
Development, Validation, and Reproducibility of Food Group-Based Frequency Questionnaires for Clinical Use in Brazil: A Pre-Hypertension and Hypertension Diet Assessment

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
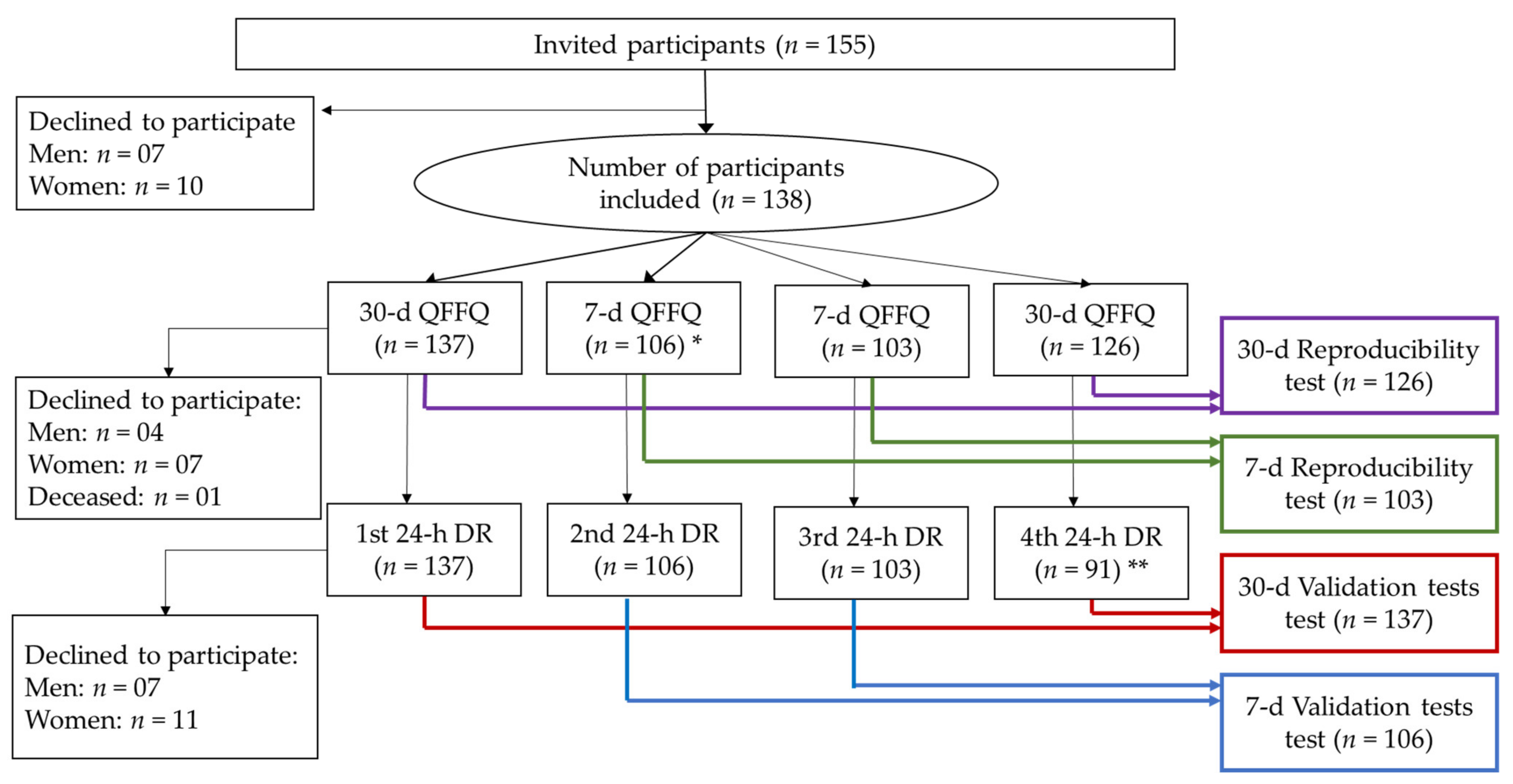
2.1. Study Participants
2.2. Food Group-Based Food Frequency Questionnaire Design (FG-FFQ)
2.3. Diet Data Collection and Assessment
2.4. Non-Dietary Data Collection
2.5. Quality Control and Pilot Study
