Nutrients and Caloric Intake Associated with Fruits, Vegetables, and Legumes in the Elderly European Population

 ,
,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Data Extraction and Calculations
2.3. Consumption Data and Calculations
2.4. Caloric Intake Estimate from Fruits and Vegetables
3. Results
3.1. IEDI GEMs Elderly Availability
3.2. IEDI GEMs Elderly Nutrition Conversion
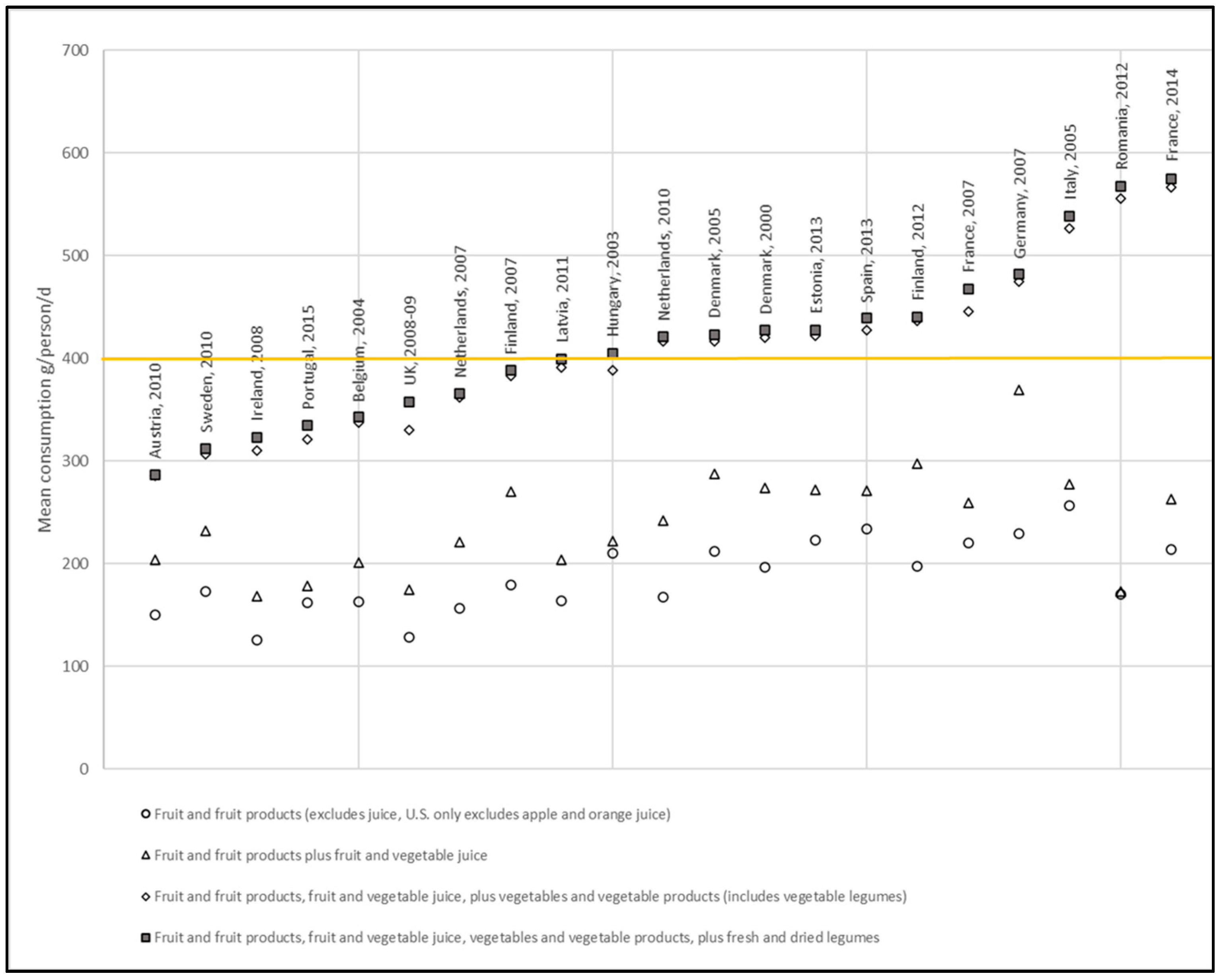
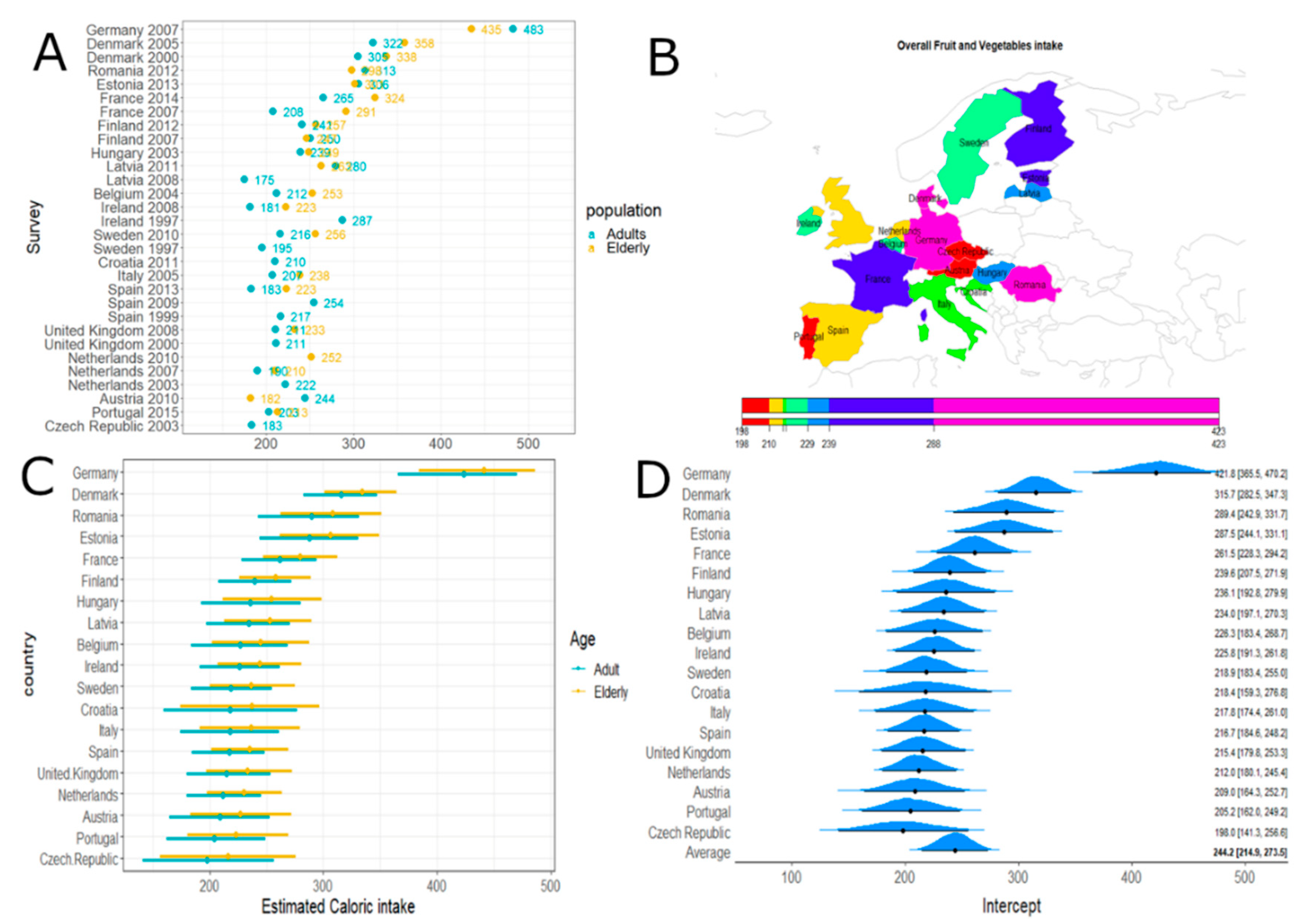
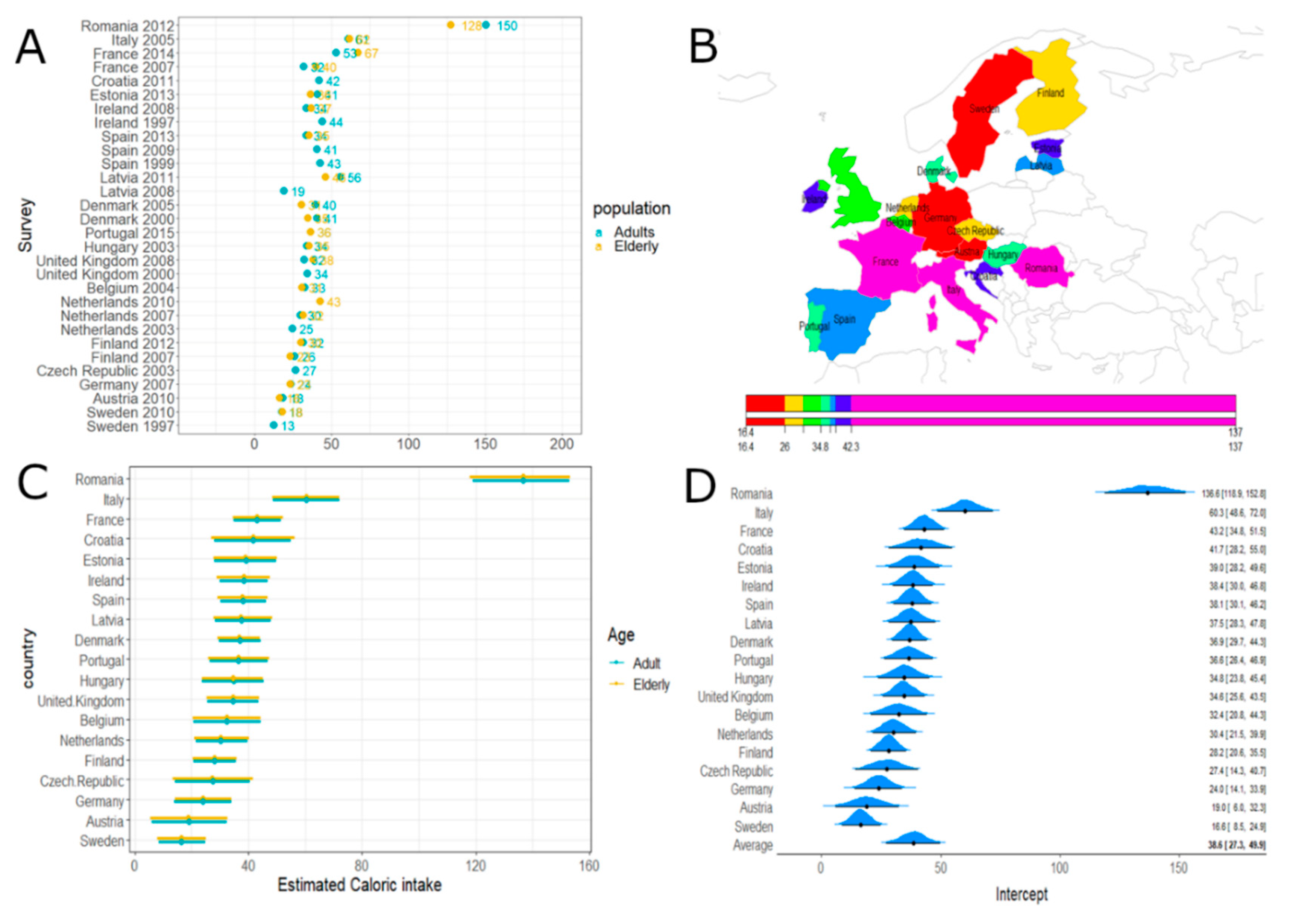
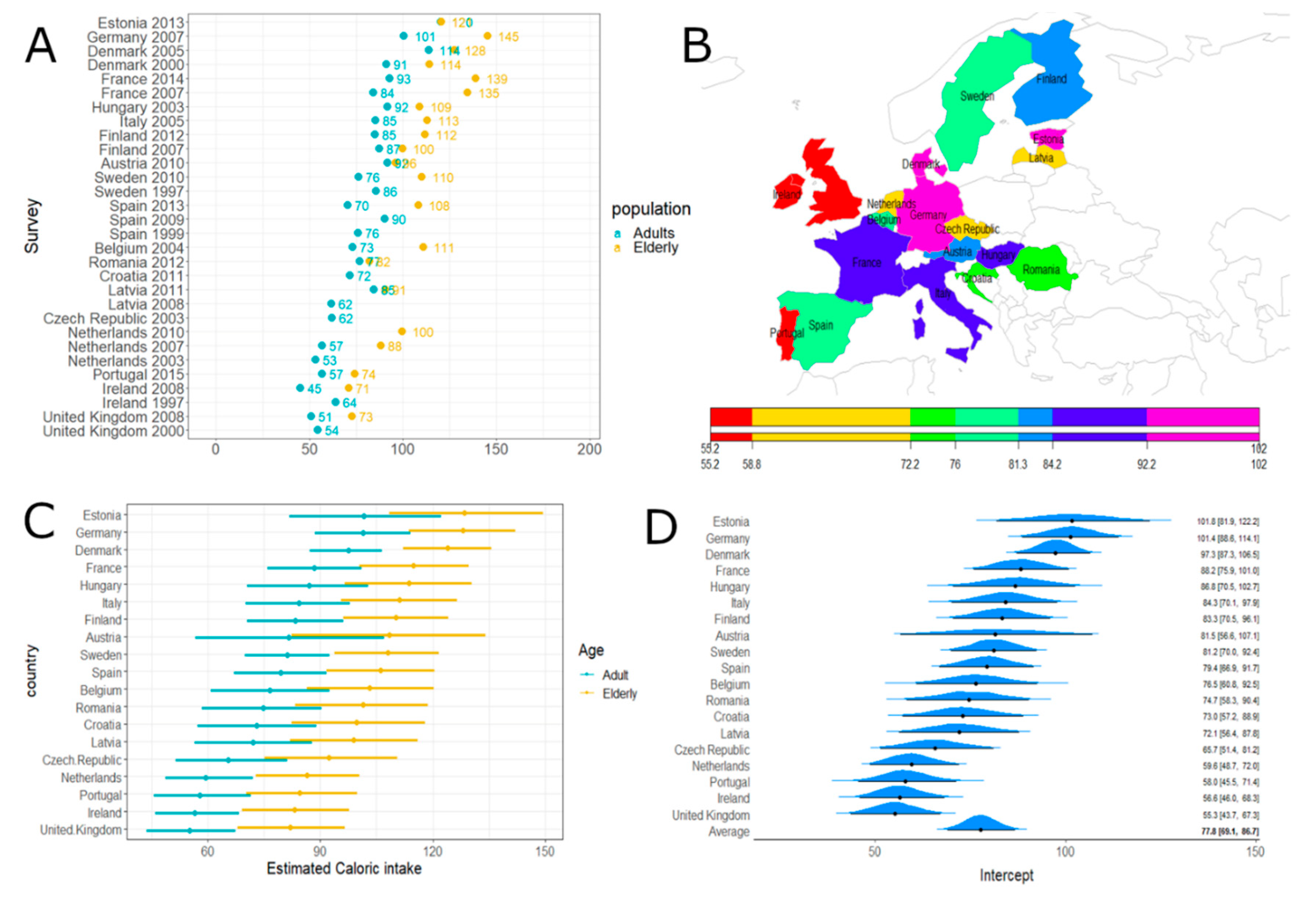
3.3. EFSA Elderly Consumption
3.4. EFSA Elderly Nutrition Conversion
3.5. Caloric Intake from Fruits and Vegetables
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Alwan, A. Global Status Report on Noncommunicable Diseases 2010; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Afshin, A.; Sur, P.J.; Fay, K.A.; Cornaby, L.; Ferrara, G.; Salama, J.S.; Mullany, E.C.; Abate, K.H.; Abbafati, C.; Abebe, Z.; et al. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef]
- World Health Organization. Diet, Nutrition and the Prevention of Chronic Diseases; World Health Organization: Geneva, Switzerland; Food and Agriculture Organization: Rome, Italy, 2003. [Google Scholar]
- Hawkesworth, S.; Dangour, A.D.; Johnston, D.; Lock, K.; Poole, N.; Rushton, J.; Uauy, R.; Waage, J. Feeding the world healthily: The challenge of measuring the effects of agriculture on health. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2010, 365, 3083–3097. [Google Scholar] [CrossRef]
- European Commission Nutrition: Fruit and Vegetables. Available online: https://ec.europa.eu/jrc/en/health-knowledge-gateway/promotion-prevention/nutrition/fruit-vegetables#_GBDStudy2016 (accessed on 14 March 2019).
