
Effects of Probiotics and Synbiotics on Weight Loss in Subjects with Overweight or Obesity: A Systematic Review



Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction and Analysis
2.4. Quality Assessment
3. Results
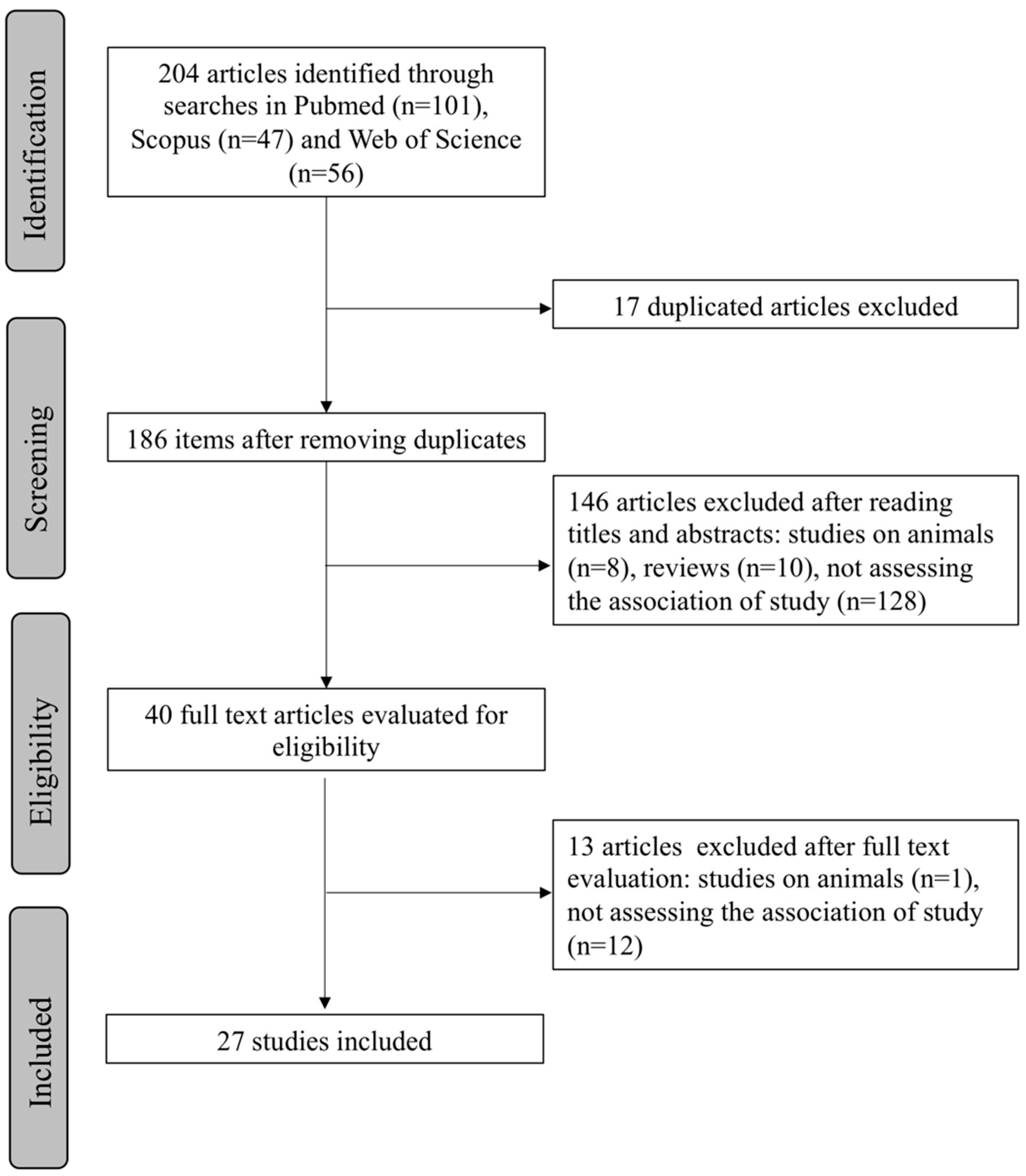
3.1. Selection Process
3.2. Study Characteristics
3.3. Probiotic Strains, Daily Doses and Total Intervention Doses
3.4. Quality Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BMI | Body Mass Index |
| CFU | Colony Forming Unit |
| Fiaf | Fasting-induced adipose factor |
| GLP | Glucagon-like peptide |
| IM | Intestinal Microbiota |
| ISAPP | International Scientific Association of Probiotics and Prebiotics |
| LAB | Lactic Acid Bacteria |
| LPS | Lipopolysaccharides |
| PPY | Pancreatic polypeptide |
| PCOS | Polycystic Ovary Syndrome |
| RCT | Randomized Controlled Trial |
| RCT-DB | Randomized Controlled Trial Double Blind |
| RCT-TB | Randomized Controlled Trial Triple Blind |
| WHO | World Health Organization |
References
- WHO. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 28 September 2021).
