Maternal Vitamin D Levels during Late Pregnancy and Risk of Allergic Diseases and Sensitization during the First Year of Life—A Birth Cohort Study

 ,
,  ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
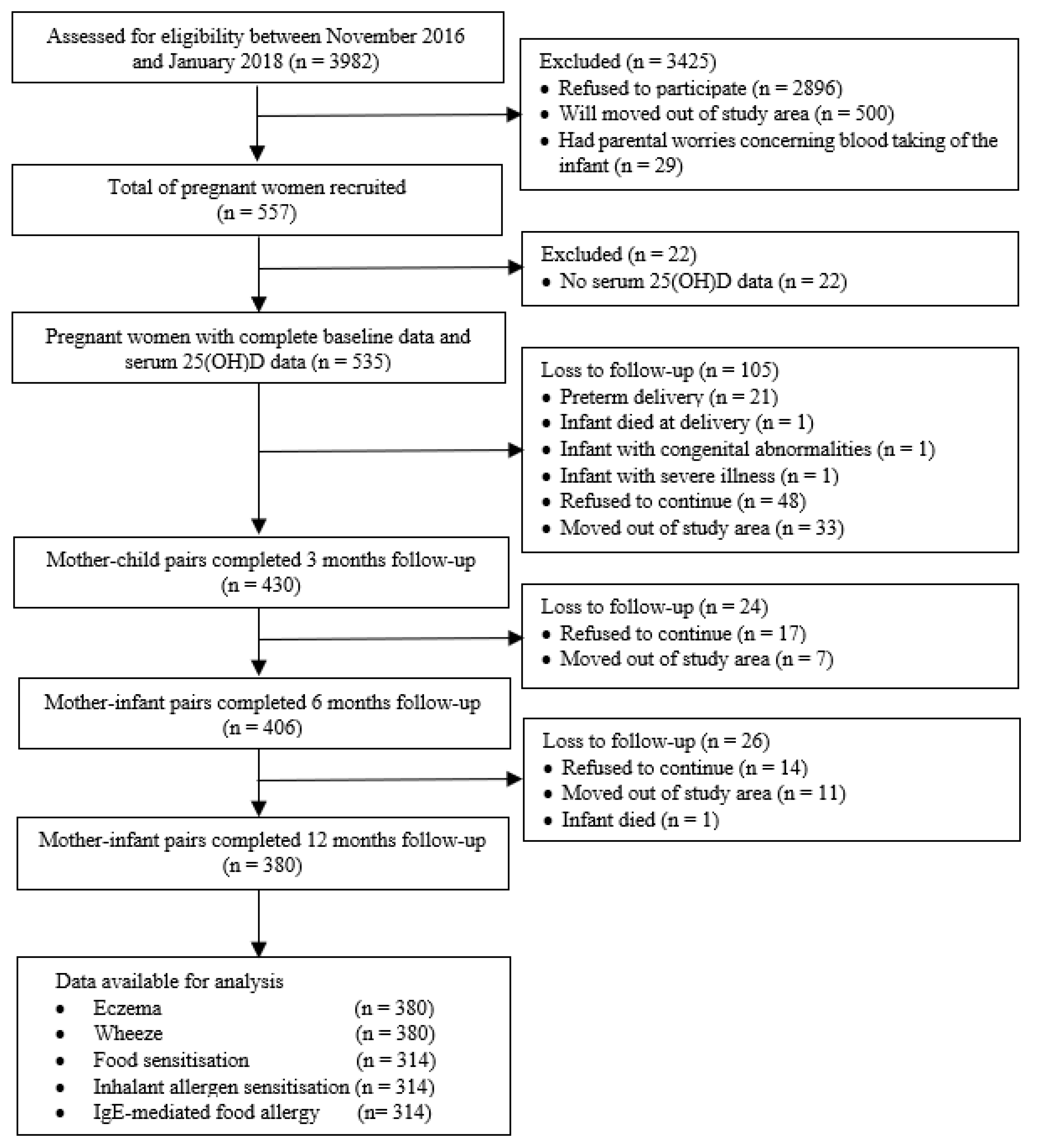
2.1. Study Design and Study Population
2.2. Serum 25-Hydroxyvitamin D [25(OH)D] Analysis
2.3. Allergic Sensitization
2.4. Allergic Outcomes
2.5. Covariates
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the Mother–Child Pairs
3.2. Allergic Outcomes in Infants
3.3. Associations between Maternal Vitamin D Levels and Allergic Diseases
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zheng, T.; Yu, J.; Oh, M.H.; Zhu, Z. The atopic march: Progression from atopic dermatitis to allergic rhinitis and asthma. J. Clin. Cell. Immunol. 2011, 3, 67–73. [Google Scholar] [CrossRef]
- Pawankar, R.; Canonica, G.W.; Holgate, S.T.; Lockey, R.F.; Blaiss, M.S. World Allergy Organisation (WAO) White Book on Allergy: Update 2013; World Allergy Organization: Milwaukee, WI, USA, 2013. [Google Scholar]
- Deckers, I.A.; McLean, S.; Linssen, S.; Mommers, M.; van Schayck, C.P.; Sheikh, A. Investigating international time trends in the incidence and prevalence of atopic eczema 1990-2010: A systematic review of epidemiological studies. PLoS ONE 2012, 7, e39803. [Google Scholar] [CrossRef]
- Wennergren, G. The prevalence of asthma has reached a plateau. Acta Paediatr. 2011, 100, 938–939. [Google Scholar] [CrossRef]
- Malik, G.; Tagiyeva, N.; Aucott, L.; McNeill, G.; Turner, S.W. Changing trends in asthma in 9–12 year olds between 1964 and 2009. Arch. Dis. Child. 2011, 96, 227–321. [Google Scholar] [CrossRef]
- Leung, A.S.Y.; Wong, G.W.K.; Tang, M.L.K. Food allergy in the developing world. J. Allergy Clin. Immunol. 2018, 141, 76–78. [Google Scholar] [CrossRef]
- Garcia-Larsen, V.; Ierodiakonou, D.; Jarrold, K.; Cunha, S.; Chivinge, J.; Robinson, Z.; Geoghegan, N.; Ruparelia, A.; Devani, P.; Trivella, M.; et al. Diet during pregnancy and infancy and risk of allergic or autoimmune disease: A systematic review and meta-analysis. PLoS Med. 2018, 15, e1002507. [Google Scholar] [CrossRef]
- Fiscaletti, M.; Stewart, P.; Munns, C.F. The importance of vitamin D in maternal and child health: A global perspective. Public Health Rev. 2017, 38, 19. [Google Scholar] [CrossRef]
- Mirzakhani, H.; Al-Garawi, A.; Weiss, S.T.; Litonjua, A.A. Vitamin D and the development of allergic disease: How important is it? Clin. Exp. Allergy 2015, 45, 114–125. [Google Scholar] [CrossRef]
- Chiu, C.Y.; Huang, S.Y.; Peng, Y.C.; Tsai, M.H.; Hua, M.C.; Yao, T.C.; Yeh, K.W.; Huang, J.L. Maternal vitamin D levels are inversely related to allergic sensitization and atopic diseases in early childhood. Pediatric Allergy Immunol. 2015, 26, 337–343. [Google Scholar] [CrossRef]