- Champagne, C.M. Dietary Interventions on Blood Pressure: The Dietary Approaches to Stop Hypertension (Dash) Trials. Nutr. Rev. 2006, 64, S53–S56. [Google Scholar] [CrossRef]
- Weaver, C.M. Potassium and Health. Adv. Nutr. 2013, 4, 368S–377S. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; de Ferranti, S.; Després, J.-P.; Fullerton, H.J.; et al. Heart Disease and Stroke Statistics—2016 Update: A Report From the American Heart Association. Circulation 2016, 133, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Aburto, N.J.; Hanson, S.; Gutierrez, H.; Hooper, L.; Elliott, P.; Cappuccio, F.P. Effect of increased potassium intake on cardiovascular risk factors and disease: Systematic review and meta-analyses. BMJ 2013, 346, f1378. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; MacGregor, G.A. Beneficial effects of potassium on human health. Physiol. Plant. 2008, 133, 725–735. [Google Scholar] [CrossRef]
- Whelton, S.P.; Hyre, A.D.; Pedersen, B.; Yi, Y.; Whelton, P.K.; He, J. Effect of dietary fiber intake on blood pressure: A meta-analysis of randomized, controlled clinical trials. J. Hypertens. 2005, 23, 475–481. [Google Scholar] [CrossRef]
- World Health Organization CINDI (Countrywide Integrated Noncommunicable Diseases Intervention) Dietary Health Guide; World Health Organization: Geneva, Switzerland, 2000.
- Jiang, X.; Huang, J.; Song, D.; Deng, R.; Wei, J.; Zhang, Z. Increased Consumption of Fruit and Vegetables Is Related to a Reduced Risk of Cognitive Impairment and Dementia: Meta-Analysis. Front. Aging Neurosci. 2017, 9, 18. [Google Scholar] [CrossRef]
- Tucker, K.L.; Hannan, M.T.; Chen, H.; Cupples, L.A.; Wilson, P.W.; Kiel, D.P. Potassium, magnesium, and fruit and vegetable intakes are associated with greater bone mineral density in elderly men and women. Am. J. Clin. Nutr. 1999, 69, 727–736. [Google Scholar] [CrossRef]
- Demigné, C.; Sabboh, H.; Rémésy, C.; Meneton, P. Protective Effects of High Dietary Potassium: Nutritional and Metabolic Aspects. J. Nutr. 2004, 134, 2903–2906. [Google Scholar] [CrossRef] [PubMed]
- Dietary Guidelines Advisory Committee. Scientific Report of the 2015 Dietary Guidelines Advisory Committee: Advisory Report to the Secretary of Health and Human Services and the Secretary of Agriculture; U.S. Department of Agriculture, Agricultural Research Service: Washington, DC, USA, 2015.
- International Agency for Research on Cancer. Fruit and Vegetables; IARC Handbooks of Cancer Prevention; World Health Organization: Geneva, Switzerland; International Agency for Research on Cancer: Lyon, France, 2003; Volume 8, ISBN 978-92-832-3008-3. [Google Scholar]
- Linnewiel-Hermoni, K.; Khanin, M.; Danilenko, M.; Zango, G.; Amosi, Y.; Levy, J.; Sharoni, Y. The anti-cancer effects of carotenoids and other phytonutrients resides in their combined activity. Arch. Biochem. Biophys. 2015, 572, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.H. Health-promoting components of fruits and vegetables in the diet. Adv. Nutr. (BethesdaMd.) 2013, 4, 384S–92S. [Google Scholar] [CrossRef] [PubMed]
- Bacchetti, T.; Turco, I.; Urbano, A.; Morresi, C.; Ferretti, G. Relationship of fruit and vegetable intake to dietary antioxidant capacity and markers of oxidative stress: A sex-related study. Nutrition 2019, 61, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Brownie, S. Why are elderly individuals at risk of nutritional deficiency? Int. J. Nurs. Pract. 2006, 12, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, M.A.; Tucker, K.L.; Ryan, N.D.; O’Neill, E.F.; Clements, K.M.; Nelson, M.E.; Evans, W.J.; Fiatarone-Singh, M.A. Higher dietary variety is associated with better nutritional status in frail elderly people. J. Am. Diet. Assoc. 2002, 102, 1096–1104. [Google Scholar] [CrossRef]
- Vellas, B.; Lauque, S.; Andrieu, S.; Nourhashemi, F.; Rolland, Y.; Baumgartner, R.; Garry, P. Nutrition assessment in the elderly. Curr. Opin. Clin. Nutr. Metab. Care 2001, 4, 5–8. [Google Scholar] [CrossRef]
- Bermejo, L.; Aparicio, A.; Andrés, P.; López-Sobaler, A.; Ortega, R. The influence of fruit and vegetable intake on the nutritional status and plasma homocysteine levels of institutionalised elderly people. Public Health Nutr. 2007, 10, 266–272. [Google Scholar] [CrossRef]
- Mingioni, M.; Mehinagic, E.; Laguna, L.; Sarkar, A.; Pirttijärvi, T.; Van Wymelbeke, V.; Artigas, G.; Chen, J.; Kautola, H.; Järvenpää, E.; et al. Fruit and vegetables liking among European elderly according to food preferences, attitudes towards food and dependency. Food Qual. Prefer. 2016, 50, 27–37. [Google Scholar] [CrossRef]
- Roos, G.; Johansson, L.; Kasmel, A.; Klumbiené, J.; Prättälä, R. Disparities in vegetable and fruit consumption: European cases from the north to the south. Public Health Nutr. 2001, 4, 35–43. [Google Scholar] [CrossRef]
- Food and Agriculture Organization; World Health Organization. Principles and Methods for the Risk Assessment of Chemicals in Food: Chapters 6 Dietary Exposure Assessment of Chemicals in Food; Environmental Health Criteria 240; Food and Agriculture Organization: Roma, Italy, 2009; pp. 29–39. [Google Scholar]
- World Health Organization Global Environment Monitoring System (GEMS)/Food Programme Database. Available online: http://www.who.int/foodsafety/chem/gems/en/ (accessed on 17 April 2019).
- Food and Agriculture Organization (FAO) FAOSTAT Statistical Database. Available online: http://www.fao.org/faostat/ (accessed on 14 November 2018).
- World Health Organization GEMS/Food Consumption Database. Available online: https://www.who.int/nutrition/landscape_analysis/nlis_gem_food/en/ (accessed on 30 May 2019).
- Van der Velde-Koerts, T.; van den Boogaard van Oosterhout, C.; Drijvers, J. GEMS International Estimated Daily Intake (IEDI) Food Consumption Cluster Diets (version 3) 2018. Available online: http://www.fao.org/3/Y5221E/y5221e0x.htm (accessed on 20 February 2019).
