
Randomized Controlled Trial for Promotion of Healthy Eating in Older Adults by Increasing Consumption of Plant-Based Foods: Effect on Inflammatory Biomarkers




Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
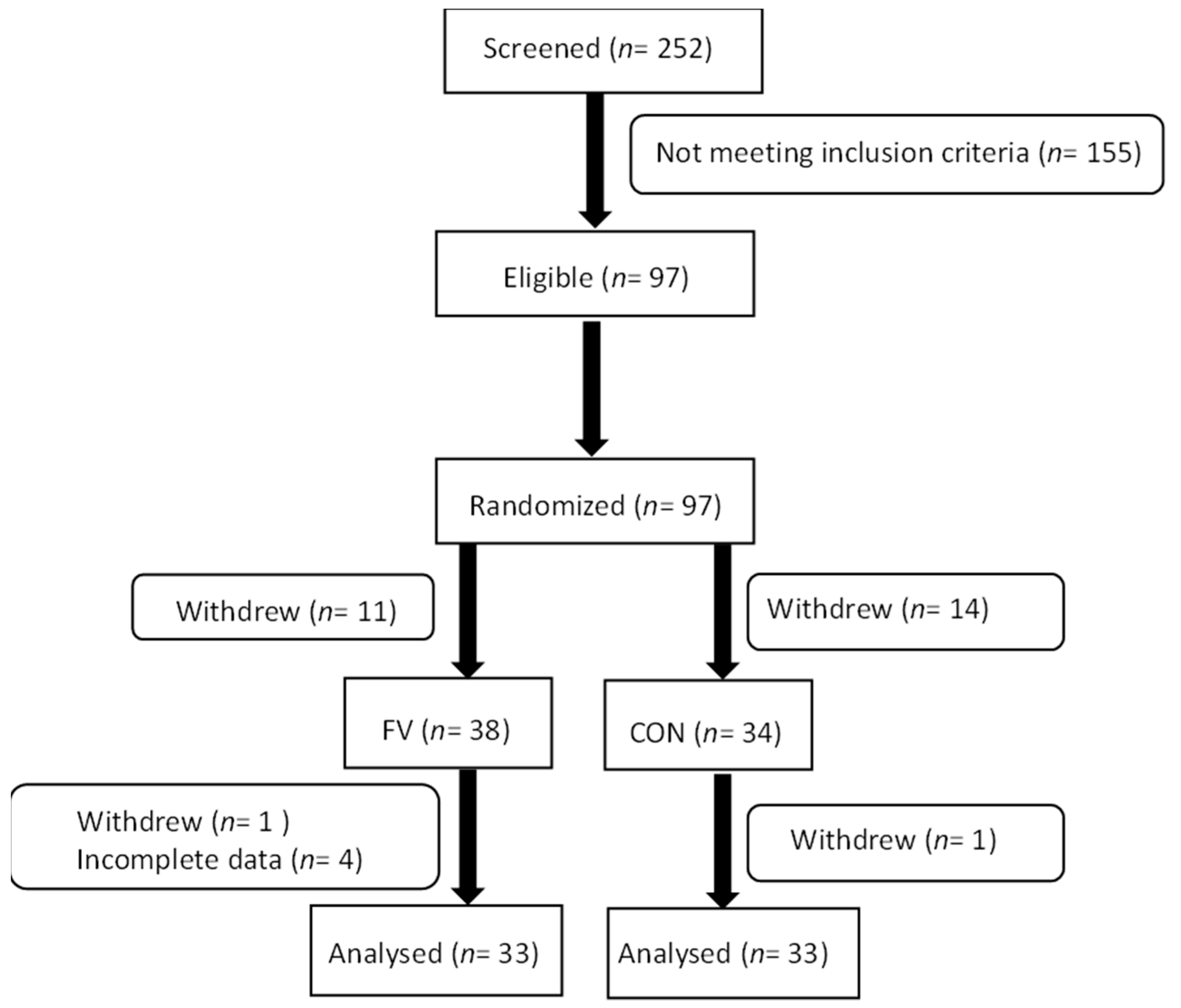
2.2. Participants
2.3. Intervention
2.4. Assessment of Dietary Patterns
2.5. Assessment of Physical Activity
2.6. Assessment of Anthropometrical Variables
2.7. Assessment of Serum Levels of Inflammatory Biomarkers
2.8. Statistical Analysis
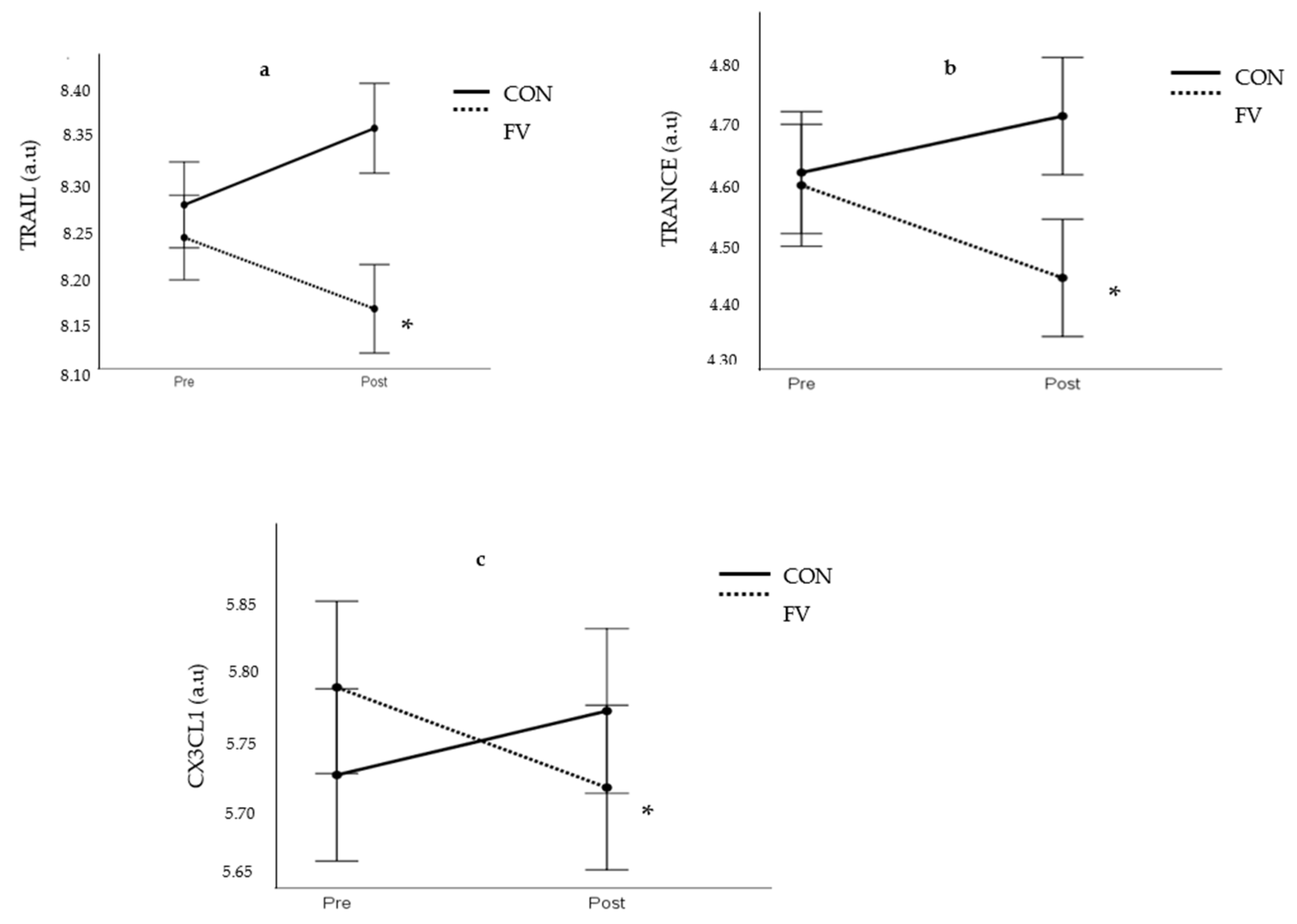
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Frasca, D.; Blomberg, B.B.; Paganelli, R. Aging, Obesity, and Inflammatory Age-Related Diseases. Front. Immunol. 2017, 8, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, L.J.; Barbagallo, M. The biology of the metabolic syndrome and aging. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 5–11. [Google Scholar]
- Franceschi, C.; Santoro, A.; Capri, M. The complex relationship between Immunosenescence and Inflammaging: Special issue on the New Biomedical Perspectives. Semin. Immunopathol. 2020, 42, 517–520. [Google Scholar]
- Guarner, V.; Rubio-Ruiz, M.E. Low-grade systemic inflammation connects aging, metabolic syndrome and cardiovascular disease. Interdiscip. Top. Gerontol. 2015, 40, 99–106. [Google Scholar]
- Lopez-Candales, A.; Hernández Burgos, P.M.; Hernandez-Suarez, D.F.; Harris, D. Linking Chronic Inflammation with Cardiovascular Disease: From Normal Aging to the Metabolic Syndrome. J. Nat. Sci. 2017, 3, e341. [Google Scholar] [PubMed]
- GBD 2017 Diet Collaborators. Health effects of dietary risks in 195 countries, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]
- Appleton, K.M.; McGill, R.; Woodside, J.V. Fruit and vegetable consumption in older people in Northern Ireland: Levels and patterns. Br. J. Nutr. 2009, 102, 949–953. [Google Scholar] [PubMed] [Green Version]
