
Vitamin C in Critically Ill Patients: An Updated Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction
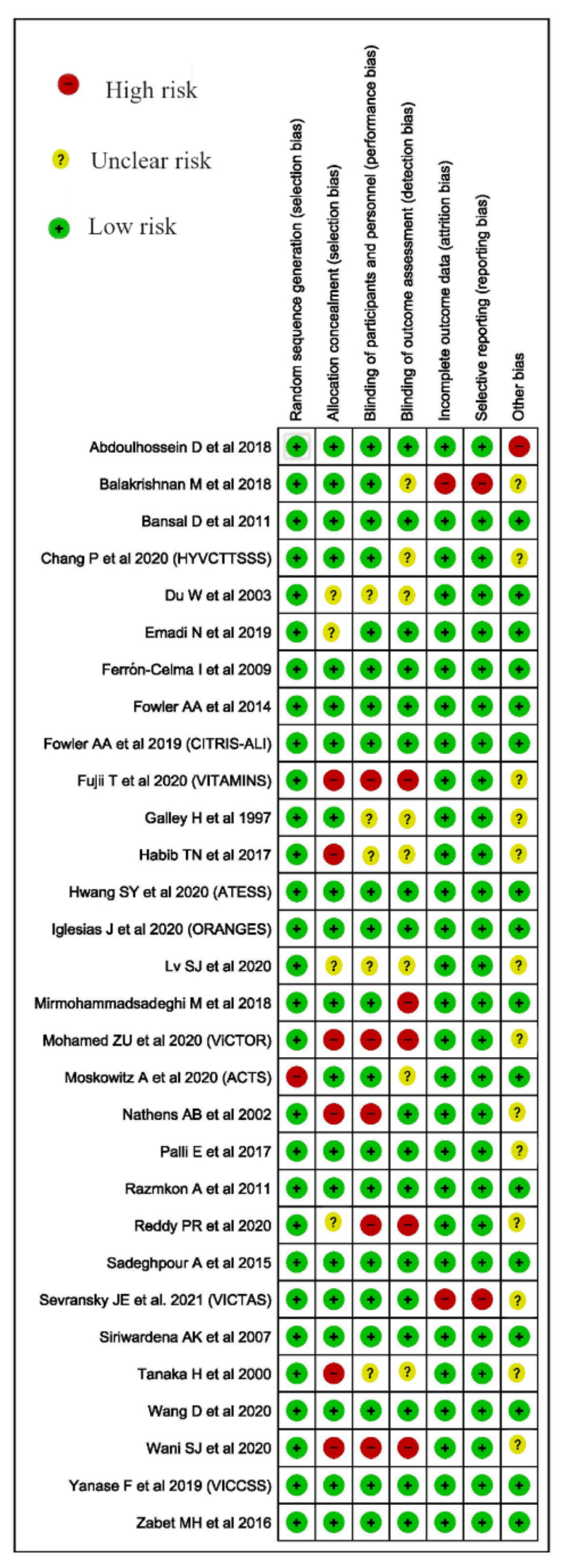
2.4. Risk of Bias
2.5. Statistical Analysis
2.6. Assessment of Heterogeneity
3. Results
3.1. Narrative Summary
3.2. Quantitative Synthesis
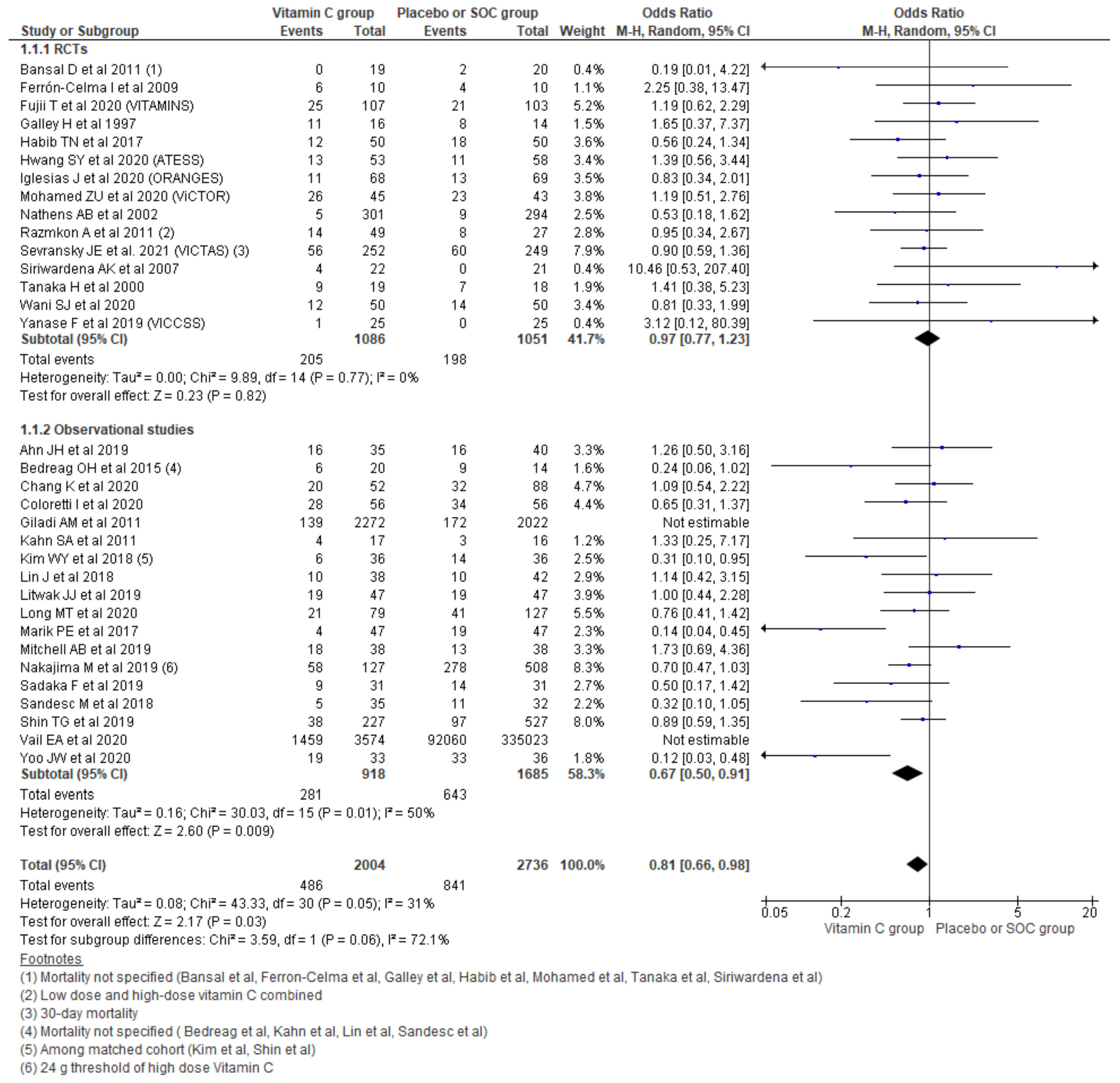
3.2.1. Hospital Mortality
Sensitivity Analysis among RCTs
Sensitivity Analysis among Observational Studies
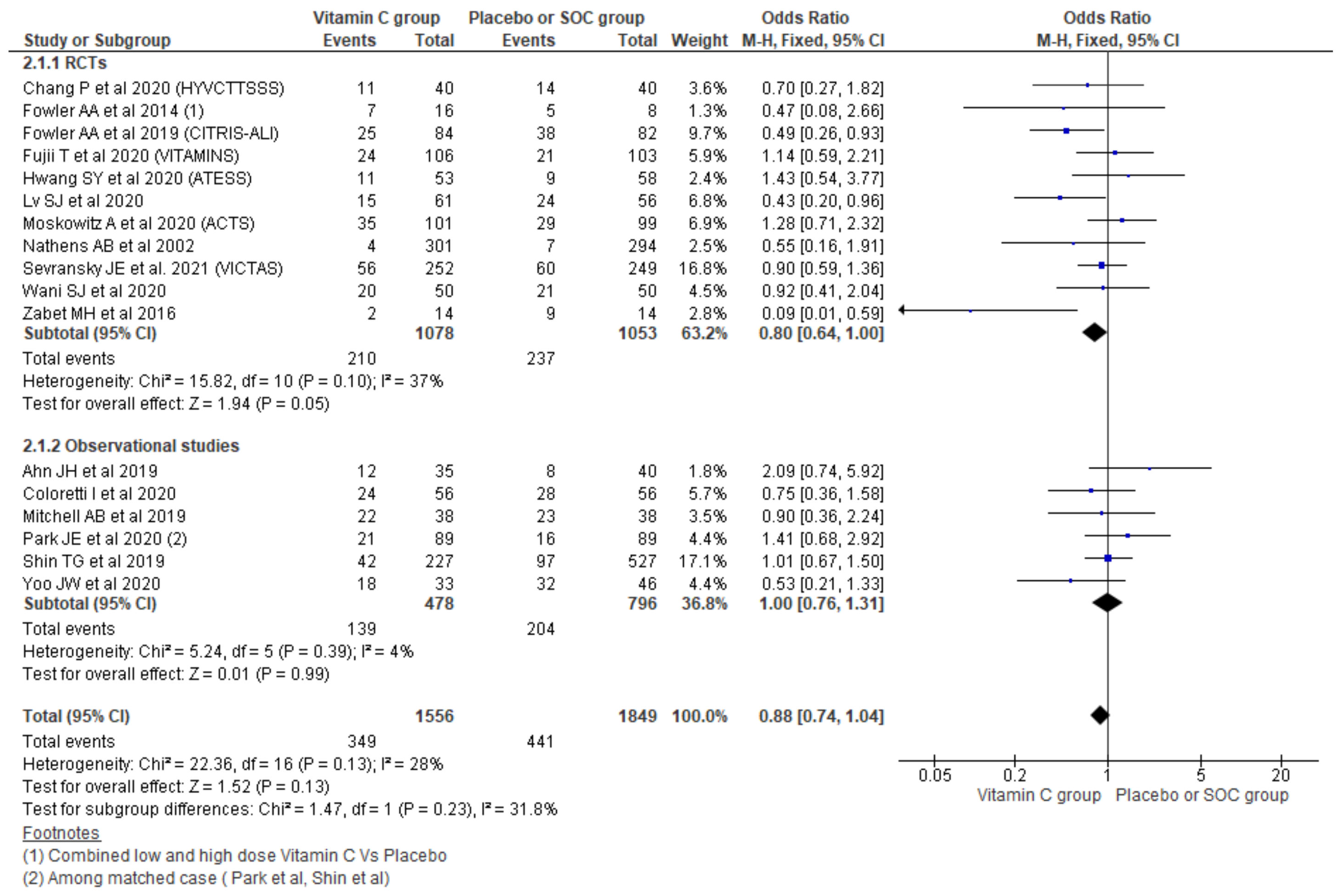
3.2.2. 28/30-Day Mortality
3.2.3. ICU Mortality
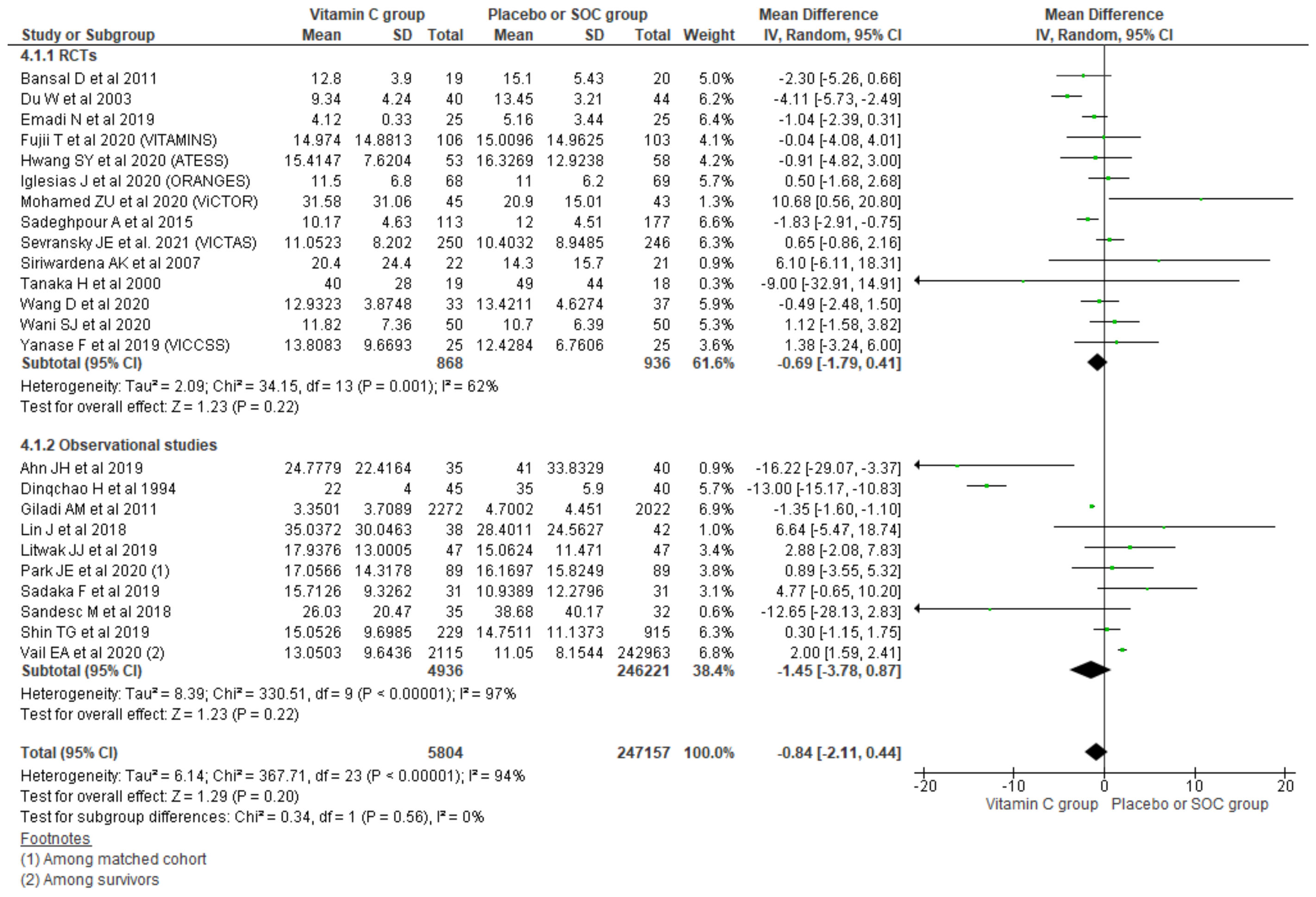
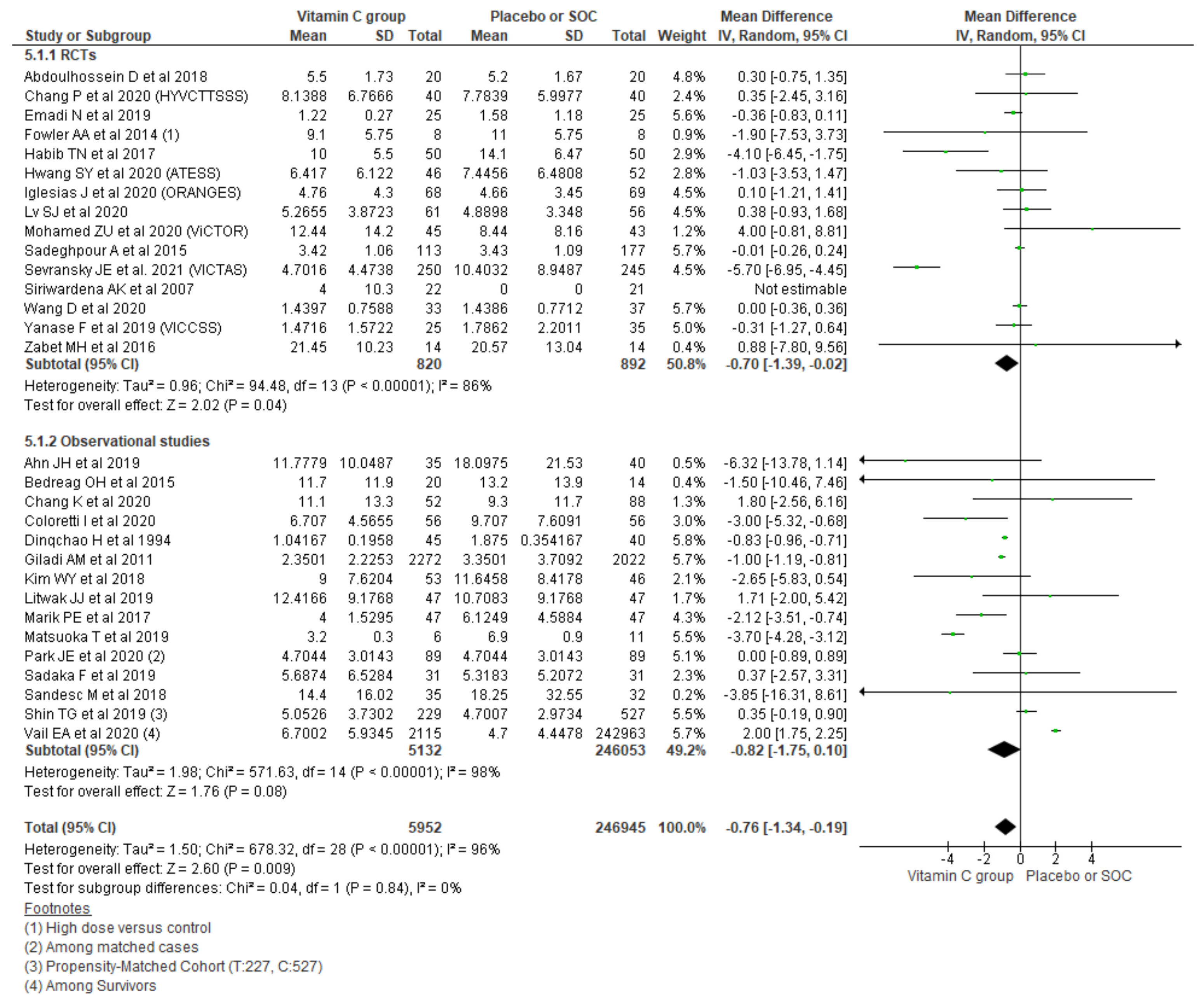
3.2.4. Length of Hospital Stay
Sensitivity Analysis among RCTs
Sensitivity Analysis among Observational Studies
3.2.5. Length of ICU Stay
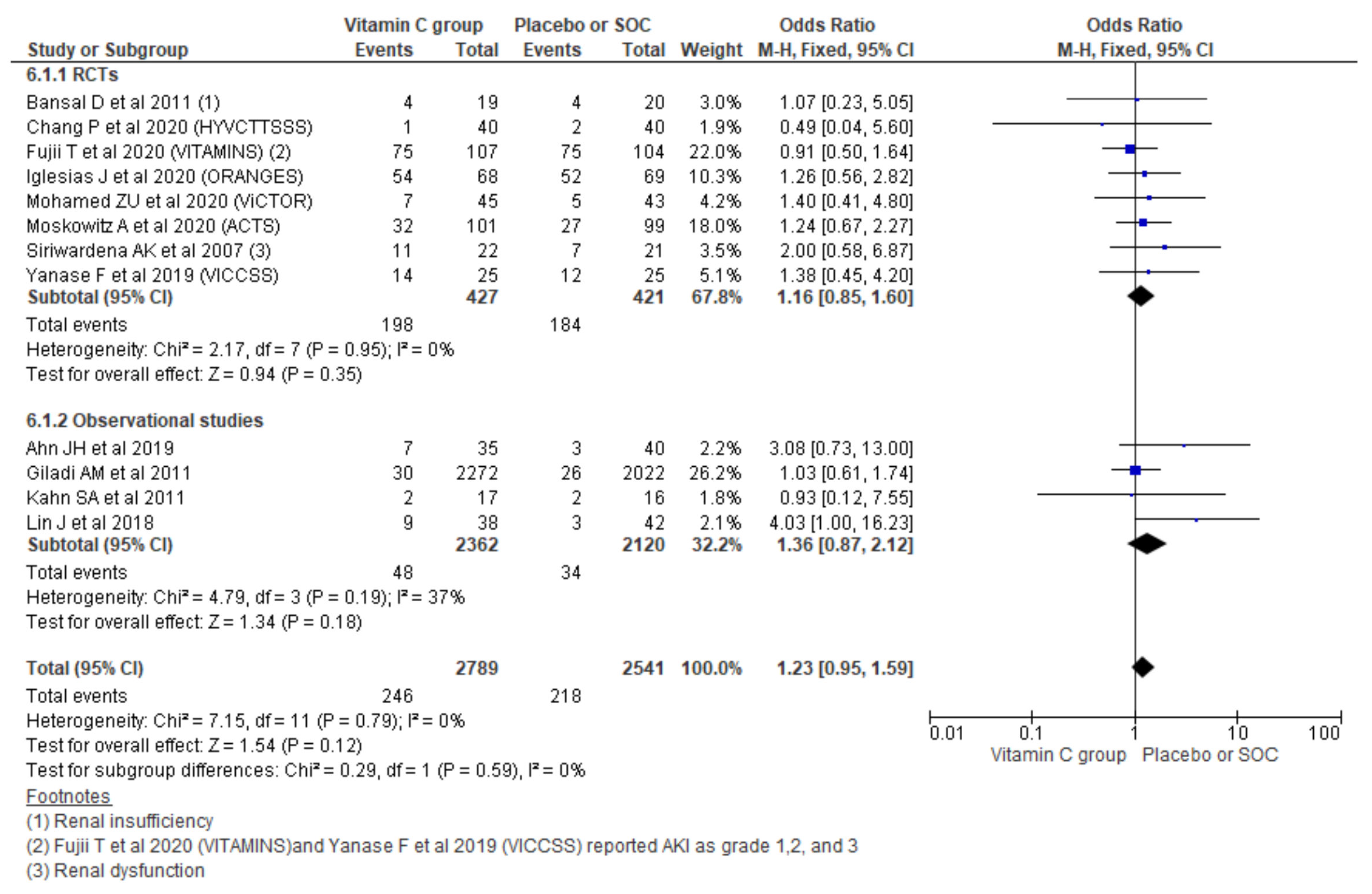
3.2.6. New-Onset Acute Kidney Injury (AKI)
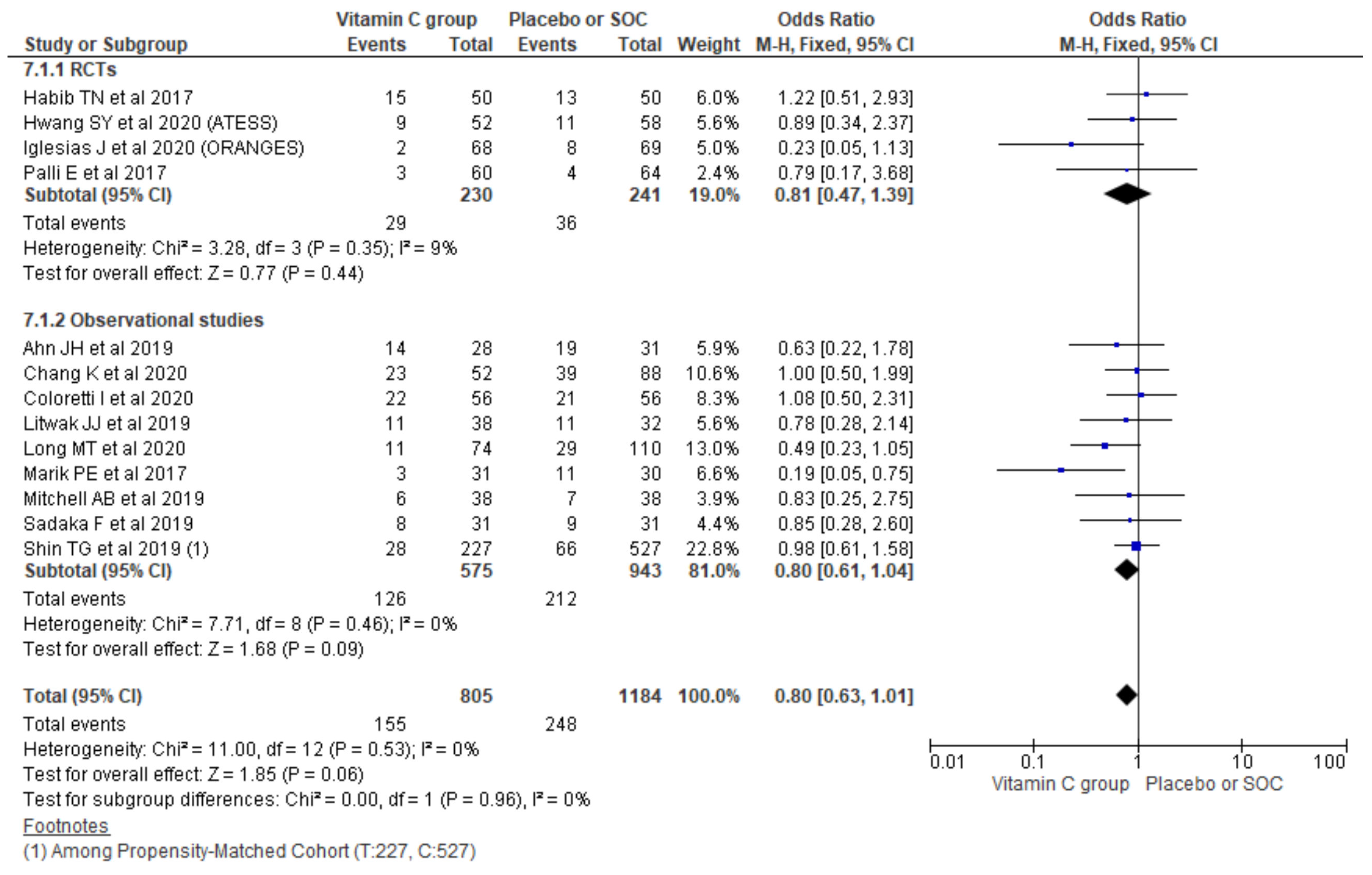
3.2.7. Renal Replacement Therapy (RRT) for AKI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fisher, B.J.; Kraskauskas, D.; Martin, E.J.; Farkas, D.; Wegelin, J.A.; Brophy, D.; Ward, K.R.; Voelkel, N.F.; Fowler, A.A.; Natarajan, R. Mechanisms of attenuation of abdominal sepsis induced acute lung injury by ascorbic acid. Am. J. Physiol. Lung Cell. Mol. Physiol. 2012, 303, L20–L32. [Google Scholar] [CrossRef]
- Fisher, B.J.; Seropian, I.M.; Kraskauskas, D.; Thakkar, J.N.; Voelkel, N.F.; Fowler, A.A.; Natarajan, R. Ascorbic acid attenuates lipopolysaccharide-induced acute lung injury. Crit. Care Med. 2011, 39, 1454–1460. [Google Scholar] [CrossRef]
- Fowler, A.A.; Syed, A.A.; Knowlson, S.; Sculthorpe, R.; Farthing, D.; DeWilde, C.; Farthing, C.A.; Larus, T.L.; Martin, E.; Brophy, D.F.; et al. Phase I safety trial of intravenous ascorbic acid in patients with severe sepsis. J. Transl. Med. 2014, 12, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Truwit, J.; Hite, R.; Morris, P.; DeWilde, C.; Jama, A.P. Effect of Vitamin C Infusion on Organ Failure and Biomarkers of Inflammation and Vascular Injury in Patients with Sepsis and Severe Acute Respiratory Failure: The CITRIS. Available online: http://jamanetwork.com (accessed on 26 January 2021).
