Probiotics as a Coadjuvant Factor in Active or Quiescent Inflammatory Bowel Disease of Adults—A Meta-Analytical Study

 , , , , and
, , , , and
Abstract
1. Introduction
2. Methods
2.1. Search Strategy and Inclusion Criteria
2.2. Data Extraction
2.3. Quality and Bias Risk Assessment
2.4. Data Synthesis and Statistical Analysis
3. Results
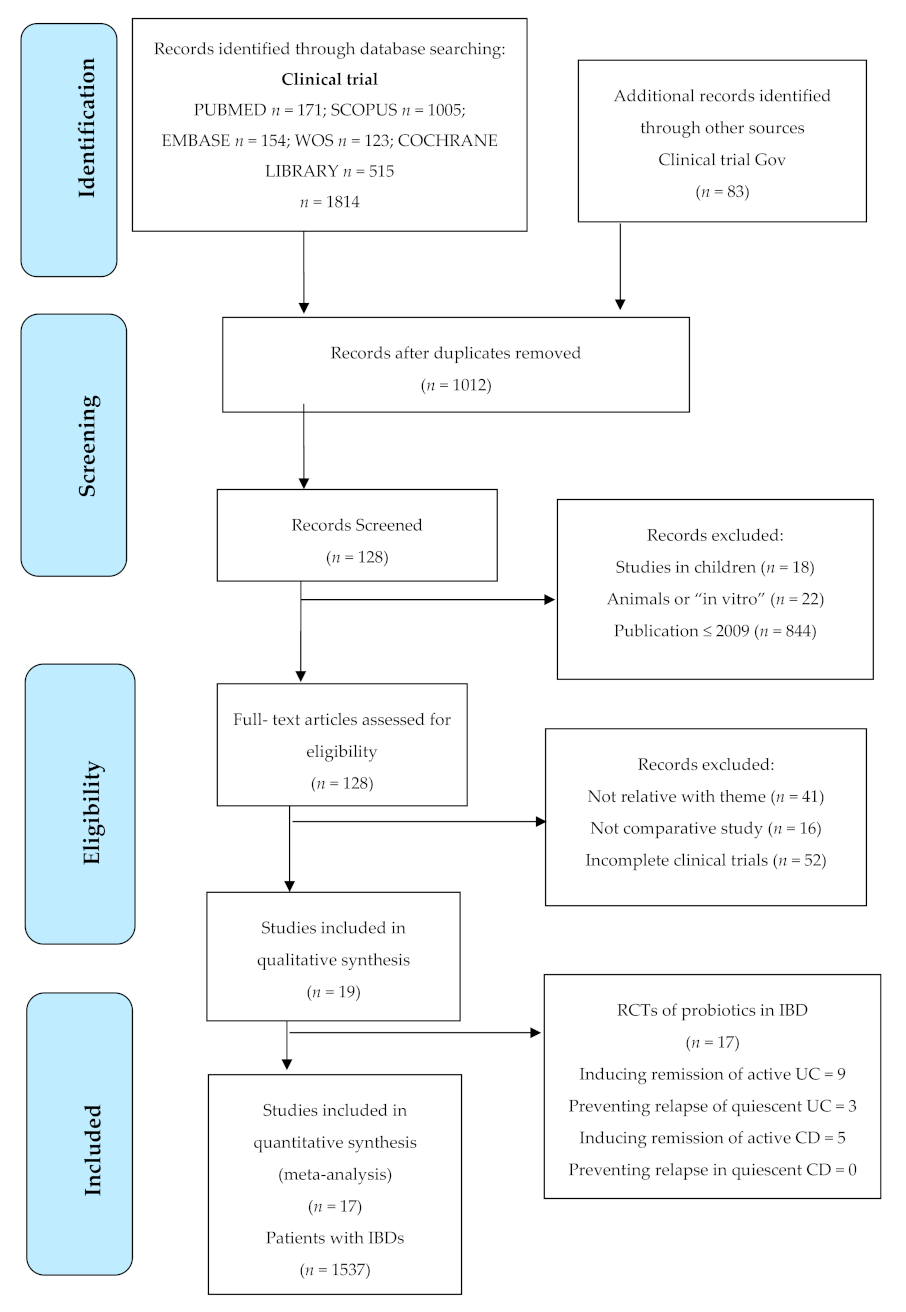
3.1. Results Obtained in the Selection of Articles
3.2. Descriptive Analysis of the Results Found
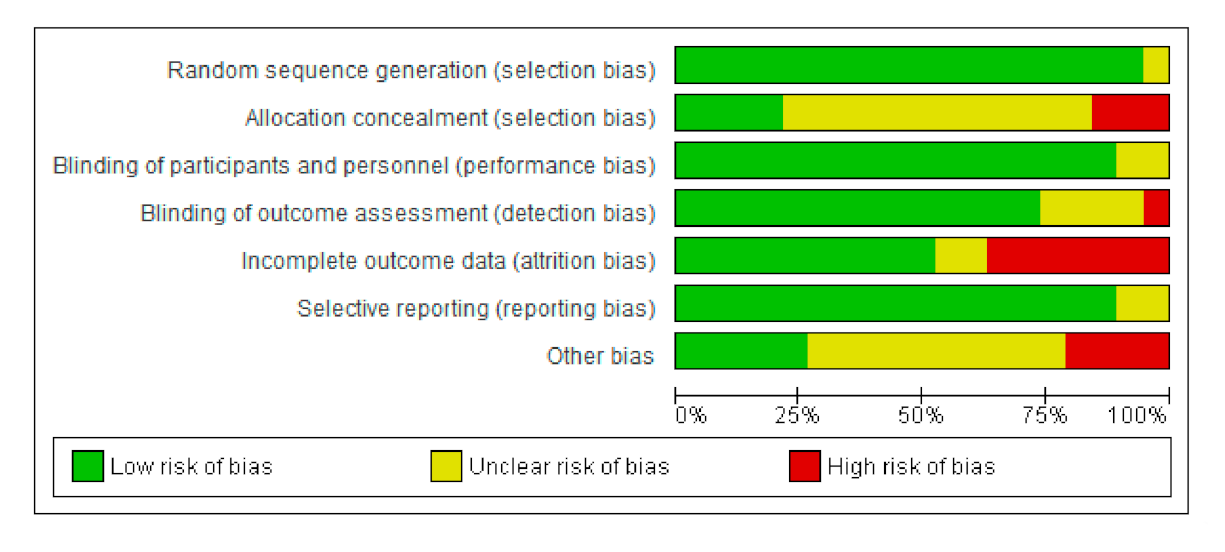
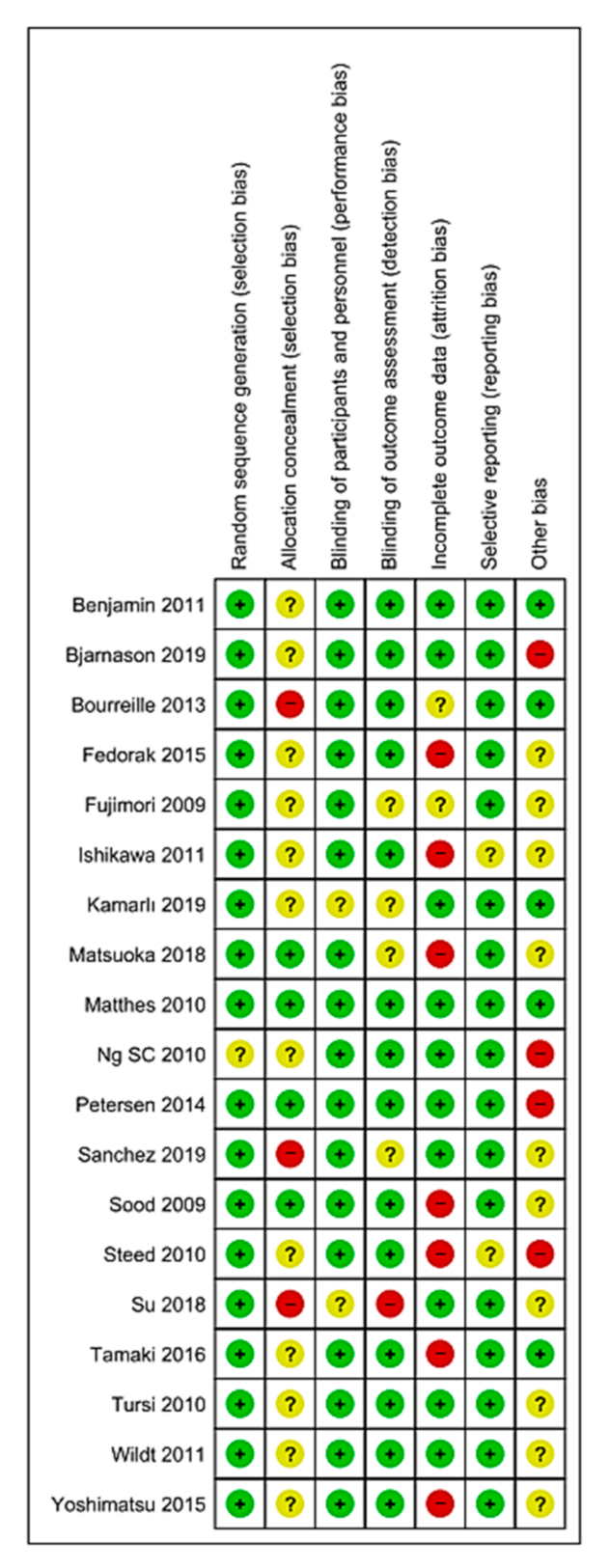
3.3. Bias Risk Assessment of the Selected Studies and Publication Bias
3.4. Results of the Meta-Analysis
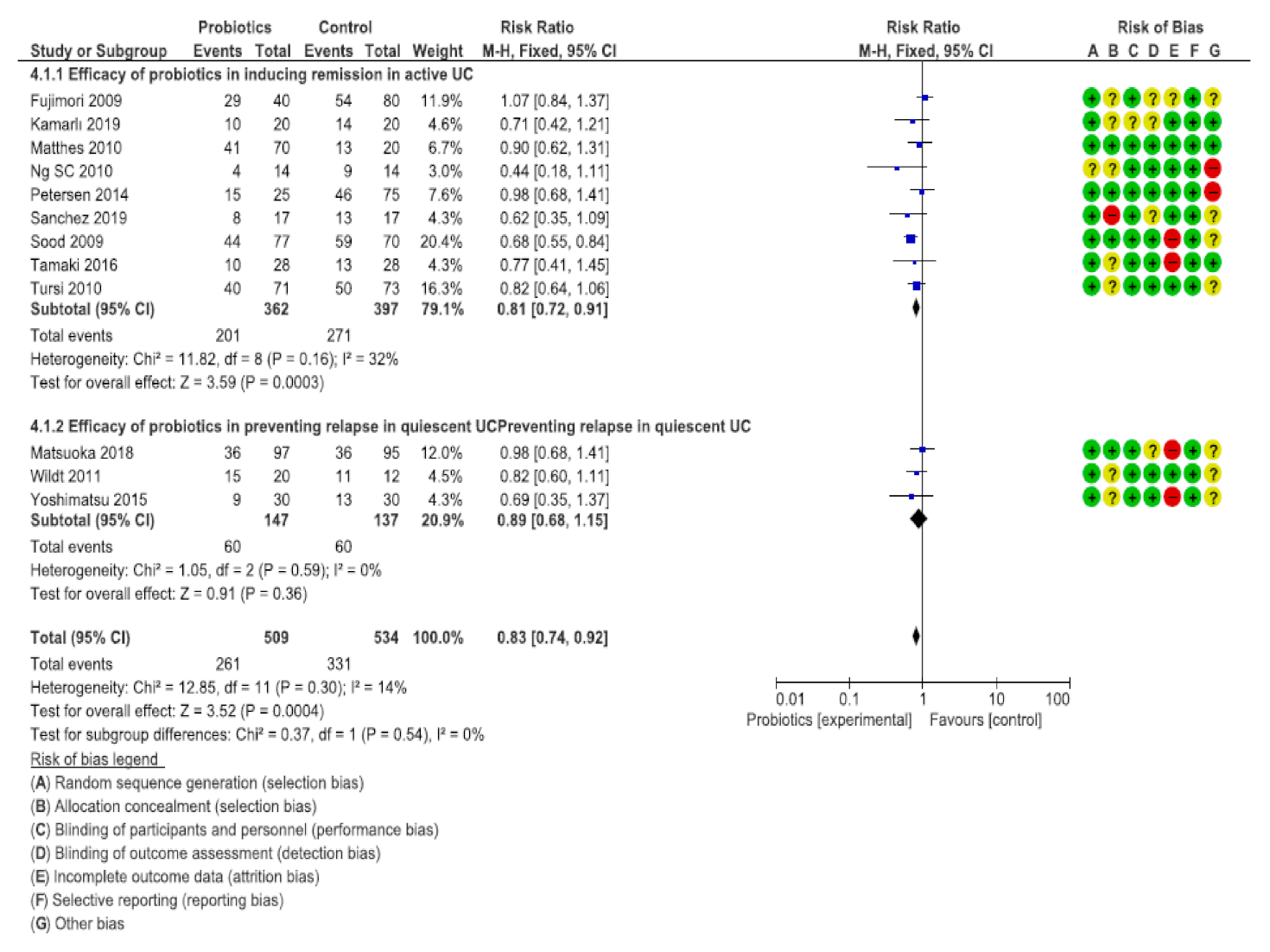
