1. Introduction
Home parenteral nutrition (HPN) is a life-sustaining therapy for patients with intestinal failure (IF) who require parenteral nutrition outside of the hospital. IF according to the European Society for Clinical Nutrition and Metabolism (ESPEN) is defined as “the reduction of gut function below the minimum necessary for the absorption of macronutrients and/or water and electrolytes, such that intravenous supplementation (IVS) is required to maintain health and/or growth” [
1,
2].
Advancements in medical care and improvements in life status contribute to prolonging life expectancy in developed countries. Life expectancy at the age of 65 rose for women and men by 9 months and 1.5 years per decade in the Swedish population from 1998 to 2017. The trends were observed also in subpopulations of polymorbid patients with myocardial infarction, ischemic stroke, hemorrhagic stroke or cancer (colon, lung, breast). The gap between the survival of a healthy population and patients with civilizational diseases is also decreasing gradually [
3]. Polish demographic statistics confirm those trends showing an increase in 3.4 years of life expectancy of 60-year-old citizens from 1960–2019. Improved treatment of cardiovascular diseases, lower tabacco and alcohol consumption, diet, physical activities, health promotion programs and legislation changes are considered as important contributing factors [
4,
5]. We observe more patients in advanced age with polymorbidity and longer survival. Therefore, population of HPN patients may continue to grow and we can expect more challenging and polymorbid patients in advanced age. Advanced age and a growing number of cancer patients in HPN contribute to the demands of financial resources in the health care system required to cover all medical needs. It is exceedingly difficult to compare data on real costs of treatment between different countries due to various systems of refoundation and organization of the health care system. Patients on HPN often require surgical procedures, advanced medical treatment of complications and cost-consuming oncological treatment.
The country’s income is associated with the reimbursement for EN and PN in the hospital and in chronic or home settings [
6]. Other observations show that reimbursement of PN increased the use of PN in hospital but the evident influence on home nutrition was not confirmed [
7]. A recent systematic review on costs of HPN showed that it is very problematic to compare the data between countries due to different methodologies and high heterogeneity of the studies. Most studies included only direct costs and were designed from a health care perspective [
8]. Direct healthcare costs (ex. HPN bags, catheters, monitoring, managing of complications) and direct non-healthcare costs (like transportation of HPN bags or consumables) account for the majority of costs in HPN [
9].
Organizing HPN teams and planning the organization of HPN requires epidemiological data on this population. Only a few countries around the world gather organized information and provide studies based on registries. Long-term observations and trend analysis of HPN populations give a possibility to estimate future perspectives on epidemiology. Since 1998, HPN has been reimbursed in Poland only by the national health fund (NHF), which gives a unique possibility of data analysis of all patients requiring this procedure. We analyzed the data from NHF in a long-term perspective concerning main prevalence data, indications for the procedure, hospitalizations and the national costs of the reimbursement of HPN.
4. Discussion
Long-term observations of the HPN population give a wide perspective on the evolution and possible future development of the outpatient treatment of IF. The prevalence of adult HPN in Poland grew from 17.65 patients per 1 min. of citizens in 2010 to 53.26 in 2020. A nearly 3-fold increase in a total number of HPN patients was confirmed in the trend analysis. 2020 was an exceptional year with a decrease in the total number of HPN patients. A projected number from the trend analysis was 2082 and real data showed 2038 HPN patients. We assume that this could be a consequence of the Covid-19 pandemic, however continuous observations in the following years are needed to confirm this.
There are only a few studies on HPN prevalence with trending analysis. However, the growing prevalence in other countries can be estimated from the point prevalence data presented in several studies. The first European multicenter report of the ESPEN Home Artificial Nutrition (HAN) group published in 1996 showed the prevalence of 4.6 to 12.2 patients per million citizens in Europe and 0.36 in Poland [
13]. An Italian study from 2005 showed 31.7 HPN patients per million citizens [
14] and data from Campalila region confirmed a 96% increase in patients on HPN (156 on HPN in April 2005 and 306 in 2012) [
15]. US analysis for 2013 showed 79 HPN patients per million citizens [
16]. Data updated from national registries come from Spain and UK. NADYA-SENPE group published reports from the Spanish HAN registry from 2013, 2016 and 2018 with a prevalence of 4.22, 6.16 and 6.61 per million citizens [
17,
18,
19]. In the UK, prevalence of HPN together with home intravenous fluids (HIVF) in 2015 was 40 per million citizens. A more than 2-fold increase in period prevalence was observed from 2005 to 2015 [
20].