- Marik, P.E.; Khangoora, V.; Rivera, R.; Hooper, M.H.; Catravas, J. Hydrocortisone, Vitamin C, and Thiamine for the Treatment of Severe Sepsis and Septic Shock: A Retrospective Before-After Study. Chest 2017, 151, 1229–1238. [Google Scholar] [CrossRef]
- Zabet, M.; Mohammadi, M.; Ramezani, M.; Khalili, H. Effect of high-dose Ascorbic acid on vasopressor′s requirement in septic shock. J. Res. Pharm. Pract. 2016, 5, 94. [Google Scholar] [CrossRef]
- Nakajima, M.; Kojiro, M.; Aso, S.; Matsui, H.; Fushimi, K.; Kaita, Y.; Goto, H.; Yamaguchi, Y.; Yasunaga, H. Effect of high-dose vitamin C therapy on severe burn patients: A nationwide cohort study. Crit. Care 2019, 23, 407. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Lin, H.; Lin, B.W.; Lin, J.-D. Effects of different ascorbic acid doses on the mortality of critically ill patients: A meta-analysis. Ann. Intensive Care 2019, 9, 58. [Google Scholar] [CrossRef] [Green Version]
- Zhang, M.; Jativa, D.F. Vitamin C supplementation in the critically ill: A systematic review and meta-analysis. SAGE Open Med. 2018, 6, 205031211880761. [Google Scholar] [CrossRef] [Green Version]
- Putzu, A.; Daems, A.-M.; Lopez-Delgado, J.C.; Giordano, V.F.; Landoni, G. The Effect of Vitamin C on Clinical Outcome in Critically Ill Patients. Crit. Care Med. 2019, 47, 774–783. [Google Scholar] [CrossRef]
- Wei, X.; Wang, Z.; Liao, X.; Guo, W.; Wen, J.Y.; Qin, T.; Wang, S. Efficacy of vitamin C in patients with sepsis: An updated meta-analysis. Eur. J. Pharmacol. 2020, 868, 172889. [Google Scholar] [CrossRef]
- Langlois, P.L.; Manzanares, W.; Adhikari, N.K.J.; Lamontagne, F.; Stoppe, C.; Hill, A.; Heyland, D.K. Vitamin C Administration to the Critically Ill: A Systematic Review and Meta-Analysis. J. Parenter. Enter. Nutr. 2019, 43, 335–346. [Google Scholar] [CrossRef]
- Shrestha, D.; Budhathoki, P.; Sedhai, Y.R.; Baniya, R.K.; Mandal, S.K.; Karki, S.; Shikhrakar, S. Role of Vitamin C in Critically Ill Patients: A Systematic Review and Meta-Analysis. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=222906 (accessed on 11 September 2021).
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- How Can I Cite Covidence? Available online: https://support.covidence.org/help/how-can-i-cite-covidence (accessed on 26 January 2021).