- Weisse, K.; Winkler, S.; Hirche, F.; Herberth, G.; Hinz, D.; Bauer, M.; Roder, S.; Rolle-Kampczyk, U.; von Bergen, M.; Olek, S.; et al. Maternal and newborn vitamin D status and its impact on food allergy development in the German LINA cohort study. Allergy 2013, 68, 220–228. [Google Scholar] [CrossRef]
- Baïz, N.; Dargent-Molina, P.; Wark, J.D.; Souberbielle, J.C.; Annesi-Maesano, I.; EDEN Mother-Child Cohort Study Group. Cord serum 25-hydroxyvitamin D and risk of early childhood transient wheezing and atopic dermatitis. J. Allergy Clin. Immunol. 2014, 133, 147–153. [Google Scholar] [CrossRef]
- Rueter, K.; Siafarikas, A.; Prescott, S.L.; Palmer, D.J. In utero and postnatal vitamin D exposure and allergy risk. Expert Opin. Drug Saf. 2014, 13, 1601–2611. [Google Scholar] [CrossRef]
- Gale, C.R.; Robinson, S.M.; Harvey, N.C.; Kassim Javaid, M.; Jiang, B.; Martyn, C.N.; Godfrey, K.M.; Cooper, C.; the Princess Anne Hospital Study Group. Maternal vitamin D status during pregnancy and child outcomes. Eur. J. Clin. Nutr. 2008, 62, 68–77. [Google Scholar] [CrossRef]
- Hennessy, Á.; Hourihane, J.O.; Malvisi, L.; Irvine, A.D.; Kenny, L.C.; Murray, D.M.; Kiely, M.E. Antenatal vitamin D exposure and childhood eczema, food allergy, asthma and allergic rhinitis at 2 and 5 years of age in the atopic disease-specific Cork BASELINE Birth Cohort Study. Allergy 2018, 73, 2182–2191. [Google Scholar] [CrossRef]
- Goldring, S.T.; Griffiths, C.J.; Martineau, A.R.; Robinson, S.; Yu, C.; Poulton, S.; Kirkby, J.C.; Stocks, J.; Hooper, R.; Shaheen, S.O.; et al. Prenatal vitamin D supplementation and child respiratory health: A randomised controlled trial. PLoS ONE 2013, 8, e66627. [Google Scholar] [CrossRef]
- Chawes, B.L.; Bønnelykke, K.; Stokholm, J.; Vissing, N.H.; Bjarnadóttir, E.; Schoos, A.M.M.; Wolsk, H.M.; Pedersen, T.M.; Vinding, R.K.; Thorsteinsdóttir, S.; et al. Effect of vitamin D3 supplementation during pregnancy on risk of persistent wheeze in the offspring: A randomized clinical trial. JAMA 2016, 315, 353–361. [Google Scholar] [CrossRef]
- Litonjua, A.A.; Carey, V.J.; Laranjo, N.; Harshfield, B.J.; McElrath, T.F.; O’Connor, G.T.; Sandel, M.; Iverson Jr, R.E.; Lee-Paritz, A.; Strunk, R.C.; et al. Effect of prenatal supplementation with vitamin D on asthma or recurrent wheezing in offspring by age 3 years: The VDAART randomized clinical trial. JAMA 2016, 315, 362–370. [Google Scholar] [CrossRef]
- Litonjua, A.A.; Carey, V.J.; Laranjo, N.; Stubbs, B.J.; Mirzakhani, H.; O’Connor, G.T.; Sandel, M.; Beigelman, A.; Bacharier, L.B.; Zeiger, R.S.; et al. Six-year follow-up of a trial of antenatal vitamin D for asthma reduction. N. Engl. J. Med. 2020, 382, 525–533. [Google Scholar] [CrossRef]