- Wakimoto, P.; Block, G. Dietary intake, dietary patterns, and changes with age: An epidemiological perspective. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, 65–80. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Nutrition in Universal Health Coverage; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Zhu, F.; Du, B.; Xu, B. Anti-inflammatory effects of phytochemicals from fruits, vegetables, and food legumes: A review. Crit. Rev. Food Sci. Nutr. 2018, 58, 1260–1270. [Google Scholar] [CrossRef] [PubMed]
- Dauchet, L.; Amouyel, P.; Hercberg, S.; Dallongeville, J. Fruit and vegetable consumption and risk of coronary heart disease: A meta-analysis of cohort studies. J. Nutr. 2006, 136, 2588–2593. [Google Scholar] [CrossRef] [Green Version]
- Dauchet, L.; Amouyel, P.; Dallongeville, J. Fruit and vegetable consumption and risk of stroke: A meta-analysis of cohort studies. Neurology 2005, 65, 1193–1197. [Google Scholar] [CrossRef] [PubMed]
- Gibson, A.; Edgar, J.D.; Neville, C.E.; Gilchrist, S.E.C.M.; McKinley, M.C.; Patterson, C.C.; Young, I.S.; Woodside, J.V. Effect of fruit and vegetable consumption on immune function in older people: A randomized controlled trial. Am. J. Clin. Nutr. 2012, 96, 1429–1436. [Google Scholar] [CrossRef] [Green Version]
- Watzl, B.; Kulling, S.E.; Möseneder, J.; Barth, S.W.; Bub, A. 4wk intervention with high intake of carotenoid-rich vegetables and fruit reduces plasma C-reactive protein in healthy, nonsmoking men. Am. J. Clin. Nutr. 2005, 82, 1052–1058. [Google Scholar] [CrossRef]
- McCall, D.O.; McGartland, C.P.; McKinley, M.C.; Sharpe, P.; McCance, D.R.; Young, I.S.; Woodside, J.V. The effect of increased dietary fruit and vegetable consumption on endothelial activation, inflammation and oxidative stress in hypertensive volunteers. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 658–664. [Google Scholar] [CrossRef] [PubMed]