- European Food Safety Authority The EFSA Comprehensive European Food Consumption Database. Available online: http://www.efsa.europa.eu/en/food-consumption/comprehensive-database (accessed on 21 February 2019).
- European Food Safety Authority Guidance of EFSA: Use of th EFSA Comprehensive European Food Consumption Database in Exposure Assessment. Efsa J. 2011, 9, 2097. [CrossRef]
- Public Health England. McCance & Widdowson Composition of Foods Integrated Dataset (CoFID). Available online: https://www.gov.uk/government/publications/composition-of-foods-integrated-dataset-cofid (accessed on 5 February 2019).
- United States Department of Agriculture, Agricultural Research Service USDA Food Composition Databases. Available online: https://ndb.nal.usda.gov/ndb/ (accessed on 5 February 2019).
- National Institutes of Health, Office of Dietary Supplements Vitamin A. Available online: https://ods.od.nih.gov/factsheets/VitaminA-HealthProfessional/ (accessed on 20 May 2020).
- Bürkner, P.C. brms: An R Package for Bayesian Regression Models using Stan. J. Stat. Softw. 2017, 80, 1–28. [Google Scholar] [CrossRef]
- R Core Team R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020.
- Wang, X.; Ouyang, Y.; Liu, J.; Zhu, M.; Zhao, G.; Bao, W.; Hu, F.B. Fruit and vegetable consumption and mortality from all causes, cardiovascular disease, and cancer: Systematic review and dose-response meta-analysis of prospective cohort studies. BMJ 2014, 349, g4490. [Google Scholar] [CrossRef] [PubMed]
- Miller, V.; Mente, A.; Dehghan, M.; Rangarajan, S.; Zhang, X.; Swaminathan, S.; Dagenais, G.; Gupta, R.; Mohan, V.; Lear, S.; et al. Fruit, vegetable, and legume intake, and cardiovascular disease and deaths in 18 countries (PURE): A prospective cohort study. Lancet 2017, 390, 2037–2049. [Google Scholar] [CrossRef]
- Aune, D.; Giovannucci, E.; Boffetta, P.; Fadnes, L.T.; Keum, N.; Norat, T.; Greenwood, D.C.; Riboli, E.; Tonstad, S.; Vatten, L.J. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality—a systematic review and dose-response meta-analysis of prospective studies. Int. J. Epidemiol. 2017, 46, 1029–1056. [Google Scholar] [CrossRef]
- Chun Yip, C.S.; Chan, W.; Fielding, R. The Associations of Fruit and Vegetable Intakes with Burden of Diseases: A Systematic Review of Meta-Analyses. J. Acad. Nutr. Diet. 2019, 119, 464–481. [Google Scholar] [CrossRef]
- Miller, V.; Yusuf, S.; Chow, C.K.; Dehghan, M.; Corsi, D.J.; Lock, K.; Popkin, B.; Rangarajan, S.; Khatib, R.; Lear, S.A.; et al. Availability, affordability, and consumption of fruits and vegetables in 18 countries across income levels: Findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet Glob. Health 2016, 4, e695–e703. [Google Scholar] [CrossRef]
- Hall, J.N.; Moore, S.; Harper, S.B.; Lynch, J.W. Global variability in fruit and vegetable consumption. Am. J. Prev. Med. 2009, 36, 402–409. [Google Scholar] [CrossRef]
- Lallukka, T.; Laaksonen, M.; Rahkonen, O.; Roos, E.; Lahelma, E. Multiple socio-economic circumstances and healthy food habits. Eur. J. Clin. Nutr. 2006, 61, 701. [Google Scholar] [CrossRef]
- Murphy, M.M.; Barraj, L.M.; Spungen, J.H.; Herman, D.R.; Randolph, R.K. Global assessment of select phytonutrient intakes by level of fruit and vegetable consumption. Br. J. Nutr. 2014, 112, 1004–1018. [Google Scholar] [CrossRef]
- Tennant, D.R.; Davidson, J.; Day, A.J. Phytonutrient intakes in relation to European fruit and vegetable consumption patterns observed in different food surveys. Br. J. Nutr. 2014, 112, 1214–1225. [Google Scholar] [CrossRef] [PubMed]
