkiewicz, I.; Taub, P. Secondary Prevention and Cardiac Rehabilitation. In ASPC Manual of Preventive Cardiology, 2nd ed.; Wong, N.D., Amsterdam, E.A., Toth, P.P., Eds.; Springer Nature: Cham, Switzerland, 2021; pp. 673–703. [Google Scholar]
- Kachur, S.; Chongthammakun, V.; Lavie, C.J.; De Schutter, A.; Arena, R.; Milani, R.V.; Franklin, B.A. Impact of cardiac rehabilitation and exercise training programs in coronary heart disease. Prog. Cardiovasc. Dis. 2017, 60, 103–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rauch, B.; Davos, C.H.; Doherty, P.; Saure, D.; Metzendorf, M.I.; Salzwedel, A.; Völler, H.; Jensen, K.; Schmid, J.P.; ‘Cardiac Rehabilitation Section’, European Association of Preventive Cardiology (EAPC), in cooperation with the Institute of Medical Biometry and Informatics (IMBI), Department of Medical Biometry, University of Heidelberg, and the Cochrane Metabolic and Endocrine Disorders Group, Institute of General Practice, Heinrich-Heine University, Düsseldorf, Germany. The prognostic effect of cardiac rehabilitation in the era of acute revascularisation and statin therapy: A systematic review and meta-analysis of randomized and non-randomized studies—The Cardiac Rehabilitation Outcome Study (CROS). Eur. J. Prev. Cardiol. 2016, 23, 1914–1939. [Google Scholar] [CrossRef] [Green Version]
- Silberman, A.; Banthia, R.; Estay, I.S.; Kemp, C.; Studley, J.; Hareras, D.; Ornish, D. The Effectiveness and Efficacy of an Intensive Cardiac Rehabilitation Program in 24 Sites. Am. J. Health Prom. 2010, 24, 260–266. [Google Scholar] [CrossRef]
- Benzer, W.; Rauch, B.; Schmid, J.P.; Zwisler, A.D.; Dendale, P.; Davos, C.H.; Kouidi, E.; Simon, A.; Abreu, A.; Pogosova, N.; et al. Exercise-based cardiac rehabilitation in twelve European countries results of the European cardiac rehabilitation registry. Int. J. Cardiol. 2017, 228, 58–67. [Google Scholar] [CrossRef]
- Anderson, L.; Oldridge, N.; Thompson, D.R.; Zwisler, A.D.; Rees, K.; Martin, N.; Taylor, R.S. Exercise-Based Cardiac Rehabilitation for Coronary Heart Disease: Cochrane Systematic Review and Meta-Analysis. J. Am. Coll. Cardiol. 2016, 6, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Halewijn, G.; Deckers, J.; Tay, H.Y. Lessons from Contemporary Trials of Cardiovascular Prevention and Rehabilitation: A Systematic Review and Meta-Analysis. Int. J. Cardiol. 2017, 232, 294–303. [Google Scholar] [CrossRef] [Green Version]