3.5. Efficacy of the Probiotics to Induce Remission in Active UC
3.6. Efficacy of Probiotics to Prevent Relapse in UC
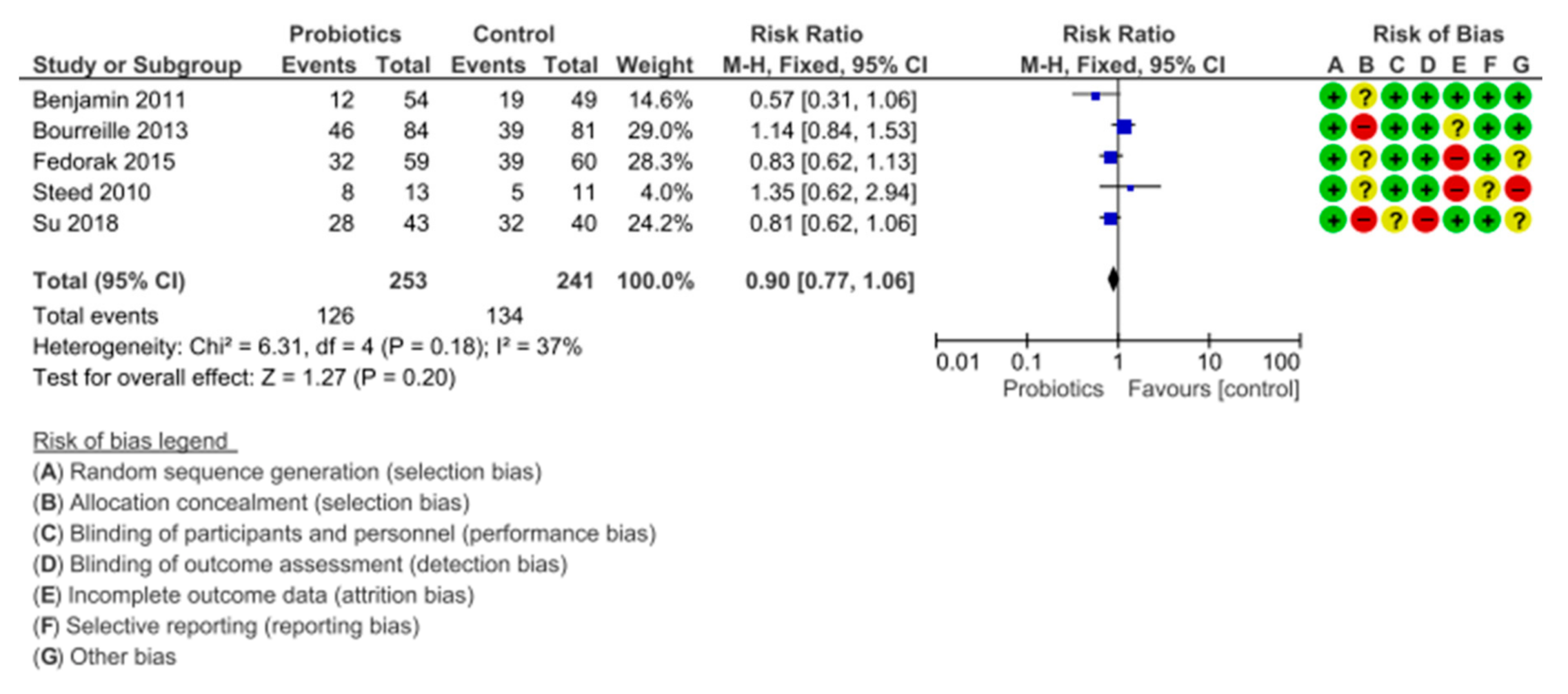
3.7. Efficacy of the Probiotics for the Remission of Crohn’s Disease
4. Discussion
4.1. Efficacy of the Probiotics in UC
4.2. Efficacy of Probiotics in Crohn’s Disease
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Argüelles-Arias, F.; Benallal, D.C.; Benítez, J.M.; Amarillo, R.P.; Iglesias, E.; Laria, L.C.; García, V.S.; Pérez, M.B.M.; Vilches, Á.; Álvarez, Á.C.; et al. Evolution of the incidence of inflammatory bowel disease in Southern Spain. Rev. Esp. Enferm. Dig. 2017, 109, 757–760. