
Qualitative Accounts of School-Aged Children’s Diets during the COVID-19 Pandemic in Rural, Central, Kenya

 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.2.1. Qualitative Statements
2.2.2. Demographics
2.2.3. Dietary Recall Data
2.2.4. Anthropometrics
2.3. Analysis
3. Results
3.1. Quantitative Analyses
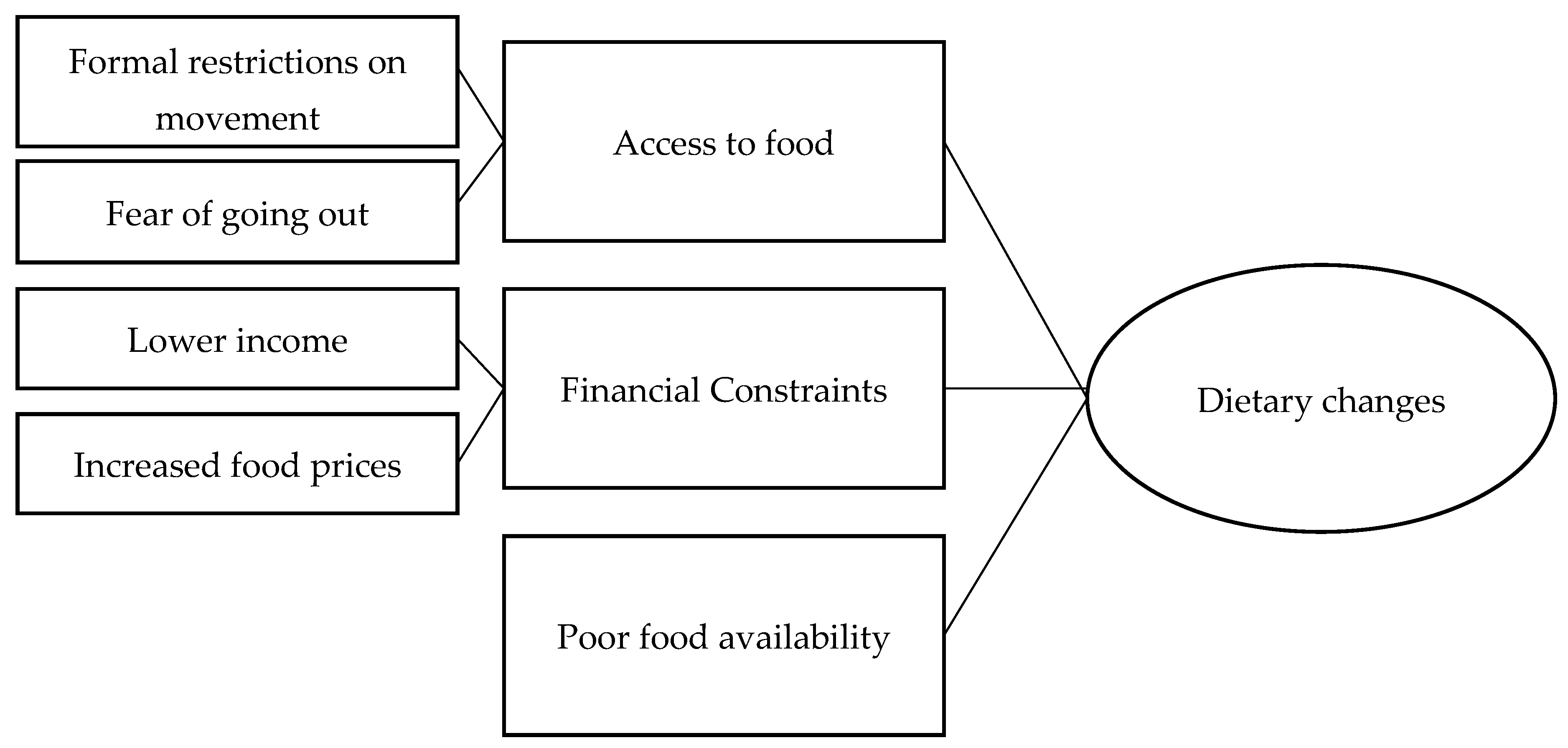
3.2. Qualitative Analyses
3.2.1. Barriers to Access
“Yes, we were unable to get some ingredients because of the fear to get to the market due to covid-19”(Participant 7)
“We would have wished to have maybe fruits in their meal but it has become hard to get to the market due to the fear of being infected”(Participant 8)
“We used to buy fruits for the child but this has become hard since movements to the market have been minimized”(Participant 16)
3.2.2. Financial Changes
“In times like this when we receive a visitor, we could add some meat to the stew but it has become hard to get some wage and casual works due to the effect of the virus”(Participant 15)
“Yes, the amount of milk used to prepare the tea has reduced since the virus broke. This is because we cannot afford to buy more because jobs have become scarce and we rely on wage work”(Participant 6)
“When cooking meat stew we usually include tomatoes but we did not because they have turned to be expensive”(Participant 9)
3.2.3. Limited Availability
“Yes, we were not able to add tomatoes to the food as the pandemic has made it hard for the vendors to transport them together with other commodities… because of various restrictions”(Participant 6)
“We are forced to take whatever is available as the pandemic has changed life”(Participant 2)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shinsugi, C.; Matsumura, M.; Karama, M.; Tanaka, J.; Changoma, M.; Kaneko, S. Factors associated with stunting among children according to the level of food insecurity in the household: A cross-sectional study in a rural community of Southeastern Kenya. BMC Public Health 2015, 15, 441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagata, J.M.; Fiorella, K.J.; Salmen, C.R.; Hickey, M.D.; Mattah, B.; Magerenge, R.; Milner, E.M.; Weiser, S.D.; Bukusi, E.A.; Cohen, C.R. Around the Table: Food Insecurity, Socioeconomic Status, and Instrumental Social Support among Women Living in a Rural Kenyan Island Community. Ecol. Food Nutrition. 