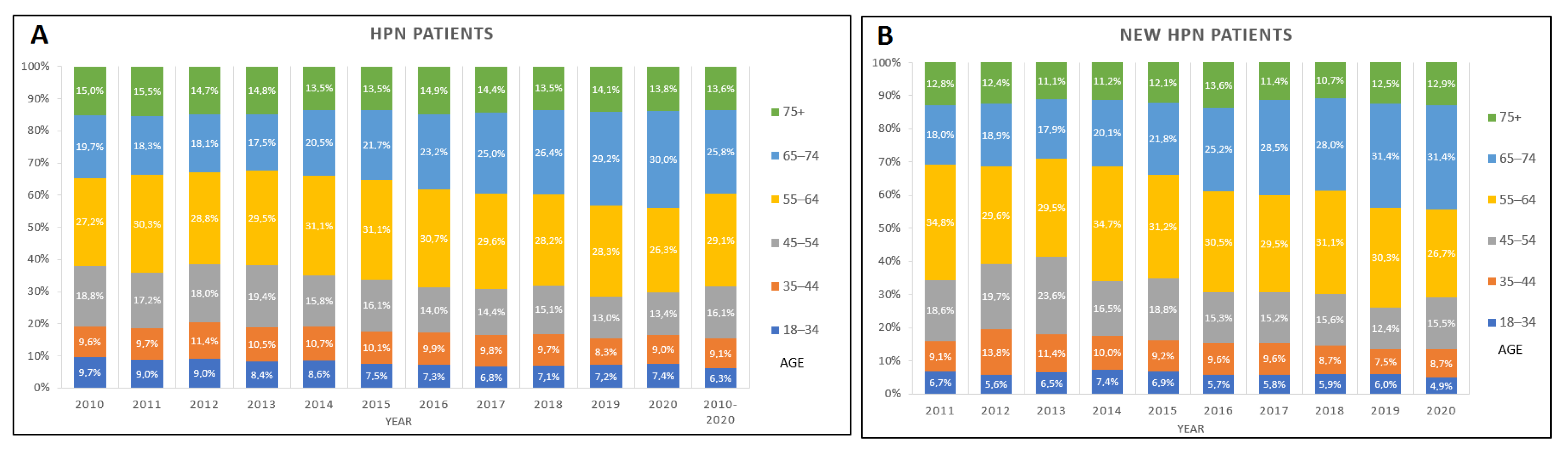
We additionally described the trends in the age distribution showing that the propotion of younger patients qualified for HPN are decreasing. Those trends are noticeable in the age range between 18–54 years old. On the other hand, the percentage of patients over 65 has increased. Similar tendencies are shown among new qualifications with increasing trends in the 65–74 age group and a decrease in young patients 35–54. This confirms the hypothesis of the aging HPN population. Data from the British Artificial Nutrition Survey (BANS) report showed that the majority of HPN patients were under 71 years old (81.5%) and two-thirds were between 41 and 70. However, in the observation period between 2005 and 2015, the age distribution didn’t change significantly in the UK [
20]. In the previously mentioned study of the ESPEN HAN group 28% of patients in Europe were older than 61 years when they started HPN and 10%—were more than 70 years old [
13]. The effect of the changing age distribution on the outcomes of HPN patients’ needs to be analyzed in future studies. A retrospective study from Canada showed that older patients on HPN have higher 2-year mortality but a lower risk of catheter-related bloodstream infections [
21].
The duration of HPN in our study was calculated as the time between the first and last reported HPN in the base of NHF. This is a limitation of the analysis, and the rates of long-term nutrition may be underrepresented. Some patients might have been on HPN for a longer time exciding the observation period of the study. However, the duration of HPN was mostly shorter than one year (71.14%). We additionally showed an increase in the rates of short term (maximal of 5 months) HPN and the risk of death during the first year after qualification for HPN was 0.59 and increased significantly in the observation period (estimate 1.210, with 95%CI: 0.504: 1.881, p-trend < 0.030). We were not able to compare the survival between the primary diagnosis. However, growing numbers of new qualifications among oncological patients may explain the trends in the risk of death and short term HPN.
