
A Cross-Sectional Study of the Street Foods Purchased by Customers in Urban Areas of Central Asia

 , ,
, ,  ,
,  ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
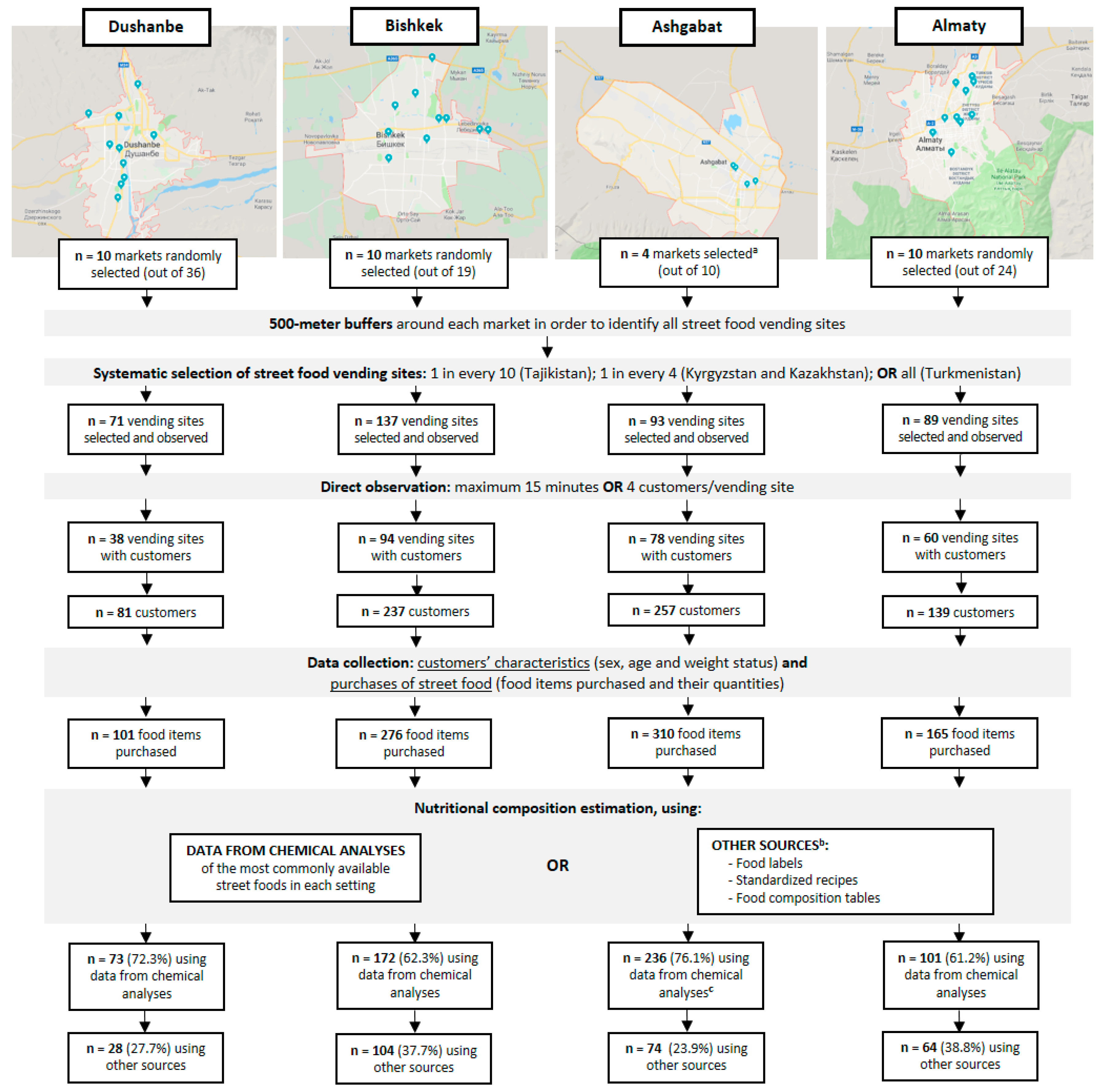
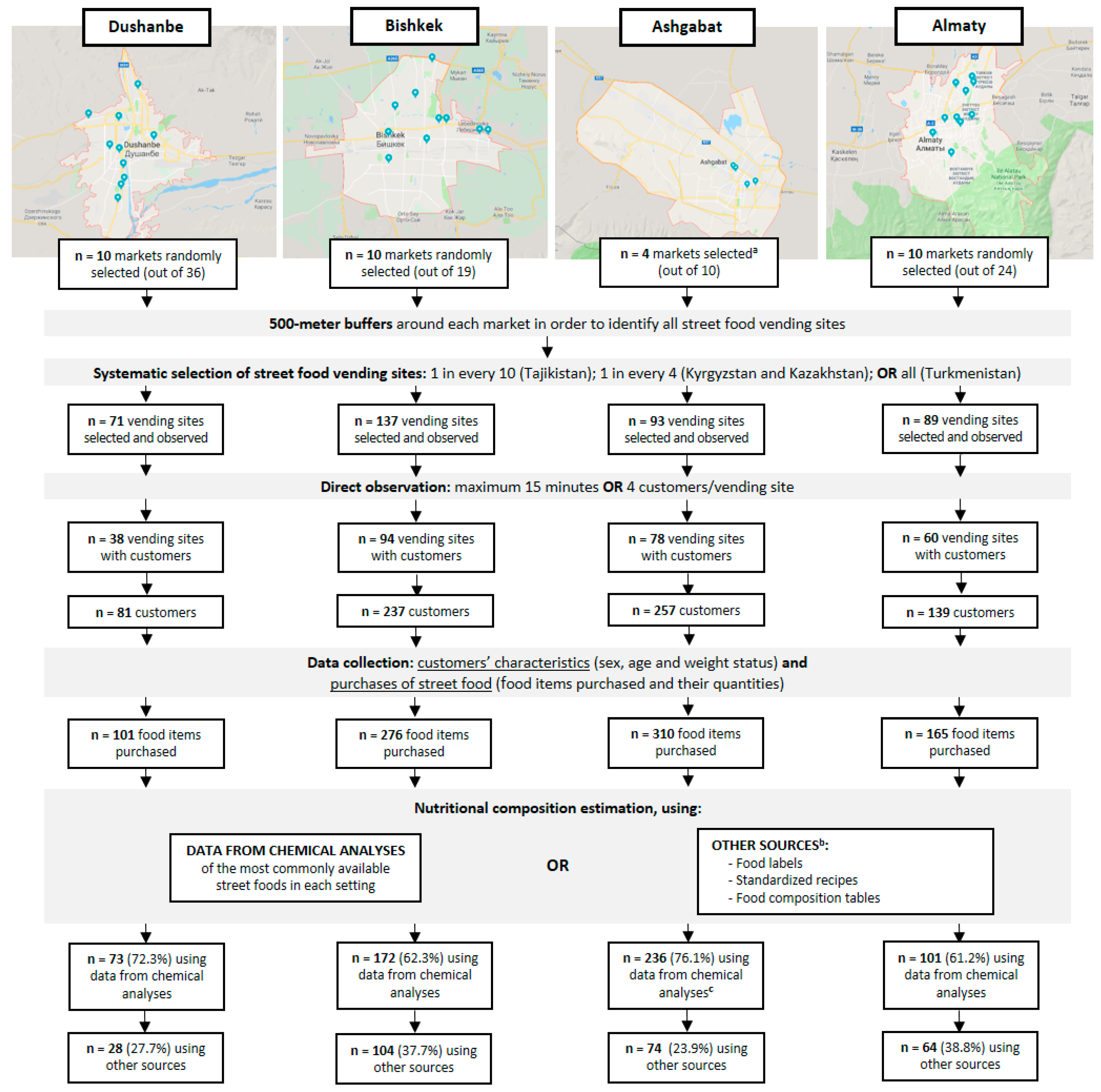
2.2. Sampling Procedure
2.3. Data Collection
2.4. Nutritional Composition Estimation
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Noncommunicable Diseases: Key Facts [Web Page]. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 21 December 2019).