- (1)
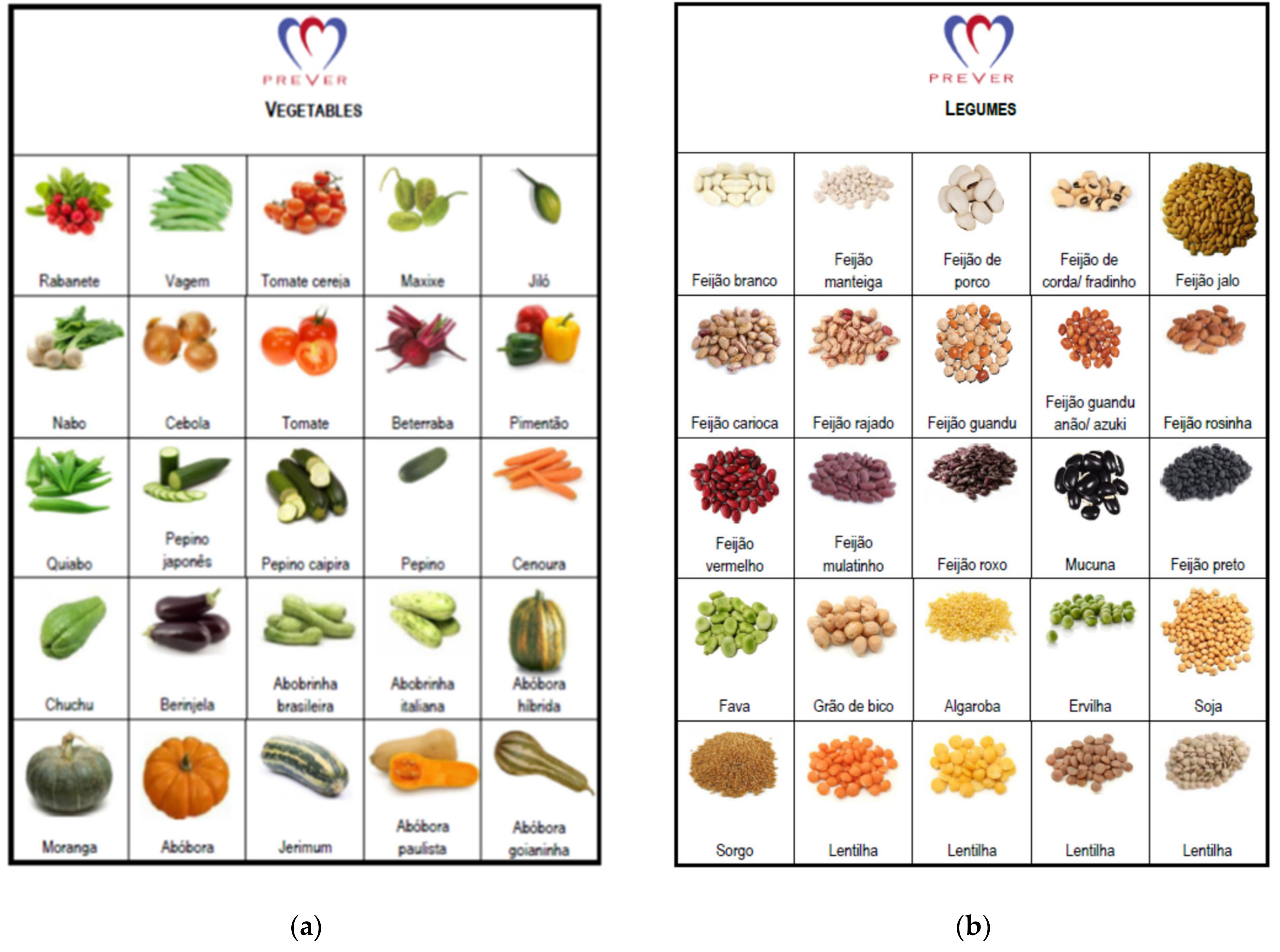
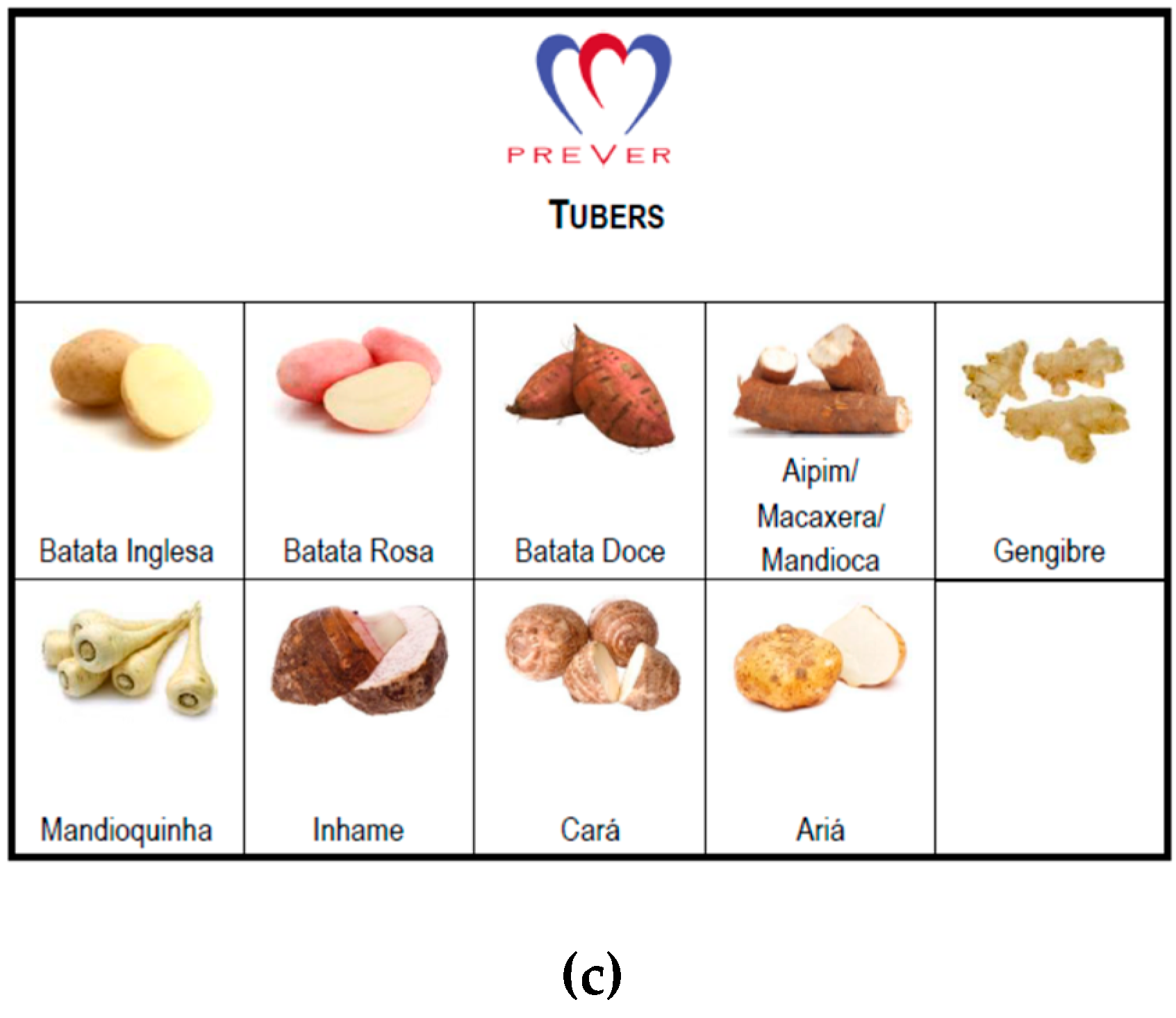
- We generated a food catalog displaying illustrations of vegetables, tubers, and legumes (Figure 2), helping participants differentiate each food group. The catalog was used during the administration of the FG-QFFQs only.
- (2)
- Examples of food items were added to the FG-QFFQ list to assist participants in remembering which items were part of each food group.