- Long, L.; Anderson, L.; He, J.; Gandhi, M.; Dewhirst, A.; Bridges, C.; Taylor, R. Exercise-based cardiac rehabilitation for stable angina: Systematic review and meta-analysis. Open Heart 2019, 6, e000989. [Google Scholar] [CrossRef] [PubMed]
- Blumenthal, J.A.; Babyak, M.A.; O’Connor, C. Effects of Exercise Training on Depressive Symptoms in Patients with Chronic Heart Failure. The HF-ACTION Randomized Trial. JAMA 2012, 308, 465–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Long, L.; Mordi, I.R.; Bridges, C.; Sagar, V.A.; Davies, E.J.; Coats, A.J.; Dalal, H.; Rees, K.; Singh, S.J.; Taylor, R.S. Exercise-based cardiac rehabilitation for adults with heart failure. Cochrane Database Syst. Rev. 2019, 1, CD003331. [Google Scholar] [CrossRef] [Green Version]
- Janssen, V.; De Gucht, V.; Dusseldorp, E.; Waure, S.M. Lifestyle Modification Programmes for Patients with Coronary Heart Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Eur. J. Prev. Cardiol. 2013, 20, 620–640. [Google Scholar] [CrossRef]
- Blumenthal, J.A.; Sherwood, A.; Smith, P.J. Enhancing Cardiac Rehabilitation with Stress Management Training: A Randomized Clinical Efficacy Trial. Circulation 2016, 133, 1341–1350. [Google Scholar] [CrossRef] [Green Version]
- Ornish, D.; Scherwitz, L.W.; Billings, J.H.; Brown, S.E.; Gould, K.L.; Merritt, T.A.; Sparler, S.; Armstrong, W.T.; Ports, T.A.; Kirkeeide, R.L.; et al. Intensive lifestyle changes for reversal of coronary heart disease. JAMA 1998, 280, 2001–2007. [Google Scholar] [CrossRef] [PubMed]
- Giannuzzi, P.; Temporelli, P.L.; Marchioli, R.; Maggioni, A.P.; Balestroni, G.; Ceci, V.; Chieffo, C.; Gattone, M.; Griffo, R.; Schweiger, C.; et al. Global secondary prevention strategies to limit event recurrence after myocardial infarction: Results of the GOSPEL study, a multicenter, randomized controlled trial from the Italian Cardiac Rehabilitation Network. Arch. Intern. Med. 2008, 168, 2194–2204. [Google Scholar] [CrossRef] [PubMed]
- West, R.R.; Jones, D.A.; Henderson, A.H. Rehabilitation after myocardial infarction trial (RAMIT): Multi-centre randomised controlled trial of comprehensive cardiac rehabilitation in patients following acute myocardial infarction. Heart 2012, 98, 637–644. [Google Scholar] [CrossRef] [Green Version]
- Zwisler, A.D.; Soja, A.M.; Rasmussen, S.; Frederiksen, M.; Abedini, S.; Appel, J.; Rasmussen, H.; Gluud, C.; Iversen, L.; Sigurd, B.; et al. Hospital-based comprehensive cardiac rehabilitation versus usual care among patients with congestive heart failure, ischemic heart disease, or high risk of ischemic heart disease: 12-month results of a randomized clinical trial. Am. Heart J. 2008, 155, 1106–1113. [Google Scholar] [CrossRef]