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Critical-Appraisal-Tools—Critical Appraisal Tools|Joanna Briggs Institute. Available online: https://joannabriggs.org/critical-appraisal-tools (accessed on 18 December 2020).
- RevMan for Non-Cochrane Reviews|Cochrane Training. Available online: https://training.cochrane.org/online-learning/core-software-cochrane-reviews/revman/revman-non-cochrane-reviews (accessed on 26 January 2021).
- Ahn, J.H.; Oh, D.K.; Huh, J.W.; Lim, C.M.; Koh, Y.; Hong, S.B. Vitamin C alone does not improve treatment outcomes in mechanically ventilated patients with severe sepsis or septic shock: A retrospective cohort study. J. Thorac. Dis. 2019, 11, 1562–1570. [Google Scholar] [CrossRef]
- Bedreag, O.H.; Rogobete, A.F.; Sărăndan, M.; Cradigati, A.C.; Păpurică, M.; Roşu, O.M.; Luca, L.; Vernic, C.; Nartiţă, R.; Săndesc, D. Influence of antioxidant therapy on the clinical status of multiple trauma patients. A retrospective single center study. Rom. J. Anaesth. Intensive Care 2015, 22, 89–96. [Google Scholar]
- Chang, K.; Harbin, M.; Shuster, C.; Griesdale, D.E.G.; Foster, D.; Sweet, D.; Wood, M.D.; Dhingra, V.K. Adding vitamin C to hydrocortisone lacks benefit in septic shock: A historical cohort study. Can. J. Anesth. 2020, 67, 1798–1805. [Google Scholar] [CrossRef]
- Coloretti, I.; Biagioni, E.; Venturelli, S.; Munari, E.; Tosi, M.; Roat, E.; Brugioni, L.; Gelmini, R.; Venturelli, C.; Girardis, M. Adjunctive therapy with vitamin c and thiamine in patients treated with steroids for refractory septic shock: A propensity matched before-after, case-control study. J. Crit. Care 2020, 59, 37–41. [Google Scholar] [CrossRef]
- Dingchao, H.; Zhiduan, Q.; Liye, H.; Xiaodong, F. The protective effects of high-dose ascorbic acid on myocardium against reperfusion injury during and after cardiopulmonary bypass. Thorac. Cardiovasc. Surg. 1994, 42, 276–278. [Google Scholar] [CrossRef]
- Giladi, A.M.; Dossett, L.A.; Fleming, S.B.; Abumrad, N.N.; Cotton, B.A. High-dose antioxidant administration is associated with a reduction in post-injury complications in critically ill trauma patients. Injury 2011, 42, 78–82. [Google Scholar] [CrossRef]
- Kahn, S.A.; Beers, R.J.; Lentz, C.W. Resuscitation after severe burn injury using high-dose ascorbic acid: A retrospective review. J. Burn Care Res. 2011, 32, 110–117. [Google Scholar] [CrossRef]
- Kim, W.Y.; Jo, E.J.; Eom, J.S.; Mok, J.; Kim, M.H.; Kim, K.U.; Park, H.K.; Lee, M.K.; Lee, K. Combined vitamin C, hydrocortisone, and thiamine therapy for patients with severe pneumonia who were admitted to the intensive care unit: Propensity score-based analysis of a before-after cohort study. J. Crit. Care 2018, 47, 211–218. [Google Scholar] [CrossRef]
- Lin, J.; Falwell, S.; Greenhalgh, D.; Palmieri, T.; Sen, S. High-dose ascorbic acid for burn shock resuscitation may not improve outcomes. J. Burn Care Res. 2018, 39, 708–712. [Google Scholar] [CrossRef]
- Litwak, J.; Cho, N.; Nguyen, H.; Moussavi, K.; Bushell, T. Vitamin C, Hydrocortisone, and Thiamine for the Treatment of Severe Sepsis and Septic Shock: A Retrospective Analysis of Real-World Application. J. Clin. Med. 2019, 8, 478. [Google Scholar] [CrossRef] [Green Version]
- Long, M.T.; Frommelt, M.A.; Ries, M.P.; Murray, M.; Osman, F.; Krause, B.M.; Kory, P.; Ries, M.-C.P. Early hydrocortisone, ascorbate and thiamine therapy for severe sep-tic shock. Crit. Care Shock 2020, 23, 23–24. [Google Scholar]
- Masood, H.; Burki, A.M.; Sultan, A.; Sharif, H.; Ghauri, A.; Khan, S.; Qureshi, M.S.S.; Qadeer, A.; Rasheed, G. Effect of Intravenous Vitamin C, Thiamine, and Hydrocortisone (The Metabolic Resuscitation Protocol) on Early Weaning from Vasopressors in Patients with Septic Shock. A Descriptive Case Series Study. Cureus 2019, 11, e5016. [Google Scholar] [CrossRef]
- Matsuoka, T.; Shinozaki, H.; Ozawa, S.; Izawa, Y.; Koyanagi, K.; Lefor, A.K.; Kobayashi, K. Administration of corticosteroids, ascorbic acid, and thiamine improves oxygenation after thoracoscopic esophagectomy. Ann. Thorac. Cardiovasc. Surg. 2020, 26, 133–139. [Google Scholar] [CrossRef]
- Mitchell, A.B.; Ryan, T.E.; Gillion, A.R.; Wells, L.D.; Muthiah, M.P. Vitamin C and Thiamine for Sepsis and Septic Shock. Am. J. Med. 2020, 133, 635–638. [Google Scholar] [CrossRef]
- Nagel, S.S.; Radu, C.A.; Kremer, T.; Meess, D.; Horter, J.; Ziegler, B.; Hirche, C.; Schmidt, V.J.; Kneser, U.; Hundeshagen, G. Safety, pharmacodynamics, and efficacy of high- versus low-dose ascorbic acid in severely burned adults. J. Burn Care Res. 2020, 41, 871–877. [Google Scholar] [CrossRef]
- Park, J.E.; Shin, T.G.; Jo, I.J.; Jeon, K.; Suh, G.Y.; Park, M.; Won, H.; Chung, C.R.; Hwang, S.Y. Impact of Vitamin C and Thiamine Administration on Delirium-Free Days in Patients with Septic Shock. J. Clin. Med. 2020, 9, 193. [Google Scholar] [CrossRef] [Green Version]
- Sadaka, F.; Grady, J.; Organti, N.; Donepudi, B.; Korobey, M.; Tannehill, D.; O’Brien, J. Ascorbic Acid, Thiamine, and Steroids in Septic Shock: Propensity Matched Analysis. J. Intensive Care Med. 2020, 35, 1302–1306. [Google Scholar] [CrossRef]
- Sandesc, M.; Rogobete, A.F.; Bedreag, O.H.; Dinu, A.; Papurica, M.; Cradigati, C.A.; Sarandan, M.; Popovici, S.E.; Bratu, L.M.; Bratu, T.; et al. Analysis of oxidative stress-related markers in critically ill polytrauma patients: An observational prospective single-center study. Bosn. J. Basic Med. Sci. 2018, 18, 191–197. [Google Scholar] [CrossRef] [Green Version]
- Shin, T.G.; Kim, Y.-J.; Ryoo, S.M.; Hwang, S.Y.; Jo, I.J.; Chung, S.P.; Choi, S.-H.; Suh, G.J.; Kim, W.Y. Early Vitamin C and Thiamine Administration to Patients with Septic Shock in Emergency Departments: Propensity Score-Based Analysis of a Before-and-After Cohort Study. J. Clin. Med. 2019, 8, 102. [Google Scholar] [CrossRef] [Green Version]
- Vail, E.A.; Wunsch, H.; Pinto, R.; Bosch, N.A.; Walkey, A.J.; Lindenauer, P.K.; Gershengorn, H.B. Use of hydrocortisone, ascorbic acid, and thiamine in adults with septic shock. Am. J. Respir. Crit. Care Med. 2020, 202, 1531–1539. [Google Scholar] [CrossRef]
- Yoo, J.W.; Kim, R.B.; Ju, S.; Lee, S.J.; Cho, Y.J.; Jeong, Y.Y.; Lee, J.D.; Kim, H.C. Clinical impact of supplementation of vitamins B1 and C on patients with sepsis-related acute respiratory distress syndrome. Tuberc. Respir. Dis. 2020, 83, 248–254. [Google Scholar] [CrossRef]
- Mean Variance Estimation. Available online: https://web.archive.org/web/20181224162602/http:/www.comp.hkbu.edu.hk/~xwan/median2mean.html (accessed on 16 February 2021).
- Identifying and Measuring Heterogeneity. Available online: https://handbook-5-1.cochrane.org/chapter_9/9_5_2_identifying_and_measuring_heterogeneity.htm (accessed on 18 December 2020).
- Abdoulhossein, D.; Taheri, I.; Saba, M.; Akbari, H.; Shafagh, S.; Zataollah, A. Effect of vitamin C and vitamin E on lung contusion: A randomized clinical trial study. Ann. Med. Surg. 2018, 36, 152–157. [Google Scholar] [CrossRef]
- Doll, S.; Ricou, B. Severe vitamin C deficiency in a critically ill adult: A case report. Eur. J. Clin. Nutr. 2013, 67, 881–882. [Google Scholar] [CrossRef] [Green Version]
- Colliou, E.; Mari, A.; Delas, A.; Delarche, A.; Faguer, S. Oxalate nephropathy following vitamin C intake within intensive care unit. Clin. Nephrol. 2017, 88, 354–358. [Google Scholar] [CrossRef]
- Emadi, N.; Nemati, M.H.; Ghorbani, M.; Allahyari, E. The effect of high-dose vitamin c on biochemical markers of myocardial injury in coronary artery bypass surgery. Braz. J. Cardiovasc. Surg. 2019, 34, 517–524. [Google Scholar] [CrossRef]
- Sevransky, J.E.; Rothman, R.E.; Hager, D.N.; Bernard, G.R.; Brown, S.M.; Buchman, T.G.; Busse, L.W.; Coopersmith, C.M.; DeWilde, C.; Ely, E.W.; et al. Effect of Vitamin C, Thiamine, and Hydrocortisone on Ventilator—and Vasopressor-Free Days in Patients With Sepsis. JAMA 2021, 325, 742. [Google Scholar] [CrossRef]
- Ferrón-Celma, I.; Mansilla, A.; Hassan, L.; Garcia-Navarro, A.; Comino, A.M.; Bueno, P.; Ferrón, J.A. Effect of Vitamin C Administration on Neutrophil Apoptosis in Septic Patients After Abdominal Surgery. J. Surg. Res. 2009, 153, 224–230. [Google Scholar] [CrossRef]
- Wani, S.J.; Mufti, S.A.; Jan, R.A.; Shah, S.U.; Qadri, S.M.; Khan, U.H.; Bagdadi, F.; Mehfooz, N.; Koul, P.A. Combination of vitamin C, thiamine and hydrocortisone added to standard treatment in the management of sepsis: Results from an open label randomised controlled clinical trial and a review of the literature. Infect. Dis. 2020, 52, 271–278. [Google Scholar] [CrossRef]
- Hwang, S.Y.; Ryoo, S.M.; Park, J.E.; Jo, Y.H.; Jang, D.-H.; Suh, G.J.; Kim, T.; Kim, Y.-J.; Kim, S.; Cho, H.; et al. Combination therapy of vitamin C and thiamine for septic shock: A multi-centre, double-blinded randomized, controlled study. Intensive Care Med. 2020, 46, 2015–2025. [Google Scholar] [CrossRef]
- Balakrishnan, M.; Gandhi, H.; Shah, K.; Pandya, H.; Patel, R.; Keshwani, S.; Yadav, N. Hydrocortisone, vitamin C and thiamine for the treatment of sepsis and septic shock following cardiac surgery. Indian J. Anaesth. 2018, 62, 934–939. [Google Scholar] [CrossRef]
- Chang, P.; Liao, Y.; Guan, J.; Guo, Y.; Zhao, M.; Hu, J.; Zhou, J.; Wang, H.; Cen, Z.; Tang, Y.; et al. Combined Treatment with Hydrocortisone, Vitamin C, and Thiamine for Sepsis and Septic Shock: A Randomized Controlled Trial. Chest 2020, 158, 174–182. [Google Scholar] [CrossRef]
- Du, W.D.; Yuan, Z.R.; Sun, J.; Tang, J.X.; Cheng, A.Q.; Shen, D.M.; Huang, C.J.; Song, X.H.; Yu, X.F.; Zheng, S.B. Therapeutic efficacy of high-dose vitamin C on acute pancreatitis and its potential mechanisms. World J. Gastroenterol. 2003, 9, 2565–2569. [Google Scholar] [CrossRef] [Green Version]
- Fujii, T.; Luethi, N.; Young, P.J.; Frei, D.R.; Eastwood, G.M.; French, C.J.; Deane, A.M.; Shehabi, Y.; Hajjar, L.A.; Oliveira, G.; et al. Effect of Vitamin C, Hydrocortisone, and Thiamine vs Hydrocortisone Alone on Time Alive and Free of Vasopressor Support among Patients with Septic Shock: The VITAMINS Randomized Clinical Trial. JAMA J. Am. Med. Assoc. 2020, 323, 423–431. [Google Scholar] [CrossRef]
- Iglesias, J.; Vassallo, A.V.; Patel, V.V.; Sullivan, J.B.; Cavanaugh, J.; Elbaga, Y. Outcomes of Metabolic Resuscitation Using Ascorbic Acid, Thiamine, and Glucocorticoids in the Early Treatment of Sepsis: The ORANGES Trial. Chest 2020, 158, 164–173. [Google Scholar] [CrossRef]
- Lv, S.J.; Zhang, G.H.; Xia, J.M.; Yu, H.; Zhao, F. Early use of high-dose vitamin C is beneficial in treatment of sepsis. Ir. J. Med. Sci. 2020, 190, 1183–1188. [Google Scholar] [CrossRef]
- Mirmohammadsadeghi, M.; Mirmohammadsadeghi, A.; Mahmoudian, M. Preventive Use of Ascorbic Acid for Atrial Fibrillation After Coronary Artery Bypass Graft Surgery. Heart Surg. Forum 2018, 21, E415–E417. [Google Scholar] [CrossRef]
- Mohamed, Z.U.; Prasannan, P.; Moni, M.; Edathadathil, F.; Prasanna, P.; Menon, A.; Nair, S.; Greeshma, C.R.; Sathyapalan, D.T.; Menon, V.; et al. Vitamin C Therapy for Routine Care in Septic Shock (ViCTOR) Trial: Effect of Intravenous Vitamin C, Thiamine, and Hydrocortisone Administration on Inpatient Mortality among Patients with Septic Shock. Indian J. Crit. Care Med. 2020, 24, 653–661. [Google Scholar] [CrossRef]