- Chawes, B.L.; Bønnelykke, K.; Jensen, P.F.; Schoos, A.M.; Heickendorff, L.; Bisgaard, H. Cord blood 25(OH)-vitamin D deficiency and childhood asthma, allergy and eczema: The COPSAC2000 birth cohort study. PLoS ONE 2014, 9, e99856. [Google Scholar] [CrossRef]
- Woon, F.C.; Chin, Y.S.; Intan Hakimah, I.; Batterham, M.; Amir Hamzah, A.L.; Gan, W.Y.; Geeta, A.; Siti Huzaifah, M.H.; Muliana, E.; Tan, M.L.; et al. Vitamin D deficiency during pregnancy and its associated factors among third trimester Malaysian pregnant women. PLoS ONE 2019, 14, e0216439. [Google Scholar] [CrossRef]
- Woon, F.C.; Chin, Y.S.; Intan Hakimah, I.; Chan, Y.M.; Batterham, M.; Amir Hamzah, A.L.; Gan, W.Y.; Geeta, A. Contribution of early nutrition on the development of malnutrition and allergic diseases in the first year of life: A study protocol for the Mother and Infant Cohort Study (MICOS). BMC Pediatrics 2018, 18, 233. [Google Scholar] [CrossRef]
- Freeman, J.; Sibley, P.; Parker, N.; Spears, R.; Wilson, K.; Levy, H. Standardization and certification of the ADVIA Centaur Vitamin D Total assay. Med. Res. Arch. 2017, 5, 1–19. [Google Scholar]
- Institute of Medicine. Dietary Reference Intakes for Calcium and Vitamin D; The National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Han, M.; Shin, S.; Park, H.; Park, K.U.; Park, M.H.; Song, E.Y. Comparison of three multiple allergen simultaneous tests: RIDA allergy screen, MAST optigen, and polycheck allergy. BioMed Res. Int. 2013, 340513. [Google Scholar] [CrossRef]
- Williams, H.C.; Burney, P.G.; Hay, R.J.; Archer, C.B.; Shipley, M.J.; Hunter, J.J.; Bingham, E.A.; Finlay, A.Y.; Pembroke, A.C.; Graham-Brown, R.A.; et al. The U.K. working Party’s diagnostic criteria for atopic dermatitis. I. Derivation of a minimum set of discriminators for atopic dermatitis. Br. J. Dermatol. 1994, 131, 383–396. [Google Scholar] [CrossRef]
- Asher, M.I.; Keil, U.; Anderson, H.R.; Beasley, R.; Crane, J.; Martinez, F.; Mitchell, E.A.; Pearce, N.; Sibbald, B.; Stewart, A.; et al. International Study of Asthma and Allergies in Childhood (ISAAC): Rationale and methods. Eur. Respir. J. 1995, 8, 483–491. [Google Scholar] [CrossRef]
- Nurmatov, U.; Nwaru, B.I.; Devereux, G.; Sheikh, A. Confounding and effect modification in studies of diet and childhood asthma and allergies. Allergy 2012, 67, 1041–1059. [Google Scholar] [CrossRef]
- Loo, E.X.L.; Sim, J.Z.T.; Loy, S.L.; Goh, A.; Chan, Y.H.; Tan, K.H.; Yap, F.; Gluckman, P.D.; Godfrey, K.M.; Van Bever, H.; et al. Associations between caesarean delivery and allergic outcomes: Results from the GUSTO study. Ann. Allergy Asthma Immunol. 2017, 118, 636–638. [Google Scholar] [CrossRef]