- World Health Organization. Noncommunicable Diseases Country Profiles; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Food and Agriculture Organization. Europe and Central Asia Regional Overview of Food Security and Nutrition; Food and Agriculture Organization of the United Nations: Budapest, Hungary, 2019. [Google Scholar]
- Popkin, B.M. Global nutrition dynamics: The world is shifting rapidly toward a diet linked with noncommunicable diseases. Am. J. Clin. Nutr. 2006, 84, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M. Contemporary nutritional transition: Determinants of diet and its impact on body composition. Proc. Nutr. Soc. 2011, 70, 82–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, M. The Nutrition Transition in Developing Asia: Dietary Change, Drivers and Health Impacts. In Eating, Drinking: Surviving: The International Year of Global Understanding—IYGU.; Jackson, P., Spiess, W.E.L., Sultana, F., Eds.; Springer International Publishing: Cham, Switzerland, 2016; pp. 83–90. [Google Scholar] [CrossRef] [Green Version]
- Popkin, B.M. Urbanization, Lifestyle Changes and the Nutrition Transition. World Dev. 1999, 27, 1905–1916. [Google Scholar] [CrossRef]
- Fellows, P.; Hilmi, M. Selling Street and Snack Foods; Rural Infrastructure and Agro-Industries Division of the Food and Agriculture Organization of the United Nations: Rome, Italy, 2012. [Google Scholar]
- Steyn, N.P.; McHiza, Z.; Hill, J.; Davids, Y.D.; Venter, I.; Hinrichsen, E.; Opperman, M.; Rumbelow, J.; Jacobs, P. Nutritional contribution of street foods to the diet of people in developing countries: A systematic review. Public Health Nutr. 2014, 17, 1363–1374. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. FEEDcities Project: The Food Environment Description in Cities in Eastern Europe and Central Asia—Kyrgyzstan; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2017. [Google Scholar]
- World Health Organization. FEEDcities Project: The Food ENVIRONMENT description in Cities in Eastern Europe and Central Asia—Tajikistan; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2017. [Google Scholar]
- World Health Organization. FEEDcities Project: The Food Environment Description in Cities in Eastern Europe and Central Asia—Turkmenistan; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2019. [Google Scholar]
- World Health Organization. FEEDcities Project: The Food Environment Description in Cities in Eastern Europe and Central Asia—Kazakhstan; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2019. [Google Scholar]
- Abrahale, K.; Sousa, S.; Albuquerque, G.; Padrao, P.; Lunet, N. Street food research worldwide: A scoping review. J. Hum. Nutr. Diet. Off. J. Br. Diet. Assoc. 2018. [Google Scholar] [CrossRef]
- United Nations. Urbanization in Central Asia: Challenges, Issues and Prospects; Center for Economic Research, United Nations Economic and Social Commission for Asia and the Pacific and United Nations Development Programme: Tashkent, Uzbekistan, 2013. [Google Scholar]
- Lunet, N.; Gelormini, M.; Jewell, J.; Morais, I.; Albuquerque, G.; Sousa, S.; Damasceno, A.; Casal, S.; Pinho, O.; Moreira, P.; et al. FEEDcities Project—A Comprehensive Characterization of the Street Food Environment in Cities; World Health Organization: Copenhagen, Denmark, 2019. [Google Scholar]
- Food and Agriculture Organization. Food and Nutrition Paper No. 46. Street Foods: Report of an FAO Expert Consultation, Jogjakarta, Indonesia. 5–9 December 1988; Food and Agriculture Organization: Jogjakarta, Indonesia, 1989. [Google Scholar]
- World Health Organization. Essential Safety Requirements for Street-Vended Foods; Food Safety Unit, Division of Food and Nutrition, World Health Organization: Geneva, Switzerland, 1996. [Google Scholar]
- Albuquerque, G.; Lança de Morais, I.; Gelormini, M.; Sousa, S.; Casal, S.; Pinho, O.; Moreira, P.; Breda, J.; Lunet, N.; Padrão, P. Macronutrient composition of street food in Central Asia: Bishkek, Kyrgyzstan. Food Sci. Nutr. 2020, 8, 5309–5320. [Google Scholar] [CrossRef]
- Albuquerque, G.; Morais, I.; Gelormini, M.; Casal, S.; Damasceno, A.; Pinho, O.; Moreira, P.; Jewell, J.; Breda, J.; Lunet, N.; et al. Street food in Dushanbe, Tajikistan: Availability and nutritional value. Br. J. Nutr. 2019, 122, 1052–1061. [Google Scholar] [CrossRef] [Green Version]
- Harris, C.V.; Bradlyn, A.S.; Coffman, J.; Gunel, E.; Cottrell, L. BMI-based body size guides for women and men: Development and validation of a novel pictorial method to assess weight-related concepts. Int. J. Obes. 2008, 32, 336–342. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Regional Office for Europe Nutrient Profile Model.; WHO Regional Office for Europe: Copenhagen, Denmark, 2015. [Google Scholar]
- AOAC International. Official Methods of Analysis of AOAC International, 20th ed.; AOAC International: Gaithersburg, MD, USA, 2016. [Google Scholar]
- Hussain, T. Food Composition Table for Pakistan, Revised edition; Ministry of Planning and Development. Government of Pakistan: Islamabad, Pakistan, 2001. [Google Scholar]
- Ministry of Food Agriculture and Livestock of Turkey. TürKomp National Food Composition Database. Available online: http://www.turkomp.gov.tr/ (accessed on 13 September 2018).