- Nadeem, N.; Woodside, J.V.; Neville, C.E.; McCall, D.O.; McCance, D.; Edgar, D.; Young, I.S.; McEneny, J. Serum amyloid A-related inflammation is lowered by increased fruit and vegetable intake, while high-sensitive C-reactive protein, IL-6 and E-selectin remain unresponsive. Br. J. Nutr. 2014, 112, 1129–1136. [Google Scholar]
- Nilsson, A.; Bergens, O.; Kadi, F. Physical activity alters inflammation in older adults by different intensity levels. Med. Sci. Sports Exerc. 2018, 50, 1502–1507. [Google Scholar] [CrossRef] [PubMed]
- Papaioannou, K.G.; Nilsson, A.; Nilsson, L.M.; Kadi, F. Healthy Eating Is Associated with Sarcopenia Risk in Physically Active Older Adults. Nutrients 2021, 13, 2813. [Google Scholar]
- Nilsson, A.; Wåhlin-Larsson, B.; Kadi, F. Physical activity and not sedentary time per se influences on clustered metabolic risk in elderly community-dwelling women. PLoS ONE 2017, 12, e0175496. [Google Scholar]
- Bergens, O.; Nilsson, A.; Kadi, F. Cardiorespiratory Fitness Does Not Offset Adiposity-Related Systemic Inflammation in Physically Active Older Women. J. Clin. Endocrinol. Metab. 2019, 104, 4119–4126. [Google Scholar]
- Min, J.K.; Kim, Y.M.; Kim, S.W.; Kwon, M.C.; Kong, Y.Y.; Hwang, I.K.; Won, M.H.; Rho, J.; Kwon, Y.G. TNF-Related Activation-Induced Cytokine Enhances Leukocyte Adhesiveness: Induction of ICAM-1 and VCAM-1 via TNF Receptor-Associated Factor and Protein Kinase C-Dependent NF-κB Activation in Endothelial Cells. J. Immunol. 2005, 175, 531–540. [Google Scholar] [CrossRef] [Green Version]
- Flierl, U.; J Bauersachs, J.; Schäfer, A. Modulation of platelet and monocyte function by the chemokine fractalkine (CX3 CL1) in cardiovascular disease. Eur. J. Clin. Invest. 2015, 45, 624–633. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Shen, Y.; Zhang, J.; Wan, C.; Wang, T.; Xu, D.; Yang, T.; Wen, F. Increased serum TRAIL and DR5 levels correlated with lung function and inflammation in stable COPD patients. Int. J. Chron. Obs. Pulmon. Dis. 2015, 10, 2405–2412. [Google Scholar]