- Moskowitz, A.; Huang, D.T.; Hou, P.C.; Gong, J.; Doshi, P.B.; Grossestreuer, A.V.; Andersen, L.W.; Ngo, L.; Sherwin, R.L.; Berg, K.M.; et al. Effect of Ascorbic Acid, Corticosteroids, and Thiamine on Organ Injury in Septic Shock: The ACTS Randomized Clinical Trial. JAMA 2020, 324, 642–650. [Google Scholar] [CrossRef]
- Nathens, A.B.; Neff, M.J.; Jurkovich, G.J.; Klotz, P.; Farver, K.; Ruzinski, J.T.; Radella, F.; Garcia, I.; Maier, R.V. Randomized, prospective trial of antioxidant supplementation in critically III surgical patients. Ann. Surg. 2002, 236, 814–822. [Google Scholar] [CrossRef]
- Palli, E.; Makris, D.; Papanikolaou, J.; Garoufalis, G.; Tsilioni, I.; Zygoulis, P.; Zakynthinos, E. The impact of N-acetylcysteine and ascorbic acid in contrast-induced nephropathy in critical care patients: An open-label randomized controlled study. Crit. Care 2017, 21, s13054-017. [Google Scholar] [CrossRef] [Green Version]
- Reddy, P.R.; Aluru, N.; Yelle, S.; Rajyalakshmi, B. Metabolic Resuscitation Using Hydrocortisone, Ascorbic Acid, and Thiamine: Do Individual Components Influence Reversal of Shock Independently? Indian J. Crit. Care Med. 2020, 24, 649–652. [Google Scholar] [CrossRef]
- Sadeghpour, A.; Alizadehasl, A.; Kyavar, M.; Sadeghi, T.; Moludi, J.; Gholizadeh, F.; Totonchi, Z.; Ghadrdoost, B. Impact of vitamin C supplementation on post-cardiac surgery ICU and hospital length of stay. Anesthesiol. Pain Med. 2015, 5, e25337. [Google Scholar] [CrossRef] [Green Version]
- Siriwardena, A.K.; Mason, J.M.; Balachandra, S.; Bagul, A.; Galloway, S.; Formela, L.; Hardman, J.G.; Jamdar, S. Randomised, double blind, placebo controlled trial of intravenous antioxidant (n-acetylcysteine, selenium, vitamin C) therapy in severe acute pancreatitis. Gut 2007, 56, 1439–1444. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Wang, M.; Zhang, H.; Zhu, H.; Zhang, N.; Liu, J. Effect of intravenous injection of vitamin c on postoperative pulmonary complications in patients undergoing cardiac surgery: A double-blind, randomized trial. Drug Des. Devel. Ther. 2020, 14, 3263–3270. [Google Scholar] [CrossRef]
- Yanase, F.; Bitker, L.; Hessels, L.; Osawa, E.; Naorungroj, T.; Cutuli, S.L.; Young, P.J.; Ritzema, J.; Hill, G.; Latimer-Bell, C.; et al. A Pilot, Double-Blind, Randomized, Controlled Trial of High-Dose Intravenous Vitamin C for Vasoplegia After Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2020, 34, 409–416. [Google Scholar] [CrossRef]
- Nabil Habib, T.; Ahmed, I. Early Adjuvant Intravenous Vitamin C Treatment in Septic Shock may Resolve the Vasopressor Dependence. Int. J. Microbiol. Adv. Immunol. 2017, 5, 77–81. [Google Scholar] [CrossRef]
- Tanaka, H.; Matsuda, T.; Miyagantani, Y.; Yukioka, T.; Matsuda, H.; Shimazaki, S. Reduction of resuscitation fluid volumes in severely burned patients using ascorbic acid administration: A randomized, prospective study. Arch. Surg. 2000, 135, 326–331. [Google Scholar] [CrossRef] [Green Version]
- Galley, H.F.; Howdle, P.D.; Walker, B.E.; Webster, N.R. The effects of intravenous antioxidants in patients with septic shock. Free Radic. Biol. Med. 1997, 23, 768–774. [Google Scholar] [CrossRef]
- Razmkon, A.; Sadidi, A.; Sherafat-Kazemzadeh, E.; Mehrafshan, A.; Jamali, M.; Malekpour, B.; Saghafinia, M. Administration of vitamin C and vitamin E in severe head injury: A randomized double-blind controlled trial. Clin. Neurosurg. 2011, 58, 133–137. [Google Scholar] [CrossRef] [Green Version]
- Bansal, D.; Bhalla, A.; Bhasin, D.K.; Pandhi, P.; Sharma, N.; Rana, S.; Malhotra, S. Safety and efficacy of vitamin-based antioxidant therapy in patients with severe acute pancreatitis: A randomized controlled trial. Saudi J. Gastroenterol. 2011, 17, 174–179. [Google Scholar] [CrossRef]
- Luo, M.; Fernandez-Estivariz, C.; Jones, D.P.; Accardi, C.R.; Alteheld, B.; Bazargan, N.; Hao, L.; Griffith, D.P.; Blumberg, J.B.; Galloway, J.R.; et al. Depletion of plasma antioxidants in surgical intensive care unit patients requiring parenteral feeding: Effects of parenteral nutrition with or without alanyl-glutamine dipeptide supplementation. Nutrition 2008, 24, 37–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hemilä, H.; Chalker, E. Vitamin C Can Shorten the Length of Stay in the ICU: A Meta-Analysis. Nutrients 2019, 11, 708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, R.; Li, Z.H.; Chen, D.; Wu, Q.C.; Zhou, X.L.; Tie, H.T. Sole and combined vitamin C supplementation can prevent postoperative atrial fibrillation after cardiac surgery: A systematic review and meta-analysis of randomized controlled trials. Clin. Cardiol. 2018, 41, 871–878. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Questionnaires | Were the Two Groups Similar and Recruited from the Same Population? | Were the Exposures Measured Similarly to Assign People to Both Exposed and Unexposed Groups? | Was the Exposure Measured in a Valid and Reliable Way? | Were Confounding Factors Identified? | Were Strategies to Deal with Confounding Factors Stated? | Were the Groups/Participants Free of the Outcome at the Start of the Study (or at the Moment of Exposure)? | Were the Outcomes Measured in a Valid and Reliable Way? | Was the Follow Up Time Reported and Sufficient to Be Long Enough for Outcomes to Occur? | Was Follow Up Complete, and If Not, Were the Reasons to Loss to Follow Up Described and Explored? | Were Strategies to Address Incomplete Follow Up Utilized? | Was Appropriate Statistical Analysis Used? | Overall Appraisal |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ahn et al., 2019 [19] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | NA | Yes | Include |
| Bedreag et al., 2015 [20] | Yes | Yes | Yes | No | NA | Yes | Yes | Yes | Yes | NA | Yes | Include |
| Chang et al., 2020 [21] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | NA | Yes | Include |
| Coloretti et al., 2020 [22] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | NA | Yes | Include |
| Dingchao et al., 1994 [23] | Yes | Yes | Yes | No | NA | Yes | Yes | Yes | Yes | NA | Yes | Include |
| Giladi et al., 2011 [24] | Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes | NA | Yes | Include |
| Kahn et al., 2011 [25] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | NA | Yes | Include |
| Kim et al., 2018 [26] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | NA | Yes | Include |
| Lin et al., 2017 [27] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | NA | Yes | Include |
| Litwak et al., 2019 [28] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | NA | Yes | Include |
| Long et al., 2020 [29] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | NA | Yes | Include |
| Marik et al., 2017 [5] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | NA | NA | Yes | Include |
| Masood et al., 2019 [30] | NA | NA | Yes | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Include |
| Matsuoka et al., 2020 [31] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | NA | Yes | Include |
| Mitchell et al., 2020 [32] | No | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | NA | Yes | Include |
| Nagel et al., 2020 [33] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | NA | Yes | Include |
| Nakajima et al., 2019 [7] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | NA | Yes | Include |
| Park et al., 2020 [34] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | NA | Yes | Include |
| Sadaka et al., 2020 [35] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | NA | Yes | Include |
| Sandesc et al., 2018 [36] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | NA | Yes | Include |
| Shin et al., 2019 [37] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | NA | Yes | Include |
| Vail et al., 2020 [38] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | NA | Yes | Include |
| Yoo et al., 2020 [39] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | NA | Yes | Include |
| ID | Population | Intervention | Comparisons | Outcome |
|---|---|---|---|---|
| Abdoulhossein et al., 2018 [42] | N = 40 [T = 20, C = 20] Age (mean ± SD): T = 40.35 ± 8.94, C = 39.95 ± 9.05 Gender, n (%); Male: T = 14(70%), C = 12(60%) GCS, n (%) 13: T = 1 (5%) C = 1(5%) 14: T = 6 (30%) C = 5 (25%) 15: T = 13 (65%) C = 14 (70%) | Intravenous infusion vitamin C (500 mg in 50 mL normal saline) was administered by pump, steady, for up to 30 min along with standard of care. | The control group received intravenous infusion distilled water (5 mL in 50 mL of normal saline), by pump, steady, for up to 30 min. | ICU stay after intervention, days T = 5.5 ± 1.73 C = 5.2 ± 1.67 |
| Ahn et al., 2019 [19] | N = 75 T = 35 C = 40 Age, mean ± SD (years) T = 67.8 ± 12.1 C = 63.6 ± 15.3 Sex, male, n [%] T = 24 [43] C = 29 [44] APACHE II score T = 25.2 ± 6.1 C = 24.1 ± 6.0 Day 1 SOFA score T = 10.3 ± 3.3 C = 11.3 ± 3.1 Vasopressors, n [%] T = 33/35 [94] C = 40/40 [100] Hydrocortisone, n [%] T = 16/35 [45] C = 27/40 [46] Creatinine, mean ± SD, mg/dL T = 1.74 ± 1.81 C = 2.15 ± 1.81AKI, n [%] T = 21/35 [47] C = 28/40 [74] | A total of 2 g of vitamin C mixed in 50 mL of 5% dextrose solution or normal saline was administered intravenously over 30 min every 8 h until ICU discharge. | Treatment protocol based on the Surviving Sepsis Guidelines. Patients could receive hydrocortisone to maintain blood pressure if required. | 28-day mortality, n [%] T = 12/35 [34] C = 8/40 [20] 90-day mortality, n [%] T = 21/35 [48] C = 19/40 [49] ICU mortality, n [%] T = 12/35 [34] C = 12/40 [30] Hospital mortality, n [%] T = 16/35 [45] C = 16/40 [40] Shock reversal, days T = 3 [2,3,4,5] C = 3 [2,3,4,5] Mechanical ventilation, days T = 8 [5,6,7,8,9,10,11,12,13,14,15,16,17] C = 8 [4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19] ICU LOS, days T = 10 [6,7,8,9,10,11,12,13,14,15,16,17,18,19] C = 11 [7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35] Hospital LOS, days T = 23 [11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40] C = 41 [19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,45,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66] ΔSOFA score, first 4 ICU days T = −1.4 ± 3.3 C = −1.4 ± 3 RRT for AKI, n [%] T = 14/28 [55] C = 19/31 [65] Recovery from AKI, T = 13/28 [45] C = 16/31 [57] Total AKI, n T = 28/35 C = 31/40 New AKI during treatment: T = 7/35 C = 3/40 |
| Balakrishnan et al., 2018 [50] | N = 24 [T = 12, C = 12] Age, mean: T = 55.41 ± 15.70; C = 53.41 ± 8.27 Male, n (%) T = 8(66.6), C = 7(58.3) Euroscore II T = 1.95 ± 1.29 C = 2.78 ± 4.06 APACHE IV Score T = 60.91 ± 17.52 C = 51.81 ±10.76 | Intravenous vitamin C (1.5 g every 6 h for 4 days), hydrocortisone (50 mg every 6 h for 4 days) as well as intravenous thiamine (200 mg every 12 h for 4 days). The vitamin C was administered as an infusion over 30–60 min and mixed in a 50-milliliter solution of either 5% dextrose in water (D5W) or normal saline. | Received saline in a black syringe. | Urea (mg/dL) Day 1: T = 76.12 ± 47.18; C = 75.29 ± 46.96 Day 2: T = 79.85 ± 59.84; C = 71.03 ± 50.76 Day 3: T = 90.61 ± 66.78; C = 89.64 ± 59.73 Day 4: T = 89.58 ± 56.55; C = 93.43 ± 52.48 Creatinine (mg/dL) Day 1: T = 2.73 ± 2.16; C = 1.52 ± 0.79 Day 2: T = 2.17 ± 1.33; C = 1.43 ± 0.81 Day 3: T = 2.24 ± 1.33; C = 1.59 ± 0.75 Day 4: T = 2.25 ± 1.46; C = 1.68 ± 0.84 |