- (3)
2.6. Statistical Analysis
3. Results
3.1. Demographic Characteristics and Interview
3.2. Food Intake Assessment
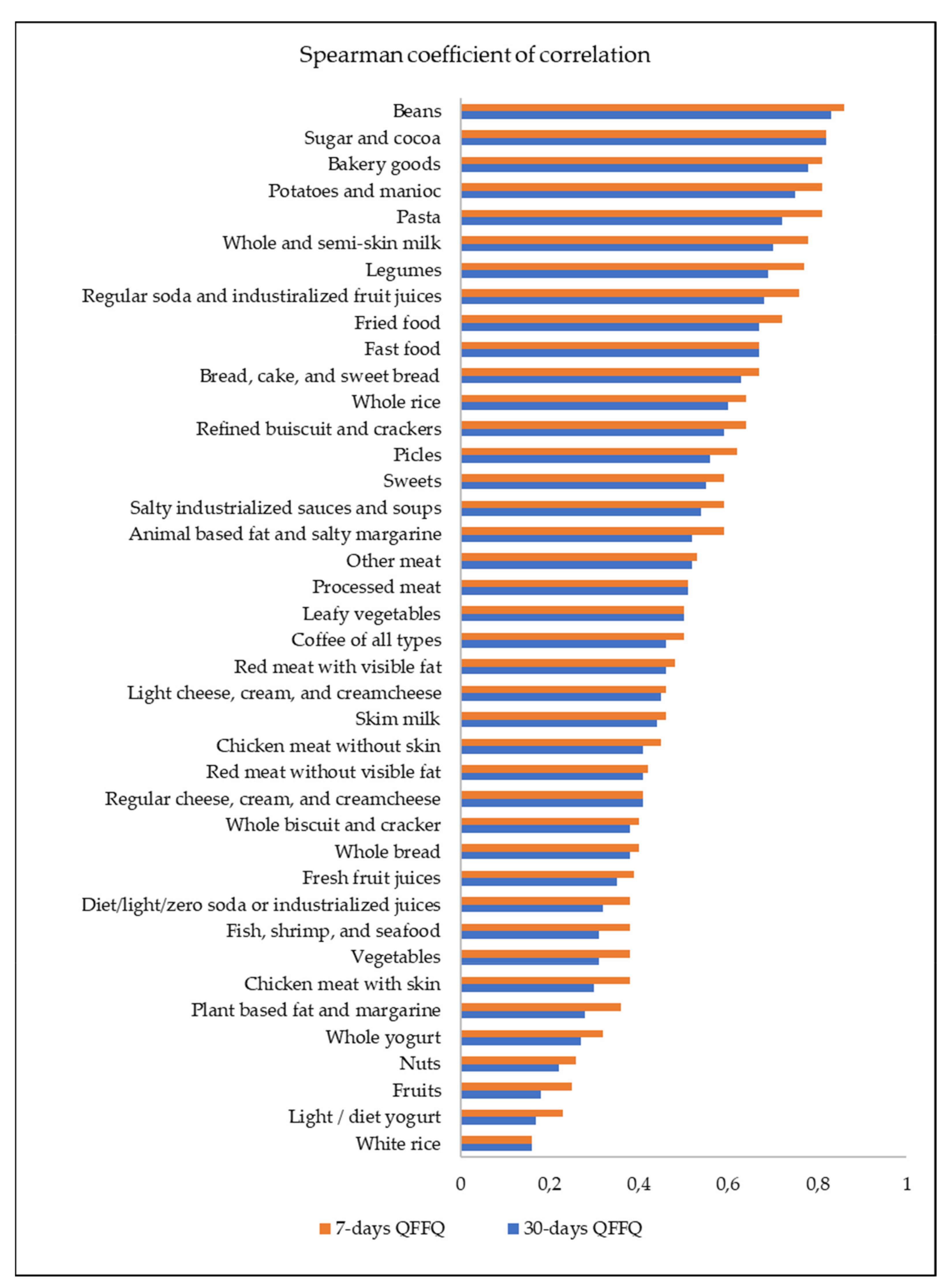
3.3. Overall Validity
3.4. Internal Validity
3.5. Reproducibility
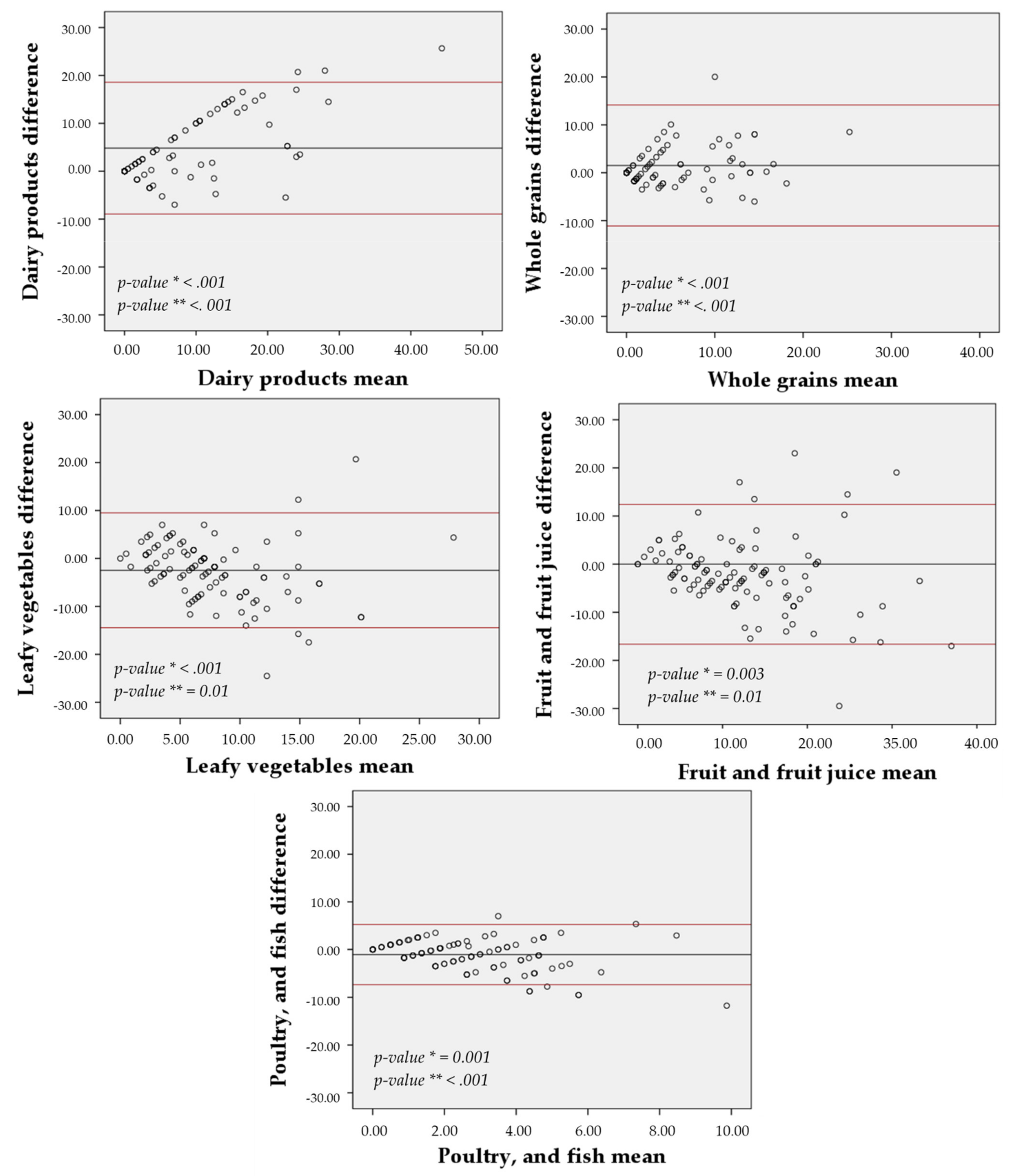
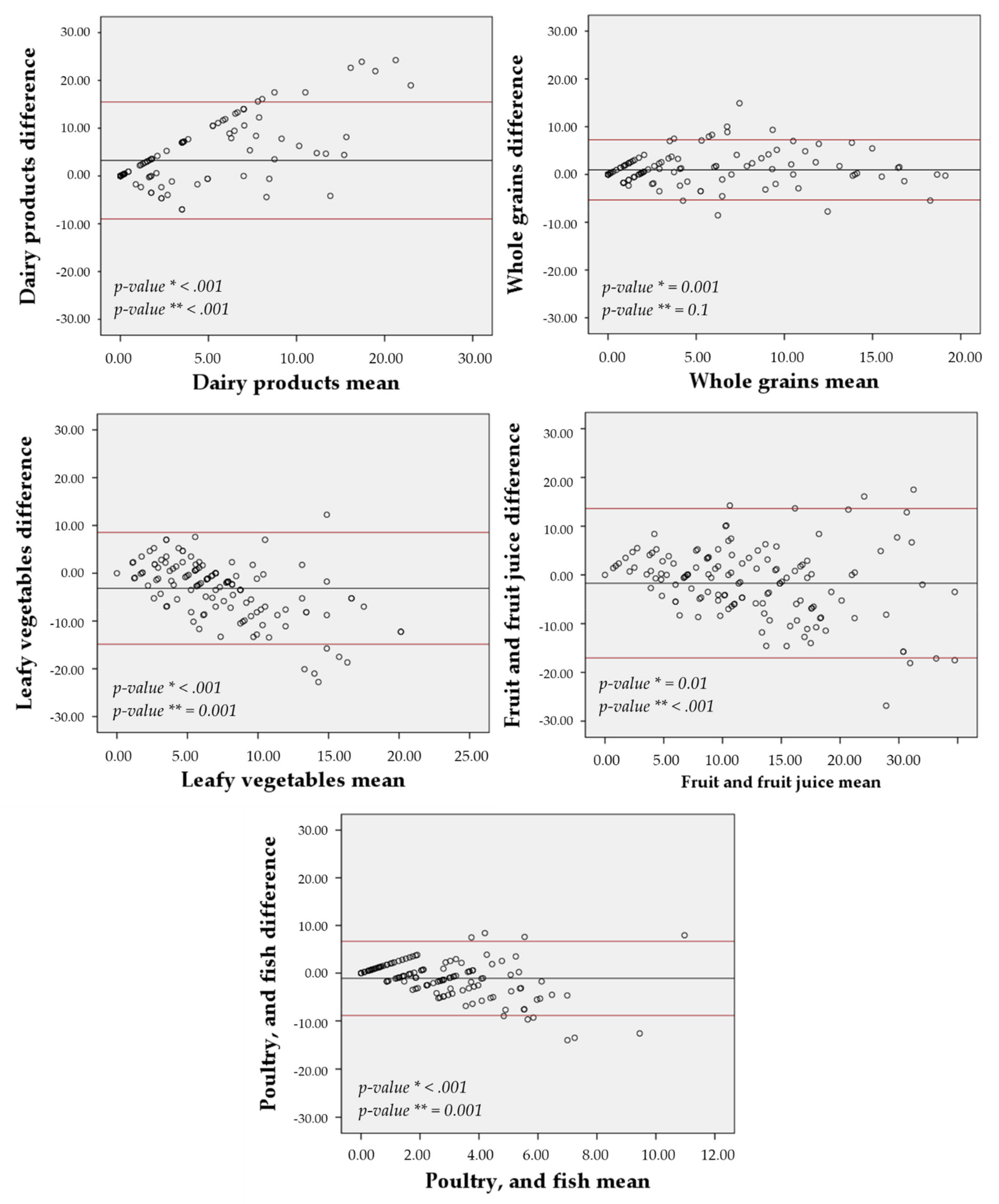
3.6. Agreement
4. Discussion
4.1. The Pilot Study and the FG-FFQ Design
4.2. Validity
4.3. Reproducibility
4.4. Strengths
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhou, B.; Carrillo-Larco, R.M.; Danaei, G.; Riley, L.M.; Paciorek, C.J.; Stevens, G.A.; Gregg, E.W.; Bennett, J.E.; Solomon, B.; Singleton, R.K.; et al. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 2021, 398, 957–980. [Google Scholar] [CrossRef]
- Picon, R.V.; Fuchs, F.D.; Riegel, G.; Fuchs, S.C. Trends in prevalence of hypertension in Brazil: A systematic review with meta-analysis. PLoS ONE 2012, 7, e48255. [Google Scholar] [CrossRef]
- Olsen, M.H.; Angell, S.Y.; Asma, S.; Boutouyrie, P.; Burger, D.; A Chirinos, J.; Damasceno, A.; Delles, C.; Gimenez-Roqueplo, A.-P.; Hering, D.; et al. A call to action and a lifecourse strategy to address the global burden of raised blood pressure on current and future generations: The Lancet Commission on hypertension. Lancet 2016, 388, 2665–2712. [Google Scholar] [CrossRef]