- Muhammad, A.; D’Souza, A.; Meade, B.; Micha, R.; Mozaffarian, D. How income and food prices influence global dietary intakes by age and sex: Evidence from 164 countries. Bmj Glob. Health 2017, 2, e000184. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Mozaffarian, D.; Sy, S.; Huang, Y.; Liu, J.; Wilde, P.E.; Abrahams-Gessel, S.; Jardim, T.D.S.V.; Gaziano, T.A.; Micha, R. Cost-effectiveness of financial incentives for improving diet and health through Medicare and Medicaid: A microsimulation study. PLoS Med. 2019, 16, e1002761. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Action Plan for the Prevention and Control of NCDs 2013–2020; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| GEMS G Code/Cluster | EFSA Countries | Fruit g/c/d | Vegetables g/c/d | Legumes g/c/d | Total g/c/d |
|---|---|---|---|---|---|
| G07 | Finland, France, UK | 293.3 | 271.3 | 19.7 | 584.3 |
| G08 | Austria, Germany, Spain | 252.9 | 321.6 | 13.7 | 588.2 |
| G10 | Estonia, Italy, Latvia | 258.1 | 348.8 | 19.3 | 626.2 |
| G11 | Belgium, Netherlands | 336.1 | 288.5 | 28.2 | 652.8 |
| G15 | Denmark, Hungary, Ireland, Romania, Portugal, Sweden | 246.9 | 354.3 | 18.9 | 620.1 |
| Countries Mean | 277.5 | 316.9 | 20.0 | 614.3 |
| Units | Male >70 Years | Female >70 Years | |
|---|---|---|---|
| Dietary fiber | g/d | 30 * | 21 * |
| Potassium | mg/d | 4700 | 4700 |
| Calcium | mg/d | 1200 * | 1200 * |
| Magnesium | mg/d | 420 | 320 |
| Phosphorus | mg/d | 700 | 700 |
| Iron | mg/d | 8 | 8 |
| Copper | mg/d | 0.9 | 0.9 |
| Zinc | mg/d | 11 | 8 |
| Manganese | mg/d | 2.3 * | 1.8 * |
| Selenium | μg/d | 55 | 55 |
| Vitamin A (as Retinol Activity Equivalents, RAE) | μg/d | 900 | 700 |
| Vitamin C | mg/d | 90 | 75 |
| Vitamin E (as Tocopherol) | mg/d | 15 | 15 |
| Vitamin K | μg/d | 120 * | 90 * |
| Thiamine (Vitamin B1) | mg/d | 1.2 | 1.1 |
| Riboflavin (Vitamin B2) | mg/d | 1.3 | 1.1 |
| Niacin (Vitamin B3) (as niacin equivalents) | mg/d | 16 | 14 |
| Vitamin B6 | mg/d | 1.7 | 1.5 |
| Pantothenic acid (Vitamin B5) | mg/d | 5 * | 5 * |
| Folate (B9) (as dietary folate equivalents, DFE) | μg/d | 400 | 400 |
| G Cluster | Availability Total F+V+L Mean (g/person/d) | Energy (kcal/d) | Dietary Fiber (g/d) * | Potassium (mg/d) * | Calcium (mg/d) * | Magnesium (mg/d) | Phosphorus (mg/d) | Iron (mg/d) | Copper (mg/d) | Zinc (mg/d) | Manganese (mg/d) * | Selenium (µg/d) | RAE (µg/d) | Vitamin E (mg/d) | Vitamin K1 (µg/d) * | Thiamine (mg/d) | Riboflavin (mg/d) | Niacin (mg/d) | Vitamin B6 (mg/d) | Folate (µg/d) | Pantothenate (mg/d) * | Vitamin C (mg/d) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| G07 | 584.3 | 202.1 | 7.9 | 1135.8 | 120.2 | 63.5 | 163.1 | 2.4 | 0.3 | 1.1 | 0.8 | 2.8 | 278.7 | 1.6 | 84.1 | 0.6 | 0.2 | 3.0 | 0.4 | 144.8 | 1.5 | 120.4 |
| G08 | 588.2 | 198.3 | 7.8 | 1180.1 | 129.5 | 62.4 | 152.6 | 2.3 | 0.3 | 1.0 | 0.8 | 2.8 | 280.1 | 1.6 | 116.1 | 0.5 | 0.2 | 2.5 | 0.5 | 151.0 | 1.4 | 118.6 |
| G10 | 626.2 | 277.3 | 11.4 | 1295.7 | 229.8 | 90.7 | 249.0 | 4.2 | 0.3 | 1.7 | 1.0 | 3.3 | 237.2 | 1.8 | 118.7 | 0.6 | 0.2 | 2.9 | 0.5 | 175.9 | 1.4 | 127.1 |
| G11 | 652.8 | 212.2 | 8.5 | 1285.8 | 137.1 | 66.5 | 169.3 | 2.5 | 0.3 | 1.2 | 1.0 | 4.0 | 426.2 | 1.6 | 84.5 | 0.5 | 0.2 | 2.7 | 0.5 | 164.8 | 1.7 | 118.6 |
| G15 | 620.1 | 222.3 | 9.9 | 1278.7 | 138.6 | 73.4 | 179.7 | 2.6 | 0.3 | 1.1 | 0.8 | 2.7 | 283.3 | 2.0 | 125.2 | 0.6 | 0.2 | 2.9 | 0.5 | 166.6 | 1.4 | 166.0 |
| U.S. RDAs (AI *) males >70 y | 30 * | 4700 * | 1200 * | 420 | 700 | 8 | 0.9 | 11 | 2.3 * | 55 | 900 | 15 | 120 * | 1.2 | 1.3 | 16 | 1.7 | 400 | 5 * | 90 | ||
| G07 | 584.3 | 202.1 | 26% | 24% | 10% | 15% | 23% | 30% | 29% | 10% | 34% | 5% | 31% | 11% | 70% | 50% | 14% | 19% | 26% | 36% | 29% | 134% |
| G08 | 588.2 | 198.3 | 26% | 25% | 11% | 15% | 22% | 28% | 34% | 9% | 34% | 5% | 31% | 10% | 97% | 41% | 13% | 15% | 29% | 38% | 28% | 132% |