- Roth, G.A.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef]
- Wright, S.M.; Aronne, L.J. Causes of obesity. Abdom. Radiol. 2012, 37, 730–732. [Google Scholar] [CrossRef]
- Blüher, M. Obesity: Global epidemiology and pathogenesis. Nat. Rev. Endocrinol. 2019, 15, 288–298. [Google Scholar] [CrossRef]
- María Magdalena Farías, N.; Catalina Silva, B.; Jaime Rozowski, N. Microbiota Intestinal: Rol en Obesidad. Rev. Chil. Nutr. 2011, 38, 228–233. [Google Scholar] [CrossRef]
- Muscogiuri, G.; Cantone, E.; Cassarano, S.; Tuccinardi, D.; Barrea, L.; Savastano, S.; Colao, A. Gut microbiota: A new path to treat obesity. Int. J. Obes. Suppl. 2019, 9, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Angelakis, E.; Armougom, F.; Million, M.; Raoult, D. The relationship between gut microbiota and weight gain in humans. Future Microbiol. 2012, 7, 91–109. [Google Scholar] [CrossRef]
- Cani, P.D.; Delzenne, N.M. The Role of the Gut Microbiota in Energy Metabolism and Metabolic Disease. Curr. Pharm. Des. 2009, 15, 1546–1558. [Google Scholar] [CrossRef]
- Le Chatelier, E.; Nielsen, T.; Qin, J.; Prifti, E.; Hildebrand, F.; Falony, G.; Almeida, M.; Arumugam, M.; Batto, J.-M.; Kennedy, S.; et al. Richness of human gut microbiome correlates with metabolic markers. Nature 2013, 500, 541–546. [Google Scholar] [CrossRef]
- Million, M.; Maraninchi, M.; Henry, M.; Armougom, F.; Richet, H.; Carrieri, P.; Valero, R.; Raccah, D.; Vialettes, B.; Raoult, D. Obesity-associated gut microbiota is enriched in Lactobacillus reuteri and depleted in Bifidobacterium animalis and Methanobrevibacter smithii. Int. J. Obes. 2011, 36, 817–825. [Google Scholar] [CrossRef] [PubMed]
- Turnbaugh, P.J.; Ley, R.E.; Mahowald, M.A.; Magrini, V.; Mardis, E.R.; Gordon, J.I. An obesity-associated gut microbiome with increased capacity for energy harvest. Nat. Cell Biol. 2006, 444, 1027–1031. [Google Scholar] [CrossRef] [PubMed]
- Ley, R.E.; Bäckhed, F.; Turnbaugh, P.; Lozupone, C.A.; Knight, R.D.; Gordon, J.I. Obesity alters gut microbial ecology. Proc. Natl. Acad. Sci. USA 2005, 102, 11070–11075. [Google Scholar] [CrossRef]
- Parekh, P.J.; Arusi, E.; Vinik, A.I.; Johnson, D.A. The Role and Influence of Gut Microbiota in Pathogenesis and Management of Obesity and Metabolic Syndrome. Front. Endocrinol. 2014, 5, 47. [Google Scholar] [CrossRef]
- Baothman, O.A.; Zamzami, M.A.; Taher, I.; Abubaker, J.; Abu-Farha, M. The role of Gut Microbiota in the development of obesity and Diabetes. Lipids Health Dis. 2016, 15, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, B.M.; Saad, M.J.A. Influence of Gut Microbiota on Subclinical Inflammation and Insulin Resistance. Mediat. Inflamm. 2013, 2013, 986734. [Google Scholar] [CrossRef] [PubMed]
- Hill, C.; Guarner, F.; Reid, G.; Gibson, G.R.; Merenstein, D.J.; Pot, B.; Morelli, L.; Canani, R.B.; Flint, H.J.; Salminen, S.; et al. Expert Consensus Document: The International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 506–514. [Google Scholar] [CrossRef] [PubMed]
- Gibson, G.R.; Hutkins, R.; Sanders, M.E.; Prescott, S.L.; Reimer, R.A.; Salminen, S.J.; Scott, K.; Stanton, C.; Swanson, K.S.; Cani, P.D.; et al. Expert consensus document: The International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of prebiotics. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 491–502. [Google Scholar] [CrossRef]
- Swanson, K.S.; Gibson, G.R.; Hutkins, R.; Reimer, R.A.; Reid, G.; Verbeke, K.; Scott, K.P.; Holscher, H.D.; Azad, M.B.; Delzenne, N.M.; et al. The International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of synbiotics. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 687–701. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef]
- Yumuk, V.; Tsigos, C.; Fried, M.; Schindler, K.; Busetto, L.; Micic, D.; Toplak, H. European Guidelines for Obesity Management in Adults. Obes. Facts 2015, 8, 402–424. [Google Scholar] [CrossRef] [PubMed]
- Dickey, R.A.; Bartuska, C.G.D.; Bray, F.W.G.; Callaway, M.C.W.; Davidson, F.T.E.; Feld, M.S.; Ferraro, M.T.R.; Hodgson, S.F.; Jellinger, F.S.P.; Kennedy, F.P.F.; et al. AACE/ACE Position Statement on the Prevention, Diagnosis, and Treatment of Obesity (1998 Revision). Endocr Pract. 1998, 4, 297–350. [Google Scholar]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.M.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Kadooka, Y.; Sato, M.; Imaizumi, K.; Ogawa, A.; Ikuyama, K.; Akai, Y.; Okano, M.; Kagoshima, M.; Tsuchida, T. Regulation of abdominal adiposity by probiotics (Lactobacillus gasseri SBT2055) in adults with obese tendencies in a randomized controlled trial. Eur. J. Clin. Nutr. 2010, 64, 636–643. [Google Scholar] [CrossRef] [PubMed]
- Omar, J.M.; Chan, Y.-M.; Jones, M.L.; Prakash, S.; Jones, P.J.H. Lactobacillus fermentum and Lactobacillus amylovorus as probiotics alter body adiposity and gut microflora in healthy persons. J. Funct. Foods 2013, 5, 116–123. [Google Scholar] [CrossRef]
- Sanchez, M.; Darimont, C.; Drapeau, V.; Emady-Azar, S.; Lepage, M.; Rezzonico, E.; Ngom-Bru, C.; Berger, B.; Philippe, L.; Ammon-Zuffrey, C.; et al. Effect of Lactobacillus rhamnosusCGMCC1.3724 supplementation on weight loss and maintenance in obese men and women. Br. J. Nutr. 2014, 111, 1507–1519. [Google Scholar] [CrossRef] [PubMed]