- World Health Organization. WHO Technical Report Series 916. Diet, Nutrition and the Prevention of Chronic Diseases: Report of a Joint WHO/FAO Expert Consultation; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Uauy, R.; Aro, A.; Clarke, R.; Ghafoorunissa; L’Abbé, M.R.; Mozaffarian, D.; Skeaff, C.M.; Stender, S.; Tavella, M. WHO Scientific Update on trans fatty acids: Summary and conclusions. Eur. J. Clin. Nutr. 2009, 63, S68. [Google Scholar] [CrossRef]
- World Health Organization. Guideline: Sodium Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- World Health Organization. Guideline: Potassium Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Popkin, B.M.; Adair, L.S.; Ng, S.W. Global nutrition transition and the pandemic of obesity in developing countries. Nutr. Rev. 2012, 70, 3–21. [Google Scholar] [CrossRef] [Green Version]
- Monteiro, C.A.; Moubarac, J.C.; Cannon, G.; Ng, S.W.; Popkin, B. Ultra-processed products are becoming dominant in the global food system. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2013, 14 (Suppl. 2), 21–28. [Google Scholar] [CrossRef]
- Martinez Steele, E.; Popkin, B.M.; Swinburn, B.; Monteiro, C.A. The share of ultra-processed foods and the overall nutritional quality of diets in the US: Evidence from a nationally representative cross-sectional study. Popul. Health Metr. 2017, 15, 6. [Google Scholar] [CrossRef] [Green Version]
- Louzada, M.; Ricardo, C.Z.; Steele, E.M.; Levy, R.B.; Cannon, G.; Monteiro, C.A. The share of ultra-processed foods determines the overall nutritional quality of diets in Brazil. Public Health Nutr. 2018, 21, 94–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poti, J.M.; Braga, B.; Qin, B. Ultra-processed Food Intake and Obesity: What Really Matters for Health-Processing or Nutrient Content? Curr. Obes. Rep. 2017, 6, 420–431. [Google Scholar] [CrossRef]
- Rauber, F.; da Costa Louzada, M.L.; Steele, E.M.; Millett, C.; Monteiro, C.A.; Levy, R.B. Ultra-Processed Food Consumption and Chronic Non-Communicable Diseases-Related Dietary Nutrient Profile in the UK (2008(-)2014). Nutrients 2018, 10, 587. [Google Scholar] [CrossRef] [Green Version]
- Juul, F.; Martinez-Steele, E.; Parekh, N.; Monteiro, C.A.; Chang, V.W. Ultra-processed food consumption and excess weight among US adults. Br. J. Nutr. 2018, 120, 90–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nago, E.S.; Lachat, C.K.; Huybregts, L.; Roberfroid, D.; Dossa, R.A.; Kolsteren, P.W. Food, energy and macronutrient contribution of out-of-home foods in school-going adolescents in Cotonou, Benin. Br. J. Nutr. 2010, 103, 281–288. [Google Scholar] [CrossRef] [Green Version]
- Namugumya, B.S.; Muyanja, C. Contribution of street foods to the dietary needs of street food vendors in Kampala, Jinja and Masaka districts, Uganda. Public Health Nutr. 2012, 15, 1503–1511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sousa, S.; Gelormini, M.; Damasceno, A.; Lopes, S.A.; Malo, S.; Chongole, C.; Muholove, P.; Casal, S.; Pinho, O.; Moreira, P.; et al. Street food in Maputo, Mozambique: Availability and nutritional value of homemade foods. Nutr. Health 2019, 25, 37–46. [Google Scholar] [CrossRef]