- Sacks, F.M.; Svetkey, L.P.; Vollmer, W.M.; Appel, L.J.; Bray, G.A.; Harsha, D.; Obarzanek, E.; Conlin, P.R.; Miller, E.R.; Simons-Morton, D.G.; et al. Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet. N. Engl. J. Med. 2001, 344, 3–10. [Google Scholar] [CrossRef]
- Appel, L.J.; Moore, T.J.; Obarzanek, E.; Vollmer, W.M.; Svetkey, L.P.; Sacks, F.M.; Bray, G.A.; Vogt, T.M.; Cutler, J.A.; Windhauser, M.M.; et al. A Clinical Trial of the Effects of Dietary Patterns on Blood Pressure. N. Engl. J. Med. 1997, 336, 1117–1124. [Google Scholar] [CrossRef]
- Guilbert, J.J. The world health report 2002-Reducing risks, promoting healthy life. Educ. Health 2003, 16, 230. [Google Scholar]
- Chobanian, A.V.; Bakris, G.L.; Black, H.R.; Cushman, W.C.; Green, L.A.; Izzo, J.L.; Jones, D.W.; Materson, B.J.; Oparil, S.; Wright, J.T.; et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003, 42, 1206–1252. [Google Scholar] [CrossRef] [PubMed]
- Lerner, M.G.; Arbor, A. Your Guide to Lowering Your Blood Pressure with DASH. DASH Eating Plan; NIH Publication No. 06-4082; National Institutes of Health/National Heart Lung and Blood Institute: Bethesda, MD, USA, 2006.
