B12 as a Treatment for Peripheral Neuropathic Pain: A Systematic Review

 , , ,
, , ,  and
and 
Abstract
1. Introduction
2. Methods
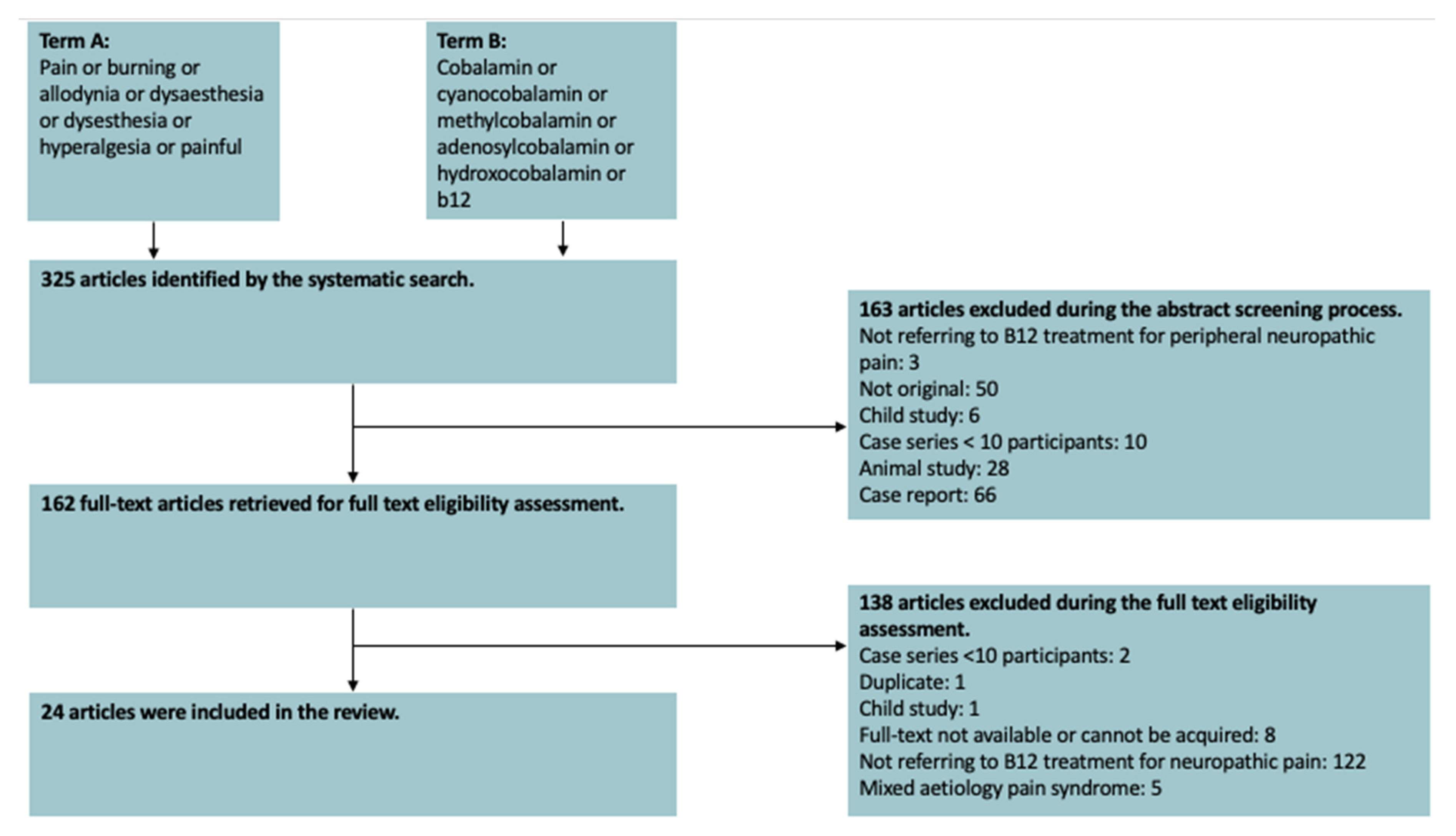
2.1. Literature Search Strategy
2.2. Inclusion and Exclusion Criteria
- The article discussed B12 as a treatment for peripheral neuropathic pain.