- Gupta, V.; Downs, S.M.; Ghosh-Jerath, S.; Lock, K.; Singh, A. Unhealthy Fat in Street and Snack Foods in Low-Socioeconomic Settings in India: A Case Study of the Food Environments of Rural Villages and an Urban Slum. J. Nutr. Educ. Behav. 2016, 48, 269–279.e261. [Google Scholar] [CrossRef] [Green Version]
- de Souza, R.J.; Mente, A.; Maroleanu, A.; Cozma, A.I.; Ha, V.; Kishibe, T.; Uleryk, E.; Budylowski, P.; Schunemann, H.; Beyene, J.; et al. Intake of saturated and trans unsaturated fatty acids and risk of all cause mortality, cardiovascular disease, and type 2 diabetes: Systematic review and meta-analysis of observational studies. BMJ (Clin. Res. Ed.) 2015, 351, h3978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Eliminating Trans. Fats in Europe. A Policy Brief; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2015. [Google Scholar]
- Eurasian Economic Commission. Technical Regulation on Butter and Fat Products—TP TC 024/2011; Eurasian Economic Commission: Moscow, Russia, 2011. (In Russian) [Google Scholar]
- Lanca de Morais, I.; Lunet, N.; Albuquerque, G.; Gelormini, M.; Casal, S.; Damasceno, A.; Pinho, O.; Moreira, P.; Jewell, J.; Breda, J.; et al. The Sodium and Potassium Content of the Most Commonly Available Street Foods in Tajikistan and Kyrgyzstan in the Context of the FEEDCities Project. Nutrients 2018, 10, 98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sousa, S.; Damasceno, A.; Gelormini, M.; Jessen, N.; Lunet, N.; Padrao, P. Powdered chicken stock may be an important source of dietary sodium intake in Maputo, Mozambique. J. Public Health 2018, 40, 659–660. [Google Scholar] [CrossRef]
- Kurlansky, M. Salt: A World History; Vintage Books: London, UK, 2003. [Google Scholar]
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; Amann, M.; Anderson, H.R.; Andrews, K.G.; Aryee, M.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef] [Green Version]
- Whelton, P.K.; Appel, L.J.; Sacco, R.L.; Anderson, C.A.; Antman, E.M.; Campbell, N.; Dunbar, S.B.; Frohlich, E.D.; Hall, J.E.; Jessup, M.; et al. Sodium, blood pressure, and cardiovascular disease: Further evidence supporting the American Heart Association sodium reduction recommendations. Circulation 2012, 126, 2880–2889. [Google Scholar] [CrossRef] [Green Version]
- D’Elia, L.; Barba, G.; Cappuccio, F.P.; Strazzullo, P. Potassium intake, stroke, and cardiovascular disease a meta-analysis of prospective studies. J. Am. Coll. Cardiol. 2011, 57, 1210–1219. [Google Scholar] [CrossRef]
- Connor Gorber, S.; Tremblay, M.; Moher, D.; Gorber, B. A comparison of direct vs. self-report measures for assessing height, weight and body mass index: A systematic review. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2007, 8, 307–326. [Google Scholar] [CrossRef]
- Malik, V.S.; Pan, A.; Willett, W.C.; Hu, F.B. Sugar-sweetened beverages and weight gain in children and adults: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2013, 98, 1084–1102. [Google Scholar] [CrossRef] [Green Version]
- Malik, V.S.; Popkin, B.M.; Bray, G.A.; Despres, J.P.; Willett, W.C.; Hu, F.B. Sugar-sweetened beverages and risk of metabolic syndrome and type 2 diabetes: A meta-analysis. Diabetes Care 2010, 33, 2477–2483. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Total n = 714 | Dushanbe n = 81 | Bishkek n = 237 | Ashgabat n = 257 | Almaty n = 139 | p | |