- Reich, B.; Benzer, W.; Harpf, H.; Hofmann, P.; Mayr, K.; Ocenasek, H.; Podolsky, A.; Pokan, R.; Porodko, M.; Puelacher, C.; et al. Efficacy of extended, comprehensive outpatient cardiac rehabilitation on cardiovascular risk factors: A nationwide registry. Eur. J. Prev. Cardiol. 2020, 27, 1026–1033. [Google Scholar] [CrossRef]
- Kränkel, N.; Bahls, M.; Van Craenenbroeck, E.M.; Adams, V.; Serratosa, L.; Solberg, E.E.; Hansen, D.; Dörr, M.; Kemps, H. Exercise training to reduce cardiovascular risk in patients with metabolic syndrome and type 2 diabetes mellitus: How does it work? Eur. J. Prev. Cardiol. 2019, 26, 701–708. [Google Scholar] [CrossRef]
- Kemps, H.; Kränkel, N.; Dörr, M.; Moholdt, T.; Wilhelm, M.; Paneni, F.; Serratosa, L.; Solberg, E.E.; Hansen, D.; Halle, M.; et al. Exercise training for patients with type 2 diabetes and cardiovascular disease: What to pursue and how to do it. A Position Paper of the European Association of Preventive Cardiology (EAPC). Eur. J. Prev. Cardiol. 2019, 26, 709–727. [Google Scholar] [CrossRef]
- Świątkiewicz, I.; Woźniak, A.; Taub, P.R. Time-Restricted Eating and Metabolic Syndrome: Current Status and Future Perspectives. Nutrients 2021, 13, 221. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, R.T.; Liss, D.T.; Finch, E.A.; Schmidt, K.K.; Hays, L.M.; Marrero, D.G.; Saha, C.A. Randomized Comparative Effectiveness Trial for Preventing Type 2 Diabetes. Am. J. Public Health 2015, 105, 2328–2334. [Google Scholar] [CrossRef]
- Jacobson, T.A.; Maki, K.C.; Orringer, C.E.; Jones, P.H.; Kris-Etherton, P.; Sikand, G.; La Forge, R.; Daniels, S.R.; Wilson, D.P.; Morris, P.B. NLA Expert Panel. National Lipid association recommendations for patient-centered management of dyslipidemia: Part 2. J. Clin. Lipidol. 2015, 9, S1–S122.e1. [Google Scholar] [CrossRef] [Green Version]
- Zomer, E.; Gurusamy, K.; Leach, R.; Trimmer, C.; Lobstein, T.; Morris, S.; James, W.P.; Finer, N. Interventions that cause weight loss and the impact on cardiovascular risk factors: A systematic review and meta-analysis. Obes. Rev. 2016, 17, 1001–1011. [Google Scholar] [CrossRef]
- Rutledge, T.; Redwine, L.S.; Linke, S.E.; Mills, P.J. A Meta-Analysis of Mental Health Treatments and Cardiac Rehabilitation for Improving Clinical Outcomes and Depression among Patients with Coronary Heart Disease. Psychosom. Med. 2013, 75, 335–349. [Google Scholar] [CrossRef] [PubMed]