- Loo, E.X.; Sim, J.Z.; Goh, A.; Teoh, O.H.; Chan, Y.H.; Saw, S.M.; Kwek, K.; Gluckman, P.D.; Godfrey, K.M.; Van Bever, H.; et al. Predictors of allergen sensitization in Singapore children from birth to 3 years. Allergy Asthma Clin. Immunol. 2016, 12, 56. [Google Scholar] [CrossRef]
- Tham, E.H.; Lee, B.W.; Chan, Y.H.; Loo, E.X.L.; Toh, J.Y.; Goh, A.; Teoh, O.H.; Yap, F.; Tan, K.H.; Godfrey, K.M.; et al. Low food allergy prevalence despite delayed introduction of allergenic foods-data from the GUSTO cohort. J. Allergy Clin. Immunol. 2018, 6, 466–475. [Google Scholar] [CrossRef]
- Loo, E.X.L.; Tham, E.H.; Phang, K.W.; Goh, A.; Teoh, O.H.; Chong, Y.S.; Shek, L.P. Associations between maternal vitamin D levels during pregnancy and allergic outcomes in the offspring in the first 5 years of life. Pediatric Allergy Immunol. 2019, 30, 117–122. [Google Scholar] [CrossRef]
- Liu, X.; Wang, G.; Hong, X.; Wang, D.; Tsai, H.J.; Zhang, S.; Arguelles, L.; Kumar, R.; Wang, H.; Liu, R.; et al. Gene-vitamin D interactions on food sensitization: A prospective birth cohort study. Allergy 2011, 66, 1442–1448. [Google Scholar] [CrossRef] [PubMed]
- Blomberg, M.; Rifas-Shiman, S.L.; Camargo, C.A., Jr.; Gold, D.R.; Asgari, M.M.; Thyssen, J.P.; Litonjua, A.A.; Gillman, M.W.; Oken, E. Low maternal prenatal 25-hydroxyvitamin D blood levels are associated with childhood atopic dermatitis. J. Investig. Dermatol. 2017, 137, 1380–1384. [Google Scholar] [CrossRef] [PubMed]
- Gazibara, T.; Elbert, N.J.; den Dekker, H.T.; de Jongste, J.C.; Reiss, I.; McGrath, J.J.; Eyles, D.W.; Burne, T.H.; Tiemeier, H.; Jaddoe, V.W.V.; et al. Associations of maternal and fetal 25-hydroxyvitamin D levels with childhood eczema: The Generation R Study. Pediatric Allergy Immunol. 2016, 27, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Palmer, C.N.; Irvine, A.D.; Terron-Kwiatkowski, A.; Zhao, Y.; Liao, H.; Lee, S.P.; Goudie, D.R.; Sandilands, A.; Campbell, L.E.; Smith, F.J.D.; et al. Common loss-of-function variants of the epidermal barrier protein filaggrin are a major predisposing factor for atopic dermatitis. Nat. Genet. 2006, 38, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Weidinger, S.; O’Sullivan, M.; Illig, T.; Baurecht, H.; Depner, M.; Rodriguez, E.; Ruether, A.; Klopp, N.; Vogelberg, C.; Weiland, S.K.; et al. Filaggrin mutations, atopic eczema, hay fever, and asthma in children. J. Allergy Clin. Immunol. 2008, 121, 1203–1209. [Google Scholar] [CrossRef]
- Jones, A.P.; Palmer, D.; Zhang, G.; Prescott, S.L. Cord blood 25-hydroxyvitamin D3 and allergic disease during infancy. Pediatrics 2012, 130, e1128–e1135. [Google Scholar] [CrossRef]