|---|---|---|---|---|---|---|
| n (%) | ||||||
| Sex | ||||||
| Male | 310 (43.4) | 53 (34.6) | 96 (40.5) | 119 (46.3) | 42 (30.2) | <0.001 |
| Female | 404 (56.6) | 28 (65.4) | 141 (59.5) | 138 (53.7) | 97 (69.8) | |
| Age a | ||||||
| <35 years | 286 (44.5) | 38 (56.7) | 101 (47.9) | 97 (41.8) | 50 (37.9) | 0.045 |
| ≥35 years | 356 (55.5) | 29 (43.3) | 110 (52.1) | 135 (58.2) | 82 (62.1) | |
| Weight status a | ||||||
| Underweight/normal weight | 503 (76.7) | 52 (76.5) | 178 (82.8) | 178 (73.6) | 95 (72.5) | 0.069 |
| Overweight/obesity | 153 (23.3) | 16 (23.5) | 37 (17.2) | 64 (26.4) | 36 (27.5) | |
| Number of items purchased | ||||||
| 1 (median) | 595 (83.3) | 66 (81.5) | 203 (85.7) | 213 (82.9) | 113 (81.3) | 0.666 |
| >1 | 119 (16.7) | 15 (18.5) | 34 (14.3) | 44 (17.1) | 26 (18.7) | |
| Purchased foods or beverages? | ||||||
| Only foods | 493 (69.1) | 55 (67.9) | 131 (55.3) | 222 (86.4) | 85 (61.2) | <0.001 |
| Only beverages | 150 (21.0) | 19 (23.5) | 79 (33.3) | 15 (5.8) | 37 (26.6) | |
| Foods and beverages | 71 (9.9) | 7 (8.6) | 27 (11.4) | 20 (7.8) | 17 (12.2) | |
| Purchased homemade or industrial? | ||||||
| Only homemade | 486 (68.1) | 58 (71.6) | 175 (73.8) | 174 (67.7) | 79 (56.8) | 0.003 |
| Only industrial | 201 (28.1) | 23 (28.4) | 58 (24.5) | 71 (27.6) | 49 (35.3) | |
| Homemade and industrial | 27 (3.8) | 0 (0.0) | 4 (1.7) | 12 (4.7) | 11 (7.9) | |
| Total (n = 564 a) | Dushanbe (n = 62 a) | Bishkek (n = 158 a) | Ashgabat (n = 242 a) | Almaty (n = 102 a) | p | |
|---|---|---|---|---|---|---|
| Median (P25–P75) | ||||||
| Amount purchased (g) | 120 (95–278) | 120 (58–281) | 176 (100–306) | 120 (99–265) | 103 (90–296) | 0.062 |
| Per total purchase | ||||||
| Energy (kcal) | 529 (329–850) | 352 (311–816) | 451 (314–615) | 568 (343–993) | 557 (326–915) | <0.001 |
| Protein (g) | 13.4 (8.5–25.6) | 12.7 (8.6–23.7) | 18.1 (10.6–23.4) | 13.2 (7.2–29.7) | 13.5 (7.0–25.5) | 0.267 |
| CHO (g) | 68.1 (42.6–107.6) | 69.1 (33.0–91.3) | 60.0 (44.7–73.9) | 70.5 (54.5–130.3) | 69.5 (40.3–101.8) | <0.001 |
| Total fat (g) | 20.1 (5.3–32.6) | 11.1 (0.9–25.6) | 16.2 (5.3–28.8) | 22.8 (9.0–44.4) | 21.5 (7.9–40.5) | <0.001 |
| SFA (g) b | 4.7 (1.2–12.4) | 2.5 (0.5–9.9) | 3.4 (1.1–12.3) | 9.0 (1.1–15.7) | 4.6 (1.7–11.1) | <0.001 |
| MUFA (g) b | 5.3 (1.6–9.4) | 3.7 (0.3–7.9) | 3.8 (1.4–9.3) | 5.9 (2.0–11.3) | 5.3 (2.5–10.7) | <0.001 |
| PUFA (g) b | 5.0 (1.3–9.1) | 2.9 (0.2–9.6) | 4.0 (0.7–7.8) | 6.5 (1.7–9.8) | 4.2 (1.9–8.9) | <0.001 |
| n−6 (g) b | 4.3 (1.2–8.6) | 2.7 (0.2–8.8) | 3.9 (0.6–7.6) | 6.3 (1.4–9.5) | 3.6 (1.9–8.9) | <0.001 |
| n−3 (g) b | 0.1 (0.0–0.2) | 0.0 (0.0–0.1) | 0.1 (0.0–0.4) | 0.1 (0.1–0.3) | 0.1 (0.0–0.2) | 0.002 |
| TFA (g) b | 0.36 (0.06–0.86) | 0.08 (0.02–0.38) | 0.29 (0.02–1.38) | 0.36 (0.06–0.55) | 0.60 (0.20–2.14) | <0.001 |
| Na (mg) c | 745 (475–1783) | 723 (479–1708) | 861 (561–1411) | 851 (477–2314) | 681 (316–2085) | 0.209 |
| K (mg) d | 304 (180–713) | 226 (121–527) | 282 (149–571) | 414 (245–850) | 288 (174–651) | <0.001 |
| Per 100 g of purchase | ||||||
| Energy (kcal) | 308 (212–605) | 274 (174–484) | 275 (158–419) | 432 (276–663) | 315 (212–621) | <0.001 |
| Protein (g) | 10.6 (5.5–17.2) | 10.0 (6.0–14.1) | 10.6 (5.5–14.8) | 11.0 (5.4–19.5) | 8.9 (5.6–16.9) | 0.154 |