- The study was conducted using human subjects.
- The article was written in the English language.
- The study was original.
- Case reports.
- Case series with less than 10 participants.
- Animal studies.
- Articles using duplicate data or entirely duplicate papers.
- Articles which could not be obtained at least as an abstract.
- Child population studies.
- Articles describing mixed nociceptive-neuropathic pain syndromes.
2.3. Data Collection Process
2.4. Synthesis of Results
2.5. Assessment of Bias
2.6. Compliance with Ethical Guidelines
3. Results
3.1. Nature of Included Studies
3.2. Risk of Bias
3.3. Peripheral Polyneuropathy
3.3.1. Heterogeneous Aetiology Cohort
3.3.2. Diabetic Peripheral Neuropathy
3.3.3. Chemotherapy Induced Peripheral Neuropathy (CIPN)
3.3.4. Alcohol-Related Polyneuropathy
3.3.5. Overall Evidence for the Use of B12 for Painful Peripheral Polyneuropathy
3.4. Entrapment Neuropathy
Overall Evidence for the Use of B12 for Painful Entrapment Neuropathies
3.5. Glossopharyngeal Neuropathy
3.6. Post-Herpetic Neuralgia
Overall Evidence for the Use of B12 for Post-Herpetic Neuralgia
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- The IASP Subcommittee on Taxonomy. Pain terms a list with definitions and notes on usage. Recommended by the IASP subcommittee on taxonomy. Pain 1979, 6, 249. Available online: https://pubmed.ncbi.nlm.nih.gov/460932/ (accessed on 19 June 2020).
- Bouhassira, D. Neuropathic pain: Definition, assessment and epidemiology. Rev. Neurol. 2018, 175, 16–25. Available online: http://www.ncbi.nlm.nih.gov/pubmed/30385075 (accessed on 19 June 2020). [CrossRef]
- Brozou, V.; Vadalouca, A.; Zis, P. Pain in platin-induced neuropathies: A systematic review and meta-analysis. Pain Ther. 2018, 7, 105–119. Available online: http://link.springer.com/10.1007/s40122-017-0092-3 (accessed on 19 June 2020). [PubMed]
- Julian, T.; Glascow, N.; Syeed, R.; Zis, P. Alcohol-related peripheral neuropathy: A systematic review and meta-analysis. J. Neurol. 2019, 266, 2907–2919. [Google Scholar] [CrossRef] [PubMed]
- Zis, P.; Varrassi, G. Painful peripheral neuropathy and cancer. Pain Ther. 2017, 6, 115–116. Available online: http://www.ncbi.nlm.nih.gov/pubmed/28669084 (accessed on 19 June 2020). [CrossRef] [PubMed]
- Pellegrino, M.; Matteoli, M.; Bertolacci, L. Effect of colchicine and vinblastine on identified leech neurons. Comp. Biochem. Physiol. C 1985, 82, 353–356. Available online: http://www.ncbi.nlm.nih.gov/pubmed/2866908 (accessed on 19 June 2020). [CrossRef]
- Liampas, A.; Velidakis, N.; Georgiou, T.; Vadalouca, A.; Varrassi, G.; Hadjigeorgiou, G.M.; Tsivgoulis, G.; Zis, P. Prevalence and management challenges in central post-stroke neuropathic pain: A systematic review and meta-analysis. Adv. Ther. 2020, 37, 3278–3291. Available online: http://www.ncbi.nlm.nih.gov/pubmed/32451951 (accessed on 19 June 2020). [CrossRef] [PubMed]