- Safavi, M.; Farajian, S.; Kelishadi, R.; Mirlohi, M.; Hashemipour, M. The effects of synbiotic supplementation on some cardio-metabolic risk factors in overweight and obese children: A randomized triple-masked controlled trial. Int. J. Food Sci. Nutr. 2013, 64, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Kadooka, Y.; Sato, M.; Ogawa, A.; Miyoshi, M.; Uenishi, H.; Ogawa, H.; Ikuyama, K.; Kagoshima, M.; Tsuchida, T. Effect of Lactobacillus gasseri SBT2055 in fermented milk on abdominal adiposity in adults in a randomised controlled trial. Br. J. Nutr. 2013, 110, 1696–1703. [Google Scholar] [CrossRef] [PubMed]
- Zarrati, M.; Salehi, E.; Nourijelyani, K.; Mofid, V.; Zadeh, M.J.H.; Najafi, F.; Ghaflati, Z.; Bidad, K.; Chamari, M.; Karimi, M.; et al. Effects of Probiotic Yogurt on Fat Distribution and Gene Expression of Proinflammatory Factors in Peripheral Blood Singlenuclear Cells in Overweight and Obese People with or without Weight-Loss Diet. J. Am. Coll. Nutr. 2014, 33, 417–425. [Google Scholar] [CrossRef]
- Lee, S.J.; Bose, S.; Seo, J.-G.; Chung, W.-S.; Lim, C.-Y.; Kim, H. The effects of co-administration of probiotics with herbal medicine on obesity, metabolic endotoxemia and dysbiosis: A randomized double-blind controlled clinical trial. Clin. Nutr. 2014, 33, 973–981. [Google Scholar] [CrossRef]
- Jung, S.; Lee, Y.J.; Kim, M.; Kim, M.; Kwak, J.H.; Lee, J.W.; Ahn, Y.-T.; Sim, J.-H.; Lee, J.H. Supplementation with two probiotic strains, Lactobacillus curvatus HY7601 and Lactobacillus plantarum KY1032, reduced body adiposity and Lp-PLA2 activity in overweight subjects. J. Funct. Foods 2015, 19, 744–752. [Google Scholar] [CrossRef]
- Ipar, N.; Aydogdu, S.D.; Yildirim, G.K.; Inal, M.; Gies, I.; Vandenplas, Y.; Dinleyici, E.C. Effects of synbiotic on anthropometry, lipid profile and oxidative stress in obese children. Benef. Microbes 2015, 6, 775–781. [Google Scholar] [CrossRef]
- Hibberd, A.A.; Yde, C.C.; Ziegler, M.L.; Honoré, A.H.; Saarinen, M.T.; Lahtinen, S.; Stahl, B.; Jensen, H.M.; Stenman, L.K. Probiotic or synbiotic alters the gut microbiota and metabolism in a randomised controlled trial of weight management in overweight adults. Benef. Microbes 2019, 10, 121–135. [Google Scholar] [CrossRef] [PubMed]
- Madjd, A.; Taylor, M.A.; Neek, L.S.; Delavari, A.; Malekzadeh, R.; Macdonald, I.A.; Farshchi, H.R. Effect of weekly physical activity frequency on weight loss in healthy overweight and obese women attending a weight loss program: A randomized controlled trial. Am. J. Clin. Nutr. 2016, 104, 1202–1208. [Google Scholar] [CrossRef] [PubMed]
- Higashikawa, F.; Noda, M.; Awaya, T.; Danshiitsoodol, N.; Matoba, Y.; Kumagai, T.; Sugiyama, M. Antiobesity effect of Pediococcus pentosaceus LP28 on overweight subjects: A randomized, double-blind, placebo-controlled clinical trial. Eur. J. Clin. Nutr. 2016, 70, 582–587. [Google Scholar] [CrossRef] [PubMed]
- Gomes, A.C.; De Sousa, R.G.M.; Botelho, P.B.; Gomes, T.L.N.; Prada, P.D.O.; Mota, J.F. The additional effects of a probiotic mix on abdominal adiposity and antioxidant Status: A double-blind, randomized trial. Obesity 2017, 25, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi-Sartang, M.; Bellissimo, N.; de Zepetnek, J.O.T.; Brett, N.R.; Mazloomi, S.M.; Fararouie, M.; Bedeltavana, A.; Famouri, M.; Mazloom, Z. The effect of daily fortified yogurt consumption on weight loss in adults with metabolic syndrome: A 10-week randomized controlled trial. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 565–574. [Google Scholar] [CrossRef]
- Kianifar, H.R.; Ahanchian, H.; Safarian, M.; Javid, A.; Farsad-Naeimi, A.; Jafari, A.; Kiani, M.A.; Dahri, M. Effects of Synbiotics on Anthropometric Indices of Obesity in Children: A randomized double-blind placebo-controlled pilot study. Top. Clin. Nutr. 2018, 33, 118–126. [Google Scholar] [CrossRef]
- Kim, J.; Yun, J.M.; Kim, M.K.; Kwon, O.; Cho, B. Lactobacillus gasseri BNR17 Supplementation Reduces the Visceral Fat Accumulation and Waist Circumference in Obese Adults: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Med. Food 2018, 21, 454–461. [Google Scholar] [CrossRef]
- Pedret, A.; Valls, R.M.; Calderón-Pérez, L.; Llauradó, E.; Companys, J.; Pla-Pagà, L.; Moragas, A.; Martín-Luján, F.; Ortega, Y.; Giralt, M.; et al. Effects of daily consumption of the probiotic Bifidobacterium animalis subsp. lactis CECT 8145 on anthropometric adiposity biomarkers in abdominally obese subjects: A randomized controlled trial. Int. J. Obes. 2019, 43, 1863–1868. [Google Scholar] [CrossRef]
- Sudha, M.R.; Ahire, J.J.; Jayanthi, N.; Tripathi, A.; Nanal, S. Effect of multi-strain probiotic (UB0316) in weight management in overweight/obese adults: A 12-week double blind, randomised, placebo-controlled study. Benef. Microbes 2019, 10, 855–866. [Google Scholar] [CrossRef]
- Hadi, A.; Sepandi, M.; Marx, W.; Moradi, S.; Parastouei, K. Clinical and psychological responses to synbiotic supplementation in obese or overweight adults: A randomized clinical trial. Complement. Ther. Med. 2019, 47, 102216. [Google Scholar] [CrossRef]
- Gutiérrez-Repiso, C.; Hernández-García, C.; García-Almeida, J.M.; Bellido, D.; Martín-Núñez, G.M.; Sánchez-Alcoholado, L.; Alcaide-Torres, J.; Sajoux, I.; Tinahones, F.J.; Moreno-Indias, I. Effect of Synbiotic Supplementation in a Very-Low-Calorie Ketogenic Diet on Weight Loss Achievement and Gut Microbiota: A Randomized Controlled Pilot Study. Mol. Nutr. Food Res. 2019, 63, 1900167. [Google Scholar] [CrossRef]
- Michael, D.R.; Jack, A.A.; Masetti, G.; Davies, T.S.; Loxley, K.E.; Kerry-Smith, J.; Plummer, J.F.; Marchesi, J.R.; Mullish, B.H.; McDonald, J.; et al. A randomised controlled study shows supplementation of overweight and obese adults with lactobacilli and bifidobacteria reduces bodyweight and improves well-being. Sci. Rep. 2020, 10, 1–12. [Google Scholar] [CrossRef]