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Martínez-Gómez, M.J.; Meliá-Fernández, C.; Romeo-Donlo, M. Nutrición en enfermedad inflamatoria intestinal. Nutr. Hosp. 2016, 33, 59–62. [Google Scholar] [CrossRef] [PubMed]
- Shah, N.D.; Parian, A.M.; Mullin, G.E.; Limketkai, B.N. Oral Diets and Nutrition Support for Inflammatory Bowel Disease. Nutr. Clin. Pr. 2015, 30, 462–473. [Google Scholar] [CrossRef] [PubMed]
- Marteau, P.; Allez, M.; Jian, R. Enfermedad de Crohn. EMC-Tratado de Med. 2013, 17, 1–8. [Google Scholar] [CrossRef]
- Yamamoto, T.; Shimoyama, T.; Kuriyama, M. Dietary and enteral interventions for Crohn’s disease. Curr. Opin. Biotechnol. 2017, 44, 69–73. [Google Scholar] [CrossRef]
- Aleksandrova, K.; Romero-Mosquera, B.; Hernandez, V. Diet, Gut Microbiome and Epigenetics: Emerging Links with Inflammatory Bowel Diseases and Prospects for Management and Prevention. Nutrients 2017, 9, 962. [Google Scholar] [CrossRef]
- Chen, W.-X.; Ren, L.-H.; Shi, R.-H. Enteric microbiota leads to new therapeutic strategies for ulcerative colitis. World J. Gastroenterol. 2014, 20, 15657–15663. [Google Scholar] [CrossRef]
- Mariño-García, A.; Núñez-Velázquez, M.; Barret-Penie, J. Microbiota, Probiotics, Prebiotics, and Synbiotics. Acta Medica. Cordoba. 2016, 17, 1–12. Available online: http://bvs.sld.cu/revistas/act/vol17_1_16/actsu216.htm (accessed on 20 December 2019).