2015, 54, 358–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kansiime, M.K.; Tambo, J.A.; Mugambi, I.; Bundi, M.; Kara, A.; Owuor, C. COVID-19 implications on household income and food security in Kenya and Uganda: Findings from a rapid assessment. World Dev. 2021, 137, 105199. [Google Scholar] [CrossRef] [PubMed]
- Demeke, M.; Kariuki, J.; Wanjiru, M. Assessing the Impact of COVID-19 on Food and Nutrition Security and Adequacy of Responses in Kenya. FAO Policy Briefing May 2020. Available online: https://evidencefrontiers.com/wp-content/uploads/2020/05/Policy-Brief_Assessing-the-Impact-of-COVID_19-on-Food-and-Nutrition-Security-1.pdf (accessed on 6 August 2021).
- QSR International Pty Ltd. NVivo (Version 12). 2018. Available online: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home (accessed on 1 June 2021).
- Aglago, E.K.; Landais, E.; Nicolas, G.; Margetts, B.; Leclercq, C.; Allemand, P.; Aderibigbe, O.; Agueh, V.D.; Amuna, P.; Annor, G.A.; et al. Evaluation of the international standardized 24-h dietary recall methodology (GloboDiet) for potential application in research and surveillance within African settings. Glob. Health 2017, 13, 35. [Google Scholar] [CrossRef] [PubMed]
- Kigutha, H.N. Assessment of dietary intake in rural communities in Africa: Experiences in Kenya. Am. J. Clin. Nutr. 1997, 65 (Suppl. 1), 1168S–1172S. [Google Scholar] [CrossRef] [PubMed]
- Gibson, R.S.; Charrondiere, U.R.; Bell, W. Measurement errors in dietary assessment using self-reported 24-hour recalls in low-income countries and strategies for their prevention. Adv. Nutr. 2017, 8, 980–991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- FAO/Government of Kenya. Kenya Food Composition Tables. Nairobi. 2018. 254. Available online: http://www.fao.org/3/I9120EN/i9120en.pdf (accessed on 1 August 2021).