- Murphy, D.R.; Hurwitz, E.L.; Gerrard, J.K.; Clary, R. Pain patterns and descriptions in patients with radicular pain: Does the pain necessarily follow a specific dermatome? Chiropr. Osteopat. 2009, 17, 9. Available online: http://www.ncbi.nlm.nih.gov/pubmed/19772560 (accessed on 19 June 2020). [CrossRef]
- Girach, A.; Julian, T.H.; Varrassi, G.; Paladini, A.; Vadalouka, A.; Zis, P. Quality of life in painful peripheral neuropathies: A systematic review. Pain Res. Manag. 2019, 23, 1–9. Available online: https://www.hindawi.com/journals/prm/2019/2091960/ (accessed on 19 June 2020). [CrossRef]
- Freynhagen, R.; Bennett, M.I. Diagnosis and management of neuropathic pain. BMJ 2009, 339, b3002. Available online: http://www.ncbi.nlm.nih.gov/pubmed/19675082 (accessed on 19 June 2020). [CrossRef]
- van Hecke, O.; Austin, S.K.; Khan, R.A.; Smith, B.H.; Torrance, N. Neuropathic pain in the general population: A systematic review of epidemiological studies. Pain 2014, 155, 654–662. Available online: http://www.ncbi.nlm.nih.gov/pubmed/24291734 (accessed on 19 June 2020). [CrossRef] [PubMed]
- Huang, Z.-F.; Lin, B.-Q.; Torsha, T.T.; Dilshad, S.; Yang, D.-S.; Xiao, J. Effect of mannitol plus vitamins B in the management of patients with piriformis syndrome. J. Back Musculoskelet. Rehabil. 2019, 32, 329–337. Available online: https://www.medra.org/servlet/aliasResolver?alias=iospress&doi=10.3233/BMR-170983 (accessed on 19 June 2020). [CrossRef]
- Xu, G.; Lv, Z.-W.; Feng, Y.; Tang, W.-Z.; Xu, G.X. A single-center randomized controlled trial of local methylcobalamin injection for subacute herpetic neuralgia. Pain Med. 2013, 14, 884–894. Available online: https://academic.oup.com/painmedicine/article-lookup/doi/10.1111/pme.12081 (accessed on 19 June 2020). [CrossRef] [PubMed]
- Kuwabara, S.; Nakazawa, R.; Azuma, N.; Suzuki, M.; Miyajima, K.; Fukutake, T.; Hattori, T. Intravenous methylcobalamin treatment for uremic and diabetic neuropathy in chronic hemodialysis patients. Intern. Med. 1999, 38, 472–475. Available online: http://joi.jlc.jst.go.jp/JST.Journalarchive/internalmedicine1992/38.472?from=CrossRef (accessed on 19 June 2020). [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. Available online: http://www.ncbi.nlm.nih.gov/pubmed/19621072 (accessed on 19 June 2020). [CrossRef]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control Clin. Trials 1996, 17, 1–12. Available online: http://www.ncbi.nlm.nih.gov/pubmed/8721797 (accessed on 19 June 2020). [CrossRef]
- Moher, D.; Pham, B.; Jones, A.; Cook, D.J.; Jadad, A.R.; Moher, M.; Tugwell, P.; Klassen, T.P. Does quality of reports of randomised trials affect estimates of intervention efficacy reported in meta-analyses? Lancet 1998, 352, 609–613. Available online: https://linkinghub.elsevier.com/retrieve/pii/S014067369801085X (accessed on 19 June 2020). [CrossRef]
- Manchikanti, L.; Falco, F.; Benyamin, R.; Kaye, A.; Mark, B.; Hirsch, J. A modified approach to grading of evidence. Pain Phys. 2014, 17, E319–E325. Available online: https://pubmed.ncbi.nlm.nih.gov/24850113/ (accessed on 19 June 2020).
