The Relationship of Diet Quality with Proportion of Daily Energy Contributed by Sandwiches Varies by Age over Adulthood in Racially and Socioeconomically Diverse Adults

 , ,
, ,
Abstract
1. Introduction
2. Methods
2.1. Sample
2.2. Dietary Collection Method
2.3. Food Coding
2.4. Eating Occasions
2.5. Source of Sandwiches/Ingredients
2.6. Healthy Eating Index 2010 (HEI-2010)
2.7. Statistical Analyses
3. Results
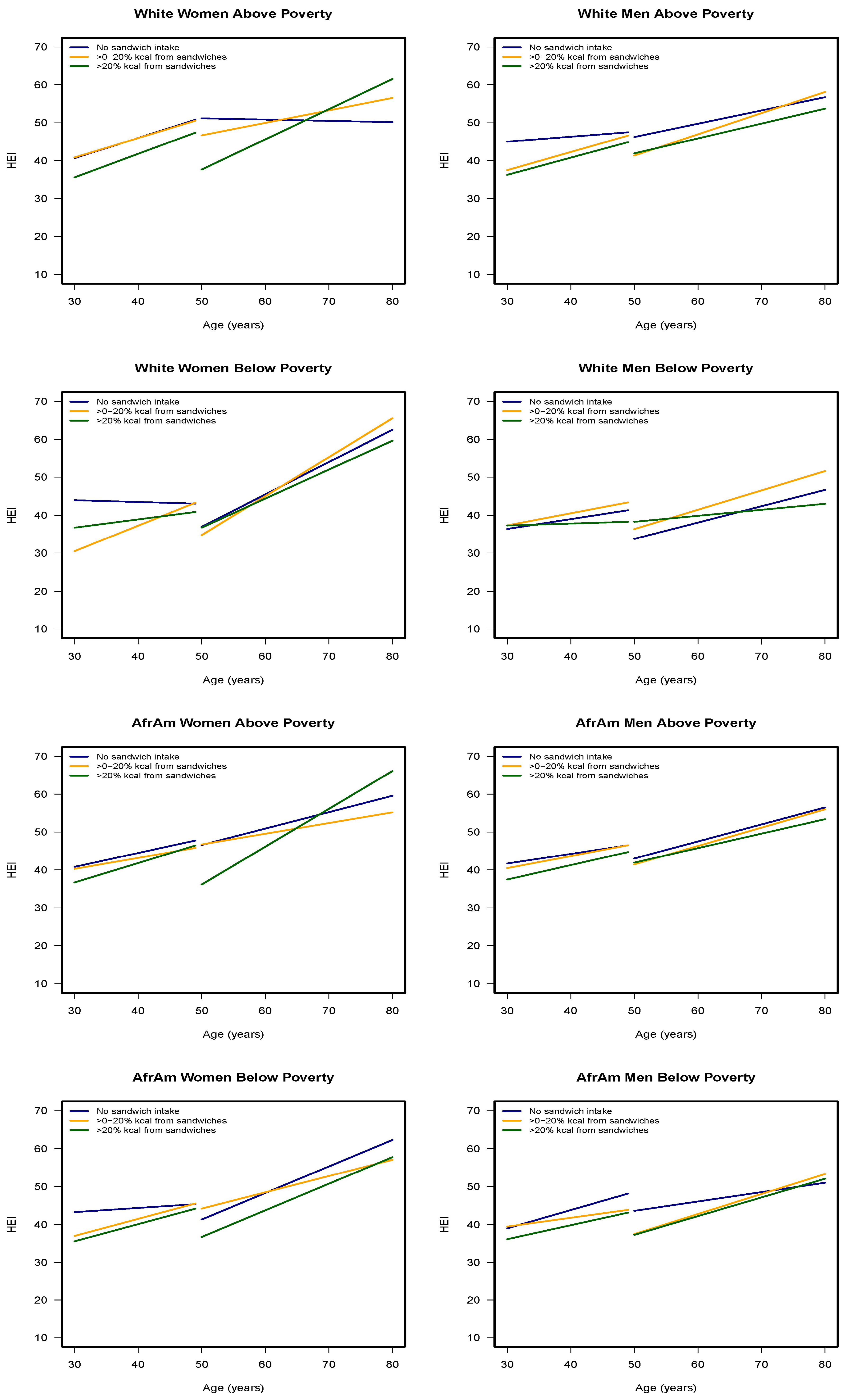
3.1. Association of Energy Contributed by Sandwiches to Diet Quality
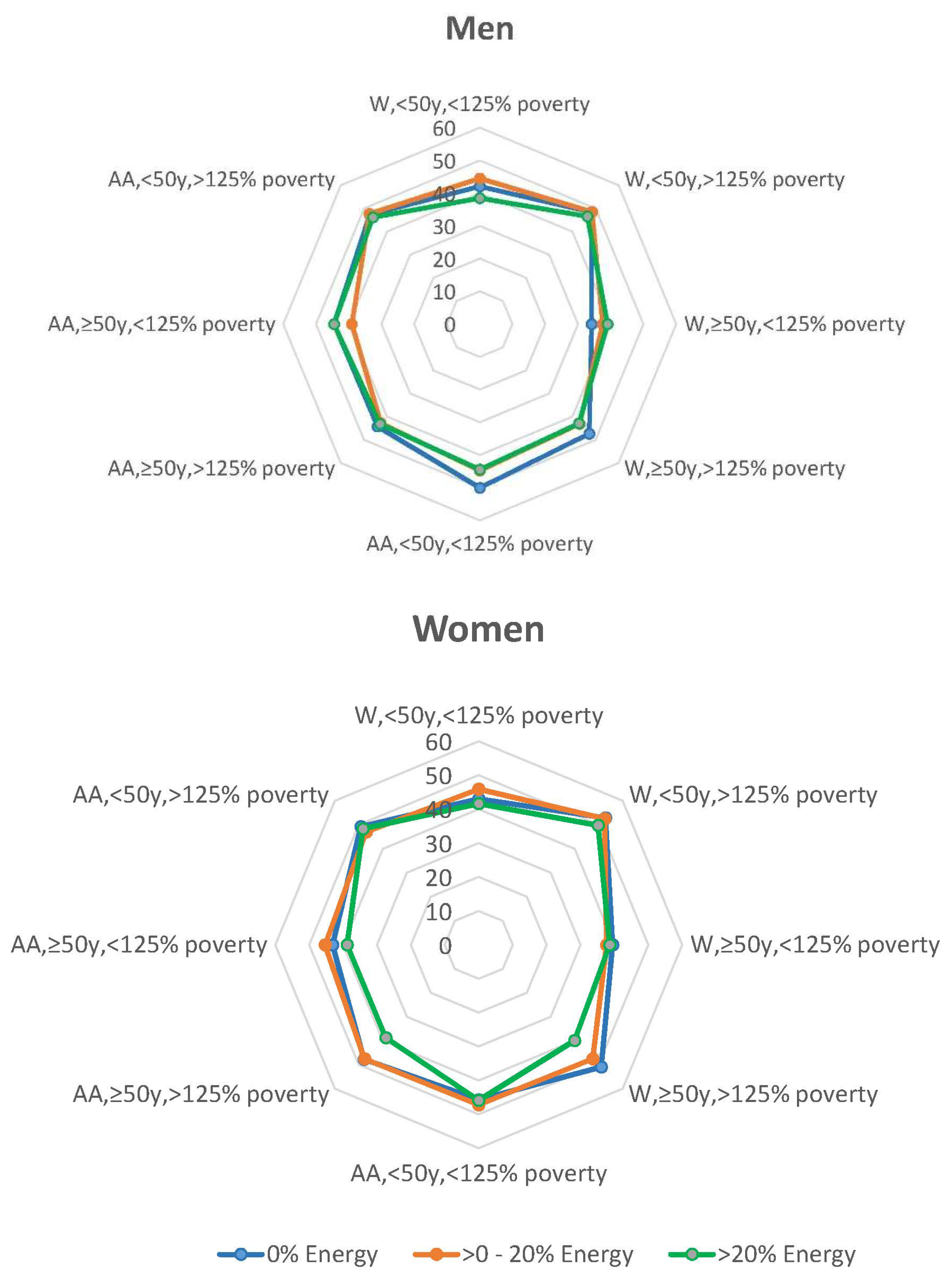
3.2. Sandwiches Consumption Patterns
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Olver, L. The Food Timeline. Available online: http://www.foodtimeline.org/foodsandwiches.html (accessed on 1 July 2020).