- Razmpoosh, E.; Zare, S.; Fallahzadeh, H.; Safi, S.; Nadjarzadeh, A. Effect of a low energy diet, containing a high protein, probiotic condensed yogurt, on biochemical and anthropometric measurements among women with overweight/obesity: A randomised controlled trial. Clin. Nutr. ESPEN 2020, 35, 194–200. [Google Scholar] [CrossRef]
- Song, E.-J.; Han, K.; Lim, T.-J.; Lim, S.; Chung, M.-J.; Nam, M.H.; Kim, H.; Nam, Y.-D. Effect of probiotics on obesity-related markers per enterotype: A double-blind, placebo-controlled, randomized clinical trial. EPMA J. 2020, 11, 31–51. [Google Scholar] [CrossRef]
- Lim, S.; Moon, J.H.; Shin, C.M.; Jeong, D.; Kim, B. Effect of Lactobacillus sakei, a Probiotic Derived from Kimchi, on Body Fat in Koreans with Obesity: A Randomized Controlled Study. Endocrinol. Metab. 2020, 35, 425–434. [Google Scholar] [CrossRef] [PubMed]
- Sergeev, I.N.; Aljutaily, T.; Walton, G.; Huarte, E. Effects of Synbiotic Supplement on Human Gut Microbiota, Body Composition and Weight Loss in Obesity. Nutrients 2020, 12, 222. [Google Scholar] [CrossRef] [PubMed]
- Michael, D.R.; Davies, T.S.; Jack, A.A.; Masetti, G.; Marchesi, J.R.; Wang, D.; Mullish, B.H.; Plummer, S.F. Daily supplementation with the Lab4P probiotic consortium induces significant weight loss in overweight adults. Sci. Rep. 2021, 11, 1–8. [Google Scholar] [CrossRef]
- Rahayu, E.S.; Mariyatun, M.; Manurung, N.E.P.; Hasan, P.N.; Therdtatha, P.; Mishima, R.; Komalasari, H.; Mahfuzah, N.A.; Pamungkaningtyas, F.H.; Yoga, W.K.; et al. Effect of probiotic Lactobacillus plantarum Dad-13 powder consumption on the gut microbiota and intestinal health of overweight adults. World J. Gastroenterol. 2021, 27, 107–128. [Google Scholar] [CrossRef] [PubMed]
- Madjd, A.; Taylor, M.A.; Mousavi, N.; Delavari, A.; Malekzadeh, R.; Macdonald, I.A.; Farshchi, H.R. Comparison of the effect of daily consumption of probiotic compared with low-fat conventional yogurt on weight loss in healthy obese women following an energy-restricted diet: A randomized controlled trial1. Am. J. Clin. Nutr. 2016, 103, 323–329. [Google Scholar] [CrossRef]
- Stenman, L.K.; Lehtinen, M.J.; Meland, N.; Christensen, J.E.; Yeung, N.; Saarinen, M.T.; Courtney, M.; Burcelin, R.; Lähdeaho, M.-L.; Linros, J.; et al. Probiotic With or Without Fiber Controls Body Fat Mass, Associated With Serum Zonulin, in Overweight and Obese Adults—Randomized Controlled Trial. EBioMedicine 2016, 13, 190–200. [Google Scholar] [CrossRef]
- Do, H.P.; Tran, B.X.; Nguyen, C.T.; Van Vo, T.; Baker, P.R.A.; Dunne, M.P. Inter-partner violence during pregnancy, maternal mental health and birth outcomes in Vietnam: A systematic review. Child. Youth Serv. Rev. 2019, 96, 255–265. [Google Scholar] [CrossRef]
- Gishti, O.; Gaillard, R.; Durmus, B.; Abrahamse, M.; Van Der Beek, E.M.; Hofman, A.; Franco, O.H.; De Jonge, L.L.; Jaddoe, V.W.V. BMI, total and abdominal fat distribution, and cardiovascular risk factors in school-age children. Pediatr. Res. 2015, 77, 710–718. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.-J.; Wang, P.-W.; Chen, T.-Y. The relationship between regional abdominal fat distribution and both insulin resistance and subclinical chronic inflammation in non-diabetic adults. Diabetol. Metab. Syndr. 2014, 6, 49. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.-P.; Lee, K.-M.; Kang, J.-H.; Yun, S.-I.; Park, H.-O.; Moon, Y.; Kim, J.-Y. Effect ofLactobacillus gasseriBNR17 on Overweight and Obese Adults: A Randomized, Double-Blind Clinical Trial. Korean J. Fam. Med. 2013, 34, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Park, D.-Y.; Ahn, Y.-T.; Park, S.-H.; Huh, C.-S.; Yoo, S.-R.; Yu, R.; Sung, M.-K.; McGregor, R.A.; Choi, M.-S. Supplementation of Lactobacillus curvatus HY7601 and Lactobacillus plantarum KY1032 in Diet-Induced Obese Mice Is Associated with Gut Microbial Changes and Reduction in Obesity. PLoS ONE 2013, 8, e59470. [Google Scholar] [CrossRef] [PubMed]
- Chang, B.J.; Park, S.U.; Jang, Y.S.; Ko, S.H.; Joo, N.M.; Kim, S.I.; Kim, C.-H.; Chang, D.K. Effect of functional yogurt NY-YP901 in improving the trait of metabolic syndrome. Eur. J. Clin. Nutr. 2011, 65, 1250–1255. [Google Scholar] [CrossRef]
- Drissi, F.; Merhej, V.; Angelakis, E.; Kaoutari, A.E.; Carrière, F.; Henrissat, B.; Raoult, D. Comparative genomics analysis of Lactobacillus species associated with weight gain or weight protection. Nutr. Diabetes 2014, 4, e109. [Google Scholar] [CrossRef]
- Zarrati, M.; Shidfar, F.; Nourijelyani, K.; Mofid, V.; Hosseinzadeh-Attar, M.J.; Bidad, K.; Najafi, F.; Gheflati, Z.; Chamari, M.; Salehi, E. Lactobacillus acidophilus La5, Bifidobacterium BB12, and Lactobacillus casei DN001 modulate gene expression of subset specific transcription factors and cytokines in peripheral blood singlenuclear cells of obese and overweight people. BioFactors 2013, 39, 633–643. [Google Scholar] [CrossRef]
- Kelishadi, R.; Farajian, S.; Safavi, M.; Mirlohi, M.; Hashemipour, M. A randomized triple-masked controlled trial on the effects of synbiotics on inflammation markers in overweight children. J. Pediatr. 2014, 90, 161–168. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, M.N.; Sivieri, K.; Alegro, J.H.A.; Saad, S.M.I. Aspectos tecnológicos de alimentos funcionais contendo probióticos. Rev. Bras. Ciênc. Farm. 2002, 38, 1–21. [Google Scholar] [CrossRef][Green Version]
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. 2013 AHA/ACC/TOS Guideline for the Management of Overweight and Obesity in Adults: A report of the American college of cardiology/American heart association task force on practice guidelines and the obesity society. J. Am. Coll. Cardiol. 2014, 63, 2985–3023. [Google Scholar] [CrossRef]