- Neville, C.E.; McKinley, M.C.; Draffin, C.R.; Gallagher, N.E.; Appleton, K.M.; Young, I.S.; Edgar, J.D.; Woodside, J.V. Participating in a fruit and vegetable intervention trial improves longer term fruit and vegetable consumption and barriers to fruit and vegetable consumption: A follow-up of the ADIT study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 158. [Google Scholar] [PubMed] [Green Version]
- Duthie, S.J.; Duthie, G.G.; Russell, W.R.; Kyle, J.A.M.; Macdiarmid, J.I.; Rungapamestry, V.; Stephen, S.; Megias-Baeza, C.; Kaniewska, J.J.; Shaw, L.; et al. Effect of increasing fruit and vegetable intake by dietary intervention on nutritional biomarkers and attitudes to dietary change: A randomised trial. Eur. J. Nutr. 2018, 57, 1855–1872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baldrick, F.R.; Elborn, J.S.; Woodside, J.V.; Treacy, K.; Bradley, J.M.; Patterson, C.C.; Schock, B.C.; Ennis, M.; Young, I.S.; McKinley, M.C. Effect of fruit and vegetable intake on oxidative stress and inflammation in COPD: A randomised controlled trial. Eur. Respir. J. 2012, 39, 1377–1384. [Google Scholar]
- Wagner, M.G.; Rhee, Y.; Honrath, K.; Blodgett Salafia, E.H.; Terbizan, D. Nutrition education effective in increasing fruit and vegetable consumption among overweight and obese adults. Appetite 2016, 100, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, L.J.; Ball, L.E.; Ross, L.J.; Barnes, K.A.; Williams, L.T. Effectiveness of Dietetic Consultations in Primary Health Care: A Systematic Review of Randomized Controlled Trials. J. Acad. Nutr. Diet. 2017, 117, 1941–1962. [Google Scholar]
- Patnode, C.D.; Evans, C.V.; Senger, C.A.; Redmond, N.; Lin, J.S. Behavioral Counseling to Promote a Healthful Diet and Physical Activity for Cardiovascular Disease Prevention in Adults without Known Cardiovascular Disease Risk Factors: Updated Systematic Review for the U.S. Preventive Services Task Force; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2017.