- Kwan, M.W.-M.; Wong, M.C.-S.; Wang, H.H.-X.; Liu, K.Q.-L.; Lee, C.L.-S.; Yan, B.P.-Y.; Yu, C.-M.; Griffiths, S.M. Compliance with the Dietary Approaches to Stop Hypertension (DASH) diet: A systematic review. PLoS ONE 2013, 8, e78412. [Google Scholar] [CrossRef]
- Blumenthal, J.A.; Epstein, D.E.; Sherwood, A.; Smith, P.J.; Craighead, L.; Caccia, C.; Lin, P.H.; Babyak, M.A.; Johnson, J.J.; Hinderliter, A. Determinants and Consequences of Adherence to the Dietary Approaches to Stop Hypertension Diet in African-American and White Adults with High Blood Pressure: Results from the ENCORE Trial. J. Acad. Nutr. Diet. 2012, 112, 1763–1773. [Google Scholar] [CrossRef]
- Fung, T.T.; Chiuve, S.E.; McCullough, M.L.; Rexrode, K.M.; Logroscino, G.; Hu, F.B. Adherence to a DASH-style diet and risk of coronary heart disease and stroke in women. Arch. Intern. Med. 2008, 168, 713–720. [Google Scholar] [CrossRef]
- Park, Y.M.M.; Steck, S.E.; Fung, T.T.; Zhang, J.; Hazlett, L.J.; Han, K.; Lee, S.H.; Kwon, H.S.; Merchant, A.T. Mediterranean diet, Dietary Approaches to Stop Hypertension (DASH) style diet, and metabolic health in U.S. adults. Clin. Nutr. 2017, 36, 1301–1309. [Google Scholar] [CrossRef]
- Kim, H.; Rebholz, C.M.; Garcia-Larsen, V.; Steffen, L.M.; Coresh, J.; Caulfield, L.E. Operational Differences in Plant-Based Diet Indices Affect the Ability to Detect Associations with Incident Hypertension in Middle-Aged US Adults. J. Nutr. 2020, 150, 842–850. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Chaimani, A.; Schwedhelm, C.; Toledo, E.; Pünsch, M.; Hoffmann, G.; Boeing, H. Comparative effects of different dietary approaches on blood pressure in hypertensive and pre-hypertensive patients: A systematic review and network meta-analysis. Crit. Rev. Food Sci. Nutr. 2018, 59, 2674–2687. [Google Scholar] [CrossRef]
- Willett, W.C. Nutritional Epidemiology: 24-Hour Dietary Recall and Diet Records Methods, 3rd ed.; Oxford University Press: Oxford, UK, 2013. [Google Scholar]
- Willett, W. Nutritional Epidemiology: Chapter Food Frequency Questionnaire pg 70-92, 3rd ed.; Oxford University Press: Oxford, UK, 2013; ISBN 9780199754038. [Google Scholar]
- Fuchs, F.D.; Fuchs, S.C.; Moreira, L.B.; Gus, M.; Nóbrega, A.C.; Poli-de-Figueiredo, C.E.; Mion, D.; Bortoloto, L.; Consolim-Colombo, F.; Nobre, F.; et al. Prevention of hypertension in patients with pre-hypertension: Protocol for the PREVER-prevention trial. Trials 2011, 12, 65. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, F.D.; Fuchs, S.C.; Moreira, L.B.; Gus, M.; Nóbrega, A.C.; Poli-de-Figueiredo, C.E.; Mion, D.; Bortolotto, L.; Consolim-Colombo, F.; Nobre, F.; et al. A comparison between diuretics and angiotensin-receptor blocker agents in patients with stage I hypertension (PREVER-treatment trial): Study protocol for a randomized double-blind controlled trial. Trials 2011, 12, 53. [Google Scholar] [CrossRef][Green Version]
- Cade, J.; Thompson, R.; Burley, V.; Warm, D. Development, validation and utilisation of food-frequency questionnaires —A review. Public Health Nutr. 2002, 5, 567–587. [Google Scholar] [CrossRef] [PubMed]
- Conway, J.M.; Ingwersen, L.A.; Moshfegh, A.J. Accuracy of dietary recall using the USDA five-step multiple-pass method in men: An observational validation study. J. Am. Diet. Assoc. 2004, 104, 595–603. [Google Scholar] [CrossRef]
- Godwin, S.L.; Chambers, E.; Cleveland, L. Accuracy of reporting dietary intake using various portion-size aids in-person and via telephone. J. Am. Diet. Assoc. 2004, 104, 585–594. [Google Scholar] [CrossRef]
- Monteiro, J.P. Consumo Alimentar. Visualizando Porções, 1st ed.; Guanabara Koogan: Rio de Janeiro, Brazil, 2007; ISBN 9788527712590. [Google Scholar]
- Pinheiro, A.B.V.; Lacerda, E.M.A.; Benzecry, E.H.; Gomes, M.C.S. Tabela Para Avaliação de Consumo Alimentar em Medidas Caseiras; Editora Atheneu: Rio de Janeiro, Brazil, 2005. [Google Scholar]
- Fuchs, S.C.; Moreira, L.B.; Camey, S.A.; Moreira, M.B.; Fuchs, F.D. Clustering of risk factors for cardiovascular disease among women in Southern Brazil: A population-based study. Cad. Saude Publica 2008, 24, 285–293. [Google Scholar] [CrossRef]
- Henn, R.L.; Fuchs, S.C.; Moreira, L.B.; Fuchs, F.D. Development and validation of a food frequency questionnaire (FFQ-Porto Alegre) for adolescent, adult and elderly populations from Southern Brazil. Cad. Saude Publica 2010, 26, 2068–2079. [Google Scholar] [CrossRef]
- Rossato, S.L.; Fuchs, S.C. Dietary data collected using 48-hour dietary recall: Within- and between-person variation. Front. Nutr. 2021, 8, 361. [Google Scholar] [CrossRef] [PubMed]
- Rossato, S.L.; Olinto, M.T.A.; Henn, R.L.; dos Anjos, L.A.; Bressan, A.W.; Wahrlich, V. Seasonal effect on nutrient intake in adults living in Southern Brazil. Cad. Saude Publica 2010, 26, 2177–2187. [Google Scholar] [CrossRef] [PubMed]
- Ministério da Saúde. Alimentos Regionais Brasileiros, 2nd ed.; Ministério da Saúde, Secretaria de Atenção à Saúde, Departamento de Atenção Básica: Brasilia, Brazil, 2015; ISBN 978-85-334-2145-5.