- Corzo, N.; Alonso, J.L.; Azpiroz, F.; A Calvo, M.; Cirici, M.; Leis, R.; Lombó, F.; Mateos-Aparicio, I.; Plou, F.J.; Ruas-Madiedo, P.; et al. Prebiotics: Concept, properties and beneficial effects. Nutr. Hosp. 2015, 31, 99–118. [Google Scholar]
- Patel, R.M.; Denning, P.W. Therapeutic use of prebiotics, probiotics, and postbiotics to prevent necrotizing enterocolitis. Clin. Perinatol. 2013, 40, 11–25. [Google Scholar] [CrossRef]
- Aguilar-Toalá, J.; García-Varela, R.; Garcia, H.; Mata-Haro, V.; González-Córdova, A.; Vallejo-Cordoba, B.; Hernandez-Mendoza, A. Postbiotics: An evolving term within the functional foods field. Trends Food Sci. Technol. 2018, 75, 105–114. [Google Scholar] [CrossRef]
- Mitsuyama, K.; Saiki, T.; Kanauchi, O.; Iwanaga, T.; Tomiyasu, N.; Nishiyama, N.; Tateishi, H.; Shirachi, A.; Ide, M.; Suzuki, A.; et al. Treatment of ulcerative colitis with germinated barley foodstuff feeding: A pilot study. Aliment. Pharmacol. Ther. 1998, 12, 1225–1230. [Google Scholar] [CrossRef] [PubMed]
- Zocco, M.A.; Verme, L.Z.D.; Cremonini, F.; Piscaglia, A.C.; Nista, E.C.; Candelli, M.; Novi, M.; Rigante, D.; Cazzato, I.; Ojetti, V.; et al. Efficacy of Lactobacillus GG in maintaining remission of ulcerative colitis. Aliment. Pharmacol. Ther. 2006, 23, 1567–1574. [Google Scholar] [CrossRef]
- Bibiloni, R.; Fedorak, R.N.; Tannock, G.W.; Madsen, K.L.; Gionchetti, P.; Campieri, M.; De Simone, C.; Sartor, R.B. VSL#3 Probiotic-Mixture Induces Remission in Patients with Active Ulcerative Colitis. Am. J. Gastroenterol. 2005, 100, 1539–1546. Available online: https://journals.lww.com/ajg/Abstract/2005/07000/VSL_3_Probiotic_Mixture_Induces_Remission_in.20.aspx (accessed on 20 December 2019). [CrossRef] [PubMed]
- Assisi, R.F. GISDI Study Group. Combined butyric acid/mesalazine treatment in ulcerative colitis with mild-moderate activity. Results of a multicentre pilot study. Minerva Gastroenterol. Dietol. 2008, 54, 231–238. Available online: https://www.minervamedica.it/en/journals/gastroenterologica-dietologica/article.php?cod=R08Y2008N03A0231 (accessed on 20 December 2019). [CrossRef] [PubMed]
- Krag, A. Safety and efficacy of Profermin® to induce remission in ulcerative colitis. World J. Gastroenterol. 2012, 18, 1773. [Google Scholar] [CrossRef] [PubMed]
- Sanromán-Alvarez, L.; De Castro-Parga, M.L.; Hernández-Ramírez, V.; Pineda-Mariño, J.R.; Salgado-Alvarez, C.; Rodríguez-Grégori, J.M. Consulta telemática realizada por Enfermería en pacientes con enfermedad inflamatoria intestinal: Valoración de su capacidad resolutiva y costes. Enfermería Clínica 2014, 24, 102–110. [Google Scholar] [CrossRef]
- Casellas, F.; Panés, J.; García-Sánchez, V.; Ginard, D.; Gomollón, F.; Hinojosa, J.; Marín-Jiménez, I.; Barreiro, M.; Bastida, G.; Lindner, L.; et al. Costes médicos directos de la enfermedad de Crohn en España. PharmacoEconomics Span. Res. Artic. 2010, 7, 38–46. [Google Scholar] [CrossRef]
- Estarli, M.; Martínez-Rodríguez, R.; Baladia, E.; Camacho, S.; Buhring, K.; Herrero-López, A.; Gil-González, D.; Barrera, E.S.A.; Agüero, S.D. Ítems de referencia para publicar Protocolos de Revisiones Sistemáticas y Metaanálisis: Declaración PRISMA-P 2015. Rev. Esp. Nutr. Hum. Diet. 2016, 20, 148. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. London: The Cochrane Collaboration 2011. Available online: https://training.cochrane.org/handbook/current (accessed on 20 December 2019).