- Mazloom, K.; Siddiqi, I.; Covasa, M. Probiotics: How Effective Are They in the Fight against Obesity? Nutrients 2019, 11, 258. [Google Scholar] [CrossRef] [PubMed]
- Cerdó, T.; García-Santos, J.A.; Bermúdez, M.G.; Campoy, C. The Role of Probiotics and Prebiotics in the Prevention and Treatment of Obesity. Nutrients 2019, 11, 635. [Google Scholar] [CrossRef]
- Benahmed, A.G.; Gasmi, A.; Doşa, A.; Chirumbolo, S.; Mujawdiya, P.K.; Aaseth, J.; Dadar, M.; Bjørklund, G. Association between the gut and oral microbiome with obesity. Anaerobe 2021, 70, 102248. [Google Scholar] [CrossRef] [PubMed]
- Radaic, A.; Kapila, Y.L. The oralome and its dysbiosis: New insights into oral microbiome-host interactions. Comput. Struct. Biotechnol. J. 2021, 19, 1335–1360. [Google Scholar] [CrossRef] [PubMed]
- de Simone, C. The Unregulated Probiotic Market. Clin. Gastroenterol. Hepatol. 2019, 17, 809–817. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Year, Country | Population | Design | Intervention | Control | Strains & Doses | Inter Period | Results |
|---|---|---|---|---|---|---|---|---|
| Kadooka et al. [23] | 2010, Japan | n = 87 n(IG) = 43 n(CG) = 44 Adults (male and female) Visceral fat 81.2–178.5 cm2 BMI: 24.2–30.7 kg/m2 Age: 33–63 years | Multi-center RCT-DB | 200 g/day of fermented milk | 200 g/day of fermented milk without Lactobacillus gasseri SBT2055 | Lactobacillus gasseri SBT2055 (5 × 1010 CFU/100 g) | 12 weeks | Body weight, BMI, waist and hip circumferences decreased significantly (p ≤ 0.001). In the active group the visceral and abdominal subcutaneous fat areas decreased significantly (p ≤ 0.01) |
| Omar et al. [24] | 2013, Canada | n = 28 n(IG) = 14 n(GC) = 14 Adults (male and female) BMI: 25–32 kg/m2 Age: 18–60 years | Cross-over RCT-DB | (i) Yogurt with probiotic 1 (ii) Yogurt with probiotic 2 Both groups were put on diet | Control yogurt | (i) 100 g of control yogurt + 10 g of 1.39 × 109 CFU microencapsulated BSH-active Lactobacillus acidophilus (ii) 100 g of control yogurt + 10 g of 1.08 × 109 CFU microencapsulated FAE-active Lactobacillus fermentum | 13 weeks | No significant differences in body weight were observed at baseline or endpoint across the three treatments. Significant reductions in total fat mass by 3% from baseline (p = 0.05) |
| Sanchez et al. [25] | 2013, Canada | n = 125 n(IG) = 62 n(GC) = 63 Healthy adults (male and female) BMI: 29–41 kg/m2 Age:18–55 years | RCT-DB | 2 capsules/day of probiotic + moderate restriction of energy in the first 12 weeks followed by 12 weeks of maintenance | Placebo | Lactobacillus rhamnosus CGMCC1.3724 (LPR) (1.62 × 108 CFU) with 300 mg of one mix of oligofructose and inulin (70:30, vv) | 24 weeks | No significant reduction in weight among the comparison groups. Significant interaction between sex and intervention. Weight loss in female in the intervention group was significantly higher than those of placebo group (p = 0.02) |
| Safavi et al. [26] | 2013, Iran | n = 70 n(IG) = 29 n(CG) = 27 Healthy children and adolescents BMI: ≥85th percentile | RCT-TB | 1 capsule/day of the synbiotic | Placebo of maltodextrin | Lactobacillus casei, Lactobacillus rhamnosus, Streptococcus thermophilus, Bifidobacterium breve, Lactobacillus acidophilus, Bifidobacterium longum and Lactobacillus bulgaricus of human origin with prebiotics (fructo-oligosaccharides), vitamins A, C and E. Every capsule contained 2 × 108 CFU of probiotic bacteria | 8 weeks | The decrease in the z scores of the BMI (p = 0.002), waist circumference (p ≤ 0.0001) and the waist-to-hip ratio (p ≤ 0.0001) were significantly higher in the synbiotic group than in the placebo group |
| Kadooka et al. [27] | 2013, Japan | n = 210 n(IG) = 140 (69/71) n(CG) = 70 Healthy adults (male and female) Average BMI 27 kg/m2 and with large areas of visceral fat (80.2–187.8 cm2) Age: 25–60 years | Multi-center RCT-DB | 200 g/day of milk fermented with strains of probiotics to different levels. Participants maintained their life style, including diet and exercise | 200 g fermented milk without probiotic | Starter cultures: lactic acid bacteria (Streptococcus thermophilus and Lactobacillus delbrueckii ssp.) and cells of Lactobacillus gasseri SBT2055 (LG2055) to levels of 106, 107 (CFU/g) | 12 weeks | Significant decrease in the areas of visceral fat, BMI, waist and hip circumference (p ≤ 0.01) in the groups with doses of 107 and 106 (CFU/g) at weeks 8 and 12 |
| Zarrati et al. [28] | 2014, Iran | n = 75 n(IG) = 25/25 n(GC) = 25 Healthy adults with overweight or obesity BMI > 25 kg/m2 Age: 20–50 years | RCT-DB | (i) Low calorie diet with probiotic yogurt (200 g/day) (ii) Consumption of the same probiotic yogurt (200 g/day) without the diet low in calories | Low calorie diet with regular yogurt consumption (200 g/day) | Lactobacillus acidophilus La5, Bifidobacterium BB12 and Lactobacillus casei DN001 108 CFU/g | 8 weeks | A reduction in the BMI, percentage of fat and leptin level, which was more evident in the groups that received the weight loss diet with probiotic yogurt. Significant differences in weight, BMI and waist circumference between groups (p = 0.001) |