Malnutrition was reported most commonly in HPN patients (34% as primary and 47% as secondary diagnosis) following intestinal malabsorption or other intestinal diseases. Advanced cancer was diagnosed as a primary disease in 17.36% of cases and secondary disease 23.1%. More than a third of patients with mechanical bowel obstruction due to cancer were gastric cancer patients following ovarian and colon cancer in 17.8% and 12.3% respectively. Having the methodology of the study in mind, it is more difficult to estimate the rates of other diseases. For instance, reported ICD-10 of Inflammatory Bowel Disease (IBD) were only for 2.11% of HPN but we may assume that some of the patients with malabsorption, malnutrition or postprocedural disorders might be also Crohn or ulcerative colitis patients. Moreover, data on the indications for HPN were provided for the whole observation period with no specified information for each year, therefore, an evolution of indications was not possible to determine. Nevertheless, high rates of oncological patients are in line with other data from the literature. In the previously mentioned NADYA study, the most frequent diagnosis in adults was “palliative cancer” (25.6%) and the cancer diagnosis concerned 44% of patients: either after radical treatment or with post-radiation enteritis [
22]. This was confirmed in other data from Spain [
23] and Switzerland [
24] (49.5% and 57.4% cancer patients). BANS report showed that cancer was the main reason for IF in HPN for one in four new registrations, however, Crohn disease remained a leading diagnosis of 14% new and 21% of HPN patients in point prevalence analysis from 2015 [
20]. Data from the Canadian registry comparing two periods 2011–2014 and 2005–2008 also showed increased rates of cancer patients (37.9% vs. 16.7%) and a reduction in short bowel syndrome patients (32% vs. 65.5%). The median age of HPN patients increased from 52 to 57 in this study confirming our data on the trends in age distribution [
25].
The reimbursement of HPN in Poland started in 1998. It covers the costs of HPN provision, monitoring and the support of a specialized nutrition team. In our study, we analyzed the costs reported by the NHF. The average cost of HPN per patient (yearly) in the observational period was € 10,251.2. NHF reimbursement of HPN has not changed in the observation time and is between € 45–55 for a patient day (depending on the zloty/euro currency conversion rate for the following years). Total costs of health care per patient (in the HPN population) were € 16,743 in comparison with the average cost of health care from 2010–2020 in general polish population—€ 486.6. This included all costs of hospital stays and treatment procedures (like surgery or oncological treatment), ambulatory care and rehabilitation, drugs reimbursement, diagnostic procedures. Since we analyzed data from NHF, we were not able to calculate the costs covered by the patients (like traveling to the hospital, caregiver, job loss or the need to limit professional work). Interestingly, we found that the cost of HPN and total costs of health care per HPN patient decreased during the observation time. NHF provided data for the general population of HPN patients and the cost per patient was calculated using data on the total number of individual patients in the following years. Consequently, a significant decrease in the cost of HPN and total costs of health care per HPN patient in the observation period can be explained by a growing rate of short-term HPN described in
Table 7. Although there are studies showing the cost of HPN of € 8000 per patient per year [
26] most calculated from € 14,000 up to € 77,000 in Europe [
9,
27,
28,
29]. The costs in Spain were 13,363.53 per patient per year and € 124.02 per patient per day. From overall costs, the HPN provision accounted for the highest percentage (74.25%), followed by management of complications (21.85%) with the CRBSI rate of 2.03 per 1000 HPN days and, outpatient monitoring (2.23%). HPN bags were the most expensive element in the HPN provision [
26]. Other studies confirmed this thesis [
30,
31,
32]. UK study—£ 30,000–40,000 per patient per year for the self-cared patient and £ 55,000–65,000 per patient per year with nursing support [
33]. Data from the US show cost of
$ 64,000 per patient per year [
34]. High costs of total health care observed in the population of HPN patients in comparison with the general population may relate to comorbidity, advanced medical therapies (surgery, oncological procedures) and the treatment of the complications. Additional costs of health care of patients with central line-associated bloodstream infections, catheter-associated urinary tract Infections or surgical site Infections were estimated:
$48,108,
$13,793 and
$28,219 [
35]. Additional analysis of hospitalizations of HPN patients from our study confirms this thesis. For nearly 40% of patients the oncological disease was a primary or secondary cause of hospitalization. For more than 20% of patients the hospitalizations involved procedures of the oncological treatment (mostly chemotherapy). Infectious complications were reported in 11% as primary and 8.7% as a secondary diagnosis in hospitalized HPN patients.
Limitations of the Study
We are aware that data analysis from the NHF has some limitations. Firstly, the analysis of the indications for HPN and hospitalizations was based on ICD-10. This method may be more useful for oncological patients however it may not always reflect the epidemiology for benign patients. Malnutrition, intestinal malabsorption or postprocedural disorders may indicate many more specific indications like IBDs. Indications and hospitalization were not analyzed annually therefore we were not able to address the trends in those areas. Additionally, cost analysis based on the data from NHF reported annually. Data on costs per HPN patient or per polish citizen needed to be calculated based on the provided data of HPN population and general statistics of polish population.


 ,
, 

{kind=link}
{kind=link}