- Sebastian, R.S.; Enns, C.W.; Goldman, J.D.; Hoy, M.K.; Moshfegh, A.J. Sandwich consumption by adults in the US: What We Eat In America, NHANES 209-2012. Food Surv. Res. Group Diet. Data Brief 2015, 14, 1–10. [Google Scholar]
- Belam, M. Is it weird to eat the same sandwich for lunch every day? The Guardian, 26 April 2018. Available online: https://www.theguardian.com/lifeandstyle/2018/apr/26/is-it-weird-to-eat-the-same-sandwich-for-lunch-every-day (accessed on 12 September 2020).
- De Oliveira Otto, M.C.; Anderson, C.A.M.; Dearborn, J.L.; Ferranti, E.P.; Mozaffarian, D.; Rao, G.; Wylie-Rosett, J.; Lichtenstein, A.H.; Cardiometabolic, H. Dietary Diversity: Implications for Obesity Prevention in Adult Populations: A Science Advisory From the American Heart Association. Circulation 2018, 138, e160–e168. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services; U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans, 8th ed.; 2015. Available online: https://health.gov/our-work/food-and-nutrition/2015-2020-dietary-guidelines/ (accessed on 12 September 2020).
- Li, Y.P.A.; Wang, D.D.; Liu, X.; Dhana, K.; Franco, O.H.; Kaptoge, S.; Di Angelantonio, E.; Stampfer, M.; Willett, W.C.; Hu, F.B. Impact of Healthy Lifestyle Factors on Life Expectancies in the US Population. Circulation 2018, 138, 345–355. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Agriculture Food and Nutrition Service. HEI Scores for Americans. Available online: https://www.fns.usda.gov/hei-scores-americans (accessed on 1 July 2020).
- Sebastian, R.S.; Wilkinson Enns, C.; Goldman, J.D.; Hoy, M.K.; Moshfegh, A.J. Sandwiches are major contributors of sodium in the diets of American adults: Results from What We Eat in America, National Health and Nutrition Examination Survey 2009–2010. J. Acad. Nutr. Diet. 2015, 115, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Papanikolaou, Y.; Fulgoni, V.L., 3rd. Type of Sandwich Consumption Within a US Dietary Pattern Can Be Associated with Better Nutrient Intakes and Overall Diet Quality: A Modeling Study Using Data from NHANES 2013-2014. Curr. Dev. Nutr. 2019, 3, nzz097. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.; Fulgoni, V.L., 3rd; Berg, E.P. Association of lunch meat consumption with nutrient intake, diet quality and health risk factors in U.S. children and adults: NHANES 2007–2010. Nutr. J. 2015, 14, 128. [Google Scholar] [CrossRef] [PubMed]
- Evans, M.K.; Lepkowski, J.M.; Powe, N.R.; LaVeist, T.; Kuczmarski, M.F.; Zonderman, A.B. Healthy aging in neighborhoods of diversity across the life span (HANDLS): Overcoming barriers to implementing a longitudinal, epidemiologic, urban study of health, race, and socioeconomic status. Ethn. Dis. 2010, 20, 267–275. [Google Scholar] [PubMed]
- US Department of Health and Human Services. The 2004 HHS Poverty Guidelines. Available online: https://aspe.hhs.gov/2004-hhs-poverty-guidelines (accessed on 1 July 2020).
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Raper, N.; Perloff, B.; Ingwersen, L.; Steinfeldt, L.; Anand, J. An overview of USDA’s Dietary Intake Data System. J. Food Compost. Anal. 2004, 17, 545–555. [Google Scholar] [CrossRef]
- McBride, J. Was it a slab, a slice, or a sliver? Agric. Res. 2001, 49, 4–7. [Google Scholar]
- US Department of Agriculture. Food and Nutrient Database for Dietary Studies. Available online: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/food-surveys-research-group/docs/fndds-download-databases/ (accessed on 1 July 2020).
- Guenther, P.M.; Kirkpatrick, S.I.; Reedy, J.; Krebs-Smith, S.M.; Buckman, D.W.; Dodd, K.W.; Casavale, K.O.; Carroll, R.J. The Healthy Eating Index-2010 is a valid and reliable measure of diet quality according to the 2010 Dietary Guidelines for Americans. J. Nutr. 2014, 144, 399–407. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute National Institutes of Health. Healthy Eating Index; How to Choose an Analysis Method on Purpose. Available online: https://epi.grants.cancer.gov/hei/tools.html (accessed on 1 July 2020).