- Pudar Hozo, S.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Fujimori, S.; Gudis, K.; Mitsui, K.; Seo, T.; Yonezawa, M.; Tanaka, S.; Tatsuguchi, A.; Sakamoto, C. A randomized controlled trial on the efficacy of synbiotic versus probiotic or prebiotic treatment to improve the quality of life in patients with ulcerative colitis. Nutrition 2009, 25, 520–525. [Google Scholar] [CrossRef]
- Sood, A.; Midha, V.; Makharia, G.K.; Ahuja, V.; Singal, D.; Goswami, P.; Tandon, R.K. The probiotic preparation, VSL#3 induces remission in patients with mild-to-moderately active ulcerative colitis. Clin. Gastroenterol. Hepatol. 2009, 7, 1202–1209. [Google Scholar] [CrossRef]
- Matthes, H.; Krummenerl, T.; Giensch, M.; Wolff, C.; Schulze, J. Clinical trial: Probiotic treatment of acute distal ulcerative colitis with.rectally administered Escherichia coli Nissle 1917 (EcN). BMC Complement. Altern. Med. 2010, 10, 13. [Google Scholar] [CrossRef]
- Ng, S.C.; Plamondon, S.; Kamm, M.A.; Hart, A.L.; Al-Hassi, H.O.; Guenther, T.; Stagg, A.J.; Knight, S.C. Immunosuppressive effects via human intestinal dendritic cells of probiotic bacteria and steroids in the treatment of acute ulcerative colitis. Inflamm. Bowel Dis. 2010, 16, 1286–1298. [Google Scholar] [CrossRef]
- Tursi, A.; Brandimarte, G.; Papa, A.; Giglio, A.; Elisei, W.; Giorgetti, G.M.; Forti, G.; Morini, S.; Hassan, C.; Pistoia, M.A.; et al. Treatment of relapsing mild-to-moderate ulcerative colitis with the probiotic VSL#3 as adjunctive to a standard pharmaceutical treatment: A double-blind, randomized, placebo-controlled study. Am. J. Gastroenterol. 2010, 105, 2218–2227. [Google Scholar] [CrossRef] [PubMed]
- Fedorak, R.N.; Feagan, B.G.; Hotte, N.; Leddin, D.; Dieleman, L.A.; Petrunia, D.M.; Enns, R.; Bitton, A.; Chiba, N.; Paré, P.; et al. The probiotic VSL#3 has anti-inflammatory effects and could reduce endoscopic recurrence after surgery for crohn’s disease. Clin. Gastroenterol. Hepatol. 2015, 13, 928–935. [Google Scholar] [CrossRef] [PubMed]
- Tamaki, H.; Nakase, H.; Inoue, S.; Kawanami, C.; Itani, T.; Ohana, M.; Kusaka, T.; Uose, S.; Hisatsune, H.; Tojo, M.; et al. Efficacy of probiotic treatment with bifidobacterium longum 536 for induction of remission in active ulcerative colitis: A randomized, double-blinded, placebo-controlled multicenter trial. Dig. Endosc. 2015, 28, 67–74. [Google Scholar] [CrossRef]
- Kamarlı Altun, H.; Akal Yıldız, E.; Akın, M. Effects of synbiotic therapy in mild-to-moderately active ulcerative colitis: A randomized placebo-controlled study. Turk. J. Gastroenterol. 2019, 30, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Morales, A.; Pérez-Ayala, M.F.; Cruz-Martínez, M.; Arenas-Osuna, J.; Ramírez-Mendoza, P.; Ceniceros, R.A.; Mora-Cañas, E.M.; Cruz-Domínguez, P.; Saavedra-Salinas, M. Ángel Probiotics’ effectiveness on symptoms, histological features and feeding tolerance in ulcerative colitis. Rev. Med. Inst. Mex. Seguro Soc. 2019, 57, 9–14. Available online: http://revistamedica.imss.gob.mx/editorial/index.php/revista_medica/article/view/817 (accessed on 20 December 2019).