- Shridhar, K.; Dhillon, P.K.; Bowen, L.; Kinra, S.; Bharathi, A.V.; Prabhakaran, D.; Reddy, K.S.; Ebrahim, S. Indian Migration Study Group. The association between a vegetarian diet and cardiovascular disease (CVD) risk factors in India: The Indian Migration Study. PLoS ONE 2014, 9, e110586. [Google Scholar] [CrossRef]
- Yokoyama, Y.; Nishimura, K.; Barnard, N.D.; Misa, T.; Makoto, W.; Akira, S.; Tomonori, O.; Yoshihiro, M. Vegetarian Diets and Blood Pressure: A Meta-analysis. JAMA Intern. Med. 2014, 174, 577–587. [Google Scholar] [CrossRef]
- Satija, A.; Bhupathiraju, S.N.; Spiegelman, D.; Chiuve, S.E.; Manson, J.E.; Willett, W.; Rexrode, K.M.; Rimm, E.B.; Hu, F.B. Healthful and Unhealthful Plant-Based Diets and the Risk of Coronary Heart Disease in U.S. Adults. J. Am. Coll. Cardiol. 2017, 70, 411–422. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Larson, N.; Steffen, L.M.; Schreiner, P.J.; Gallaher, D.D.; Duprez, D.A.; Shikany, J.M.; Rana, J.S.; Jacobs, D.R., Jr. Plant-Centered Diet and Risk of Incident Cardiovascular Disease during Young to Middle Adulthood. J. Am. Heart Assoc. 2021, 17, e020718. [Google Scholar]
- Whelton, P.K.; He, J.; Appel, L.J.; Cutler, J.A.; Havas, S.; Kotchen, T.A.; Roccella, E.J.; Stout, R.; Vallbona, C.; Winston, M.C.; et al. Primary prevention of hypertension: Clinical and public health advisory from The National High Blood Pressure Education Program. JAMA 2002, 288, 1882–1888. [Google Scholar] [CrossRef]
- Pérez-Martínez, P.; Mikhailidis, D.P.; Athyros, V.G.; Bullo, M.; Couture, P.; Covas, M.I.; de Koning, L.; Delgado-Lista, J.; Díaz-López, A.; Drevon, C.A.; et al. Lifestyle recommendations for the prevention and management of metabolic syndrome: An international panel recommendation. Nutr. Rev. 2017, 75, 307–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heymsfield, S.B.; Harp, J.B.; Reitman, M.L.; Beetsch, J.W.; Schoeller, D.A.; Erondu, N.; Pietrobelli, A. Why do obese patients not lose more weight when treated with low-calorie diets? A mechanistic perspective. Am. J. Clin. Nutr. 2007, 85, 346–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, L.; Cheng, Z.; Zhang, Y.; Li, Y.; Mei, D. The impact of medication adherence on clinical outcomes of coronary artery disease: A meta-analysis. Eur. J. Prev. Cardiol. 2017, 24, 962–970. [Google Scholar] [CrossRef] [PubMed]
- Freeman, A.M.; Taub, P.R.; Lo, H.C.; Ornish, D. Intensive Cardiac Rehabilitation: An Underutilized Resource. Curr. Cardiol. Rep. 2019, 21, 19. [Google Scholar] [CrossRef]