- De Souza, A.M.; Pereira, R.A.; Yokoo, E.M.; Levy, R.B.; Sichieri, R. Most consumed foods in Brazil: National Dietary Survey 2008–2009. Rev. Saude Publica 2013, 47 (Suppl. 1), 190S–199S. [Google Scholar]
- Blanton, C.A.; Moshfegh, A.J.; Baer, D.J.; Kretsch, M.J. The USDA automated multiple-pass method accurately estimates group total energy and nutrient intake. J. Nutr. 2006, 136, 2594–2599. [Google Scholar] [CrossRef]
- Rossato, S.L.; Fung, T.T.; Rodrigues, M.P. A Data Entry System for Dietary Surveys Based on Visual Basic for Applications Programming. J. Acad. Nutr. Diet. 2017, 117, 1165–1169. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. Br. Med. J. 2000, 320, 1240–1243. [Google Scholar] [CrossRef]
- Cole, T.J.; Flegal, K.M.; Nicholls, D.; Jackson, A.A. Body mass index cut offs to define thinness in children and adolescents: International survey. Br. Med. J. 2007, 335, 194–197. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef]
- Teufel, N.I. Development of culturally competent food-frequency questionnaires. Am. Soc. Nutr. 1997, 65, 1173S–1178S. [Google Scholar] [CrossRef]
- Samet, J.M.; Humble, C.G.; Skipper, B.E. Alternatives in the collection and analysis of food frequency interview data. Am. J. Epidemiol. 1984, 120, 572–581. [Google Scholar] [CrossRef] [PubMed]
- Apovian, C.M.; Murphy, M.C.; Cullum-Dugan, D.; Lin, P.H.; Gilbert, K.M.; Coffman, G.; Jenkins, M.; Bakun, P.; Tucker, K.L.; Moore, T.J. Validation of a web-based dietary questionnaire designed for the DASH (Dietary Approaches to Stop Hypertension) diet: The DASH Online Questionnaire. Public Health Nutr. 2010, 13, 615–622. [Google Scholar] [CrossRef] [PubMed]
- Niedzwiedzka, E.; Wadolowska, L.; Kowalkowska, J. Reproducibility of A Non-Quantitative Food Frequency Questionnaire (62-Item FFQ-6) and PCA-Driven Dietary Pattern Identification in 13-21-Year-Old Females. Nutrients 2019, 11, 2183. [Google Scholar] [CrossRef]
- Martela, K.; Kuźniewicz, R.; Pluskiewicz, W.; Tabor, E.; Zagórski, P. Relevance of the semi-quantitative short Food Frequency Questionnaire in assessment of calcium consumption by female inhabitants of Zabrze over the age of 55 years (the Silesia Osteo Active Study). Arch. Osteoporos. 2019, 14, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Bredin, C.; Naimimohasses, S.; Norris, S.; Wright, C.; Hancock, N.; Hart, K.; Moore, J.B. Development and relative validation of a short food frequency questionnaire for assessing dietary intakes of non-alcoholic fatty liver disease patients. Eur. J. Nutr. 2020, 59, 571–580. [Google Scholar] [CrossRef]
- Affret, A.; Wagner, S.; El Fatouhi, D.; Dow, C.; Correia, E.; Niravong, M.; Clavel-Chapelon, F.; De Chefdebien, J.; Fouque, D.; Stengel, B.; et al. Validity and reproducibility of a short food frequency questionnaire among patients with chronic kidney disease. BMC Nephrol. 2017, 18, 297. [Google Scholar] [CrossRef]
- Akoglu, H. User’s guide to correlation coefficients. Turkish J. Emerg. Med. 2018, 18, 91–93. [Google Scholar] [CrossRef] [PubMed]
- Imaeda, N.; Goto, C.; Sasakabe, T.; Mikami, H.; Oze, I.; Hosono, A.; Naito, M.; Miyagawa, N.; Ozaki, E.; Ikezaki, H.; et al. Reproducibility and validity of food group intake in a short food frequency questionnaire for the middle-aged Japanese population. Environ. Health Prev. Med. 2021, 26, 28. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall (n = 137) | Men (n = 55) | Women (n = 82) | p-Value * | |
|---|---|---|---|---|
| Age | 61 ± 10 | 63 ± 11 | 61 ± 9 | 0.2 |
| Education, in years of study | 8.6 ± 4.0 | 9.9 ± 4.2 | 7.8 ± 3.6 | 0.07 |
| Body mass index (kg/m2) | 30.5 ± 5.6 | 29.5 ± 4.8 | 31.2 ± 6.1 | 0.09 |
| First visit | ||||
| Systolic blood pressure (mm Hg) | 137.8 ± 18.9 | 139.2 ± 19.3 | 136.9 ± 18.7 | 0.5 |
| Diastolic blood pressure (mm Hg) | 82.4 ± 12 | 82 ± 11.7 | 82.6 ± 12.3 | 0.8 |
| Body mass index (kg/m2) | 30.5 ± 5.6 | 29.4 ± 4.8 | 31.2 ± 6 | 0.08 |
| Fourth Visit | ||||
| Systolic blood pressure (mm Hg) | 135.3 ± 21.8 | 137.3 ± 20.6 | 134 ± 22.7 | 0.4 |
| Diastolic blood pressure (mm Hg) | 80.1 ± 12.8 | 80.8 ± 13.8 | 79.6 ± 12.1 | 0.6 |
| Body mass index (kg/m2) | 30.2 ± 5.6 | 29 ± 4.1 | 31 ± 6.3 | 0.06 |
| Overall (n = 137) | Men (n = 55) | Women (n = 82) | p-Value1 | |
|---|---|---|---|---|
| Time Spent to Assess Dietary Intake in Minutes [Mean ± SD] | ||||
| 30-day FG-QFFQ 2 | 0:20 ± 0:07 | 0:21 ± 0:09 | 0:20 ± 0:06 | 0.7 |
| 7-day FG-QFFQ 2 | 0:15 ± 0:05 | 0:15 ± 0:06 | 0:15 ± 0:04 | 0.7 |
| Mean difference 2,3 | 0:04 ± 0:08 | 0:05 ± 0:08 | 0:03 ± 0:06 | <0.001 |
| 24-h dietary recall | 0:19 ± 0:05 | 0:19 ± 0:06 | 0:19 ± 0:04 | 0.5 |
| First visit | ||||
| 30-day FG-QFFQ | 0:21 ± 0:08 | 0:21 ± 0:10 | 0:22 ± 0:07 | 0.7 |
| 24-h dietary recall | 0:19 ± 0:06 | 0:20 ± 0:08 | 0:18 ± 0:05 | 0.09 |
| Second Visit | ||||
| FG-QFFQ 7-days | 0:15 ± 0:05 | 0:14 ± 0:04 | 0:16 ± 0:06 | 0.07 |
| 24-h dietary recall | 0:20 ± 0:09 | 0:21 ± 0:09 | 0:20 ± 0:09 | 0.6 |