| Lee et al. [29] | 2014, Korea Republic | n = 50 n(IG) = 25 n(GC) = 25 Healthy female Waist circumference > 85 cm, BMI > 25 kg/m2 Age: 19–65 years | RCT-DB | Supplementation 2 times/day with 3 g of Bofutsushosan (BTS) and DUOLAC 7 probiotic. It was suggested to the participants to limit energy intake to 20–25 kcal/kg | 3 g of Bofutsushosan (BTS) and placebo capsules 2 times/day | DUOLAC 7: 5000 million viable cells of Streptococcus thermophilus (KCTC 11870BP), Lactobacillus plantarum (KCTC 10782BP), Lactobacillus acidophilus (KCTC 11906BP), Lactobacillus rhamnosus (KCTC 12202BP), Bifidobacterium lactis (KCTC 11904BP), Bifidobacterium longum (KCTC 12200BP) and Bifidobacterium breve (KCTC 12201BP) | 8 weeks | Both groups showed significant reductions in weight and waist circumference (p = 0.000). No significant differences were observed in body composition |
| Jung et al. [30] | 2015, Korea Republic | n = 120 n(IG) = 60 n(CG) = 60 Adults (male and female) BMI: 25–30 kg/m2 Age 20–65 years | RCT-DB | 2 g probiotic powder, two times/day (immediately after breakfast and dinner). Participants maintained their diet and normal lifestyle | 2 g of powder containing 1.34 g of crystalline cellulose, 0.6 g of lactose and 0.06 g of blueberry | 2 g powder of strains Lactobacillus curvatus HY7601 and Lactobacillus plantarum KY1032, each at 2.5 × 109 CFU/capsule | 12 weeks | The probiotic group showed reductions in body weight (p = 0.008), BMI (p = 0.006) and waist circumference (p = 0.015) in relation to the initial value. When the changes were compared anthropometrically (differences with relative to baseline) between control and probiotics groups, the group of probiotics had greater reductions in body weight (p = 0.001) and BMI (p = 0.001) |
| Ipar et al. [31] | 2015, Turkey | n = 86 n(IG) = 43 n(CG) = 43 Children with primary obesity Age: 4–17 years | Open label RCT | Supplementation with synbiotic and 10% caloric reduction and increase in physical activity | 10% caloric reduction and increase in physical activity | Probiotics: Lactobacillus acidophilus (4.3 × 108 CFU/sachet), Lactobacillus rhamnosus (4.3 × 108 CFU/sachet), Bifidobacterium bifidum (4.3 × 108 CFU/sachet), Bifidobacterium longum (4.3 × 108 CFU/sachet), Enterococcus faecium (8.2 × 108 CFU/sachet). Prebiotics: fructo-oligosaccharides (FOS) 625 mg, lactulose 400 mg | 4 weeks | One month of supplementation with synbiotic resulted in significant weight reduction (p ≤ 0.001) and BMI (p ≤ 0.01) |
| Stenman et al. [32] | 2016, Finland | n = 225 n(IG) = 168 (57/55/56) n(CG) = 57 Adults (male and female) Waist hip ratio ≥ 0.88 for female, BMI: 28–34.9 kg/m2 Age: 18–65 years | RCT-DB | (i). Probiotic Bifidobacterium animalis ssp. lactis 420 (B420) (ii). Probiotic of polydextrose (LU) (iii). Probiotic Bifidobacterium animalis ssp. lactis 420 (B420) + Probiotic (LU + B420) | Placebo, cellulose microcrystalline 12 g/day | B420, 1010 CFU/day prebiotic of polydextrose 12 g/day B420, 1010 CFU/day in 12 g of polydextrose | 24 weeks | The probiotic B420 and the synbiotic LU + B420 seemed to improve weight control in the population analyzed by protocol due to changes in body fat mass (p = 0.02) |
| Madjd et al. [33] | 2016, Iran | n = 89 n(IG) = 44 n(CG) = 45 Premenopausal obese or overweight female, healthy BMI: 27–40 kg/m2 Age: 18–50 years | RCT-SB | 400 g/day of yogurt probiotic, enriched with culture. Both groups are put on a diet for weight loss and physical activity | 400 g/day standard yogurt low in fat with main meals | Starter cultures: Streptococcus thermophilus and Lactobacillus Bulgaricus. Probiotic: Lactobacillus acidophilus LA5 and Bifidobacterium lactis BB12, with a minimum total of 1 × 107 CFU. | 12 weeks | No significant differences were observed in weight loss and anthropometric measurements between groups after the intervention |
| Higashikawa et al. [34] | 2016, Japan | n = 62 n(IG) = 21/21 n(GC) = 20 Adults (male and female), healthy BMI: 25–30 kg/m2 Age: 20–70 years | RCT-DB | Powder of Pediococcus pentosaceus LP28 alive with dextrin. Powder of heat-killed Pediococcus pentosaceus LP28 with dextrin. | Placebo (dextrin) | Live LP29 7.5 mL 1010 CFU Dead LP29 7.5 mL 1010 CFU | 12 weeks | The LP28 removed by heat showed significant reductions in the BMI (p = 0.035), body fat percentage (p = 0.002), body fat mass (p = 0.004) and waist circumference (p = 0.009). |
| Gomes et al. [35] | 2017, Brazil | n = 43 n(IG) = 21 n(GC) = 22 Female with overweight or obesity, healthy BMI: 24.9–40 kg/m2 Age: 20–59 years | RCT-DB | 4 sachet of probiotic daily before breakfast+ dietary intervention | Placebo+ Dietary intervention | 1 × 109 CFU of each of the probiotic strains: Lactobacillus acidophilus LA-14, Lactobacillus casei LC-11, Lactococcus lactis LL-23, Bifidobacterium bifidum BB-06, Bifidobacterium lactis BL-4 (Danisco). Totaling 2 × 1010 CFU/day | 8 weeks | Dietary intervention+ probiotic group showed greater reductions in waist circumference (p = 0.03), waist-height ratio (p = 0.02), conicity index (p = 0.03) in comparison with the dietary intervention |
| Mohammadi-Sartang et al. [36] | 2018, Iran | n = 94 n(IG) = 44 n(CG) = 43 Adults (male and female) BMI: 25–34.9 kg/m2 Age: 20–65 years | RCT-DB | Two daily servings (2 × 250 g) of fortified yogurt containing 5 g protein powder, 3 g inulin as a prebiotic, 500 mg calcium and 500 IU vitamin D3. All participants received a diet energy restriction for the study intervention 500 kcal less, with a composition of macronutrients of 55% of carbohydrates, 15% of protein and 30% fat | Two daily servings (2 × 250 g) of low fat natural yogurt, that contained 300 mg of calcium. Starter cultures: Streptococcus thermophilus and Lactobacillus bulgaricus | Starter cultures: S. thermophilus and L. Bulgaricus enriched with at least 107 CFU/g of Bifidobacterium lactis Bb-12 | 10 weeks | Decreases in BMI (kg/m2), waist circumference (cm), body fat mass (kg) and body fat percentage (%) in both groups at the end of the study comparison with the initial values. Reductions in waist circumference (p = 0.002), body fat (p = 0.023) and body fat percentage (p = 0.028) higher in the fortified yogurt group compared to low-fat yogurt group |