| Bedreag et al., 2015 [20] | N = 34 [T = 20 C = 14] Gender, % male; T = 75 C = 85.71 Age, mean (SD), years T = 52 (14.5) C = 53.8 (20.9) APACHE II, mean (SD) T = 10.7 (5.8) C = 10.8 (7.6) ISS, mean (SD) T = 26.1 (8,4) C = 31.1 (9.4) GCS < 7, n (%) T = 1 (5) C = 6 (42.8) Urea (mg/dL), T = 59.5 (10.5) C = 64.1 (3.1) | Antioxidant therapy consisted of the administration of vitamin C, vitamin B1 and N-acetylcysteine (NAC).All patients received vitamin C (i.v): 1 g three times daily, for 5 days; vitamin B1 (i.v.): 100 mg daily for 3 days; and N-Acetylcysteine (i.v.): 300 mg twice a day, for the whole period of the ICU stay. | Standard of care. | Incidence of sepsis T = 8/20 C = 9/14 LOS in ICU T = 11.7 ± 11.9, C = 13.2 ± 13.9 Mortality T = 6/20 (30%) C = 9/14 (64.2%) Urea (mg/dL), mean (SD) at discharge from ICU T:27.8 (10.5); C: 57.1 (20.8) |
| Chang K et al., 2020 [21] | N = 140 T = 52 C = 88 Age, mean (SD) T = 63.9 (15.7) C = 63.6 (14.5) Female, n (%) T = 21 (40) C = 34 (39) APACHE IV, T = 95.1 (32.3) C = 86.1 (28.4) SOFA, T = 9.9 (3.8) C = 8.6 (3.1) Vasopressors, n (%) T = 51 (98) C = 85 (97) | Vitamin C at a dose of at least 1500 mg every six hours for up to 96 h. | Patients were treated following the Surviving Sepsis Campaign guidelines. | Hospital death, n (%) T = 20/52(39) C = 32/88 (36) ICU death, n (%) T = 16/52 (31) C = 20/88 (23) Ventilator-free days, T = 16.0 (11.8) C = 17.8 (11.8) Vasopressor-free days, T = 16.9 (11.8) C = 19.7 (11.5) ICU LOS, mean (SD) T = 11.1 (13.3) C = 9.3 (11.7) Dialysis, n (%) T = 23/52 (44) C = 39/88 (44) Vasopressors, n (%) T = 51 (98) C = 85 (97) |
| Chang P et al., 2020 [51] | N = 80 T = 40 C = 40 Age, y T = 59.5 ± 15.0 C = 63.7 ± 12.8 Sex, male T = 22 (57.5) C = 21 (52.5) Mechanical ventilation T = 30 (75) C = 32 (80) Vasopressors T = 22 (55) C = 24 (60) SOFA score T = 9.6 ± 4.5 C = 10.1 ± 4.0 APACHE II score T = 22.1 ± 8.4 C = 23.8 ± 7.6 CRF n (%) T = 4/40 (10) C = 5/40 (12.5) AKI n (%) T = 17/40 (42.5) C = 21/40 (52.5) | IV hydrocortisone (50 mg every 6 h for 7 days or until ICU discharge, whichever occurred first), vitamin C (1.5 g every 6 h for 4 days or until ICU discharge, whichever occurred first), and IV thiamine (200 mg every 12 h for 4 days or until ICU discharge, whichever occurred first) | Same frequency and volume of saline. | 28-d mortality T = 11/40 (27.5) C = 14/40 (35) ICU LOS, d T = 7.5 (4–12.8) C = 7.5 (4–11.8) Duration of vasopressors, h T = 46 (23.8–102.5) C = 58.5 (28–104) New AKI after entering ICU T = 1/40 (2.5) C = 2/40 (5) Change in SOFA score, 72 h T = 3.5 ± 3.3 C = 1.8 ± 3.0 Duration mechanical ventilation, h T = 126.5 (63.5–239.3) C = 94.5 (39.8–211) Lactate clearance, 72 h, % T = 21.3 (−49.7 to 44.2) C = 0 (−35.1 to 47.7) |
| Coloretti et al., 2020 [22] | N = 112 T = 56 C = 56 Age (years) T = 69 (56–76) C = 69 (56–77) Male n(%) T = 37 (66.1) C = 32 (57.1) SAPS II score T = 61 (47–72) C = 56 (47–71) SOFA score T = 11 (8–12) C = 11 (8–13) Medical admission n(%) T = 36 (64.3) C = 33 (58.9) | Use of intravenous vitamin C at the dosage of 1.5 g every 6 h and thiamine at the dosage of 200 mg every 12 h up to discontinuation of vasoactive drugs or steroids. | Current sepsis management guidelines. | 30-day mortality n (%) T = 24/56 (42.8) C = 28/56 (50.0) Hospital mortality n (%) T = 28/56(50.0) C = 34/56 (60.7); Mechanical ventilation: T: 41/56; C: 48/56 Vasopressors length (days) T = 3 (2–5) C = 4 (2–7) Mechanical ventilation (days) T = 3 (0–8) C = 6 (2–15) RRT n(%) T = 22/56 (39.2) C = 21/56 (37.5) ICU LOS (days) T = 6 (4–10) C = 9 (5–15) |
| Dingchao et al., 1994 [23] | N = 85 [T = 45 C = 40] There were no significant differences in age, weight, CPB time and aortic clamping time between the two groups. | Receiving 250 mg/kg of ascorbic acid. Ascorbic acid was introduced intravenously 30 min before CPB and at the aortic decamping (125 mg/kg each time). | Standard of care without ascorbic acid. | ICU stay (hour) T = 25 ± 4.7 C = 45 ± 8.5 Hospital stay (day) T = 22 ± 4.0 C = 35 ± 5.9 |
| Du et al., 2003 [52] | N = 84 [ T = 40, C = 44] Age, mean years T = 40 ± 12 C = 43 ± 14 Gender (M/F) T= 25/15 C = 28/16 | In the treatment group, vitamin C (10 g/day) was given intravenously for 5 days, high dose. | In the control group (n = 44), vitamin C (1 g/day) was given intravenously for 5 days (Low dose). | Hospital LOS T = 9.34 ± 4.24 C = 13.45 ± 3.21 |
| Emadi et al., 2019 [45] | N = 50 [T = 25 C = 25] Age (years) T = 60 ± 6.62 C = 63.64 ± 8.26 Gender (male/female) (%) T = 72/28 C = 56/44 | Received 5 g of intravenous vitamin C before induction of anesthesia and 5 g of vitamin C in the cardioplegic solution. | Given the same amount of placebo (normal saline). | Intubation time (h) T = 10.76 ± 2.14 C = 11.72 ± 2.57 ICU stay (days) T = 1.22 ± 0.27 C = 1.58 ± 1.18 Hospital stay (days) T = 4.12 ± 0.33 C = 5.16 ± 3.44 |
| Fowler et al., 2014 [3] | N = 26 [TH = 8, TL = 8, C = 8] Gender(M/F): TH = 4/4 TL = 5/3 C = 4/4 Age, range in years TH = 49–92 TL = 30–70 C = 54–68 APACHE II score, mean (range). TH = 24.0 (12–33) TL = 20.4 (12–23) C = 20.4 (15–29) SOFA score, mean ± SE. TH = 10.8 ± 4.4 TL = 10.1 ± 2.0 C = 13.3 ± 2.9 | Low dose ascorbic acid (Lo-AscA): TL 50 mg/kg/24 h High dose ascorbic acid (Hi-AscA) TH: 200 mg/kg/24 h. Ascorbic acid dosage was divided into 4 equal doses and administered over 30 min every 6 h for 96 h in 50 mL of 5% dextrose and water. Study drug infusion was initiated 2–4 h following informed consent and randomization. | Placebo: 5% dextrose and water. | Days on Vasopressor, mean (range) TH = 3.6 (2–8); TL = 2.1 (1–6); C = 3.9 (1–10) Ventilator Free Days, mean (range) TH = 4.8 (0–19); TL = 8.4 (0–22); C = 7.6 (0–23) ICU Length of Stay, mean (range) TH = 9.1 (2–25); TL = 8.1 (1–19); C = 11.0 (2– 25) 28-Day mortality, TH = 4/8 (50.6%); TL = 3/8 (38.1%); C = 5/8 (62.5%) |
| Fowler et al., 2019 [4] | N = 167 [T = 84 C = 83] Age, median (IQR), y T = 54 (39–67) C = 57 (44–70) Gender, number (%) Men T = 45 (54) C = 45 (54) Women T = 39 (46) C = 38 (46) Incidence of shock, No. (%) At baseline, vasopressor in use T = 57 (68) C = 60 (72) SOFA scores, mean (SD) At randomization T = 9.8 (3.2) C = 10.3 (3.1) At 96 h T = 8.02 (4.2) C = 6.96 (3.5) Corticosteroid use during study, No. (%) T = 56 (67) C = 54 (65) | Vitamin C at 50 mg/kg actual body weight infused intravenously every 6 h for total 96 h in 5% dextrose in water. | Placebo (5% dextrose in water alone). | All-cause mortality in 28 days, T = 25/84 C = 38/82 The ventilator-free days T = 13.1 C = 10.6 The ICU-free days to day 28 T = 10.7 C = 7.7 Transfer out of the ICU by hour 168 or less T = 21/84 C = 10/83 The hospital-free days T = 22.6 C = 15.5 Creatinine 0 h: T = 1.1(1.3)C = 1.7(1.8)48 h: T (82) = 1.6 (1.4); C(73) = 1.2 (1.0) 96 h: T(78) = 1.1(1.1); C(65) = 1.1(0.9) 168 h: T(64) = 1.0(1.2); C(55) = 1.2 (1.6) |
| Fujii et al., 2020 [53] | N = 211 T = 107 C = 104 Age, mean (SD), y T = 61.9 (15.9) C = 61.6 (13.9) Sex, No. (%) Male n (%) T = 68 (63.6) C = 65 (62.5) Female (%) T = 39 (36.4) C = 39 (37.5) Weight, median (IQR), kg T = 81.0 (66.0–95.0) C = 83.0 (67.5–102.0) Mechanical ventilation T = 66 (61.7) C = 65 (62.5) Norepinephrine T = 99 (92.5) C = 97 (93.3) Vasopressin T = 22 (20.6) C = 22 (21.2) Epinephrine T = 13 (12.1) C = 9 (8.7) Metaraminol T = 8 (7.5) C = 10 (9.6) Inotropes Milrinone T = 6 (5.6) C = 2 (1.9) RRT T = 12 (11.2) C = 12 (11.5) AKI, No. (%)h T = 74 (69.2) C = 75 (72.1) Stage 1 (mild) T = 27 C = 32 Stage 2 (moderate) T = 34 C = 23 Stage 3 (severe) T = 13 C = 20 APACHE III score T = 77.4 (29.7) C = 83.3 (28.8) SOFA score T = 8.6 (2.7) C = 8.4 (2.7) Serum creatinine, Median (IQR), mg/dL T = 1.73 (1.16–2.64); C = 1.78 (1.07–2.90) | IV vitamin C (1.5 g every 6 h), hydrocortisone (50 mg every 6 h) and thiamine (200 mg every 12 h). | Received IV hydrocortisone (50 mg every 6 h). | 28-d Mortality, No. (%) T = 24/106 (22.6) [n = 106] C = 21/103 (20.4) [n = 103] 90-d Mortality, No. (%) T = 30/105 (28.6) [n = 105] C = 25/102 (24.5) [n = 102] ICU mortality, No. (%) T = 21/107 (19.6) C = 19/104 (18.3) Hospital mortality, No. (%) T = 25/107 (23.4) C = 21/103 (20.4) [n = 103] 28-d Cumulative vasopressor-free days, median (IQR) T = 25.6 (17.8 to 26.8) [n = 106] C = 25.8 (19.6 to 26.8) [n = 103] 28-d Cumulative MV-free days, median (IQR) T = 25.3 (5.2 to 28.0) [n = 106] C = 24.8 (9.5 to 28.0) [n = 103] 28-d RRT–free days, T = 28.0 (23.5 to 28.0) [n = 105] C = 28.0 (21.0 to 28.0) [n = 103] 28-d ICU-free days, T = 21.9 (0 to 25.8) [n = 106] C = 22.1 (3.9 to 25.8) [n = 103] Hospital LOS, d T = 12.3 (6.2 to 26.0) [n = 106] C = 12.3 (6.2 to 26.1) [n = 103] AKI (1,2,3) T = 75/107, C = 75/104 Stage 1 T = 18/107 (16.8) C = 14/104 (13.5) Stage 2 T = 18/107 (16.8) C = 22/104 (21.2) Stage 3 T = 39/107 (36.4) C = 39/104 (37.5) |
| Giladi et al., 2011 [24] | N = 4294 T = 2272 C = 2022 Male n (%) T = 1832 (81%) C = 1452 (72%) White race n (%) T = 1291 (79%) C = 1587 (78%) Mean age, years (SD) T = 40 ± 17 C = 39 ± 18 Mean admission GCS (SD) T = 12 ± 5 C = 13 ± 4 Mean ISS (SD) T = 20 ± 12.3 C = 21 ± 12.6 Mean predicted survival(SD) by TRISS methodology T = 0.822 ± 0.285 C = 0.885 ± 0.222 Renal failure, n (%) T = 30/2272 (1.3%) C = 26/2022 (1.3%) | Intravenous ascorbic acid 1000 mg intravenously in 100 mL of NS every 8 h, alpha-tocopherol 1000 IU (1 mL) via naso- or orogastric tube every 8 h, and selenium 200 mcg intravenously in 100 mL NS once daily. Ascorbic acid was administered as a bolus over 1 h and selenium as a bolus over 2 h, although both were permitted to be changed to an enteral dosage form once enteral access was established. The treatment course was 7 days or until discharge from hospital, whichever came first. | No antioxidants, only standard of care. | Mortality: T = 139/2272(6.1%) C = 172/2022(8.5%) ICU-LOS days, (IQR) T = 2 (1–4) C = 3 (1–6) Hospital LOS, days,(IQR) T = 3 (1–6) C = 4 (2–8). Ventilator free days (IQR) T = 3 (1–6) C = 3 (1–6). Respiratory failure, n (%) T = 395/2272 (17.4%) C = 558/2022 (27.6%) Ventilator-dependent respiratory failure, n (%) T = 160/2272 (7.1%) C = 218/2022 (10.8%) Renal failure, n (%) T = 30/2272 (1.3%) C = 26/2022 (1.3%) SIRS, n (%) T = 360/2272 (15.0%) C = 283/2022 (13.8%) ICU subset analysis Hospital stay T = 8.8 days C = 10.6 days ICU stay T = 3.9 days C = 4.9 days |
| Hwang et al., 2020 [49] | N = 111 T = 53 C = 58 Age (years) T = 70 (62–76)C = 69 (62–74) Sex (male) T = 20 (37.7) C = 22 (37.9) Chronic renal disease T = 3 (5.7) C = 0 (0) SOFA score T = 8 (6–10) C = 8 (6–10) APACHE II score T = 22 (14–32) C = 22 (17–32) Acute kidney injury Stage 1 T = 13/53 (24.5) C = 15/58 (25.9) Stage 2 T = 13/53 (24.5) C = 17/58 (29.3) Stage 3 T = 15/53 (28.3) C = 13/58 (22.4) Mechanical ventilation at enrolment T = 12 (22.6) C = 14 (24.1) | Vitamin C (50 mg/kg, maximum single dose 3 g, daily dose 6 g) and thiamine (200 mg) were mixed in a 50-milliliter 0.9% saline bag, respectively, and intravenously administered to patients over 60 min every 12 h for a total of 48 h. | Identical volume of 0.9% saline from the placebo drug ampoule was administered to patients using the same protocol. | 7-day mortality T = 5/53 (9.4) C = 6/58 (10.3) 28-day mortality T = 11/53 (20.8) C = 9/58 (15.5) 90-day mortality T = 17/53 (32.1) C = 16/58 (27.6) In-hospital mortality T = 13/53 (24.5) C = 11/58 (19) ICU mortality T = 7/46 (15.2) C = 7/52 (13.5) Shock reversal T = 44/53 (83) C = 49 /58(84.5) Vasopressor-free days T = 11 (5–12) C = 11 (10–12) Mechanical ventilation (days) T = 6 (3–12) [n = 23] C = 7 (3–8) [n = 24] Ventilator-free days T = 11 (2–14) C = 11 (3–14) New use of RRT T = 9/52 (17.3) C = 11/58 (19) RRT-free days T = 14 (14–14) [n = 52] C = 14 (14–14) [n = 58] ICU LOS (day) T = 5 (3–11) [n = 46] C = 5.5 (4–12.5) [n = 52] ICU-free days T = 9 (3–11) C = 9 (0–11) Hospital LOS (day) T = 14 (11–21) C = 13.5 (9–26) |