- Fulton, S.L.; McKinley, M.C.; Young, I.S.; Cardwell, C.R.; Woodside, J.V. The Effect of Increasing Fruit and Vegetable Consumption on Overall Diet: A Systematic Review and Meta-analysis. Crit. Rev. Food Sci. Nutr. 2016, 56, 802–816. [Google Scholar]
- Fulton, S.L.; McKinley, M.C.; Neville, C.E.; Baldrick, F.R.; Mulligan, C.; McCall, D.O.; McCance, D.R.; Edgar, J.D.; Elborn, J.S.; Young, I.S.; et al. The effect of increased fruit and vegetable consumption on selected macronutrient and micronutrient intakes in four randomised-controlled. Br. J. Nutr. 2017, 117, 1270–1278. [Google Scholar] [CrossRef] [Green Version]
- Kaiser, K.A.; Brown, A.W.; Bohan Brown, M.M.; Shikany, J.M.; Mattes, R.D.; Allison, D.B. Increased fruit and vegetable intake has no discernible effect on weight loss: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2014, 100, 567–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kopf, J.C.; Suhr, M.J.; Clarke, J.; Eyun, S.-I.; Riethoven, J.-J.M.; Ramer-Tait, A.E.; Rose, D.J. Role of whole grains versus fruits and vegetables in reducing subclinical inflammation and promoting gastrointestinal health in individuals affected by overweight and obesity: A randomized controlled trial. Nutr. J. 2018, 17, 72. [Google Scholar]
- McEvoy, C.T.; Wallace, I.R.; Hamill, L.L.; Hunter, S.J.; Neville, C.E.; Patterson, C.C.; Woodside, J.V.; Young, I.S.; McKinley, M.C. Increasing Fruit and Vegetable Intake Has No Dose-Response Effect on Conventional Cardiovascular Risk Factors in Overweight Adults at High Risk of Developing Cardiovascular Disease. J. Nutr. 2015, 145, 1464–1471. [Google Scholar] [CrossRef] [Green Version]
- Valentine, R.J.; Vieira, V.J.; Woods, J.A.; Evans, E.M. Stronger relationship between central adiposity and C-reactive protein in older women than men. Menopause 2009, 16, 84–89. [Google Scholar] [PubMed]
- McCall, D.O.; McGartland, C.P.; McKinley, M.C.; Patterson, C.C.; Sharpe, P.; McCance, D.R.; Young, I.S.; Woodside, J.V. Dietary intake of fruits and vegetables improves microvascular function in hypertensive subjects in a dose-dependent manner. Circulation 2009, 119, 2153–2160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rallidis, L.S.; Lekakis, J.; Kolomvotsou, A.; Zampelas, A.; Vamvakou, G.; Efstathiou, S.; Dimitriadis, G.; Raptis, S.A.; Kremastinos, D.T. Close adherence to a Mediterranean diet improves endothelial function in subjects with abdominal obesity. Am. J. Clin. Nutr. 2009, 90, 263–268. [Google Scholar] [PubMed]
- Van Duyn, M.A.; Pivonka, E. Overview of the health benefits of fruit and vegetable consumption for the dietetics professional: Selected literature. J. Am. Diet. Assoc. 2000, 100, 1511–1521. [Google Scholar]