- Pike, K.C.; Inskip, H.M.; Robinson, S.; Lucas, J.S.; Cooper, C.; Harvey, N.C.; Godfrey, K.M.; Roberts, G.; Southampton Women’s Survey Study Group. Maternal late-pregnancy serum 25-hydroxyvitamin D in relation to childhood wheeze and atopic outcomes. Thorax 2012, 67, 950–956. [Google Scholar] [CrossRef]
- Rothers, J.; Wright, A.L.; Stern, D.A.; Halonen, M.; Camargo, C.A., Jr. Cord blood 25-hydroxyvitamin D levels are associated with aeroallergen sensitization in children from Tucson, Arizona. J. Allergy Clin. Immunol. 2011, 128, 1093–1099. [Google Scholar] [CrossRef]
- Agudelo-Zapata, Y.; Maldonado-Acosta, L.M.; Sandoval-Alzate, H.F.; Poveda, N.E.; Garcés, M.F.; Cortés-Vásquez, J.A.; Linares-Vaca, A.F.; Mancera-Rodríguez, C.A.; Perea-Ariza, S.A.; Ramírez-Iriarte, K.Y.; et al. Serum 25hydroxyvitamin D levels throughout pregnancy: A longitudinal study in healthy and preeclamptic pregnant women. Endocr. Connect. 2018, 7, 698–707. [Google Scholar] [CrossRef]
- Thomas, S.D.C.; Fudge, A.N.; Whiting, M.; Coates, P.S. The correlation between third-trimester maternal and newborn-serum 25-hydroxy-vitamin D in a selected South Australian group of newborn samples. BMJ Open 2011, 1, e000236. [Google Scholar] [CrossRef]
- Nicolaidou, P.; Hatzistamatiou, Z.; Papadopoulou, A.; Kaleyias, J.; Floropoulou, E.; Lagona, E.; Tsagris, V.; Costalos, C.; Antsaklis, A. Low vitamin D status in mother-newborn pairs in Greece. Calcif. Tissue Int. 2006, 78, 337–342. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total | Maternal 25(OH)D Levels | |||||
|---|---|---|---|---|---|---|
| Characteristics | Included in Age 12 Month Analysis (n = 380) | Loss to Follow-Up (n = 155) | p-Value | Deficient < 30 nmol/L (n = 164) | Nondeficient ≥ 30 nmol/L (n = 216) | p-Value |
| Maternal 25(OH)D levels | ||||||
| Deficient (<30 nmol/L) | 164 (43.2) | 63 (40.6) | 0.594 | |||
| Nondeficient (≥30 nmol/L) | 216 (56.8) | 92 (59.4) | ||||
| Gestational age at blood withdrawal (weeks) | ||||||
| Median (IQR) | 32 (29, 36) | 31 (28–35) | 0.013 | |||
| Family characteristics | ||||||
| Maternal age (years) | 30.1 ± 4.2 | 29.6 ± 4.0 | 0.225 | 30.0 ± 4.0 | 30.2 ± 4.3 | 0.591 |
| Maternal ethnicity, Malay (%) | 350 (92.1) | 143 (92.3) | 0.952 | 161 (98.2) | 189 (87.5) | 0.001 |
| Maternal educational level, higher (%) | 312 (82.1) | 126 (81.3) | 0.824 | 129 (78.7) | 183 (84.7) | 0.127 |
| Monthly household income | ||||||
| Low (< RM 2300) | 52 (13.7) | 40 (25.8) | 0.003 | 26 (15.9) | 26 (12.0) | 0.062 |
| Moderate (RM 2300–5599) | 209 (55.0) | 72 (46.5) | 97 (59.1) | 112 (51.9) | ||
| High (≥RM 5600) | 119 (31.3) | 43 (27.7) | 41 (25.0) | 78 (36.1) | ||