| Iglesias et al., 2020 [54] | Total patients (N) = 137 T = 68 C = 69 Age T = 70 ± 12 C = 67 ± 14 Sex (male) T = 32 (47%) C = 27 (39%) ESRD T = 3 (0.4%) C = 0 (0%) CKD T = 10 (7%) C = 4 (2.9%) Mechanical ventilation T = 34 (50%) C = 35 (51%) Vasopressors T = 56 (82%) C = 47 (68%) AKI T = 54 (79%) C = 52 (75%) Day 1 SOFA T = 8.3 ± 3 C = 7.9 ± 3.5 APACHE II T = 24 ± 7.6 C = 24.9 ± 8.7 APACHE IV T = 88 ± 28.3 C = 87.5 ± 29.7 | Ascorbic acid 1500 mg q 6 h, thiamine 200 mg every 12 h and hydrocortisone 50 mg q6 h. | A matching saline placebo for a maximum of 4 days. | Days of HAT therapy or placebo T = 3.3 ± 0.8 C = 3.25± 1 Vasopressor after study enrollment T = 4 (6%) C = 10 (14.5%) RRT for AKI T = 2/68 (3%) C = 8/69 (11.5%) ΔSOFA score at 72 h T = 2.9 ± 3.3 C = 1.93 ± 3.5 Duration of vasopressors, h T = 27 ± 22 C = 53 ± 38 Hospital mortality (%) T = 11/68 (16%) C = 13/69 (19.4%) ICU mortality (%) T = 6/68 (9%) C = 10/69 (14%) Hospital LOS, d T = 11.5 ± 6.8 C = 11 ± 6.2 ICU LOS, d T = 4.76 ± 4.3 C = 4.66 ± 3.45 Ventilator-free days T = 22 ± 6.2 C = 22.4 ± 4.3 AKI T = 54/68 (79%) C = 52/69 (75%) (Serum creatinine (mg/dL) SCr 24 h T = 1.74± 1.21 C = 1.85 ± 1.6 SCr 48 h T = 1.62± 1.32 C = 1.8± 1.71 SCr 72 h T = 1.47± 1.3 C = 1.67 ± 1.71 SCr at discharge T = 1.32± 1.13 C = 1.37± 1.18 |
| Kahn et al., 2011 [25] | N = 33 [T = 17, C = 16] Age (yr) T = 42 ± 16 C = 50 ± 20 Male T = 16 C = 16 APACHE II T = 17 ±7 C = 18 ±8 Inhalation: T = 4 C = 4 | LR based on Parkland formula with 66 mg/kg/hr VC administered during resuscitation until the patient was down to maintenance fluid (approximately 24 h). | LR solution only according to the Parkland formula. | Mortality T = 4/17 C = 3/16 Need of vasopressors, mean hours T = 6 ± 9, C = 11 ± 10 Renal failure: T = 2/17 C = 2/16 Pneumonia: T = 7/17 C = 10/16 Fasciotomy: T = 3/17 C = 3/16 |
| Kim et al., 2018 [26] | N = 99 T = 53 C = 46 Male: T = 41 (77) C = 29 (63) Chronic kidney disease: T = 8 (15) C = 8 (17) ARDS at ICU admission T = 12 (23) C = 10 (22) APACHE II score at ICU admission T = 28 (21−32) C = 27 (22−32) SOFA score at ICU admission T = 11 (8–14) C = 11 (7–12) Use of MV in 1st day T = 43 (81) C = 36 (78) Vasopressor use in 1st day T = 33 (62) C = 22 (48) Use of RRT in 1st day T = 19 (36) C = 5 (11) Creatinine, mg/dL T = 1.1 (0.7–1.9) C = 0.8 (0.6–1.6) | Treatment group was treated with vitamin C protocol. The protocol consisted of intravenous vitamin C (1.5 g every 6 h for 4 days), hydrocortisone (50 mg every 6 h for 7 days followed by a taper over 3 days) and intravenous thiamine (200 mg every 12 h for 4 days). Treatment group was administered 6 g of vitamin C per day (divided into four equal doses). | The patients who were admitted to the same ICU between June 2016 and January 2017 were not treated with the vitamin C protocol and thus formed the control group. | At 28-day vasopressor-free days; T:18.8 ± 11.2, C: 19.6 ± 11.4 At 28-day ventilator-free days T: 10.7 ± 10.8, C:9.7 ± 10.9 ICU stay, d T:9 (4–14); C:12 (6–17) Hospital mortality: T:11/53 (21); C:17/46 (37) Among PPM cohort (T = 36, C = 36) At 28-day vasopressor-free; T = 19.8 ± 10.8, C = 20.5 ± 11.1 At 28-day ventilator-free days; T = 12.3 ± 11.0, C = 9.9 ± 10.7ICU stay, d T = 9 (5–14) C = 12 (7–17) Hospital mortality T = 6 (17) C = 14 (39) |
| Lin et al., 2018 [27] | N = 80 T = 38 C = 42 Age T = 41 ± 15 C = 42.4 ± 17 Inhalation injury T = 52% C = 36% Admission BUN (mg/dL) T = 12 (7–17) C = 12 (9–15) Admission Cr (mg/dL) T = 1.18 ± 0.6 C = 1.26 ± 0.5 mg/d | High dose ascorbic acid was started for Burn Shock Resuscitation at a dose of 66 mg/kg/hr, along with BSR based on Parkland formula calculations and received lactated Ringers for resuscitation. | Burn shock resuscitation (BSR) based on Parkland formula calculations and received lactated Ringers for resuscitation. | Mortality T = 10/38(26%) C = 10/42(24%) Ventilator days T = 11 (6–28) C = 5.5 (1–22) Hospital LOS (days) T = 29 (18–57) C = 24.5 (14–46) Abdominal Compartment Syndrome (ACS) T = 2/38 (5.2%) C = 1/42 (2.3%) AKI T = 9/38 (23%) C = 3/42 (7%) Ventilator-Associated Pneumonia (VAP) T = 11/38 (29%) C = 6/42 (14%) day 1 BUN (mg/dL) T = 12 (7–15) C = 12 (6–17) day 1 Cr (mg/dL) T = 1.26 ± 0.6 C = 1.42 ± 0.5 mg/d |
| Litwak et al., 2019 [28] | N = 94 (T = 47 C = 47) Age, mean SD, year T = 58.3 ±17.0 C= 60.1 ±14.0 Sex, male, No (%) T = 28 (59.6) C = 29 (61.7) CKD T = 4 (8.5) C = 10 (21.3) Mechanical ventilation, No (%) T = 43 (91.5) C = 39 (83.0) Vasopressors, No (%) T = 47 (100) C = 47 (100) AKI, No (%) T = 38 (80.9) C = 32 (68.1) Day 1 SOFA, mean SD T = 10.6 ± 10.6 C= 9.7 ± 10.0 APACHE II, mean SD T = 21.5± 8.0 C = 20.0 ±7.4 APACHE IV, T = 88.6 ± 29.1 C = 84.1 ± 25.4 Creatinine, median (IQR), mg/dL (excluding CKD) T = 1.4 (0.9–2.2) C = 1.4 (0.9–2.5) | At least one dose of each of the following medications intravenously: 1.5 g vitamin C every 6 h, 200–300 mg hydrocortisone daily (50 mg every 6 h or 100 mg every 8 h) and thiamine 200 mg every 12 h. | Standard of care but could receive hydrocortisone. | Hospital mortality T = 19/47 C = 19/47 ICU mortality T = 17/47 C = 18/47 RRT for AKI T= 11 of 38 C = 11 of 32 ICU LOS, days T = 11.0 (7.0–19.0) C = 10.0(5.0–17.0) Hospital LOS, days T = 19.0(9.0–26.0) C = 14.0 (8.0–23.0) Vasopressors, hours T = 84.2(37.0–169.3) C = 62.5(32.6–105.9) Change in SOFA score in 72 h, mean ± SD T = 1.3 ± 4.1 C= 0.1 ± 4.7 Sub group analysis Hospital mortality T = 7/20 C = 19/47 ICU mortality T = 6/20 C = 18/47 RRT for AKI T = 5 of 16 C= 11 of 32 ICU LOS days T = 14.5(7.5–22.0) C = 10.0 (5.0–17.0) Hospital LOS, days T = 19.0(9.3–23.5) C = 14.0(8.0–23.0) |
| Long et al., 2020 [29] | N = 206 T = 79 C = 127 Age, Yrs (mean, SD) T = 64.4 (13.9) C = 61.1 (16.2) Male gender n,% T = 43 (54.4) C = 71 (55.9) ESRD T = 5/79 (6.3) C = 17/127(13.4) Ventilator initiation, n, % T = 33 (41.7) C = 71 (55.9) Hydrocortisone use, n,% T = 79(100) C= 40 (31.5) | Hydrocortisone 50 mg IV every 6 h, vitamin C in a dose of 1.5 g IV every 6 h and thiamine 200 mg IV every 12 h, until the patient was either liberated from vasopressors, was discharged from the ICU or until 4 days of therapy had elapsed, whichever came first. | Standard of care: Surviving Sepsis Campaign Guidelines. | APACHE IV score T = 80.0 C = 88.2Observed ICU mortality, N (%) T = 9/79 (11.4) C = 33/127 (26.0) Hospital mortality T = 21/79 (26.6) C = 41/127 (32.3) Vasopressor duration, hours(median)T = 13.9 C = 24.2 New RRT initiation n (%)T = 11/74 (14.9%) C = 29/110 (26.4%) Ventilator duration days T = 3.4 C = 3.3 ICU LOS, days(median) T = 2.0 C = 2.5 Hospital LOS, days(median)T = 9.5 C = 9.1 |
| Lv et al., 2020 [55] | N = 117 T = 61 C = 56 Sex, male, n (%) T = 30 (49.2) C = 29 (51.8) Age, mean ± SD, T = 58.7 ± 14.3 C = 60.2 ± 14.1 CRF, n (%) T = 3 (4.9) C = 4 (7.1) Ventilator, n (%) T = 31 (50.8) C = 28 (50.0) Vasoactive drugs, n (%) T = 35 (57.4) C = 33 (58.9) AKI, n (%)T = 29/61 (47.5) C = 27/56 (48.2) APACHE II, Median [IQR] T = 21.0 (19.0, 28.0) C = 23.0 (20.0, 29.0) Day 1 SOFA, mean ± SD T = 8.6 ± 2.9 C = 8.9 ± 3.1 | Vitamin C from the day of entering ICU, administered intravenously by 3.0 g of vitamin C dissolved into 5% dextrose (100 mL/time, 2 times/day) until ICU discharge. | Intravenously by 5% dextrose (100 mL/time, 2 times/day) as placebo. | 28-day mortality (%) T = 15/61 (24.6) C = 24/56 (42.9) ICU stay, day, Median [IQR] T = 4.1 (3.2, 8.3) C = 3.9 (3.1, 7.5) SOFA after72 h Median [IQR] T = 4.2 (1.2, 6.6) C = 2.1 (1.1, 4.3) Application time of vasoactive drugs [h, (IQR)] T = 25.6 (18.8, 40.6) C = 43.8 (24.7, 66.8) |
| Marik 2017 [5] | N = 94 [T = 47 C = 47] Sex, male, n T = 27 C = 23 Ventilation, N (%) T = 22 (47) C = 26 (55) Vasopressors, N (%) T= 22 (46) C = 22 (46) AKI, N (%)T = 31/47 (66) C = 30/47 (64) Day 1 SOFA, mean ± SD; T = 8.3 ± 2.8 C = 8.7 ± 3.7 APACHE II, mean ± SD; T= 22.1 ± 6.3 C = 22.6 ± 5.7; CRF T = 7/47 (15) C = 8/47 (17) Creatinine mean ±SD, mg/dL T = 1.9 ± 1.4 C = 1.9 ± 1.1 | Intravenous vitamin C (1.5 g every 6 h for 4 days or until ICU discharge), hydrocortisone (50 mg every 6 h for 7 days or until ICU discharge followed by a taper over 3 days), as well as intravenous thiamine (200 mg every 12 h for 4 days or until ICU discharge). | Patients received hydrocortisone (50 mg every 6 h) at the discretion of the attending physician and all standard of care. | Hospital mortality, N; T = 4/47 C= 19/47 ICU LOS, median and IQR, d T = 4 (3–5) C = 4 (4–10) Vasopressors, mean ± SD, h T= 18.3 ± 9.8 C = 54.9 ± 28.4 Change in SOFA, 72 h T = 4.8 ± 2.4 C = 0.9 ± 2.7 RRT for AKI, No. (%) T = 3/31 (10%) C = 11/30 (33%) |
| Masood et al., 2019 [30] | N = 50 Mean age: 46.7 ± 18.4 (range: 16 to 77 years old) Gender: Male 28 (56); Female 22 (44) | IV thiamine 200 mg BD for 5 days along with IV vitamin C 1500 mg QID and IV hydrocortisone 50 mg QID for 5 days. | - | Median days in ICU= 8.3 [IQR = 5] Mortality, N = 24/50 (48%) SOFA score= 8.5 ± 1.5 Duration of vasopressor support < 24 h = 29 (58%) 24–48 h = 13 (26%) |
| Matsuoka et al., 2020 [31] | N = 17 T = 6 C = 11 Age (years) T = 67.7 ± 1.4 C = 69.7 ± 2.3 Male N (%) T = 4 (67) C = 10 (91) Both group received Methyl-prednisolone | Received ascorbic acid (1.5 g) and thiamine (200 mg) as per protocol. | Standard postoperative management. | Ventilation (days): T = 2.0 ± 0.0; C = 4.2 ± 0.3 ICU LOS (days): T = 3.2 ± 0.3; C = 6.9 ± 0.9 ARDS: T = 0 (0) C = 1 (9) Pneumonia T = 2 (33) C = 5 (45) |
| Mirmohammadsadeghi et al., 2018 [56] | N = 314 T = 160 C = 154 Age (mean years) T = 62.1 C = 62.7 Age >70 years T = 5 C = 6 Gender (male) T = 128 C = 116 | 2 g of vitamin C intravenously (IV) 24 h preoperatively, and postoperatively 500 mg every 12 h IV for 48 h in ICU, and 500 mg every 12 h PO for 48 h in ward. | Standard of care. | Postoperative stroke (%) T = 3/160 (1.9) C = 1/154 (0.7) Postoperative TIA (%) T = 0/160 (0) C = 2/154 (1.3) ICU stay (hours) T = 50.4 C = 52.5 Hospital stay (days) T = 8.13 C = 8.22 Atrial fibrillation (patients) T = 12/160 C = 12/154 Inotrope dependent T = 37/160 C = 39/154 |
| Mitchell et al., 2019 [32] | N = 76 T = 38 C = 38 Mean age, years ± SD T = 68 ± 10 C = 68 ± 10 Male, n (%) T = 36 (95) C = 37 (97) Mean SOFA score ± SD T = 6.9 ± 4 C = 6 ± 3 Need for vasopressors, n (%) T = 30 (79) C = 29 (76 Ventilation, n (%) T = 19 (50) C = 17 (45) CKD/ESRD T = 9/38 (24) C = 8/38 (21) | Vitamin C was administered at a dose of 1.5 g IV every 6 h and thiamine 200 mg IV every 12 h for 4 days in addition to hydrocortisone. | IV prednisolone alone. | ICU mortality n (%) T = 12/38 (32) C = 13/38 (34) Hospital mortality n (%) T = 18/38 (47) C = 20/38 (53) 28 day Mortality n (%) T = 22/38 (58) C = 23/38 (61) 60 day Mortality n (%) T = 22/38 (58) C = 25/38 (66) AKI requiring RRT, n (%) T = 6/38 (16) C = 7/38 (18) Vasopressor duration, days T = 2.5 C = 4.8 Hospital LOS, days T = 20 C = 32.6 ICU LOS, days T = 7.1 C = 15.6 |