- Johansson, I.; Van Guelpen, B.; Hultdin, J.; Johansson, M.; Hallmans, G.; Stattin, P. Validity of food frequency questionnaire estimated intakes of folate and other B vitamins in a region without folic acid fortification. Eur. J. Clin. Nutr. 2010, 64, 905–913. [Google Scholar] [PubMed] [Green Version]
- Xinying, P.X.; Noakes, M.; Keogh, J. Can a food frequency questionnaire be used to capture dietary intake data in a 4 week clinical intervention trial? Asia Pac. J. Clin. Nutr. 2004, 13, 318–323. [Google Scholar] [PubMed]
- Thomson, C.A.; Giuliano, A.; Rock, C.L.; Ritenbaugh, C.K.; Flatt, S.W.; Faerber, S.; Newman, V.; Caan, B.; Graver, E.; Hartz, V.; et al. Measuring Dietary Change in a Diet Intervention Trial: Comparing Food Frequency Questionnaire and Dietary Recalls. Am. J. Epidemiol. 2003, 157, 754–762. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| FV | CON | |||
|---|---|---|---|---|
| Men | Women | Men | Women | |
| (n = 16) | (n = 17) | (n = 14) | (n = 19) | |
| Weight (kg) | 91.7 ± 11.7 | 69.3 ± 7.2 | 87.8 ± 7.8 | 71.9 ± 5.6 |
| Height (cm) | 181 ± 7 | 164 ± 6.6 | 179 ± 7.5 | 166 ± 4.5 |
| BMI (kg/m2) | 27.9 ± 3.1 | 25.9 ± 2.8 | 27.5 ± 2.1 | 26.2 ± 1.9 |
| Waist circumference (cm) | 103 ± 9.4 | 86 ± 4.7 | 102 ± 5.7 | 87 ± 5.5 |
| Before Intervention | During Intervention | |||
|---|---|---|---|---|
| FV | CON | FV | CON | |
| Fruit and vegetable (servings/day) | 2.2 ± 1.3 | 2.2 ± 1.4 | 4.2 ± 1.8 * | 2.6 ± 1.6 |
| PRE | POST | |||
|---|---|---|---|---|
| FV | CON | FV | CON | |
| Total energy (kcal) | 1699 ± 427 | 1816 ± 544 | 1861 ± 474 * | 1797 ± 523 |
| Carbohydrates (g) | 166 ± 46 | 180 ± 59 | 197 ± 63 * | 174 ± 52 |
| Fiber (g) | 23 ± 10 | 26 ± 11 | 29 ± 12 * | 26 ± 10 |
| Protein (g) | 68 ± 19 | 71 ± 23 | 73 ± 20 | 71 ± 22 |
| Fat (g) | 77 ± 24 | 82 ± 28 | 79 ± 25 | 81 ± 29 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nilsson, A.; Cano, A.; Bergens, O.; Kadi, F. Randomized Controlled Trial for Promotion of Healthy Eating in Older Adults by Increasing Consumption of Plant-Based Foods: Effect on Inflammatory Biomarkers. Nutrients 2021, 13, 3753. https://doi.org/10.3390/nu13113753
Nilsson A, Cano A, Bergens O, Kadi F. Randomized Controlled Trial for Promotion of Healthy Eating in Older Adults by Increasing Consumption of Plant-Based Foods: Effect on Inflammatory Biomarkers. Nutrients. 2021; 13(11):3753. https://doi.org/10.3390/nu13113753
Chicago/Turabian StyleNilsson, Andreas, Antonio Cano, Oscar Bergens, and Fawzi Kadi. 2021. "Randomized Controlled Trial for Promotion of Healthy Eating in Older Adults by Increasing Consumption of Plant-Based Foods: Effect on Inflammatory Biomarkers" Nutrients 13, no. 11: 3753. https://doi.org/10.3390/nu13113753
APA StyleNilsson, A., Cano, A., Bergens, O., & Kadi, F. (2021). Randomized Controlled Trial for Promotion of Healthy Eating in Older Adults by Increasing Consumption of Plant-Based Foods: Effect on Inflammatory Biomarkers. Nutrients, 13(11), 3753. https://doi.org/10.3390/nu13113753