| G10 | 626.2 | 277.3 | 38% | 28% | 19% | 22% | 36% | 53% | 38% | 15% | 42% | 6% | 26% | 12% | 99% | 51% | 15% | 18% | 27% | 44% | 28% | 141% |
| G11 | 652.8 | 212.2 | 28% | 27% | 11% | 16% | 24% | 31% | 34% | 11% | 44% | 7% | 47% | 11% | 70% | 43% | 16% | 17% | 28% | 41% | 34% | 132% |
| G15 | 620.1 | 222.3 | 33% | 27% | 12% | 17% | 26% | 32% | 33% | 10% | 36% | 5% | 31% | 13% | 104% | 52% | 14% | 18% | 32% | 42% | 29% | 184% |
| U.S. RDAs (AI *) females >70 y | 21 * | 4700 * | 1200 * | 320 | 700 | 8 | 0.9 | 8 | 1.8 * | 55 | 700 | 15 | 90 * | 1.1 | 1.1 | 14 | 1.5 | 400 | 5 * | 75 | ||
| G07 | 584.3 | 202.1 | 38% | 24% | 10% | 20% | 23% | 30% | 29% | 13% | 43% | 5% | 40% | 11% | 93% | 55% | 16% | 21% | 30% | 36% | 29% | 161% |
| G08 | 588.2 | 198.3 | 37% | 25% | 11% | 20% | 22% | 28% | 34% | 12% | 44% | 5% | 40% | 10% | 129% | 45% | 16% | 18% | 32% | 38% | 28% | 158% |
| G10 | 626.2 | 277.3 | 54% | 28% | 19% | 28% | 36% | 53% | 38% | 21% | 54% | 6% | 34% | 12% | 132% | 56% | 18% | 21% | 31% | 44% | 28% | 169% |
| G11 | 652.8 | 212.2 | 41% | 27% | 11% | 21% | 24% | 31% | 34% | 15% | 56% | 7% | 61% | 11% | 94% | 47% | 19% | 19% | 32% | 41% | 34% | 158% |
| G15 | 620.1 | 222.3 | 47% | 27% | 12% | 23% | 26% | 32% | 33% | 14% | 46% | 5% | 40% | 13% | 139% | 56% | 17% | 20% | 36% | 42% | 29% | 221% |
| Country EFSA Database | Year | G Cluster | Consumption Total F+V+J+L mean (g/p/d) | Energy (Kcal/d) | Dietary Fiber (g/d) * | Potassium (mg/d, from g/d) * | Calcium (mg/d) * | Magnesium (mg/d) | Phosphorus (mg/d) | Iron (mg/d) | Copper (mg/d, from ug/d) | Zinc (mg/d) | Manganese (mg/d) * | Selenium (µg/d) | RAE (µg/d) | Vitamin E (mg/d) | Vitamin K1 (µg/d) * | Thiamine (mg/d) | Riboflavin (mg/d) | Niacin (mg/d) | Vitamin B6 (mg/d) | Folate (µg/d) | Pantothenate (mg/d) * | Vitamin C (mg/d) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| U.S. RDAs or AI *: males >70 y | 30 * | 4700 * | 1200 * | 420 | 700 | 8 | 0.9 | 11 | 2.3 * | 55 | 900 | 15 | 120 | 1.2 | 1.3 | 16 | 1.7 | 400 | 5 * | 90 | ||||
| U.S. RDAs (AI *) females >70 y | 21 * | 4700 * | 1200 * | 320 | 700 | 8 | 0.9 | 8 | 1.8 * | 55 | 700 | 15 | 90 * | 1.1 | 1.1 | 14 | 1.5 | 400 | 5 * | 75 | ||||
| Austria | 2010 | G08 | 287.2 | 164.3 | 3.0 | 543.7 | 51.1 | 30.4 | 55.6 | 1.0 | 0.1 | 0.3 | 0.5 | 0.9 | 59.5 | 0.7 | 51.9 | 0.2 | 0.1 | 1.0 | 0.2 | 52.3 | 0.5 | 68.9 |
| Belgium | 2004 | G11 | 342.2 | 165.2 | 4.5 | 668.2 | 64.3 | 34.4 | 80.1 | 1.1 | 0.2 | 0.4 | 0.4 | 1.6 | 117.5 | 1.1 | 48.7 | 0.3 | 0.1 | 1.4 | 0.2 | 75.0 | 0.6 | 59.4 |
| Denmark | 2000 | G15 | 427.3 | 220.5 | 5.1 | 848.1 | 76.5 | 44.8 | 90.3 | 1.5 | 0.2 | 0.5 | 0.5 | 0.9 | 182.1 | 1.3 | 37.8 | 0.5 | 0.1 | 1.8 | 0.3 | 74.5 | 0.8 | 78.0 |
| Denmark | 2005 | G15 | 423.0 | 253.3 | 4.7 | 885.2 | 73.1 | 46.4 | 94.8 | 1.5 | 0.2 | 0.5 | 0.6 | 1.3 | 167.9 | 1.1 | 38.6 | 0.4 | 0.1 | 1.7 | 0.3 | 74.2 | 0.8 | 79.6 |
| Estonia | 2013 | G10 | 427.4 | 219.6 | 5.4 | 794.6 | 82.0 | 42.0 | 87.1 | 1.7 | 0.2 | 0.5 | 0.5 | 1.1 | 137.0 | 0.9 | 30.3 | 0.3 | 0.1 | 1.5 | 0.3 | 68.1 | 0.8 | 70.9 |
| Finland | 2007 | G07 | 388.6 | 182.7 | 4.5 | 637.1 | 69.1 | 37.8 | 81.4 | 1.3 | 0.1 | 0.5 | 0.4 | 0.8 | 101.6 | 0.9 | 29.9 | 0.4 | 0.1 | 1.5 | 0.2 | 68.7 | 0.8 | 93.4 |
| Finland | 2012 | G07 | 440.7 | 199.2 | 4.8 | 720.5 | 72.3 | 41.1 | 85.9 | 1.2 | 0.2 | 0.5 | 0.5 | 0.8 | 165.2 | 1.1 | 37.1 | 0.5 | 0.1 | 1.6 | 0.3 | 86.6 | 0.9 | 97.2 |
| France | 2007 | G07 | 467.2 | 241.7 | 8.0 | 954.9 | 124.8 | 57.7 | 148.4 | 3.7 | 0.2 | 1.0 | 0.8 | 4.3 | 188.7 | 1.3 | 49.1 | 0.4 | 0.1 | 1.9 | 0.3 | 118.2 | 1.0 | 70.9 |