| Mohamed et al., 2020 [57] | N = 88 T = 45 C = 43 Age, mean T = 58.69 ± 14.89 C = 59.37 ± 15.01 Male T = 31 (69) C = 32 (74) CKD T = 6 (14) C = 11 (25) GCS T = 15 (2–15) C = 15 (2–15) SOFA T = 11.22 ± 2.99 C = 10.89 ± 3.82 Creatinine (mg/dL) T = 2.8 ± 1.6 C = 2.5 ± 1.9 | Intravenous hydrocortisone (50 mg every 6 h), vitamin C (AA) (1.5 g every 6 h) and thiamine (200 mg every 12 h) for 4 days. | Standard of care for septic shock. | Mortality (%) T = 26/45 (57) C = 23/43 (53) Reversal shock (hrs) T = 34.58 ± 22.63 C = 45.42 ± 24.4 Mechanical ventilation T = 22 (48.8) C = 20 (46.5) SOFA at 72 h T = 8.9 ± 3.6 C = 9.3 ± 3.8 Change in SOFA T = 2.23 ± 2.4 C = 1.38 ± 3.1 New onset of AKI T = 7/45 (15) C = 5/43 (12) ICU LOS T = 12.44 ± 14.2 C = 8.44 ± 8.16 Hospital LOS T = 31.58 ± 31.06 C = 20.9 ± 15.01 |
| Moskowitz et al., 2020 [58] | N = 200 T= 101 C= 99 Age, mean y, (SD) T = 68.9 (15.0) C = 67.7 (13.9) Sex, Female T = 44 (43.6) C = 45 (45.5) Chronic kidney disease stage 2 (Mild) T = 1 (1.0) C = 1 (1.0) 3 (Moderate) T = 4 (4.0) C = 6 (6.1) 4 (Severe) T = 2 (2.0) C = 3 (3.0) Unknown 3 (3.0)3 (3.0) SOFA mean (SD) T = 9.1 (3.5) C= 9.2 (3.2) Ventilation, No. (%) T = 48 (47.5) C = 44 (44.4) | Ascorbic acid (1500 mg), hydrocortisone (50 mg) and thiamine (100mg) every 6 h for 4 days or until intensive care unit (ICU) discharge. Hydrocortisone was administered intravenously as a push dose in 1 mL of saline over 1 to 2 min. | 0.9% sodium chloride in a matching volume (approximately 100 mL) using the same techniques at the same time points. | SOFA score at 72 h, mean (SD): T = 4.4 (4.1) [n = 90] C = 5.1 (4.3) [n = 88] 30 d, Mortality n (%) T = 35/101 (34.7) C = 29/99 (29.3) AKI n (%) T = 32/101(31.7) C = 27/99 (27.3) Ventilator-free days, median (IQR) T = 6 (2–7) C = 6 (0–7) Shock-free days, median (IQR) T = 5 (3–5) C = 4 (1–5) Incidence of delirium, No./total (%) T = 31/83 (37.4) C = 35/76 (46.1) ICU-free days, median (IQR) T = 22 (3–25) C = 21 (4–25) |
| Nagel et al., 2020 [33] | N = 38 T = 19 C = 19 Age (years) T = 47 ± 18.8 C = 49 ± 17.9 Gender (female:male) T = 6 13 C = 6:13 ABSI(abbreviated burn severity index) T = 7 (5–12) C = 7 (4–12) Admission Crea (mg/dL): T = 0.99 ± 0.34 C= 1.14 ± 0.64 | High dose ascorbic acid was infused continuously over 24 h with 66 mg/kg per hour intravenously. | Low dose ascorbic acid 3.5 g as a single infusion. | Mortality (%) T (HDAA) = 5/19 (26.3) C (LDAA) = 2/19 (10.5) 24-hr Vasopressor use (%) T = 5/19 (26.3) C = 8/19(42.1) 24–72 hrs Vasopressor use T = 5/19(26.3); C = 10/19 (52.6) Hospital LOS (d) T = 39 ± 33 C = 58 ± 46 Pneumonia (%) T = 2/19 (10.5) C = 2/19(10.5) Ventilation (d) T = 19.5 ± 26.0 C = 10.1 ± 20.9 AKI (AKIN 1, 2, 3): T = 15/19; C = 13/18 RRT (%) T = 4/19 (21.0) C = 3/19 (15.8) 24-hr Crea (mg/dL): T = 1.85 ± 0.9 C = 1.67 ± 1.18 72-hr Crea (mg/dL): T = 1.27 ± 0.76 C = 1.32 ± 1.23 |
| Nakajima et al., 2019 [7] | Before PSM N = 2713 T = 157 C = 2556 Age (years), median (IQR) T = 67 (48–80) C = 69 (51–80) Male, n (%) T = 87 (55.4) C = 1561 (61.1) Inhalation injury, n (%) T = 45 (28.7) C = 523 (20.5) After PSM N = 785 T = 157 C = 628 Age(years), median (IQR) T = 67 (48–80) C = 67.5 (50–80) Male n(%) T = 87 (55.4) C = 332 (52.9) Inhalation injury n (%) T = 45 (28.7) C = 181 (28.8) | High dose vitamin C was administered under the following two varying thresholds: dosage more than (1) 10 g within 2 days of admission and (2) 24 g within 2 days of admission. High-dose vitamin C administered as a continuous intravenous infusion during the initial 24 h period after admission. | Standard of care. | In hospital mortality 10 g threshold of high dose Vitamin C T = 72/157 C = 364/628 24 g threshold of high dose Vitamin C T = 58/127 C = 278/508 |
| Nathens et al., 2002 [59] | N = 595 T = 301 C = 294 Age (mean± SD) T = 38± 15 C = 39 ± 15 Gender Male T = 230 (76) C = 222 (76) Illness severity ISS (mean ±SD) T = 19.1± 10 C = 20 ± 11 APACHE II (mean ±SD) T = 13.6± 6 C = 14.3± 6 | Alpha-tocopherol 1000 IU (20 mL) q8h per naso- or orogastric tube and 1000 mg ascorbic acid given intravenously in 100 mL of D5W q8h for the shorter duration of admission to the ICU or 28 days. | Standard of care. | Duration of ventilation (mean days) T = 3.7 C = 4.6 Ventilator-free days (mean) T = 24.1 C = 23.3 Multiple organ dysfunction score (mean) T = 2.4 C = 3.2 ICU length of stay, days (mean) T = 5.3 C = 6.4 Hospital length of stay (mean) T = 14.6 C = 15.1 Multiple organ failure T = 8/301 (2.7%) C = 18/294 (6.1%) Mortality 28-day T = 4/301 (1.3%) C = 7/294 (2.4%) ICU T = 3/301 (1.0%) C = 9/294 (3.1%) Hospital T = 5/301 (1.7%) C = 9/294 (3.1%) |
| Palli et al., 2017 [60] | N = 124 [T = 60 C = 64] Age (yrs) T= 51.34 (2.71) C = 50.51 (2.65) Male n (%) T = 46 (76.66) C = 55 (85.93) APACHE II score T = 14.44 (1.01) C = 13.29 (0.78) SOFA score T = 5.94 (0.5) C = 6.14 (0.41)Ventilator T= 32/60 (53.33) C = 44/64 (68.75) Vasoactive therapy, n (%) T = 20/60 (33.33) C = 25/64 (39.06) | Intravenously receive NAC (1200 mg) and ascorbic acid (2 g) dissolved separately in 100 mL of normal saline (N/S) 0.9%, 2 h before and at 10 h and 18 h following the infusion of contrast agent. | 200 mL of intravenous N/S 0.9%. | ICU LOS (days, median) T = 32.5 (5.11) C = 27.5 (4.49) ICU mortality, n (%) T = 15/60 (25) C = 11/64 (17.18) RRT 10 days post contrast agent, n (%) T = 3/60 (5) C = 4/64 (6.25) |
| Park et al., 2020 [34] | Before Matching N = 435(T = 94, C = 341) Male [T = 55 (58.5), C = 229 (67.1)] Age: T = 69 (60–76), C = 69 (61–76) CKD T = 7/94 (7.5) C = 23/341 (10.3) Creatinine (mg/dL) T = 2.1 ± 1.5 C = 1.8 ± 1.6 APACHE II score T = 30.2 ± 8.1 C = 28.4 ± 9.2 SOFA score T = 11.5 ±3.4 C = 10.1 ± 3.7 Mechanical ventilation, T = 53 (56.4) C = 173 (50.7) After Matching N = 178(T = 89, C = 89) Male: [T = 52 (58.4) C = 55 (61.8)] Age: T = 69 (61–76), C = 71 (62–78) CKD T = 7/89 (7.8) C = 9/89 (10.1) Creatinine (mg/dL) T = 1.9 ± 1.4 C = 2.2 ± 2.3 APACHE II score T = 30.0 ± 7.9 C = 30.0 ± 8.9 SOFA score T = 11.4 ± 3.5 C = 11.5 ± 3.4 Mechanical ventilation, T = 49 (55.1) C = 48 (53.9) | Vitamin C (3 g/12 h or 1.5 g/6 h) and thiamine (200 mg/12 h) mixed in 50- or 100-milliliter solution bags of 5% dextrose in water or normal saline were administered intravenously within 6 h of shock recognition. | Protocol-driven therapies based on the updated Surviving Sepsis Campaign guidelines were provided for all included patients. | Before Matching Delirium free days T= 11 C = 13 Delirium coma free days T = 13 C = 11 Incidence of delirium = 62/94 C = 194/341 Duration of delirium, days T= 2 C = 1 Hospital stay, days T = 16 C = 13 ICU stay, days T = 4 C= 4 28-day mortality T = 23/94 C = 72/341 Among matched cohort Delirium free days T = 11 C = 12 Delirium coma free days T = 11 C= 12 Incidence of delirium T = 57/89 C = 54/89 Hospital stay days median (IQRs) T = 16 (8–27); C= 13 (7–28) ICU stay days T= 4 (3–7); C= 4 (3–7) 28-day mortality T= 21/89; C= 16/89 |
| Reddy et al., 2020 [61] | N = 19 [T1 = 7 T2 = 5 C = 7] Age mean (SD) T1 = 56.5 (12) T2 = 53.8 (11) C = 55.4 (12.3) Male T1= 3 (15.7) T2 = 4 (21) C = 3 (15.7) APACHE score, mean (SD) T1= 17 (3.8) T2 = 18.4 (2.5) C = 21.2 (6.5) SOFA score, mean (SD) T1 = 11 (3.4) T2 = 9.2 (0.4) C = 8.8 (2.9) | T1 (hydrocortisone + vitamin C)- Hydrocortisone 200 mg over 24 h infusion and ascorbic acid in dose of 1.5 g IV every 6 h T2 (hydrocortisone + vitamin C + thiamine)- Hydrocortisone 200 mg over a 24-hour infusion, ascorbic acid in dose of 1.5 g IV every 6 h and thiamine dose of 200 mg IV every 12 h | Hydrocortisone was administered as 200 mg over a 24-hour infusion only. | Time to shock reversal (minutes), mean (SD) T1(7) = 2525 (3086); T2 (5) = 1860 (749); C(5) = 7422 (8348) Time to vasopressor reduction (minutes) from SOFA (h) 4–3 mean (SD) T1 (5) = 2310 (2515); T2 (5) = 1800 (1282); C (6) = 4935 (6406) |
| Sadaka et al., 2020 [35] | N = 62; T = 31, C = 31 Age, years (SD) T = 67 (16) C = 70 (12) Male, n (%) T = 16 (52) C = 16 (52) APACHE III score (SD) T = 95 (30) C = 96 (29) Mechanical ventilation, n (%) T = 27 (87) C = 27 (87) Creatinine (SD) T = 2.6 (2.4) C = 2.4 (1.9) | Intravenous (IV) ascorbic acid (1.5 g every 6 h for 4 days), hydrocortisone (50 mg every 6 h for 7 days) and thiamine (200 mg every 12 h for 4 days). | Patients were managed as per sepsis management guidelines. | ICU mortality, n (%) T = 3/31 (9.6) C = 13/31 (42.0) Hospital mortality, n (%) T = 9/31 (29) C = 14/31 (45) ICU LOS, days, median (IQR) T = 6.4 (1.2–9.6) C = 4.0 (2.5–9.2) LOHS, days, median (IQR) T = 15.0 (10.0–22.0) C = 9.3 (3.7–19.5) RRT for AKI, n (%) T = 8/31 (26) C = 9/31 (29) Duration of Vasopressors, days, media (IQR) T = 4.5 (4.0–6.0) C = 2.0 (1.0–3.0) Ventilation-free days, median (IQR) T = 10.2 (5.0–15.0) C = 10.2 (1.6–18.0) |
| Sadeghpour et al., 2015 [62] | N = 290; T = 113, C = 177 Age, y T = 57.28 ± 14.09 C = 54.22 ± 14.39 Male T = 80 (70.8) C = 111 (62.7) Intubation time, h T = 11.83 ± 3.91 C = 14.14 ± 9.52 | A total of 2 g of vitamin C intravenously, immediately before surgery in the operating theatre, followed by 1 g daily oral doses of the tablets for the first four postoperative days. | Equal number of identical placebo tablets. | ICU Stay T = 3.42 ± 1.06 C = 3.43 ± 1.09 Hospital Stay T = 10.17 ± 4.63 C = 12 ± 4.51 Death, Impaired Renal Function and Infection T = 4/113 (3.54) C = 18/177 (10.2) |
| Sandesc et al., 2018 [36] | N = 67; T = 35 C = 32 Age (yrs), mean (SD) T = 45.62 (16.88) C = 42.67 (16.72) Gender (male), % (n) T = 74.28 (26) C = 75 (24) APACHE II, mean (SD) T = 11.74 (7.11) C = 12.09 (15.94) Lac (mmol/mL) T = 4.89 (1.99) C = 5.1 (2.5) | Antioxidant therapy included continuous intravenous sodium ascorbate 3000 mg/24 h and N-acetylcysteine 1200 mg/24 h. | Antioxidant Therapy. | Sepsis, n (%) T = 13/35 (37.14) C = 28/32 (88.75) MODS, n (%) T = 8/35 (22.85) C = 21/32 (65.62) Mechanical ventilation > 96 h, n (%) T = 19/35 (54.28) C = 17/32 (53.21) ICU LOS, mean (SD) T = 14.4 (16.02) C = 18.25 (32.55) LOHS days, T = 26.03 (20.47) C = 38.68 (40.17) Mortality, n (%) T = 5/35 (14.28) C = 11/32 (33.6) |
| Shin et al., 2019 [37] | N:1144 T:229 C:915 Age N:67 (58–75) T:67 (58–76) C:67 (60–75) Male N:713 (62.3) T:136 (59.4) C:577 (63.1) CKD N:78 (6.8) T:15 (6.6) C:63 (6.9) Vasopressor use N:966 (84.4) T:217 (94.8) C:749 (81.9) Mechanical ventilation N:328 (17.9) T:67 (39.3) C:261 (28.5) SOFA in 24 h N:8 (5–11) T:9 (6–12) C:8 (5–11) APACHE II N:20 (15–27) T:27 (21–52) C:27 (20–56) | Within 6 h of shock recognition, vitamin C and thiamine were mixed in 50- or 100-milliliter solution bags of 5% dextrose in water or normal saline and intravenously administered for 1 day (vitamin C, 3 g/12 h or 1.5 g/6 h; thiamine, 200 mg/12 h). | All patients with septic shock were treated with protocol-driven resuscitation bundle therapy based on the Surviving Sepsis Campaign guidelines. | Overall Cohort 28-day mortality: T: 42/229 (18.3); C:160/915 (17.5) In-hospital mortality: T:38/229 (16.6); C:167/915 (18.3) ICU stay (days) T:4 (3–8); C:4 (3–8) Hospital stay (days); T:14 (9–22); C:13 (8–23) Ventilation T:6.0(3.0–15.0); C:6.0(3.0–12.0) New use of RRT T:28 (12.3); C:106 (11.9) Propensity-Matched Cohort (T:227, C:527 28-day mortality T:42/227 (18.5); C:92/527 (17.5) In-hospital mortality: T:38/227 (16.7); C:97/527 (18.4) ICU stay (days) T:4 (3–8); C:4 (3–7) Hospital stay (days) T:14 (9–22); C:13 (8–23) Ventilation T:5.5 (3.0–15.0); C:5.0 (3.0–10.0) New use of RRT T = 28/227 (12.4) C = 66/527 (12.9) |