- Ridker, P.M.; Everett, B.M.; Thuren, T.; MacFadyen, J.G.; Chang, W.H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig, W.; Anker, S.D.; et al. Antiinflammatory therapy with canakinumab for atherosclerotic disease. N. Engl. J. Med. 2017, 377, 1119–1131. [Google Scholar] [CrossRef]
- Everett, B.M.; Cornel, J.H.; Lainscak, M.; Anker, S.D.; Abbate, A.; Thuren, T.; Libby, P.; Glynn, R.J.; Ridker, P.M. Anti-Inflammatory Therapy With Canakinumab for the Prevention of Hospitalization for Heart Failure. Circulation 2019, 139, 1289–1299. [Google Scholar] [CrossRef] [PubMed]
- Świątkiewicz, I.; Magielski, P.; Kubica, J. C-Reactive Protein as a Risk Marker for Post-Infarct Heart Failure over a Multi-Year Period. Int. J. Mol. Sci. 2021, 22, 3169. [Google Scholar] [CrossRef] [PubMed]
- Szewczyk-Golec, K.; Woźniak, A.; Reiter, R.A. Inter-relationship of the chronobiotic, melatonin, with leptin and adiponectin: Implications for obesity. J. Pineal Res. 2015, 59, 277–291. [Google Scholar] [CrossRef]
- Szewczyk-Golec, K.; Rajewski, P.; Gackowski, M.; Mila-Kierzenkowska, C.; Wesołowski, R.; Sutkowy, P.; Pawłowska, M.; Wozniak, A. Melatonin supplementation lowers oxidative stress and regulates adipokines in obese patients on a calorie-restricted diet. Oxid. Med. Cell Longev. 2017, 2017, 8494107. [Google Scholar] [CrossRef]
- Kupczyk, D.; Bilski, R.; Sokołowski, K.; Pawłowska, M.; Woźniak, A.; Szewczyk-Golec, K. Paraoxonase 1: The Lectin-Like Oxidized LDL Receptor Type I and Oxidative Stress in the Blood of Men with Type II Obesity. Dis. Markers 2019, 2019, 6178017. [Google Scholar] [CrossRef] [Green Version]
- Świątkiewicz, I.; Mila-Kierzenkowska, C.; Woźniak, A.; Szewczyk-Golec, K.; Nuszkiewicz, J.; Wróblewska, J.; Rajewski, P.; Eussen, S.J.P.M.; Færch, K.; Manoogian, E.N.C.; et al. Pilot Clinical Trial of Time-Restricted Eating in Patients with Metabolic Syndrome. Nutrients 2021, 13, 346. [Google Scholar] [CrossRef]
- Piotrowicz, E.; Pencina, M.J.; Opolski, G.; Zareba, W.; Banach, M.; Kowalik, I.; Orzechowski, P.; Szalewska, D.; Pluta, S.; Glówczynska, R.; et al. Effects of a 9-Week Hybrid Comprehensive Telerehabilitation Program on Long-term Outcomes in Patients with Heart Failure: The Telerehabilitation in Heart Failure Patients (TELEREH-HF) Randomized Clinical Trial. JAMA Cardiol. 