- Wildt, S.; Nordgaard, I.; Hansen, U.; Brockmann, E.; Rumessen, J.J. A randomised double-blind placebo-controlled trial with Lactobacillus acidophilus La-5 and Bifidobacterium animalis subsp. lactis BB-12 for maintenance of remission in ulcerative colitis. J. Crohns Colitis 2011, 5, 115–121. [Google Scholar] [CrossRef]
- Matsuoka, K.; Uemura, Y.; Kanai, T.; Kunisaki, R.; Suzuki, Y.; Yokoyama, K.; Yoshimura, N.; Hibi, T. Efficacy of bifidobacterium breve fermented milk in maintaining remission of ulcerative colitis. Dig. Dis. Sci. 2018, 63, 1910–1919. [Google Scholar] [CrossRef]
- Yoshimatsu, Y.; Yamada, A.; Furukawa, R.; Sono, K.; Osamura, A.; Nakamura, K.; Aoki, H.; Tsuda, Y.; Hosoe, N.; Takada, N.; et al. Effectiveness of probiotic therapy for the prevention of relapse in patients with inactive ulcerative colitis. World J. Gastroenterol. 2015, 21, 5985–5994. [Google Scholar] [CrossRef]
- Bourreille, A.; Cadiot, G.; Le Dréau, G.; Laharie, D.; Beaugerie, L.; Dupas, J.; Marteau, P.; Rampal, P.; Moyse, M.; Saleh, A.; et al. Saccharomyces boulardii does not prevent relapse of crohn’s disease. Clin. Gastroenterol. Hepatol. 2013, 11, 982–987. [Google Scholar] [CrossRef]
- Shadnoush, M.; Hosseini, R.S.; Khalilnezhad, A.; Navai, L.; Goudarzi, H.; Vaezjalali, M. Effectiveness of probiotic therapy for the prevention of relapse in patients with inactive ulcerative colitis. Korean J. Gastroenterol. 2015, 65, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Steed, H.; Macfarlane, G.T.; Blackett, K.L.; Bahrami, B.; Reynolds, N.; Walsh, S.V.; Cummings, J.H.; Macfarlane, S. Clinical trial: The microbiological and immunological effects of synbiotic consumption—A randomized double-blind placebo-controlled study in active Crohn’s disease. Aliment. Pharmacol. Ther. 2010, 32, 872–883. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, H.; Matsumoto, S.; Ohashi, Y.; Imaoka, A.; Setoyama, H.; Umesaki, Y.; Tanaka, R.; Otani, T. Beneficial effects of probiotic bifidobacterium and galacto-oligosaccharide in patients with ulcerative colitis: A randomized controlled study. Digestion 2011, 84, 128–133. [Google Scholar] [CrossRef]
- Petersen, A.M.; Mirsepasi, H.; Halkjær, S.I.; Mortensen, E.M.; Nordgaard-Lassen, I.; Krogfelt, K.A. Ciprofloxacin and probiotic Escherichia coli Nissle add-on treatment in active ulcerative colitis: A double-blind randomized placebo controlled clinical trial. J. Crohn’s Colitis 2014, 8, 1498–1505. [Google Scholar] [CrossRef] [PubMed]
- Shadnoush, M.; Hosseini, R.S.; Khalilnezhad, A.; Navai, L.; Goudarzi, H.; Vaezjalali, M. Effects of Probiotics on Gut Microbiota in Patients with Inflammatory Bowel Disease: A Double-blind, Placebo-controlled Clinical Trial. Korean J. Gastroenterol. 2015, 65, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Su, H.; Kang, Q.; Wang, H.; Yin, H.; Duan, L.; Liu, Y.; Fan, R. Effects of glucocorticoids combined with probiotics in treating Crohn’s disease on inflammatory factors and intestinal microflora. Exp. Ther. Med. 2018, 16, 2999–3003. [Google Scholar] [CrossRef] [PubMed]
- Derwa, Y.; Gracie, D.J.; Hamlin, P.J.; Ford, A.C. Systematic review with meta-analysis: The efficacy of probiotics in inflammatory bowel disease. Aliment. Pharmacol Ther. 2017, 46, 389–400. [Google Scholar] [CrossRef] [PubMed]
- Fujiya, M.; Ueno, N.; Kohgo, Y. Probiotic treatments for induction and maintenance of remission in inflammatory bowel diseases: A meta-analysis of randomized controlled trials. Clin. J. Gastroenterol. 2014, 7, 1–13. [Google Scholar] [CrossRef]
- Jia, K.; Tong, X.; Wang, R.; Song, X. The clinical effects of probiotics for inflammatory bowel disease: A meta-analysis. Medicine 2018, 97, e13792. [Google Scholar] [CrossRef] [PubMed]