| France | 2014 | G07 | 575.3 | 240.7 | 7.8 | 1145.4 | 144.6 | 61.0 | 145.6 | 2.4 | 0.3 | 0.9 | 0.7 | 2.7 | 203.5 | 1.9 | 75.9 | 0.5 | 0.2 | 2.3 | 0.4 | 148.4 | 1.1 | 88.0 |
| Germany | 2007 | G08 | 481.5 | 390.0 | 4.8 | 1202.7 | 97.3 | 64.0 | 123.5 | 2.8 | 0.2 | 0.6 | 0.9 | 1.9 | 102.0 | 1.1 | 43.5 | 0.3 | 0.1 | 2.0 | 0.3 | 69.0 | 0.9 | 109.3 |
| Hungary | 2003 | G15 | 404.7 | 171.8 | 6.4 | 663.6 | 86.6 | 40.8 | 104.1 | 1.8 | 0.2 | 0.6 | 0.4 | 1.3 | 97.6 | 1.0 | 60.1 | 0.4 | 0.1 | 1.4 | 0.3 | 71.6 | 0.7 | 64.5 |
| Ireland | 2008 | G15 | 323.3 | 142.6 | 4.3 | 669.2 | 66.6 | 37.6 | 93.5 | 1.3 | 0.2 | 0.6 | 0.4 | 1.8 | 186.8 | 1.1 | 48.1 | 0.4 | 0.1 | 1.6 | 0.3 | 80.3 | 0.8 | 61.5 |
| Italy | 2005 | G10 | 538.6 | 197.3 | 7.0 | 1416.1 | 130.2 | 81.9 | 159.5 | 2.7 | 0.4 | 1.0 | 0.6 | 3.1 | 308.6 | 3.4 | 101.1 | 0.7 | 0.2 | 3.5 | 0.4 | 144.0 | 1.3 | 109.8 |
| Latvia | 2011 | G10 | 399.4 | 178.2 | 6.2 | 751.0 | 112.0 | 44.3 | 92.1 | 2.4 | 0.2 | 0.6 | 0.7 | 1.0 | 188.8 | 1.1 | 45.6 | 0.3 | 0.1 | 1.5 | 0.3 | 100.6 | 0.8 | 80.5 |
| Netherlands | 2007 | G11 | 365.4 | 154.5 | 4.4 | 676.5 | 77.2 | 38.7 | 83.0 | 1.3 | 0.2 | 0.5 | 0.5 | 1.7 | 124.3 | 1.1 | 87.3 | 0.4 | 0.1 | 1.5 | 0.3 | 98.9 | 0.8 | 74.8 |
| Netherlands | 2010 | G11 | 420.4 | 186.3 | 5.4 | 796.3 | 91.3 | 44.8 | 100.2 | 1.7 | 0.2 | 0.5 | 0.5 | 1.9 | 153.1 | 1.4 | 89.8 | 0.4 | 0.1 | 1.6 | 0.3 | 112.8 | 0.9 | 82.8 |
| Portugal | 2015 | G15 | 334.3 | 142.3 | 4.3 | 701.2 | 82.8 | 44.9 | 99.3 | 1.7 | 0.2 | 0.6 | 0.5 | 1.3 | 151.0 | 1.5 | 28.1 | 0.4 | 0.1 | 1.4 | 0.3 | 80.3 | 0.7 | 60.6 |
| Romania | 2012 | G15 | 567.5 | 221.8 | 7.8 | 1152.7 | 115.1 | 57.8 | 140.1 | 2.1 | 0.3 | 0.8 | 0.6 | 2.1 | 273.3 | 2.1 | 49.8 | 0.4 | 0.1 | 2.4 | 0.4 | 113.2 | 1.0 | 80.2 |
| Spain | 2013 | G08 | 439.2 | 186.5 | 6.0 | 815.9 | 83.8 | 50.3 | 111.3 | 1.7 | 0.3 | 0.7 | 0.6 | 2.9 | 110.9 | 1.5 | 57.9 | 0.5 | 0.1 | 2.0 | 0.3 | 106.3 | 0.9 | 93.2 |
| Sweden | 2010 | G15 | 312.2 | 163.7 | 3.5 | 559.4 | 49.0 | 32.5 | 67.2 | 1.0 | 0.1 | 0.4 | 0.4 | 0.8 | 89.3 | 0.9 | 21.4 | 0.3 | 0.1 | 1.3 | 0.2 | 60.0 | 0.6 | 66.8 |
| United Kingdom | 2008 | G07 | 357.5 | 171.8 | 5.8 | 783.0 | 76.9 | 47.7 | 120.8 | 1.8 | 0.2 | 0.8 | 0.7 | 6.6 | 160.2 | 1.5 | 57.7 | 0.4 | 0.1 | 1.9 | 0.4 | 93.1 | 0.9 | 64.8 |
| Mean of EFSA studies | 415.4 | 199.7 | 5.4 | 827.9 | 87.0 | 46.7 | 103.0 | 1.8 | 0.2 | 0.6 | 0.6 | 1.9 | 155.7 | 1.3 | 51.9 | 0.4 | 0.1 | 1.7 | 0.3 | 90.3 | 0.8 | 78.8 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Azzolina, D.; Vedovelli, L.; Gallipoli, S.; French, M.; Ghidina, M.; Lamprecht, M.; Tsiountsioura, M.; Lorenzoni, G.; Gregori, D. Nutrients and Caloric Intake Associated with Fruits, Vegetables, and Legumes in the Elderly European Population. Nutrients 2020, 12, 2746. https://doi.org/10.3390/nu12092746
Azzolina D, Vedovelli L, Gallipoli S, French M, Ghidina M, Lamprecht M, Tsiountsioura M, Lorenzoni G, Gregori D. Nutrients and Caloric Intake Associated with Fruits, Vegetables, and Legumes in the Elderly European Population. Nutrients. 2020; 12(9):2746. https://doi.org/10.3390/nu12092746
Chicago/Turabian StyleAzzolina, Danila, Luca Vedovelli, Silvia Gallipoli, Megan French, Marco Ghidina, Manfred Lamprecht, Melina Tsiountsioura, Giulia Lorenzoni, and Dario Gregori. 2020. "Nutrients and Caloric Intake Associated with Fruits, Vegetables, and Legumes in the Elderly European Population" Nutrients 12, no. 9: 2746. https://doi.org/10.3390/nu12092746
APA StyleAzzolina, D., Vedovelli, L., Gallipoli, S., French, M., Ghidina, M., Lamprecht, M., Tsiountsioura, M., Lorenzoni, G., & Gregori, D. (2020). Nutrients and Caloric Intake Associated with Fruits, Vegetables, and Legumes in the Elderly European Population. Nutrients, 12(9), 2746. https://doi.org/10.3390/nu12092746