2020, 5, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.J.; Beatty, A.L.; Beckie, T.M.; Brewer, L.C.; Brown, T.M.; Forman, D.E.; Franklin, B.A.; Keteyian, S.J.; Kitzman, D.W.; Regensteiner, J.G.; et al. Home-Based Cardiac Rehabilitation: A Scientific Statement from the American Association of Cardiovascular and Pulmonary Rehabilitation, the American Heart Association, and the American College of Cardiology. J. Am. Coll. Cardiol. 2019, 74, 133–153. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Variable | ICR Group (n = 101) | SCR Group (n = 213) | p-Value between Groups |
|---|---|---|---|
| Age (years) | 66.0 (±9.0) | 65.0 (±15.0) | 0.731 |
| Gender (male/female) n (%) | 69/32 (68.3/31.7) | 156/57 (73.2/26.8) | 0.366 |
| Race (white/other) n (%) | 77/24 (76.2/23.8) | 154/59 (72.3/27.7) | 0.460 |
| BMI ≥25/30 kg/m2 n (%) | 71 (76.3)/24 (24.7) | 142 (73.6)/54 (27.3) | 0.615 |
| Coronary artery disease n (%) | 96 (95.0) | 187 (87.8) | 0.044 |
| STEMI n (%) | 15 (14.9) | 31 (14.6) | 0.944 |
| NSTEMI n (%) | 11 (10.9) | 43 (20.2) | 0.041 |
| PCI n (%) | 66 (65.3) | 107 (50.5) | 0.013 |
| CABG n (%) | 30 (29.7) | 59 (27.7) | 0.713 |
| Angina at the enrollment n (%) | 23 (22.8) | 71 (33.3) | 0.056 |
| Ischemic stroke n (%) | 2 (2.0) | 17 (8.0) | 0.037 |
| PAD n (%) | 8 (7.9) | 19 (8.9) | 0.768 |
| Hypertension n (%) | 67 (66.3) | 160 (75.1) | 0.104 |
| Heart valve replacement n (%) | 5 (5.0) | 33 (15.6) | 0.007 |
| Type 2 diabetes mellitus n (%) | 24 (23.8) | 62 (29.1) | 0.321 |
| Heart transplant n (%) | 3 (3.0) | 10 (4.7) | 0.474 |
| Chronic symptomatic heart failure n (%) | 22 (21.8) | 68 (31.9) | 0.063 |
| Chronic kidney disease n (%) | 26 (25.7) | 74 (34.7) | 0.110 |
| Atrial fibrillation n (%) | 35 (30.4) | 19 (18.8) | 0.002 |
| Hyperlipidemia n (%) | 93 (92.1) | 168 (78.9) | 0.004 |
| Smoking current/former n (%) | 0/37 (0/36.6) | 12/90 (5.6/42.3) | 0.061 |
| Family history of premature ASCVD n (%) | 31 (30.7) | 88 (41.3) | 0.07 |
| Regular aerobic exercise n (%) | 42 (41.6) | 123 (57.7) | 0.024 |
| ASA n (%) | 94 (93.1) | 183 (85.9) | 0.066 |
| Beta blocker n (%) | 78 (77.2) | 146 (68.5) | 0.112 |
| ACEI n (%) | 28 (27.7) | 65 (30.5) | 0.613 |
| ARB n (%) | 28 (27.7) | 43 (20.3) | 0.142 |
| Statin n (%) | 91 (90.1) | 175 (82.2) | 0.068 |
| Diuretic n (%) | 28 (27.7) | 82 (38.5) | 0.062 |
| Antidepressant agent n (%) | 15 (14.9) | 82 (38.7) | <0.0001 |
| Hemoglobin (g/dL) | 13.3 (±1.8) | 12.5 (±2.1) | 0.001 |
| Creatinine (mg/dL) | 1.15 (±1.0) | 1.38 (±1.43) | 0.155 |
| Glomerular filtration rate (mL/min) | 55.3 (±9.9) | 52.8 (±13.4) | 0.091 |
| Leukocyte count (103/µL) | 7.0 (±1.9) | 8.3 (±8.7) | 0.164 |
| Fasting plasma glucose (mg/dL) | 105.5 (±23.2) | 111.5 (±33.2) | 0.065 |