| CHO (g) | 53.5 (25.2–74.8) | 49.9 (25.2–58.9) | 31.0 (17.3–57.6) | 56.8 (29.6–108.9) | 42.8 (30.2–75.2) | <0.001 |
| Total fat (g) | 10.1 (3.3–22.7) | 5.2 (1.8–14.9) | 7.7 (2.3–14.9) | 17.3 (4.1–30.1) | 11.4 (4.7–24.1) | <0.001 |
| SFA (g) b | 2.7 (0.7–7.2) | 1.8 (0.7–4.3) | 2.1 (0.4–5.2) | 3.9 (0.7–11.0) | 2.7 (1.4–7.9) | <0.001 |
| MUFA (g) b | 2.8 (0.9–6.8) | 1.5 (0.6–4.7) | 2.2 (0.7–3.9) | 4.1 (1.2–9.6) | 3.2 (1.4–6.8) | <0.001 |
| PUFA (g) b | 2.7 (1.1–6.4) | 1.5 (0.3–5.0) | 1.5 (0.8–3.8) | 3.6 (1.3–7.1) | 3.7 (1.5–6.7) | <0.001 |
| n−6 (g) b | 2.7 (1.0–6.0) | 1.3 (0.3–4.1) | 1.4 (0.7–3.4) | 3.5 (1.2–6.7) | 3.6 (1.2–6.5) | <0.001 |
| n−3 (g) b | 0.1 (0.0–0.2) | 0.0 (0.0–0.1) | 0.1 (0.0–0.1) | 0.1 (0.0–0.2) | 0.1 (0.0–0.2) | <0.001 |
| TFA (g) b | 0.21 (0.05–0.51) | 0.08 (0.03–0.15) | 0.22 (0.02–0.55) | 0.21 (0.04–0.46) | 0.32 (0.18–1.45) | <0.001 |
| Na (mg) c | 514 (411–1042) | 467 (348–657) | 508 (325–740) | 611 (467–1216) | 519 (324–1027) | 0.005 |
| K (mg) d | 247 (150–474) | 145 (114–250) | 205 (124–303) | 328 (150–631) | 286 (166–461) | <0.001 |
| Na/K ratio d | 4.7 (2.7–6.3) | 6.6 (4.1–8.0) | 5.2 (3.1–8.7) | 4.4 (2.6–5.6) | 4.3 (2.3–5.6) | <0.001 |
| Sex | Age | Weight Status | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Male (n = 242 a) | Female (n = 322 a) | p | <35 years (n = 226 a) | ≥35 years (n = 281 a) | p | Underweight /Normal Weight (n = 398 a) | Overweight /Obesity (n = 122 a) | p | |
| Median (P25–P75) | Median (P25–P75) | Median (P25–P75) | |||||||
| Amount purchased (g) | 120 (96–317) | 120 (90–265) | 0.051 | 132 (96–296) | 120 (68.1–265.0) | 0.029 | 120 (96–278) | 120 (81–265) | 0.411 |
| Per total purchase | |||||||||
| Energy (kcal) | 555 (337–930) | 509 (311–717) | 0.018 | 500 (327–893) | 557 (329–750) | 0.957 | 488 (324–730) | 570 (343–978) | 0.020 |
| Protein (g) | 15.9 (9.6–30.7) | 13.2 (7.6–13.2) | 0.004 | 15.3 (8.6–26.2) | 13.2 (8.5–24.2) | 0.292 | 13.2 (8.5–24.2) | 13.6 (8.5–26.2) | 0.529 |
| CHO (g) | 68.1 (45.1–122.3) | 68.1 (40.5–100.1) | 0.271 | 68.1 (41.5–118.3) | 68.1 (42.8–100.1) | 0.992 | 68.1 (41.5–100.1) | 72.3 (49.3–122.3) | 0.051 |
| Total fat (g) | 22.8 (6.5–35.2) | 16.0 (5.3–30.9) | 0.002 | 20.9 (7.6–35.1) | 18.5 (5.2–31.8) | 0.317 | 19.4 (5.3–31.2) | 22.8 (6.3–43.9) | 0.006 |
| SFA (g) b | 7.3 (1.5–12.8) | 3.2 (1.1–11.1) | 0.025 | 5.8 (1.5–12.3) | 3.7 (1.0–12.3) | 0.149 | 4.6 (1.1–12.3) | 4.6 (1.3–12.8) | 0.475 |
| MUFA (g) b | 6.3 (1.7–9.7) | 4.4 (1.5–9.3) | 0.041 | 5.9 (1.9–9.5) | 4.4 (1.1–9.3) | 0.119 | 4.9 (1.6–9.3) | 5.7 (1.5–11.0) | 0.237 |
| PUFA (g) b | 5.6 (1.3–9.5) | 4.5 (1.3–8.4) | 0.429 | 5.6 (1.4–9.6) | 4.0 (1.3–8.3) | 0.111 | 4.5 (1.3–9.1) | 5.2 (1.4–9.6) | 0.441 |
| n−6 (g) b | 4.7 (1.2–9.0) | 4.2 (1.3–8.3) | 0.559 | 5.1 (1.2–9.5) | 3.5 (1.2–7.6) | 0.126 | 4.3 (1.2–8.4) | 3.9 (1.4–9.5) | 0.471 |
| n−3 (g) b | 0.1 (0.1–0.3) | 0.1 (0.0–0.2) | 0.105 | 0.1 (0.1–0.3) | 0.1 (0.0–0.2) | 0.120 | 0.1 (0.0–0.2) | 0.1 (0.0–0.3) | 0.891 |
| TFA (g) b | 0.38 (0.05–1.15) | 0.31 (0.06–0.67) | 0.002 | 0.38 (0.11–0.86) | 0.32 (0.03–0.76) | 0.036 | 0.31 (0.05–0.73) | 0.40 (0.06–1.00) | 0.025 |
| Na (mg) c | 906 (560–2165) | 672 (470–1687) | 0.030 | 1062 (560–1943) | 561 (416–1653) | 0.001 | 753 (470–1750) | 709 (470–2042) | 0.937 |