| Kianifar et al. [37] | 2018, Iran | n = 46 n(IG) = 23 n(CG) = 23 Kids (male and female) with obesity BMI: ≥85th percentile Age: 7–13 years | Pilot-Study RCT-DB | Restrictive diet, physical activity plan and 1 capsule of synbiotics per day | Same as the treatment group, received a restrictive diet and physical activity plan but with a capsule of placebo per day | Fructo-oligosaccharide, vitamins A, C and E, 108 UFC of a combination of Lactobacillus casei, Lactobacillus rhamnosus, Streptococcus thermophilus, Bifidobacterium breve, Lactobacillus acidophilus, Bifidobacterium infantis and Lactobacillus bulgaricus | 12 weeks | Significant reductions in z score of BMI and percentage of fat in both groups (p ≤ 0.001). Waist circumference decreased significantly only in the group intervened with synbiotics (p ≤ 0.001). |
| Kim et al. [38] | 2018, Korea Republic | n = 90 n(IG) = 60 (30/30) n(CG) = 30 Adults without comorbidities with overweight or obesity BMI: 25–35 kg/m2 Age: 20–75 years | RCT-DB | Two capsules/day (400 mg/capsule) low dose or high of probiotic. Both groups reduced 200 kcal/day their energy intake and increased by 100 kcal/day their physical activity, during intervention period | Two capsules (400 mg/capsule) of placebo that composed of maltodextrin, crystalline cellulose and magnesium stearate | Lactobacillus gasseri, low-dose BNR17 (109 CFU) or high dose (1010 CFU | 12 weeks | BMI, hip circumference and waist–hip ratio were not significantly different between groups at weeks 0, 6, and 12. The waist circumference in the intervened groups and hip circumference in the low dose group decreased significantly after BNR17 consumption for 12 weeks within each group (p = 0.045, 0.012 and 0.033, respectively). |
| Pedret et al. [39] | 2018, Spain | n = 126 n(IG) = 86 (42/44) n(CG) = 40 Adults (male and female) Abdominal obesity (circumference of waist ≥ 102 cm for female) Age > 18 years | RCT-DB | 1 capsule per day of the following probiotics: Bifidobacterium animalis CECT 8145, heat killed Bifidobacterium animalis 8145. Dietary recommendations were made according to the 2013 guidelines of Adults Treatment Panel (ATP III). | Placebo (300 mg of maltodextrin) | (i) 100 mg of the live strain, 1010 CFU/capsule containing 200 mg of maltodextrin (ii) 100 mg/capsule of CECT strain 8145 killed by heat to a concentration of 1010 CFU before thermal treatment, which contained 200 mg of maltodextrin | 12 weeks | Treatment with Ba8145 decreased the BMI as compared to its initial value and the placebo group (p ≤ 0.05). Both interventions by Ba8145 decreased the waist circumference, the ratio of waist circumference/height and the conicity index (p ≤ 0.05), relative to its initial value. The changes relative to the placebo group were also significant (p ≤ 0.05) |
| Sudha et al. [40] | 2019, India | n = 90 n(IG) = 45 n(CG) = 45 Adults (male and female), healthy BMI: 25–32 kg/m2 Age: 30–65 years | RCT-DB | Two capsules/day of probiotic UB0316 | Placebo of maltodextrin. | UB0316: Lactobacillus salivarius UBLS-22, Lactobacillus casei UBLC42 Lactobacillus plantarum, UBLP-40 Lactobacillus acidophilus UBLA-34 Bifidobacterium breve UBBr-01, Bacillus coagulans Unique IS2, 5 109 CFU/capsule, and 100 mg of fructo- oligosaccharides | 12 weeks | At 12 weeks, supplementation of UB0316 showed significant reductions in BMI (p = 0.0001), body weight (p ≤ 0.0001), and in the waist-to-hip ratio (p = 0.007), compared to the placebo group |
| Hadi et al. [41] | 2019, Iran | n = 60 n(IG) = 30 n(CG) = 30 Adults (male and female) BMI: 25–35 kg/m2 Age: 20–50 years | RCT-DB | Consumption of a synbiotic capsule per day of 500 mg. Participants maintained their diet and normal lifestyle | Placebo (starch) | Lactobacillus acidophilus, Lactobacillus casei, Bifidobacterium bifidum (2 × 109 CFU/capsule), inulin | 8 weeks | Significant decrease in body weight (p = 0.03). Trend towards a significant decrease in BMI (p = 0.06) and waist circumference (p = 0.08) compared to the control group |
| Gutiérrez-Repiso et al. [42] | 2019, Spain | n = 33 n(IG) = 24 (15/9) n(GC) = 9 Adults (male and female) BMI ≥ 30 kg/m2 | RCT-SB | All participants underwent a weight loss program of two phases. Phase 1: ketogenic diet very low in calories (VLCKD) with supplementation of vitamins and minerals + synbiotic. Phase 2: low calorie diet (LCD) + synbiotic 2 | Phase 1: placebo Phase 2: the control group split in two: one continued receiving the placebo (control) and the other group received synbiotic 2 (placebo group + synbiotic 2) | Synbiotic phase 1: Bifidobacterium lactis, Lactobacillus rhamnosus, Bifidobacterium longum ES1 and prebiotic fiber. Synbiotic phase 2: Bifidobacterium animalis subsp. lactis and prebiotic fiber | 16 weeks (8 weeks each phase) | In all three treatments, the caloric restriction induced significant changes in weight, waist circumference and BMI during the entire intervention. In the group placebo-synbiotic 2, the weight loss percentage was significantly higher than in the group of synbiotic 1-synbiotic 2 (p = 0.030) |