| Lipoprotein (a) (mg/dL) | 47.3 (±61.5) | 45.3 (±53.0) | 0.833 |
| TSH (mIU/L) | 2.3 (±1.5) | 2.6 (±2.1) | 0.276 |
| LVEF (%) | 58.0 (±13.0) | 55.0 (±16.0) | 0.078 |
| Variable | ICR Group (n = 101) | SCR Group (n = 213) | p-Value between Groups | ||||
|---|---|---|---|---|---|---|---|
| Initial | Discharge | p-Value | Initial | Discharge | p-Value | ||
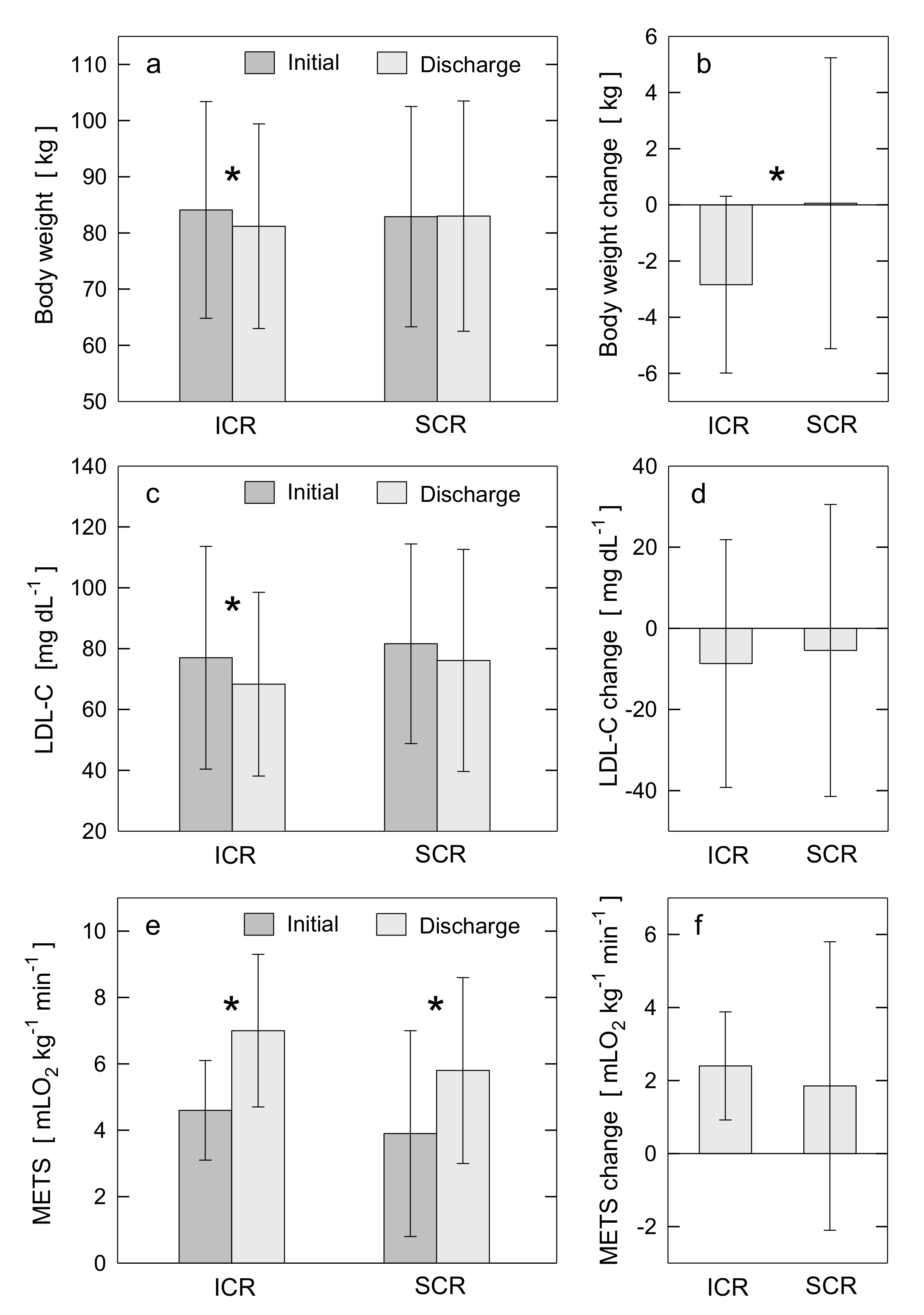
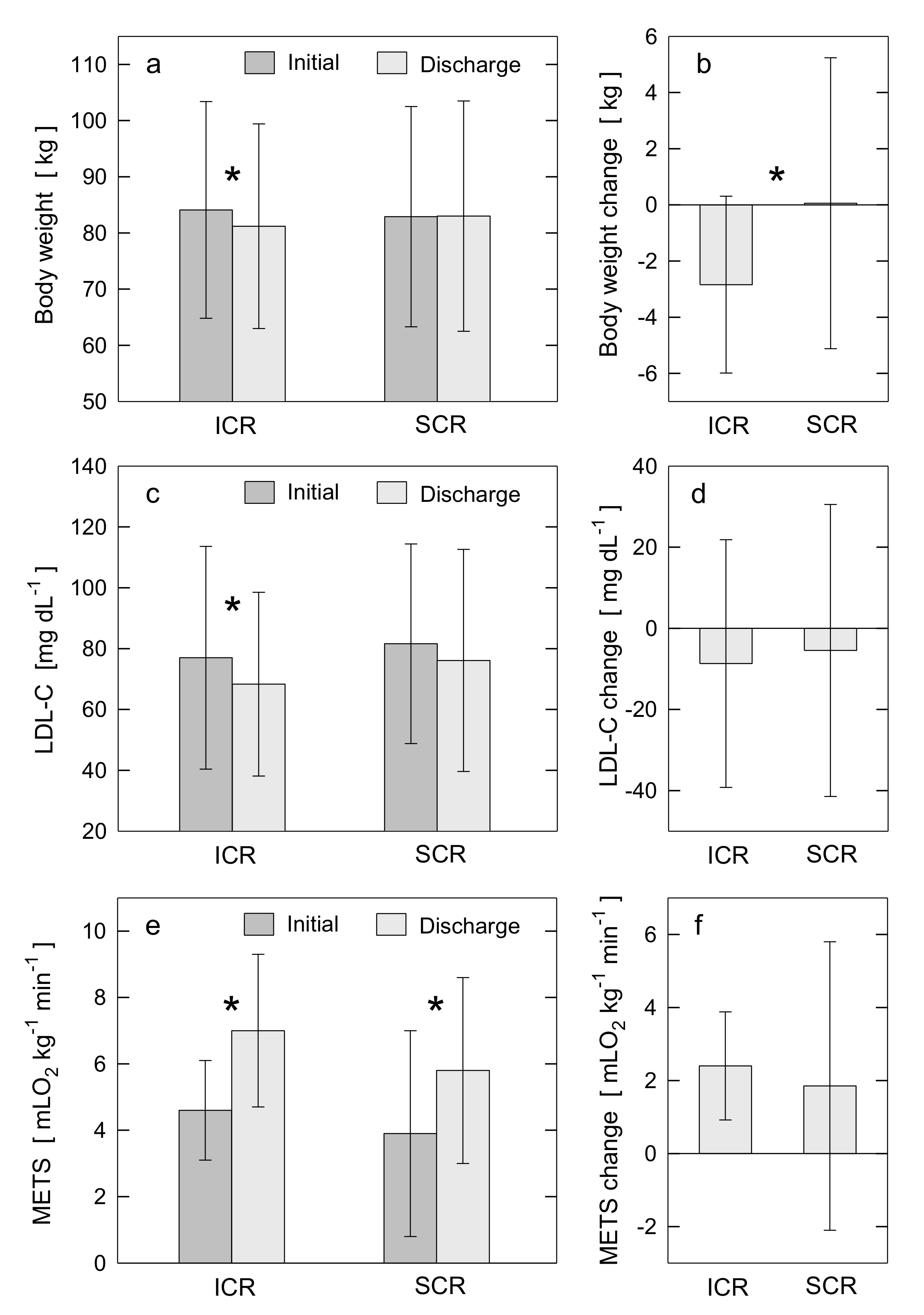
| Body weight (kg) | 84.1 (±19.3) | 81.2 (±18.2) | <0.0001 | 82.9 (±19.6) | 83.0 (±20.5) | 0.878 | <0.0001 |
| BMI (kg/m2) | 28.2 (±6.2) | 27.2 (±5.8) | <0.0001 | 27.9 (±5.4) | 27.8 (±5.3) | 0.518 | <0.0001 |
| Body fat (%) | 31.7 (±9.6) | 29.8 (±9.8) | <0.0001 | 32.0 (±8.5) | 31.0 (±8.7) | 0.002 | 0.049 |
| Visceral fat rating | 12.9 (±4.9) | 11.4 (±4.8) | <0.0001 | 12.5 (±5.1) | 11.6 (±4.5) | 0.001 | 0.163 |
| Muscle mass (%) | 67.5 (14.2) | 67.5 (±13.3) | 0.930 | 79.0 (±26.8) | 72.7 (±21.1) | 0.005 | 0.005 |
| Waist circumference (cm) | 99.6 (±15) | 96.3 (±13.7) | <0.0001 | 100.6 (±16) | 99.3 (±15.5) | 0.002 | 0.002 |
| Total cholesterol (mg/dL) | 151.6 (±44.8) | 141.2 (±36.5) | 0.005 | 156.0 (±43.2) | 149.0 (±44.5) | 0.098 | 0.552 |
| LDL-C (mg/dL) | 77.0 (±36.6) | 68.3 (±30.2) | 0.006 | 81.6 (±32.8) | 76.1 (±36.5) | 0.112 | 0.488 |
| LDL particle number (nmol/L) | 1023.8 (±379.4) | 957.3 (±362.5) | 0.026 | 1074.3 (±561.8) | 1095.3 (±277.3) | 0.777 | 0.504 |
| Non-HDL-C (mg/dL) | 104.4 (±41.8) | 90.4 (±37.9) | 0.001 | 105.9 (±38.8) | 99.5 (±41.1) | 0.113 | 0.200 |
| HDL-C (mg/dL) | 48.5 (±14.1) | 48.2 (±16.3) | 0.718 | 49.3 (±16.5) | 49.7 (±16.3) | 0.637 | 0.558 |
| Triglycerides (mg/dL) | 131.1 (±59.5) | 122.5 (±56.6) | 0.089 | 125.3 (±66.5) | 125.8 (±78.4) | 0.937 | 0.265 |
| Glycated hemoglobin (%) | 5.8 (±0.9) | 5.7 (±0.7) | 0.025 | 6.4 (±1.3) | 6.4 (±1.0) | 0.930 | 0.357 |
| Peak exercise capacity (METs) | 4.6 (±1.5) | 7.0 (±2.3) | <0.0001 | 3.9 (±3.1) | 5.8 (±2.8) | <0.0001 | 0.177 |
| Systolic BP (mmHg) | 122.0 (±16.8) | 117.0 (±16.9) | 0.001 | 119.0 (±17.4) | 116.0 (±16.4) | 0.055 | 0.220 |
| Diastolic BP (mmHg) | 71.0 (±9.6) | 63.0 (±9.5) | <0.0001 | 65.0 (±10.4) | 63.0 (±10.2) | 0.048 | <0.0001 |
| Heart rate (bpm) | 69.0 (±11.0)) | 68.0 (±11.6) | 0.752 | 72.0 (±13.6) | 74.0 (±13.2) | 0.005 | 0.043 |
| CES-D score (-) | 10.4 (±10.3) | 5.4 (±5.7) | <0.0001 | - | - | - | |
| SF-36 physical health score (-) | 44.3 (±9.7) | 51.2 (±7.8) | <0.0001 | - | - | - | |
| SF-36 mental health score (-) | 50.1 (±10.0) | 55.6 (±5.4) | <0.0001 | - | - | - | |