| Third visit | ||||
| 7-day FG-QFFQ | 0:15 ± 0:08 | 0:16 ± 0:11 | 0:15 ± 0:05 | 0.4 |
| 24-h dietary recall | 0:19 ± 0:08 | 0:19 ± 0:08 | 0:18 ± 0:07 | 0.5 |
| Fourth visits | ||||
| 30-day FG-QFFQ | 0:19 ± 0:08 | 0:20 ± 0:10 | 0:18 ± 0:06 | 0.1 |
| 24-h dietary recall | 0:18 ± 0:07 | 0:17 ± 0:06 | 0:19 ± 0:07 | 0.1 |
| Food Items and Food Groups (Servings per Week) | Mean ± SD | ||
|---|---|---|---|
| 30-Day FG-QFFQ (n = 137) | 7-Day FG-QFFQ (n = 106) | 24-h DR (n = 137) | |
| Sugar and cocoa | 5.3 ± 6.5 | 4.1 ± 5.6 | 13.9 ± 10 |
| Coffee of all types | 12.4 ± 7.7 | 12.1 ± 7.3 | 12.7 ± 6.3 |
| Sweets | 4.3 ± 4.3 | 4.2 ± 4.9 | 6.6 ± 6.2 |
| Red meat with visible fat | 1.7 ± 1.9 | 1.5 ± 2.3 | 0.8 ± 1.4 |
| Red meat without visible fat | 1.9 ± 1.9 | 2.3 ± 3.2 | 4.1 ± 3.3 |
| Chicken meat without skin | 1.0 ± 1.4 | 1.2 ± 1.5 | 1.0 ± 1.7 |
| Chicken meat with skin | 1.5 ± 1.9 | 1.4 ± 1.7 | 2.7 ± 2.9 |
| Processed meat | 3.3 ± 3.8 | 3.6 ± 4.0 | 3.7 ± 4.2 |
| Other meat | 0.5 ± 0.6 | 0.5 ± 0.9 | 2.5 ± 2.8 |
| Fish, shrimp, and seafood | 0.6 ± 0.7 | 0.6 ± 0.9 | 0.5 ± 1.2 |
| White rice | 6.8 ± 3.6 | 6.9 ± 4.8 | 6.1 ± 3.2 |
| Whole rice | 0.6 ± 1.4 | 0.6 ± 1.5 | 0.4 ± 1.3 |
| Refines biscuit and cracker | 1.4 ± 2.9 | 1.3 ± 2.7 | 1.5 ± 2.8 |
| Whole biscuit and cracker | 0.4 ± 0.9 | 0.5 ± 1.5 | 0.4 ± 1.1 |
| Pasta | 1.3 ± 1.1 | 1.3 ± 1.4 | 2.1 ± 2.3 |
| Bread, cake, and sweet bread | 7.3 ± 5.1 | 8.0 ± 7.6 | 8.1 ± 5.5 |
| Whole bread | 3.8 ± 4.7 | 4.1 ± 7.5 | 2.9 ± 4.4 |
| Salty industrialized sauces and soups | 2.2 ± 2.8 | 2.3 ± 3.0 | 6.1 ± 4.5 |
| Regular soda and industrialized juices | 2.6 ± 3.7 | 2.8 ± 4.1 | 3.5 ± 4.5 |
| Diet/light/zero soda and industrialized juices | 1.3 ± 3.0 | 1.9 ± 4.1 | 1.6 ± 3.1 |
| Bakery goods | 0.2 ± 0.4 | 0.2 ± 0.4 | 0.2 ± 0.8 |
| Fast food | 0.3 ± 0.8 | 0.2 ± 0.4 | 0.4 ± 1.4 |
| Nuts | 1.0 ± 1.9 | 1.0 ± 2.2 | 0.4 ± 1.2 |
| Beans | 5.4 ± 4.2 | 5.1 ± 3.4 | 3.8 ± 2.9 |
| Legumes | 0.7 ± 1.0 | 0.6 ± 1.1 | 0.1 ± 0.5 |
| Light/diet yogurt | 0.4 ± 1.7 | 0.7 ± 3.7 | 0.6 ± 1.7 |
| Whole yogurt | 0.9 ± 2.1 | 0.6 ± 1.5 | 0.1 ± 0.5 |
| Skim milk | 3.3 ± 5.5 | 3.3 ± 5.2 | 0.2 ± 1.3 |
| Whole and semi-skim milk | 4.9 ± 6.0 | 5.0 ± 6.8 | 10.8 ± 7.2 |
| Light cheese, cream, and cream cheese | 1.0 ± 2.4 | 0.9 ± 2.3 | 0.7 ± 1.7 |
| Regular cheese, cream, and cream cheese | 3.5 ± 3.7 | 4.0 ± 5.0 | 5.4 ± 5.1 |
| Pickles | 0.6 ± 1.4 | 0.5 ± 0.9 | 1.0 ± 2.1 |
| Fried foods | 0.8 ± 1.0 | 0.8 ± 0.9 | 0.7 ± 1.4 |
| Animal-based fat and salty margarine | 2.4 ± 3.8 | 2.2 ± 3.8 | 25 ± 9.5 |
| Plant-based fat and salty margarine | 11.1 ± 5.7 | 13.1 ± 9.8 | 5.4 ± 5.0 |
| Potatoes and manioc | 1.8 ± 1.6 | 1.6 ± 1.8 | 2.9 ± 2.8 |
| Fruits | 9.6 ± 5.1 | 9.4 ± 6.2 | 12.6 ± 8.6 |
| Fresh fruit juices | 5.3 ± 3.1 | 5.4 ± 3.7 | 0.9 ± 1.8 |
| Vegetables | 2.2 ± 3.7 | 1.9 ± 3.5 | 9.0 ± 6.3 |
| Leafy vegetables | 5.8 ± 3.4 | 6.5 ± 5.0 | 11.9 ± 6.7 |
| Food Items and Food Groups (Servings per Week) | 30-Day FG-QFFQ | p-Value | 7-Day FG-QFFQ | p-Value |
|---|---|---|---|---|
| Sugar and cocoa | 0.51 | <0.001 | 0.52 | <0.001 |
| Coffee of all types | 0.69 | <0.001 | 0.73 | <0.001 |
| Sweets | 0.51 | <0.001 | 0.43 | <0.001 |
| Red meat with visible fat | 0.22 | 0.009 | 0.10 | 0.315 |
| Red meat without visible fat | 0.41 | <0.001 | 0.43 | <0.001 |
| Chicken meat without skin | 0.37 | <0.001 | 0.17 | 0.074 |
| Chicken meat with skin | 0.13 | 0.1 | 0.23 | 0.018 |
| Processed meat | 0.72 | <0.001 | 0.70 | <0.001 |
| Other meat | 0.29 | 0.001 | 0.13 | 0.196 |
| Fish, shrimp, and seafood | 0.18 | 0.03 | 0.13 | 0.188 |
| White rice | 0.57 | <0.001 | 0.57 | <0.001 |
| Whole rice | 0.68 | <0.001 | 0.35 | <0.001 |
| Refines biscuit and cracker | 0.55 | <0.001 | 0.62 | <0.001 |
| Whole biscuit and cracker | 0.62 | <0.001 | 0.67 | <0.001 |
| Pasta | 0.24 | 0.005 | 0.45 | <0.001 |
| Bread, cake, and sweet bread | 0.78 | <0.001 | 0.55 | <0.001 |
| Whole bread | 0.81 | <0.001 | 0.62 | <0.001 |
| Salty industrialized sauces and soups | 0.32 | <0.001 | 0.33 | 0.001 |
| Regular soda and industrialized juices | 0.6 | <0.001 | 0.34 | <0.001 |
| Diet/light/zero soda and industrialized juices | 0.76 | <0.001 | 0.84 | <0.001 |
| Bakery goods | 0.24 | 0.005 | 0.29 | 0.002 |
| Fast food | 0.15 | 0.08 | 0.16 | 0.108 |
| Nuts | 0.66 | <0.001 | 0.78 | <0.001 |
| Beans | 0.35 | <0.001 | 0.50 | <0.001 |
| Legumes | 0.11 | 0.2 | 0.34 | <0.001 |
| Light/diet yogurt | 0.56 | <0.001 | 0.57 | <0.001 |
| Whole yogurt | 0.09 | 0.3 | 0.48 | <0.001 |
| Skim milk | 0.23 | 0.007 | 0.29 | 0.002 |
| Whole and semi-skim milk | 0.55 | <0.001 | 0.49 | <0.001 |
| Light cheese, cream, and cream cheese | 0.76 | <0.001 | 0.74 | <0.001 |
| Regular cheese, cream, and cream cheese | 0.66 | <0.001 | 0.57 | <0.001 |
| Pickles | 0.21 | 0.02 | 0.45 | <0.001 |
| Fried foods | 0.45 | <0.001 | 0.41 | <0.001 |
| Animal-based fat and salty margarine | 0.74 | <0.001 | 0.66 | <0.001 |
| Plant-based fat and salty margarine | 0.46 | <0.001 | 0.29 | 0.002 |
| Potatoes and manioc | 0.26 | 0.003 | 0.29 | 0.002 |