- Healthy Aging in Neighborhoods of Diversity across the Life Span. Healthy Eating Index 2010 Calculation. Available online: https://handls.nih.gov/06Coll-w01HEI.htm (accessed on 1 July 2020).
- Singer, J.D.; Willett, J.B. Applied Longitudinal Data Analysis: Modeling Change and Event Occurrence; Oxford University Press: New York, NY, USA, 2003. [Google Scholar]
- Ibrahim, J.G.; Molenberghs, G. Missing data methods in longitudinal studies: A review. Test 2009, 18, 1–43. [Google Scholar] [CrossRef] [PubMed]
- Stata Corp. Stata Statistical Software, Release 16.0; Stata Corporation: College Station, TX, USA, 2019. [Google Scholar]
- An, R.; Andrade, F.; Grigsby-Toussaint, D. Sandwich consumption in relation to daily dietary intake and diet quality among US adults, 2003–2012. Public Health 2016, 140, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Fanelli Kuczmarski, M.; Mason, M.A.; Beydoun, M.A.; Allegro, D.; Zonderman, A.B.; Evans, M.K. Dietary Patterns and Sarcopenia in an Urban African American and White Population in the United States. J. Nutr. Gerontol. Geriatr. 2013, 32, 291–316. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Visit 1 | Visit 2 | Visit 3 |
|---|---|---|---|
| 2004–2009 | 2009–2013 | 2013–2017 | |
| n | 2177 | 2140 | 2066 |
| Age, X ± SE | 48.33 ± 0.20 | 53.18 ± 0.19 | 56.64 ± 0.20 |
| Sex, % female | 56.5% | 58.8% | 59.0% |
| Race, % AA | 57.9% | 61.4% | 60.9% |
| Income, <125% poverty a | 42.9% | 39.8% | 40.7% |
| Women | Men | |||||||
|---|---|---|---|---|---|---|---|---|
| Age at Baseline Visit | <50 Years | ≥50 Years | <50 Years | ≥50 Years | ||||
| N | % Energy Sandwich | N | % Energy Sandwich | N | % Energy Sandwich | N | % Energy Sandwich | |
| <125% Poverty a | ||||||||
| White | 295 | 19.21 ± 0.92 | 223 | 18.12 ± 1.03 | 168 | 19.75 ± 1.26 | 126 | 25.31 ± 1.56 |
| African American | 700 | 17.65 ± 0.60 | 412 | 17.68 ± 0.84 | 436 | 19.79 ± 0.76 | 266 | 19.10 ± 0.99 |
| >125% Poverty | ||||||||
| White | 509 | 15.41 ± 0.69 | 455 | 16.20 ±0.73 | 400 | 20.14 ± 0.80 | 373 | 18.40 ± 0.85 |
| African American | 584 | 17.65 ± 0.64 | 531 | 17.20 ± 0.68 | 499 | 20.81 ± 0.80 | 406 | 19.73 ± 0.85 |
| HEI-2010 | HEI-2010 | HEI-2010 | HEI-2010 | |||||
| <125% Poverty | ||||||||
| White | 295 | 41.64 ± 0.66 | 223 | 45.66 ± 0.84 | 168 | 40.09 ± 0.81 | 126 | 40.48 ± 0.96 |
| African American | 700 | 44.13 ± 0.41 | 412 | 47.50 ± 0.58 | 436 | 43.50 ± 0.46 | 266 | 43.32 ± 0.64 |
| >125% Poverty | ||||||||
| White | 509 | 47.97 ± 0.64 | 455 | 49.08 ± 0.66 | 400 | 44.90 ± 0.63 | 373 | 47.49 ± 0.68 |
| African American | 584 | 45.73 ± 0.45 | 531 | 50.11 ± 0.54 | 499 | 44.67 ± 0.47 | 406 | 46.91 ± 0.57 |
| Age at Baseline Visit <50 Years | % | Age at Baseline Visit ≥ 50 Years | % |
|---|---|---|---|
| Breakfast | Breakfast | ||
| Egg | 46.1 | Egg | 45.3 |
| Cured and processed meats | 32.1 | Cured and processed meats | 33.0 |
| Poultry | 5.2 | Poultry | 5.1 |
| Lunch | Lunch | ||
| Cured and processed meats | 32.7 | Cured and processed meats | 31.6 |