| Maternal work status, working (%) | 267 (70.3) | 103 (66.5) | 0.387 | 118 (72.0) | 149 (69.0) | 0.530 |
| Parity, multiparous (%) | 226 (59.5) | 83 (53.5) | 0.208 | 101 (61.6) | 125 (57.9) | 0.465 |
| Family history of allergic disease, yes (%) | 257 (67.6) | 98 (63.2) | 0.328 | 109 (66.5) | 148 (68.5) | 0.672 |
| Maternal antibiotics use during pregnancy, yes (%) | 44 (11.6) | 6 (12.0) a | 0.930 | 37 (22.6) | 56 (25.9) | 0.450 |
| Pet keeping, yes (%) | 93 (24.5) | − | − | 13 (7.9) | 31 (14.4) | 0.053 |
| Infant characteristics | ||||||
| Gestational age at birth (weeks) | 38.9 ± 1.1 | 38.8 ± 1.0 a | 0.579 | 38.8 ± 1.1 | 38.9 ± 1.2 | 0.867 |
| Birth weight (kg) | 3.1 ± 0.4 | 3.1 ± 0.4 a | 0.845 | 3.1 ± 0.4 | 3.1 ± 0.4 | 0.620 |
| Mode of delivery, vaginal (%) | 278 (73.2) | 36 (72.0) a | 0.862 | 119 (72.6) | 159 (73.6) | 0.819 |
| Sex, male (%) | 190 (50.0) | 31 (62.0) a | 0.110 | 77 (47.0) | 113 (52.3) | 0.300 |
| Older siblings, yes (%) | 226 (59.5) | 83 (53.5) | 0.208 | 101 (61.6) | 125 (57.9) | 0.465 |
| Daycare attendance, yes (%) | 207 (54.5) | − | − | 82 (50.0) | 125 (57.9) | 0.127 |
| Antibiotic use, yes (%) | 224 (58.9) | − | − | 93 (56.7) | 131 (60.6) | 0.439 |
| Exclusive breastfeeding till 6 months (%) | 177 (46.6) | 13 (50.0) b | 0.735 | 74 (45.1) | 103 (47.7) | 0.620 |
| Allergic Diseases | N (%) |
|---|---|
| Eczema in the past 12 months (n = 380) | 105 (27.6) |
| Wheeze in the past 12 months (n = 380) | 23 (6.1) |
| Food sensitization at 12 months (n = 314) 1 | 86 (27.4) |
| Beef (n = 314) | 45 (14.3) |
| Peanut (n = 314) | 34 (10.8) |
| Egg white (n = 314) | 22 (7.0) |
| Egg yolk (n = 314) | 10 (3.2) |
| Soya (n = 314) | 14 (4.5) |
| Cow’s milk (n = 314) | 7 (2.2) |
| Shrimp (n = 314) | 6 (1.9) |
| Crab (n = 314) | 6 (1.9) |
| Clam (n = 314) | 4 (1.3) |
| Codfish (n = 314) | 4 (1.3) |
| Wheat (n = 314) | 4 (1.3) |
| Salmon (n = 314) | 3 (1.0) |
| Chocolate (n = 314) | 2 (0.6) |
| Rice (n = 314) | 2 (0.6) |
| Tuna (n = 314) | 2 (0.6) |
| Chicken (n = 314) | 1 (0.3) |
| Orange (n = 314) | 1 (0.3) |
| Inhalant allergen sensitization at 12 months (n = 314) 1 | 34 (10.8) |
| Dermatophagoides farinae (n = 314) | 20 (6.4) |
| Dermatophagoides pteronyssinus (n = 314) | 17 (5.4) |
| Blomia tropicalis (n = 314) | 13 (4.1) |
| Candida (n = 314) | 7 (2.2) |
| Cat dander (n = 314) | 7 (2.2) |
| House dust (n = 314) | 6 (1.9) |
| Dog dander (n = 314) | 4 (1.3) |
| Cockroach mix (n = 314) | 4 (1.3) |
| Penicillium (n = 314) | 3 (1.0) |
| Cladosporium (n = 314) | 2 (0.6) |
| Aspergillus (n = 314) | 1 (0.3) |
| Bermuda grass (n = 314) | 1 (0.3) |
| IgE-mediated food allergy at 12 months (n = 314) | 12 (3.8) |
| Eggs (n = 314) | 10 (3.2) |