| Siriwardena et al., 2007 [63] | N = 43 T = 22 C = 21 Age (SD) T = 64 (13) C = 71 (14) Sex (% male) T = 8(36%) C = 7(33%) APACHE admission (SD) T = 10.5 (3.4) C = 11.0 (3.5) MODS at admission (IQR) T = 1.36(0–2) C = 1.19 (0–2) | Selenium in 50 mL of normal saline, ascorbic acid in 100 mL of normal saline and n-Acetylcysteine as per protocol. | Maximal conventional therapy plus intravenous placebo for 7 days. | Organ dysfunction (day 7) Organ dysfunction (%) T = 7/22 (32) C = 4/21 (19) APACHE (SD) T = 5.73 (3.28) C = 5.33 (1.06) Renal dysfunction (%) T = 11/22 (50) C = 7/21 (33) LOHS (days)T = 20.4 (24.4) C = 14.3 (15.7) Days in ICU T = 4.0 (10.3) C = 0.0 (0.0) All-cause mortality T = 4/22 (18.2%) C = 0/21 (0.0%) |
| Vail et al., 2020 [38] | N = 338,597, T = 3574; C = 335,023 Female, N (%) T = 1671 (46.8) C = 163,190 (48.7) Age, mean ±SD, years T = 64.6 ± 14.8 C = 66.1 ± 14.7 RRT at admission, N (%) T = 999 (28.0) C = 52,015 (15.5) | At least one charge for high-dose IV ascorbic acid (one or more vials totaling ≥500 mg in one calendar day) and at least one charge for both IV hydrocortisone and IV thiamine (of any dose) on or within one day of ascorbic acid administration | Routine treatment of septic shock without hydrocortisone, ascorbic acid or thiamine. | LOHS, median (IQR), days Survivors T = 12 (7, 20) C = 10 (6, 17) Non survivors T = 5 (2, 12) C = 5 (2, 12) ICU stay: Survivors T = 6 (3, 11) C = 4 (2, 8) Non survivors T = 4 (2, 9) C = 3 (1, 8) IMV T = 2625/3574 (73.4) C = 201,229/335,023 (60.1) NIMV T = 1175/3574 (32.9) C = 104,970/335,023 (31.3) Vasopressor use, Survivors T = 2 (1, 4) C = 2 (1, 3) Non-survivors T = 3 (2, 6) C = 2 (1, 4) Hospital mortality T = 1459/3574 (40.8) C = 92,060/335,023 (27.5) |
| Wang et al., 2020 [64] | N = 70 T = 33 C = 37 Age (years) T = 59.15 ± 8.11 C = 55.00 ± 9.92 M/F T = 13 (39.39)/20 (60.61) C = 14 (37.84)/23 (62.16) | Intravenous vitamin C 1 g (diluted to 10 mL) with a total of 3 g, 10 min after induction of anesthesia, 10 min before cardiac reanimation and at the moment of sternal closure. | Intravenous 10 mL saline. | ICU stay (h) T = 39.5 (20.8–44.3) C = 39.5 (20.5–44.5) LOHS (days) T = 14 (10–15) C = 12 (11–17) Atrial fibrillation T = 10/33 (30.30) C = 10/37 (27.03) Extubation time (min) T = 660 (401–920) C = 660 (358–862) Pulmonary complication T = 4 (12.12) C = 12 (32.43) |
| Wani et al., 2020 [48] | N = 100 T = 50 C = 50 Age (Median, IQR) T = 65 (59, 25–72) C = 70 (56, 25–72) Male: n (%) T = 28 (56%) C = 31 (62%) APACHE II Median (IQR) T = 18.5 (15–24.75) C = 20 (15–24) SOFA Mean ± SD (Range) T = 9.22 ± 3.54 (4–16) C = 9.36 ± 3.66 (2–16) Renal disease n (%) T = 6 (12.0%) C = 4 (8.0%) Acute kidney injury n (%) T = 37 (74%) C = 39 (78%) | Intravenous vitamin C (1.5 g q 6 hourly for 4 days or until discharge from the hospital), hydrocortisone (50 mg q 6 hourly for 7 days or until ICU discharge followed by a taper over 3 days) and intravenous thiamine (200 mg q 12 hourly for 4 days or until discharge from the hospital). | Standard of care, consisted of broad-spectrum antibiotics, intravenous fluids, vasopressors and mechanical ventilation as indicated. | Hospital mortality N (%) T = 12/50 (24%) C = 14/50 (28%) Ventilation N (%) T = 3/50 (6%) C = 3/50 (6%) Duration of vasopressor use (Mean ± SD, hours) Range T = 75.72 ± 30.29 (20–140) C = 96.13 ± 40.50 (30–200) LOHS (Mean ± SD, days) (Range) T = 11.82 ± 7.36 (4–36) C = 10.70 ± 6.39 (2–27) 30 day mortality N (%) T = 20/50 (40%) C = 21/50 (42%) SOFA score Day 4 T = 5.64 ± 3.55 C = 6.62 ± 3.94 |
| Yanase et al., 2020 [65] | N = 50 T = 25 C = 25 Age, years, (IQR) T = 67.0 (82.0, 74.0) C = 64.0 (59.0, 69.0) Sex, male T = 15/25 (60.0%) C = 23/25 (92.0%) Serum creatinine (μmol/L): T = 85.0 (75.0, 98.0) C = 92.0 (80.0, 100.0) | Vitamin C 1500 mg in normal saline (100-milliliter bag) administered 6 hourly in the vitamin C group. | Normal saline (100-milliliter bag) administered 6 hourly in the placebo group. | ICU LOS, days T = 1.4 (0.5, 2.5) C = 1.5 (0.5, 3.3) LOHS, days T = 13.2 (7.9, 20.2) C = 12.5 (8.1, 16.7) ICU mortality T = 1/25 (4.0%) C = 0/25 (0.0%) Hospital mortality T = 1/25 (4.0%) C = 0/25 (0.0%) AKI (1, 2, 3): T = 14/25; C = 12/25 Stage 1 T = 3/25 (12.0%) C = 1/25 (4.0%) Stage 2 T = 10/25 (40.0%) C = 9/25 (36.0%) Stage 3 T = 1/25 (4.0%) C = 2/25 (8.0%) Atrial fibrillation T = 11/25(44.0%) C = 8/25(32.0%) |
| Yoo et al., 2020 [39] | N = 79 T = 33 C = 46 Age, yr T = 66 (55.5–81) C = 73.5 (63–79) Male sex T = 20 (60.6) C = 34 (73.9 CKD T = 4 (12.1) C = 3 (6.5) APACHE II T = 26 (20.5–32.5) C = 30 (24–33.3) SOFA T = 13 (11–15) C = 12 (10–14.3) AKI T = 18 (54.5) C = 29 (63) RRT T = 7 (21.2) C = 13 (28.3) | The total supplementation of vitamin B1 was 200 mg/day intravenously infused 50 mg every 6 h. A total of 2 g of vitamin C intravenously infused 500 mg every 6 h. | No vitamin B and C supplementation, only standard of care. | 14-Day mortality T = 15/33 (45.5) C = 22/46 (47.8) 30-Day mortality T = 18/33 (54.5) C = 32/46 (69.6) ICU mortality T = 18/33 (54.5) C = 32/46 (69.6) In hospital mortality T = 19/33 (59.4) C = 33/36 (71.7) Ventilator free days T = 7.7 ± 10.8 C = 2.7 ± 7.3 ICU-free days T = 6.9 ± 9.8 C = 2.2 ± 6.5 |
| Zabet et al., 2016 [6] | N = 28 T = 14 C = 14 Age years, SD T = 64.14 ± 15.98 C = 63.71 ± 13.84 Sex (male) T = 10 (71.42) C = 11 (78.57) APACHE II score T = 19.07 ± 5.18 C = 23 ± 5.61 SOFA score T = 11.78 ± 2.22 C = 12.35 ± 3.00 | 25 mg/kg intravenous ascorbic acid every 6 h for 72 h. | 50 mL of dextrose 5% solution as intravenous infusion over 30 min. | ICU LOS (days) T = 21.45 ± 10.23 C = 20.57 ± 13.04 28-day mortality T = 2/14 (14.28) C = 9/14 (64.28) Duration of norepinephrine administration (h) T = 49.64 ± 25.67 C = 71.57 ± 1.60 |
| Ferron Celma et al., 2009 [47] | N = 20 T = 10 C = 10 Age (y) T = 67.8 ± 4.5 C = 65.1 ± 3.6 POSSUM Score T = 55.0 ± 3.3 C = 50.4 ± 1.4 Sex (Men/Women) T = 5/5 C = 6/4 Pressors T = 3/10 C = 2/10 Ventilatory support T = 3/10 C = 2/10 Creatinine (mg/dL) T = 2.15 ± 0.12 C = 1.99 ± 0.21 Lactate (meq/L) T = 3.22 ± 1.25 C = 1.97 ± 0.55 | 450 mg/day of the vitamin C administered in 5% dextrose water in 3 divided doses. | Identical administration of 5% dextrose. | Mortality T = 6/10 C = 4/10 |
| Habib et al., 2017 [66] | N = 100 T = 50 C = 50 Male T = 28 (56) C = 30 (60) Age Mean ± SD. T = 42.78 ± 9.49 C = 41.70 ± 10.2 APACHE II T = 22.0 ± 6.70 C = 21.8 ± 7.07 SOFA Mean ± SD. T = 10.2 ± 3.42 C = 11.4 ± 5.08 BUN mg/dL T = 100.23 ± 11.31 C = 100.40 ± 17.30 S. Cr mg/dL T = 3.22 ± 2.21 C = 5.83 ± 0.16 | Intravenous 1.5 gm vitamin C (ascorbic acid, Cevarol) every 6 h in the first 24 h after admission until ICU discharge plus conventional sepsis treatment. | Conventional sepsis treatment only. | Vasopressor Mean ± SD. T = 2.30 ± 1.2 C = 6.50 ± 2.57 Ventilator Mean ± SD. T = 4.60 ± 2.08 C = 7.87 ± 3.01 ICU LOS Mean ± SD. T = 10.00 ± 5.50 C = 14.10 ± 6.47 RRT T = 15/50 (30%) C = 13/50 (26%) Survivors T = 38/50 (76%) C = 32/50 (64%) Non-survivors T = 12/50 (24%) C = 18/50 (36%) |
| Tanaka et al., 2000 [67] | N = 37 T = 19 C = 18 Age, mean ±SD, y T = 40 ± 20 C = 49 ± 22 Male T = 13 C = 12 Inhalational injuries T = 15/19 C = 12/18 | An injectable ascorbic acid solution was diluted 10-fold with distilled water. The ascorbic acid solution was administered as a continuous intravenous infusion. | Fluid resuscitation without ascorbic acid. | LOHS, mean ± SD, d T = 40 ± 28 C= 49 ± 44 Ventilation, mean ± SD, d T = 12.1 ± 8.8 C = 21.3 ± 15.6 Mortality, no of patients T = 9/19 C = 7/18 |
| Galley et al., 1997 [68] | N = 30 T = 16 C = 14 Age median (range) T = 67 (21–78) C = 70 (22–89) Male: Female T = 13:3 C = 9:5 APACHE II median (range) T = 27.5 (17–54) C = 24 (11–35) | Intravenous antioxidant therapy comprising n-acetylcysteine 150 mg/kg for 30 min then 20 mg/kg/h plus bolus doses of 1 g ascorbic acid (vitamin C) and 400 mg alpha-tocopherol (vitamin E). | Comparable volume of 5% dextrose as placebo. | Mortality, n T = 11/16 C = 8/14 |
| Razmkon et al., 2011 [69] | N = 76 T1 = 26 T2 = 23 C = 27 Age (y; mean, range) T1 = 31.1 (16–67) T2 = 29.5 (19–75) C = 29.4 (16–68) Sex (male/female) T1 = 20/6 T2 = 20/3 C = 23/4 Admission GCSs (mean, range) T1 = 5.9 (3–8) T2 = 6.1 (3–8) C = 6.5 (3–8) | T1 group, low-dose vitamin C (500 mg/d IV) for 7 days; T2 group, high-dose vitamin C (10 g IV on the first (admission) day and repeated on the fourth day, followed by vitamin C 4 g/d IV for the remaining 3 days | Identical placebo. | Hospital mortality T1 = 7/26 T2 = 7/23 C = 8/27 Mortality after 2 months T1 = 8/26 T2 = 7/23 C = 8/27 Mortality after 6 months T1 = 9/26 T2 = 7/23 C = 8/27 |
| Bansal et al., 2011 [70] | N = 39 [T = 19, C = 20] Age (years) Mean ±SD T = 39.9 (10.9) C = 38.6 (11.4) Males (%) T = 15 (79) C = 15 (75) APACHE score (SD) T = 11.2(2.9) C = 11.5 (2.7) | vitamin C (1000 mg in 100 mL of normal saline), vitamin E (200 mg oral) and vitamin A (10,000 IU intramuscularly). | The control group was given the standard treatment only. | Organ dysfunction(day 7) T = 7 /19 (37) C = 8/20 (40) LOHS (days) Mean (SD) T = 12.8 (3.9) C = 15.1 (5.43) Renal insufficiency T = 4/19 C = 4/20 Mortality T = 0/19 C= 2/20 |
| Sevransky et al., 2021 [46] | N = 501(T = 252, C = 249) Median age, 62 [IQR, 50–70] years Female: 46% | Intravenous vitamin C (1.5 g), thiamine (100 mg) and hydrocortisone (50 mg) every 6 h. | Matching placebo. | Mortality in 30-day: T:56 /252; C: 60/249 Mortality 180-day: T:102 /252; C: 94/249 ICU mortality: T:52 /252; C: 49/249 ICU stay, median (IQR), day; T:4 (2–8) [n = 250] C:4 (2–8) [n = 245] Hospital stay, median (IQR), day; T: 10 (6–17) [n = 250]; C: 9 (5–17) [n = 246] Ventilator- and vasopressor-free days {median(IQR)}: T: 25 (0–29) days; C: 26 (0–28) days |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shrestha, D.B.; Budhathoki, P.; Sedhai, Y.R.; Mandal, S.K.; Shikhrakar, S.; Karki, S.; Baniya, R.K.; Kashiouris, M.G.; Qiao, X.; Fowler, A.A. Vitamin C in Critically Ill Patients: An Updated Systematic Review and Meta-Analysis. Nutrients 2021, 13, 3564. https://doi.org/10.3390/nu13103564
Shrestha DB, Budhathoki P, Sedhai YR, Mandal SK, Shikhrakar S, Karki S, Baniya RK, Kashiouris MG, Qiao X, Fowler AA. Vitamin C in Critically Ill Patients: An Updated Systematic Review and Meta-Analysis. Nutrients. 2021; 13(10):3564. https://doi.org/10.3390/nu13103564
Chicago/Turabian StyleShrestha, Dhan Bahadur, Pravash Budhathoki, Yub Raj Sedhai, Sujit Kumar Mandal, Shreeja Shikhrakar, Saurab Karki, Ram Kaji Baniya, Markos G. Kashiouris, Xian Qiao, and Alpha A. Fowler. 2021. "Vitamin C in Critically Ill Patients: An Updated Systematic Review and Meta-Analysis" Nutrients 13, no. 10: 3564. https://doi.org/10.3390/nu13103564
APA StyleShrestha, D. B., Budhathoki, P., Sedhai, Y. R., Mandal, S. K., Shikhrakar, S., Karki, S., Baniya, R. K., Kashiouris, M. G., Qiao, X., & Fowler, A. A. (2021). Vitamin C in Critically Ill Patients: An Updated Systematic Review and Meta-Analysis. Nutrients, 13(10), 3564. https://doi.org/10.3390/nu13103564