- World Health Organisation. Food and Agriculture Organisation of the United Nations. In Vitamin and Mineral Requirements in Human Nutrition, 2nd ed.; WHO and FAO of the United Nations: Bankok, Thailand, 2004; pp. 17–299. [Google Scholar]
- United Nations University; World Health Organization. Food and Agriculture Organization of the United Nations. In Human Energy Requirements: Report of a Joint FAO/WHO/UNU Expert Consultation; FAO: Rome, Italy, 2004. [Google Scholar]
- World Health Organistion AnthroPlus Software. Version 1.0.4. 2007. Available online: https://www.who.int/tools/growth-reference-data-for-5to19-years/application-tools (accessed on 5 August 2021).
- Stata Statistical Software. Release version 14.0; StataCorp, College Station, Texas USA. 2015. Available online: https://www.stata.com/stata14/ (accessed on 10 July 2021).
- Ben Hassen, T.; El Bilali, H.; Allahyari, M.S. Impact of COVID-19 on Food Behavior and Consumption in Qatar. Sustainability 2020, 12, 6973. [Google Scholar] [CrossRef]
- Oni, T.; Micklesfield, L.K.; Wadende, P.; Obonyo, C.O.; Woodcock, J.; Mogo, E.R.; Odunitan-Wayas, F.A.; Assah, F.; Tatah, L.; Foley, L.; et al. Implications of COVID-19 control measures for diet and physical activity, and lessons for addressing other pandemics facing rapidly urbanising countries. Glob. Health Action 2020, 13, 1810415. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Nutrient | Median (Range) | N Inadequate Intake |
|---|---|---|
| Kcal | 1613.7 (868.1–2638.2) | 6 |
| Calcium (mg) | 506.7 (266.1–1090.4) | 10 |
| Iron (mg) | 11.2 (5.7–30.4) | 1 |
| Magnesium (mg) | 274.0 (128.8–420.6) | 0 |
| Zinc (mg) | 6.9 (4.2–9.9) | 2 |
| Selenium (mcg) | 24.9 (9.9–35.6) | 0 |
| Vitamin A Retinol Equivalents (mcg) | 246.1 (134.6–464.7) | 6 |
| Thiamin (mg) | 0.7 (0.3–2.3) | 5 |
| Riboflavin (mg) | 1.3 (0.6–2.1) | 2 |
| Niacin (mg) | 7.8 (4.3–17.9) | 9 |
| Folate (mcg) | 331.4 (171.2–573.7) | 3 |
| Vitamin B12 (mcg) | 2.1 (0.9–5.7) | 2 |
| Vitamin C (mg) | 55.1 (17.1–105.2) | 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jarman, M.; Zeidler, H.; Shapiro, L.; Clarke, R.; Mooya, H.; Simatende, B.; Matthews, D.; Koteng, G.; Wadende, P.; Farrow, C. Qualitative Accounts of School-Aged Children’s Diets during the COVID-19 Pandemic in Rural, Central, Kenya. Nutrients 2021, 13, 3543. https://doi.org/10.3390/nu13103543
Jarman M, Zeidler H, Shapiro L, Clarke R, Mooya H, Simatende B, Matthews D, Koteng G, Wadende P, Farrow C. Qualitative Accounts of School-Aged Children’s Diets during the COVID-19 Pandemic in Rural, Central, Kenya. Nutrients. 2021; 13(10):3543. https://doi.org/10.3390/nu13103543
Chicago/Turabian StyleJarman, Megan, Henriette Zeidler, Laura Shapiro, Rebecca Clarke, Haatembo Mooya, Barnabas Simatende, Danielle Matthews, Grace Koteng, Pamela Wadende, and Claire Farrow. 2021. "Qualitative Accounts of School-Aged Children’s Diets during the COVID-19 Pandemic in Rural, Central, Kenya" Nutrients 13, no. 10: 3543. https://doi.org/10.3390/nu13103543
APA StyleJarman, M., Zeidler, H., Shapiro, L., Clarke, R., Mooya, H., Simatende, B., Matthews, D., Koteng, G., Wadende, P., & Farrow, C. (2021). Qualitative Accounts of School-Aged Children’s Diets during the COVID-19 Pandemic in Rural, Central, Kenya. Nutrients, 13(10), 3543. https://doi.org/10.3390/nu13103543