| K (mg) d | 343 (180–718) | 291 (180–691) | 0.239 | 340 (180–777) | 250 (175–648) | 0.078 | 313 (180–691) | 288 (180–778) | 0.931 |
| Per 100 g of purchase | |||||||||
| Energy (kcal) | 286 (210–552) | 314 (212–638) | 0.370 | 287 (185–531) | 314 (228–663) | 0.016 | 306 (210–552) | 382 (253–674) | 0.025 |
| Protein (g) | 10.6 (5.5–17.1) | 10.6 (5.5–17.4) | 0.929 | 8.7 (5.2–15.0) | 11.0 (6.4–18.2) | 0.003 | 10.6 (5.4–17.1) | 10.8 (6.5–19.5) | 0.132 |
| CHO (g) | 53.5 (24.2–67.4) | 53.1 (25.5–77.1) | 0.325 | 40.2 (20.6–63.7) | 56.8 (26.3–106.9) | <0.001 | 50.9 (22.7–70.5) | 56.8 (29.6–101.8) | 0.030 |
| Total fat (g) | 9.3 (3.5–24.1) | 10.8 (3.2–20.1) | 0.926 | 10.0 (3.7–20.9) | 10.0 (3.3–24.0) | 0.554 | 10.0 (2.5–20.1) | 13.2 (4.3–30.1) | 0.065 |
| SFA (g) b | 3.2 (0.7–9.0) | 2.6 (0.7–7.0) | 0.277 | 3.0 (1.3–7.1) | 2.6 (0.7–8.9) | 0.438 | 2.7 (0.7–7.1) | 2.7 (0.7–10.9) | 0.322 |
| MUFA (g) b | 2.6 (0.9–7.4) | 3.0 (0.9–6.1) | 0.619 | 2.8 (1.1–6.4) | 2.5 (0.7–7.1) | 0.971 | 2.8 (0.8–6.3) | 3.4 (1.1–10.7) | 0.111 |
| PUFA (g) b | 2.6 (1.1–5.6) | 3.0 (1.1–6.6) | 0.645 | 2.6 (0.9–5.4) | 2.7 (1.1–6.4) | 0.229 | 2.6 (1.1–5.8) | 3.8 (1.3–6.6) | 0.023 |
| n−6 (g) b | 2.5 (1.0–5.3) | 2.7 (1.0–6.5) | 0.572 | 2.4 (0.8–5.0) | 2.7 (1.0–6.3) | 0.243 | 2.5 (0.9–5.6) | 3.3 (1.2–6.6) | 0.032 |
| n−3 (g) b | 0.1 (0.0–0.2) | 0.1 (0.0–0.1) | 0.210 | 0.1 (0.0–0.1) | 0.1 (0.0–0.2) | 0.773 | 0.1 (0.0–0.1) | 0.1 (0.0–0.2) | 0.368 |
| TFA (g) b | 0.21 (0.04–0.57) | 0.20 (0.05–0.48) | 0.752 | 0.21 (0.08–0.46) | 0.19 (0.03–0.52) | 0.593 | 0.21 (0.05–0.46) | 0.25 (0.04–0.76) | 0.219 |
| Na (mg) c | 505 (412–1042) | 521 (411–1065) | 0.980 | 484 (345–1064) | 525 (435–1042) | 0.377 | 490 (388–1042) | 620 (467–1136) | 0.045 |
| K (mg) d | 246 (145–500) | 249 (150–461) | 0.337 | 244 (145–474) | 264 (150–461) | 0.266 | 244 (150–454) | 305 (166–500) | 0.060 |
| Na/K ratio d | 5.3 (3.1–6.3) | 4.3 (2.6–5.9) | 0.141 | 5.3 (2.7–6.6) | 4.2 (3.0–5.8) | 0.046 | 4.9 (2.6–6.3) | 4.2 (3.0–5.8) | 0.604 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sousa, S.; Morais, I.L.d.; Albuquerque, G.; Gelormini, M.; Casal, S.; Pinho, O.; Motta, C.; Damasceno, A.; Moreira, P.; Breda, J.; et al. A Cross-Sectional Study of the Street Foods Purchased by Customers in Urban Areas of Central Asia. Nutrients 2021, 13, 3651. https://doi.org/10.3390/nu13103651
Sousa S, Morais ILd, Albuquerque G, Gelormini M, Casal S, Pinho O, Motta C, Damasceno A, Moreira P, Breda J, et al. A Cross-Sectional Study of the Street Foods Purchased by Customers in Urban Areas of Central Asia. Nutrients. 2021; 13(10):3651. https://doi.org/10.3390/nu13103651
Chicago/Turabian StyleSousa, Sofia, Inês Lança de Morais, Gabriela Albuquerque, Marcello Gelormini, Susana Casal, Olívia Pinho, Carla Motta, Albertino Damasceno, Pedro Moreira, João Breda, and et al. 2021. "A Cross-Sectional Study of the Street Foods Purchased by Customers in Urban Areas of Central Asia" Nutrients 13, no. 10: 3651. https://doi.org/10.3390/nu13103651
APA StyleSousa, S., Morais, I. L. d., Albuquerque, G., Gelormini, M., Casal, S., Pinho, O., Motta, C., Damasceno, A., Moreira, P., Breda, J., Lunet, N., & Padrão, P. (2021). A Cross-Sectional Study of the Street Foods Purchased by Customers in Urban Areas of Central Asia. Nutrients, 13(10), 3651. https://doi.org/10.3390/nu13103651