| Cow’s milk (n = 314) | 3 (1.0) |
| Wheat (n = 314) | 2 (0.6) |
| Soy (n = 314) | 1 (0.3) |
| Allergic Outcomes | Crude | Adjusted 1 | Adjusted 2 | |||
|---|---|---|---|---|---|---|
| RR (95% CI) | p-Value | RR (95% CI) | p-Value | RR (95% CI) | p-Value | |
| Eczema (n = 380) | ||||||
| Nondeficient (≥30 nmol/L) | 1 | 1 | 1 | |||
| Deficient (<30 nmol/L) | 1.02 (0.77–1.35) | 0.884 | 1.04 (0.79–1.38) | 0.770 | 1.10 (0.83–1.46) | 0.495 |
| Wheeze (n = 380) | ||||||
| Nondeficient (≥30 nmol/L) | 1 | 1 | 1 | |||
| Deficient (<30 nmol/L) | 1.01 (0.48–2.13) | 0.973 | 1.04 (0.50–2.18) | 0.915 | 1.10 (0.61–2.00) | 0.755 |
| Food allergen sensitization (n = 314) | ||||||
| Nondeficient (≥30 nmol/L) | 1 | 1 | 1 | |||
| Deficient (<30 nmol/L) | 1.22 (0.85–1.75) | 0.282 | 1.08 (0.76–1.54) | 0.650 | 1.05 (0.75–1.48) | 0.782 |
| Inhalant allergen sensitization (n = 314) | ||||||
| Nondeficient (≥30 nmol/L) | 1 | 1 | 1 | |||
| Deficient (<30 nmol/L) | 0.58 (0.29–1.16) | 0.122 | 0.58 (0.29–1.15) | 0.121 | 0.59 (0.29–1.19) | 0.137 |
| IgE-mediated food allergy (n = 314) | ||||||
| Nondeficient (≥30 nmol/L) | 1 | 1 | 1 | |||
| Deficient (<30 nmol/L) | 0.54 (0.18–1.62) | 0.269 | 0.64 (0.30–1.40) | 0.268 | 0.68 (0.31–1.53) | 0.355 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Woon, F.C.; Chin, Y.S.; Ismail, I.H.; Abdul Latiff, A.H.; Batterham, M.; Chan, Y.M.; on behalf of the MICOS Research Group. Maternal Vitamin D Levels during Late Pregnancy and Risk of Allergic Diseases and Sensitization during the First Year of Life—A Birth Cohort Study. Nutrients 2020, 12, 2418. https://doi.org/10.3390/nu12082418
Woon FC, Chin YS, Ismail IH, Abdul Latiff AH, Batterham M, Chan YM, on behalf of the MICOS Research Group. Maternal Vitamin D Levels during Late Pregnancy and Risk of Allergic Diseases and Sensitization during the First Year of Life—A Birth Cohort Study. Nutrients. 2020; 12(8):2418. https://doi.org/10.3390/nu12082418
Chicago/Turabian StyleWoon, Fui Chee, Yit Siew Chin, Intan Hakimah Ismail, Amir Hamzah Abdul Latiff, Marijka Batterham, Yoke Mun Chan, and on behalf of the MICOS Research Group. 2020. "Maternal Vitamin D Levels during Late Pregnancy and Risk of Allergic Diseases and Sensitization during the First Year of Life—A Birth Cohort Study" Nutrients 12, no. 8: 2418. https://doi.org/10.3390/nu12082418
APA StyleWoon, F. C., Chin, Y. S., Ismail, I. H., Abdul Latiff, A. H., Batterham, M., Chan, Y. M., & on behalf of the MICOS Research Group. (2020). Maternal Vitamin D Levels during Late Pregnancy and Risk of Allergic Diseases and Sensitization during the First Year of Life—A Birth Cohort Study. Nutrients, 12(8), 2418. https://doi.org/10.3390/nu12082418