| Fruits | 0.54 | <0.001 | 0.57 | <0.001 |
| Fresh fruit juices | 0.38 | <0.001 | 0.55 | <0.001 |
| Vegetables | 0.22 | 0.01 | 0.36 | <0.001 |
| Leafy vegetables | 0.57 | <0.001 | 0.36 | <0.001 |
| Food Items | 30-Day FG-QFFQ 1 | 7-Day FG-QFFQ 1 | ||||||
|---|---|---|---|---|---|---|---|---|
| Initial Model | Final Model | Initial Model | Final Model | |||||
| R | A | r | α | r | A | r | α | |
| Global internal validity | 0.59 | 0.74 | 0.61 | 0.76 | ||||
| Sugar and cocoa 5 | 0.14 | 0.53 | 0.32 | 0.65 | −0.07 | 0.65 | - | - |
| Coffee of all types | 0.31 | 0.49 | 0.23 | 0.67 | 0.33 | 0.60 | 0.25 | 0.74 |
| Sweets | 0.28 | 0.51 | 0.24 | 0.65 | 0.33 | 0.60 | 0.28 | 0.74 |
| Red meat with visible fat | 0.16 | 0.53 | 0.28 | 0.65 | 0.41 | 0.61 | 0.46 | 0.73 |
| Red meat without visible fat | 0.23 | 0.52 | 0.24 | 0.66 | 0.17 | 0.62 | 0.25 | 0.74 |
| Chicken meat without skin 7 | 0.10 | 0.53 | 0.20 | 0.66 | 0.39 | 0.62 | - | - |
| Chicken meat with skin 2,6 | −0.01 | 0.54 | - | - | 0.05 | 0.63 | - | - |
| Processed meat 6 | 0.32 | 0.50 | 0.35 | 0.64 | 0.15 | 0.62 | 0.13 | 0.75 |
| Other meat | 0.07 | 0.53 | 0.13 | 0.66 | 0.03 | 0.63 | - | - |
| Fish, shrimp, and seafood 2 | −0.05 | 0.54 | - | - | 0.35 | 0.62 | 0.38 | 0.74 |
| White rice | 0.24 | 0.51 | 0.37 | 0.64 | 0.39 | 0.60 | 0.49 | 0.72 |
| Whole rice 2,6 | −0.03 | 0.54 | - | - | 0.02 | 0.63 | - | - |
| Refines biscuit and cracker 3,5 | 0.07 | 0.53 | - | - | −0.04 | 0.63 | - | - |
| Whole biscuit and cracker 3,5 | 0.09 | 0.53 | - | - | −0.03 | 0.63 | - | - |
| Pasta | 0.07 | 0.53 | 0.18 | 0.66 | 0.24 | 0.62 | 0.20 | 0.74 |
| Bread, cake, and sweet bread | 0.23 | 0.51 | 0.46 | 0.62 | 0.46 | 0.58 | 0.61 | 0.70 |
| Whole bread 1,6 | −0.12 | 0.56 | - | - | 0.03 | 0.64 | - | - |
| Salty industrialized sauces and soups 5 | 0.11 | 0.53 | 0.17 | 0.66 | −0.03 | 0.63 | - | - |
| Regular soda and industrialized juices | 0.19 | 0.52 | 0.36 | 0.64 | 0.00 | 0.63 | - | - |
| Diet/light/zero soda and industrialized juices | 0.15 | 0.52 | 0.13 | 0.66 | 0.03 | 0.63 | - | - |
| Bakery goods | 0.06 | 0.53 | 0.18 | 0.66 | 0.00 | 0.63 | - | - |
| Fast food 6 | 0.20 | 0.53 | 0.20 | 0.66 | −0.04 | 0.63 | - | - |
| Nuts 3 | 0.06 | 0.53 | - | - | 0.13 | 0.62 | 0.11 | 0.74 |
| Beans | 0.14 | 0.52 | 0.19 | 0.66 | 0.11 | 0.62 | 0.14 | 0.74 |
| Legumes | 0.24 | 0.53 | 0.09 | 0.66 | 0.13 | 0.62 | 0.14 | 0.74 |
| Light/diet yogurt 2,5 | −0.05 | 0.54 | - | - | −0.05 | 0.64 | - | - |
| Whole yogurt 3 | 0.06 | 0.53 | - | - | 0.17 | 0.62 | 0.14 | 0.74 |
| Skim milk 2,5 | −0.08 | 0.56 | - | - | −0.08 | 0.64 | - | - |
| Whole and semi-skim milk | 0.20 | 0.52 | 0.32 | 0.64 | 0.34 | 0.60 | 0.40 | 0.73 |
| Light cheese, cream, and cream cheese 3,6 | 0.04 | 0.53 | - | - | 0.05 | 0.63 | - | - |
| Regular cheese, cream, and cream cheese | 0.23 | 0.51 | 0.20 | 0.66 | 0.33 | 0.60 | 0.38 | 0.73 |
| Pickles 5 | 0.33 | 0.52 | 0.32 | 0.66 | −0.10 | 0.63 | - | - |
| Fried foods 5,6 | 0.21 | 0.53 | 0.36 | 0.66 | 0.09 | 0.63 | - | - |
| Animal-based fat and salty margarine 5 | 0.06 | 0.53 | 0.18 | 0.66 | −0.11 | 0.64 | - | - |
| Plant-based fat and salty margarine | 0.22 | 0.51 | 0.22 | 0.66 | 0.41 | 0.58 | 0.46 | 0.73 |
| Potatoes and manioc | 0.21 | 0.52 | 0.28 | 0.66 | 0.28 | 0.62 | 0.31 | 0.74 |
| Fruits 3 | 0.14 | 0.53 | - | - | 0.34 | 0.60 | 0.39 | 0.73 |
| Fresh fruit juices 4 | 0.28 | 0.51 | - | - | 0.39 | 0.60 | 0.40 | 0.73 |
| Vegetables 3 | 0.13 | 0.53 | - | - | 0.10 | 0.62 | 0.13 | 0.74 |
| Leafy vegetables 3 | 0.02 | 0.54 | - | - | 0.46 | 0.59 | 0.52 | 0.72 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rossato, S.L.; Mosele, F.; Moreira, L.B.; Rodrigues, M.P.; Lima, R.F.; Fuchs, F.D.; Fuchs, S.C. Development, Validation, and Reproducibility of Food Group-Based Frequency Questionnaires for Clinical Use in Brazil: A Pre-Hypertension and Hypertension Diet Assessment. Nutrients 2021, 13, 3881. https://doi.org/10.3390/nu13113881
Rossato SL, Mosele F, Moreira LB, Rodrigues MP, Lima RF, Fuchs FD, Fuchs SC. Development, Validation, and Reproducibility of Food Group-Based Frequency Questionnaires for Clinical Use in Brazil: A Pre-Hypertension and Hypertension Diet Assessment. Nutrients. 2021; 13(11):3881. https://doi.org/10.3390/nu13113881
Chicago/Turabian StyleRossato, Sinara L., Francisca Mosele, Leila B. Moreira, Marcela Perdomo Rodrigues, Ruchelli França Lima, Flávio D. Fuchs, and Sandra C. Fuchs. 2021. "Development, Validation, and Reproducibility of Food Group-Based Frequency Questionnaires for Clinical Use in Brazil: A Pre-Hypertension and Hypertension Diet Assessment" Nutrients 13, no. 11: 3881. https://doi.org/10.3390/nu13113881
APA StyleRossato, S. L., Mosele, F., Moreira, L. B., Rodrigues, M. P., Lima, R. F., Fuchs, F. D., & Fuchs, S. C. (2021). Development, Validation, and Reproducibility of Food Group-Based Frequency Questionnaires for Clinical Use in Brazil: A Pre-Hypertension and Hypertension Diet Assessment. Nutrients, 13(11), 3881. https://doi.org/10.3390/nu13113881