| Beef | 23.7 | Beef | 20.7 |
| Poultry | 16.3 | Poultry | 14.4 |
| Dinner | Dinner | ||
| Beef | 40.9 | Beef | 31.1 |
| Cured and processed meats | 18.4 | Cured and processed meats | 24.2 |
| Poultry | 14.3 | Poultry | 14.2 |
| Snack | Snack | ||
| Cured and processed meats | 29.8 | Cured and processed meats | 28.1 |
| Beef | 16.0 | Peanut Butter | 15.7 |
| Poultry | 14.5 | Poultry | 14.7 |
| Age at Baseline Visit <50 Years | Age at Baseline Visit ≥ 50 Years | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Sandwich Type | % | Where Obtained, % | Sandwich Type | % | Where Obtained, % | ||||
| Fast Food Restaurant | Other Restaurant b | Store c | Fast Food Restaurant | Other Restaurant b | Store c | ||||
| Cured and processed meats | 28.7 | 17.5 | 1.6 | 80.8 | Cured and processed meats | 29.9 | 12.9 | 2.7 | 84.4 |
| Beef | 22.9 | 53.2 | 5.9 | 40.8 | Beef | 18.5 | 50.2 | 7.5 | 42.3 |
| Poultry | 14.4 | 32.2 | 6.6 | 61.2 | Poultry | 13.4 | 24.8 | 3.4 | 71.9 |
| Egg | 9.6 | 35.2 | 4.6 | 60.2 | Egg | 9.2 | 29.5 | 3.1 | 67.4 |
| Hot dogs | 8.7 | 5.1 | 1.0 | 93.9 | Hot dogs | 8.5 | 5.8 | 9.7 | 92.8 |
| Fish | 6.4 | 33.5 | 2.3 | 64.2 | Fish | 8.4 | 23.9 | 7.8 | 68.3 |
| Peanut Butter | 3.8 | 0 | 0 | 100 | Cheese | 5.1 | 9.7 | 3.2 | 87.1 |
| Cheese | 3.7 | 16.9 | 2.4 | 79.8 | Peanut Butter | 3.8 | 0 | 0 | 100 |
| Pork | 1.0 | 2.9 | 0 | 97.1 | Pork | 1.8 | 2.3 | 2.3 | 95.3 |
| Vegetable and fruit | 0.9 | 13.3 | 10.0 | 76.7 | Vegetable and fruit | 1.4 | 15.2 | 3.0 | 81.8 |
| Mean | 26.9 | 3.5 | 63.7 | Mean | 22.4 | 4.0 | 73.6 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fanelli Kuczmarski, M.; Beydoun, M.A.; Cotugna, N.; Schwenk, E.; Evans, M.K.; Zonderman, A.B. The Relationship of Diet Quality with Proportion of Daily Energy Contributed by Sandwiches Varies by Age over Adulthood in Racially and Socioeconomically Diverse Adults. Nutrients 2020, 12, 2807. https://doi.org/10.3390/nu12092807
Fanelli Kuczmarski M, Beydoun MA, Cotugna N, Schwenk E, Evans MK, Zonderman AB. The Relationship of Diet Quality with Proportion of Daily Energy Contributed by Sandwiches Varies by Age over Adulthood in Racially and Socioeconomically Diverse Adults. Nutrients. 2020; 12(9):2807. https://doi.org/10.3390/nu12092807
Chicago/Turabian StyleFanelli Kuczmarski, Marie, May A. Beydoun, Nancy Cotugna, Elizabeth Schwenk, Michele K. Evans, and Alan B. Zonderman. 2020. "The Relationship of Diet Quality with Proportion of Daily Energy Contributed by Sandwiches Varies by Age over Adulthood in Racially and Socioeconomically Diverse Adults" Nutrients 12, no. 9: 2807. https://doi.org/10.3390/nu12092807
APA StyleFanelli Kuczmarski, M., Beydoun, M. A., Cotugna, N., Schwenk, E., Evans, M. K., & Zonderman, A. B. (2020). The Relationship of Diet Quality with Proportion of Daily Energy Contributed by Sandwiches Varies by Age over Adulthood in Racially and Socioeconomically Diverse Adults. Nutrients, 12(9), 2807. https://doi.org/10.3390/nu12092807