| PHQ-9 score (-) | - | - | - | 5.0 (±4.5) | 3.3 (±3.8) | 0.001 | |
| QOLS score (-) | - | - | - | 22.6 (±5.1) | 24.7 (±3.9) | <0.0001 | |
| Dietary cholesterol intake (mg/day) | 248.0 (±230.6) | 55.3 (±67.1) | <0.0001 | 158.5 (±43.3) | 130.6 (±44.8) | 0.009 | 0.002 |
| Dietary fat intake (g/day) | 71.9 (±41.4) | 32.0 (±20) | <0.0001 | 64.1 (±26.5) | - | - | |
| Dietary fiber intake (g/day) | 21.7 (±10.3) | 30.6 (±11.4) | <0.0001 | 24.1 (±1.6) | - | - | |
| Major Adverse Cardiac Event | ICR Group (n = 101) | SCR Group (n = 213) | p-Value between Groups |
|---|---|---|---|
| All-cause death n (%) Cardiovascular death n (%) | 1 (1.0) 1 (1.0) | 5 (2.3) 3 (1.4) | 0.412 0.757 |
| Non-fatal myocardial infarction n (%) | 1 (1.0) | 4 (1.9) | 0.557 |
| Hospitalization for unstable angina n (%) | 5 (5.0) | 10 (4.7) | 0.921 |
| PCI n (%) | 4 (4.0) | 7 (3.3) | 0.762 |
| CABG n (%) | 0 (0.0) | 1 (0.5) | 0.490 |
| Peripheral artery revascularization n (%) | 0 (0.0) | 3 (1.4) | 0.231 |
| Ischemic stroke n (%) | 0 (0.0) | 0 (0.0) | |
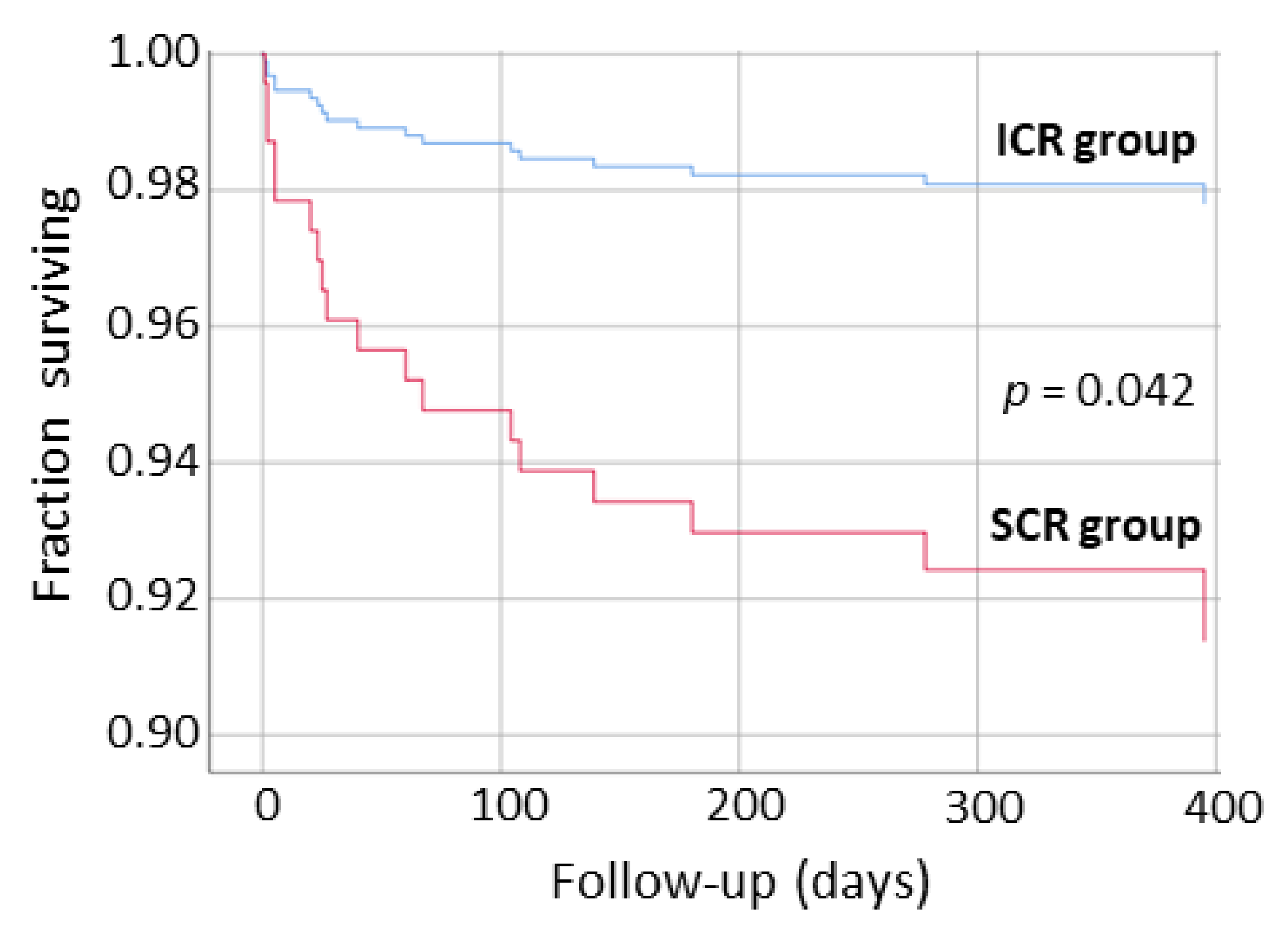
| Hospitalization for heart failure n (%) | 2 (2.0) | 16 (7.5) | 0.049 |
| Heart valve repair or replacement n (%) | 1 (1.0) | 1 (0.5) | 0.588 |
| Heart transplant or LVAD implantation n (%) | 0 (0.0) | 1 (0.5) | 0.490 |
| Total MACE n (%) | 11 (10.9%) | 37 (17.4%) | 0.136 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Świątkiewicz, I.; Di Somma, S.; De Fazio, L.; Mazzilli, V.; Taub, P.R. Effectiveness of Intensive Cardiac Rehabilitation in High-Risk Patients with Cardiovascular Disease in Real-World Practice. Nutrients 2021, 13, 3883. https://doi.org/10.3390/nu13113883
Świątkiewicz I, Di Somma S, De Fazio L, Mazzilli V, Taub PR. Effectiveness of Intensive Cardiac Rehabilitation in High-Risk Patients with Cardiovascular Disease in Real-World Practice. Nutrients. 2021; 13(11):3883. https://doi.org/10.3390/nu13113883
Chicago/Turabian StyleŚwiątkiewicz, Iwona, Salvatore Di Somma, Ludovica De Fazio, Valerio Mazzilli, and Pam R. Taub. 2021. "Effectiveness of Intensive Cardiac Rehabilitation in High-Risk Patients with Cardiovascular Disease in Real-World Practice" Nutrients 13, no. 11: 3883. https://doi.org/10.3390/nu13113883
APA StyleŚwiątkiewicz, I., Di Somma, S., De Fazio, L., Mazzilli, V., & Taub, P. R. (2021). Effectiveness of Intensive Cardiac Rehabilitation in High-Risk Patients with Cardiovascular Disease in Real-World Practice. Nutrients, 13(11), 3883. https://doi.org/10.3390/nu13113883