| Michael et al. [43] | 2020, Bulgaria | n = 220 n(IG) = 110 n(GC) = 110 Healthy adults (male and female) Waist circumference > 100 cm in male and >89 cm in female. BMI: 25–39.4 kg/m2 Age: 30–65 years | RCT-DB | Consumption of a capsule of the probiotic Lab4P. Participants kept their usual life style | Placebo of cellulose microcrystalline | Lab4P: Lactobacillus acidophilus CUL60 (NCIMB 30157), Lactobacillus acidophilus CUL21 (NCIMB 30156), Lactobacillus plantarum CUL66 (NCIMB 30280), Bifidobacterium bifidum CUL20 (NCIMB 30153) and Bifidobacterium animalis subsp. Lactis CUL34 (NCIMB 30172) for a total of 5 × 1010 (CFU) per capsule | 24 weeks | Significant decrease in weight between groups (p ≤ 0.0001), BMI (p ≤ 0.0001), waist circumference (p ≤ 0.0001) and the ratio waist/height (p ≤ 0.0001) |
| Razmpoosh et al. [44] | 2020, Iran | n = 70 n(IG) = 35 n(CG) = 35 Women with overweight and obesity, non-smokers. BMI ≥ 25 kg/m2 | RCT | Participants received a diet low in energy with 50 g/day of kashk yogurt (high in protein, calcium and enriched with probiotics) | Diet low in energy without kashk | 1.85 × 106 (CFU/g) L. acidophilus La5 and 1.79 × 106 CFU/g of B. lactis Bb12 | 8 weeks | Significant reductions in the intervention group in BMI (p = 0.018), percentage of body fat (p = 0.037) and waist circumference (p = 0.047) in comparison with the control group |
| Song et al. [45] | 2020, Korea Republic | n = 50 n(IG) = 25 n(GC) = 25 Adults (male and female) healthy, with obesity (agree with the Obesity guidelines of Asia-Pacific) BMI > 25 kg/m2 Age: 20–60 years | RCT-DB | 2 probiotics capsules/day | Placebo of fructo-oligosaccharide and magnesium. stearate. | Bifidobacterium breve CBT BR3 isolated from Korean infant stools (15 billion viable cells/2 capsules), Lactobacillus plantarum CBT LP3 isolated from kimchi, Korean fermented vegetable products (15 billion viable cells/2 capsules) | 12 weeks | Significantly reduction of waist circumference (p = 0.049) and the relationship between visceral and subcutaneous fat area (p ≤ 0.001) in the probiotics group |
| Lim et al. [46] | 2020, Korea Republic | n = 114 n(IG) = 57 n(CG) = 57 Adults (male and female), healthy BMI > 25 kg/m2 Age: 20–65 years | RCT-DB | 2 probiotic capsules per day. Healthy life style recommendations were made and the participants were encouraged to maintain a favorable lifestyle | Placebo | Lactobacillus sakei CJLS03 5 × 109 CFU | 12 weeks | Body fat mass decreased by 0.2 kg in the probiotic group and increased by 0.6 kg in the placebo group (p = 0.018). After 12 weeks, the waist circumference was 0.8 cm smaller in the CJLS03 group than in the placebo group (p = 0.013). BMI and body weight did not change after 12 weeks |
| Sergeev et al. [47] | 2020, USA | n = 20 n(IG) = 10 n(GC) = 10 Adults (male and female) with overweight or obesity Average BMI: 33.5 kg/m2 Age: 47.4 years | RCT | A weight-loss eating plan was followed (low in carbohydrates high in protein), plus a capsule of synbiotic per day | The same eating plan as the intervention group was followed placebo group, but received a placebo capsule per day | One capsule contained: 15 × 109 CFU of patented strains of Lactobacillus acidophilus DDS-1, Bifidobacterium lactis UABla-12, Bifidobacterium longum UABl-14 and Bifidobacterium bifidum UABb-10. The prebiotic component was a mix of trans-galacto-oligosaccharides (GOS) at a dose of 5.5 g/day | 12 weeks | No statistically significant differences in the body composition (body mass, BMI, body fat mass, percentage of body fat, lean body mass) between placebo and synbiotic groups at the end of clinical trial |
| Michael et al. [48] | 2021, Bulgaria | n = 70 n(IG) = 35 n(CG) = 35 Adults (male and female) with overweight, healthy BMI: 25–29.9 kg/m2 Waist circumference of males> 100 cm; females > 89 cm Age: 45–65 years | RCT-DB | Daily consumption of a probiotic Lab4P capsule. Participants maintained their diet and normal lifestyle | Placebo | Lab4P: Lactobacillus acidophilus CUL60 (NCIMB 30157, Lactobacillus acidophilus CUL21 (NCIMB 30156), Lactobacillus plantarum CUL66 (NCIMB 30280), Bifidobacterium bifidum CUL2, Bifidobacterium animalis subsp. Lactis CUL34 (NCIMB 30172) for a total of 5 × 1010 CFU/capsule | 36 weeks | Significant decrease in body weight (p ≤ 0.0001) between groups, predominantly in the probiotic group. Significant decrease among groups in waist and hip circumference (p < 0.0001) |
| Rahayu et al. [49] | 2021, Indonesia | n = 60 n(IG) = 30 n(CG) = 30 Adults (male and female) healthy BMI ≥ 25 kg/m2 | RCT | 1 g of powdered skimmed milk with probiotic | 1 g of powdered skimmed milk without probiotic | Lactobacillus plantarum Dad-13 of 2 × 109 CFU/pack | 12 weeks | Significant decrease in body weight and BMI (p ≤ 0.05) after 90 days of ingestion of probiotics |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Álvarez-Arraño, V.; Martín-Peláez, S. Effects of Probiotics and Synbiotics on Weight Loss in Subjects with Overweight or Obesity: A Systematic Review. Nutrients 2021, 13, 3627. https://doi.org/10.3390/nu13103627
Álvarez-Arraño V, Martín-Peláez S. Effects of Probiotics and Synbiotics on Weight Loss in Subjects with Overweight or Obesity: A Systematic Review. Nutrients. 2021; 13(10):3627. https://doi.org/10.3390/nu13103627
Chicago/Turabian StyleÁlvarez-Arraño, Valentina, and Sandra Martín-Peláez. 2021. "Effects of Probiotics and Synbiotics on Weight Loss in Subjects with Overweight or Obesity: A Systematic Review" Nutrients 13, no. 10: 3627. https://doi.org/10.3390/nu13103627
APA StyleÁlvarez-Arraño, V., & Martín-Peláez, S. (2021). Effects of Probiotics and Synbiotics on Weight Loss in Subjects with Overweight or Obesity: A Systematic Review. Nutrients, 13(10), 3627. https://doi.org/10.3390/nu13103627