- Ganji-Arjenaki, M.; Rafieian-Kopaei, M. Probiotics are a good choice in remission of inflammatory bowel diseases: A meta-analysis and systematic review. J. Cell. Physiol. 2018, 233, 2091–2103. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Zuo, Z.X.; Mao, A.P. Effect of probiotics on inducing remission and maintaining therapy in ulcerative colitis, Crohn’s disease, and pouchitis: Meta-analysis of randomized controlled trials. Inflamm. Bowel Dis. 2014, 20, 21–35. [Google Scholar] [CrossRef] [PubMed]
- Dong, J.; Teng, G.; Wei, T.; Gao, W.; Wang, H. Methodological quality assessment of meta-analyses and systematic reviews of probiotics in inflammatory bowel disease and pouchitis. PLoS ONE 2016, 11, e0168785. [Google Scholar] [CrossRef]
- Mardini, H.; Grigorian, A. Probiotic mix VSL#3 is effective adjunctive therapy for mild to moderately active ulcerative colitis: A meta-analysis. Inflamm. Bowel Dis. 2014, 20, 1562–1567. [Google Scholar] [CrossRef]
- Mimura, T.; Rizzello, F.; Helwig, U. Once daily high dose probiotic therapy (VSL#3) for maintaining remission in recurrent or refractory pouchitis. Gut 2004, 53, 108–114. [Google Scholar]
- Gionchetti, P.; Rizzello, F.; Helwig, U. Prophylaxis of pouchitis onset with probiotic therapy: A double-blind, placebo-controlled trial. Gastroenterology 2003, 124, 1202–1209. [Google Scholar] [CrossRef]
- Bjarnason, I.; Sission, G.; Hayee, B. A randomised, double-blind, placebo-controlled trial of a multi-strain probiotic in patients with asymptomatic ulcerative colitis and Crohn’s disease. Inflammopharmacology 2019, 27, 465–473. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Probiotic Compared with Placebo for Ulcerative Colitis | |||||
|---|---|---|---|---|---|
| Outcome | No. of Participants (Studies) Follow-Up | Certainty of the Evidence (GRADE) | Relative Effect (95% CI) | Absolute Anticipated Effects | |
| Placebo Risk | The Risk Difference with Probiotics | ||||
| Efficacy of probiotics in inducing remission in active UC | 759 (9 RCTs) | ⨁⨁⨁◯ MODERATE | RR 0.81 (0.72 to 0.91) | 683 × 1000 | 130 less to 1000 (191 less to 61) |
| Efficacy of probiotics in preventing relapse in quiescent UC | 284 (3 RCTs) | ⨁⨁⨁◯ MODERATE | RR 0.89 (0.68 to 1.15) | 438 × 1000 | 48 less to 1000 (140 less to 66) |
| Probiotic Compared with Placebo for Crohn’s Disease | |||||
|---|---|---|---|---|---|
| Outcome | No. of Participants (Studies) Follow-Up | Certainty of the Evidence (GRADE) | Relative Effect (95% CI) | Absolute Anticipated Effects | |
| Placebo Risk | The Risk Difference with Probiotics | ||||
| Efficacy of probiotics in inducing remission in active Crohn’s disease | 494 (5 RCTs) | ⨁⨁⨁◯ MODERATE | RR 0.90 (0.77 to 1.06) | 556 × 1000 | 56 less to 1000 (128 less to 33) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pabón-Carrasco, M.; Ramirez-Baena, L.; Vilar-Palomo, S.; Castro-Méndez, A.; Martos-García, R.; Rodríguez-Gallego, I. Probiotics as a Coadjuvant Factor in Active or Quiescent Inflammatory Bowel Disease of Adults—A Meta-Analytical Study. Nutrients 2020, 12, 2628. https://doi.org/10.3390/nu12092628
Pabón-Carrasco M, Ramirez-Baena L, Vilar-Palomo S, Castro-Méndez A, Martos-García R, Rodríguez-Gallego I. Probiotics as a Coadjuvant Factor in Active or Quiescent Inflammatory Bowel Disease of Adults—A Meta-Analytical Study. Nutrients. 2020; 12(9):2628. https://doi.org/10.3390/nu12092628
Chicago/Turabian StylePabón-Carrasco, Manuel, Lucia Ramirez-Baena, Samuel Vilar-Palomo, Aurora Castro-Méndez, Raúl Martos-García, and Isabel Rodríguez-Gallego. 2020. "Probiotics as a Coadjuvant Factor in Active or Quiescent Inflammatory Bowel Disease of Adults—A Meta-Analytical Study" Nutrients 12, no. 9: 2628. https://doi.org/10.3390/nu12092628
APA StylePabón-Carrasco, M., Ramirez-Baena, L., Vilar-Palomo, S., Castro-Méndez, A., Martos-García, R., & Rodríguez-Gallego, I. (2020). Probiotics as a Coadjuvant Factor in Active or Quiescent Inflammatory Bowel Disease of Adults—A Meta-Analytical Study. Nutrients, 12(9), 2628. https://doi.org/10.3390/nu12092628