- Sil, A.; Kumar, H.; Mondal, R.D.; Anand, S.S.; Ghosal, A.; Datta, A.; Sawant, S.V.; Kapatkar, V.; Kadhe, G.; Rao, S. A randomized, open labeled study comparing the serum levels of cobalamin after three doses of 500 mcg vs. a single dose methylcobalamin of 1500 mcg in patients with peripheral neuropathy. Korean J. Pain 2018, 31, 183. Available online: https://synapse.koreamed.org/DOIx.php?id=10.3344/kjp.2018.31.3.183 (accessed on 19 June 2020). [CrossRef]
- Negrão, L.; Almeida, P.; Alcino, S.; Duro, H.; Libório, T.; Melo Silva, U.; Figueira, R.; Gonçalves, S.; Neto Parra, L. Effect of the combination of uridine nucleotides, folic acid and vitamin B12 on the clinical expression of peripheral neuropathies. Pain Manag. 2014, 4, 191–196. Available online: https://www.futuremedicine.com/doi/10.2217/pmt.14.10 (accessed on 19 June 2020). [CrossRef]
- Prabhoo, R.; Panghate, A.; Dewda, R.P.; More, B.; Prabhoo, T.; Rana, R. Efficacy and tolerability of a fixed dose combination of methylcobalamin and pregabalin in the management of painful neuropathy. N. Am. J. Med. Sci. 2012, 4, 605. Available online: http://www.najms.org/text.asp?2012/4/11/605/103336 (accessed on 19 June 2020). [PubMed]
- Swami, O.; Dongre, Y. Sustained-release pregabalin with methylcobalamin in neuropathic pain: An Indian real-life experience. Int. J. Gen. Med. 2013, 6, 413–417. Available online: http://www.dovepress.com/sustained-release-pregabalin-with-methylcobalamin-in-neuropathic-pain--peer-reviewed-article-IJGM (accessed on 19 June 2020). [CrossRef] [PubMed][Green Version]
- Mimenza Alvarado, A.; Aguilar Navarro, S. Clinical trial assessing the efficacy of gabapentin plus b complex (b1/b12) versus pregabalin for treating painful diabetic neuropathy. J. Diabetes Res. 2016, 4078695. Available online: http://www.hindawi.com/journals/jdr/2016/4078695/ (accessed on 19 June 2020). [CrossRef] [PubMed]
- Vasudevan, D.; Naik, M.; Mukaddam, Q. Efficacy and safety of methylcobalamin, alpha lipoic acid and pregabalin combination versus pregabalin monotherapy in improving pain and nerve conduction velocity in type 2 diabetes associated impaired peripheral neuropathic condition. [MAINTAIN]: Results of a pilot study. Ann. Indian Acad. Neurol. 2014, 17, 19. Available online: http://www.annalsofian.org/text.asp?2014/17/1/19/128535 (accessed on 19 June 2020).
- Talaei, A.; Siavash, M.; Majidi, H.; Chehrei, A. Vitamin B 12 may be more effective than nortriptyline in improving painful diabetic neuropathy. Int. J. Food Sci. Nutr. 2009, 60 (Suppl. 5), 71–76. Available online: http://www.tandfonline.com/doi/full/10.1080/09637480802406153 (accessed on 19 June 2020). [CrossRef]
- Maladkar, M.; Rajadhyaksha, G.; Venkataswamy, N.; Hariharan, R.; Lohati, S. Efficacy, safety, and tolerability of Epalrestat compared to Methylcobalamine in patients with diabetic neuropathy. Int. J. Diabetes Dev. Ctries. 2009, 29, 28. Available online: http://www.ijddc.com/text.asp?2009/29/1/28/50712 (accessed on 19 June 2020). [CrossRef]
- Trippe, B.S.; Barrentine, L.W.; Curole, M.V.; Tipa, E. Nutritional management of patients with diabetic peripheral neuropathy with L-methylfolate-methylcobalamin-pyridoxal-5-phosphate: Results of a real-world patient experience trial. Curr. Med. Res. Opin. 2016, 32, 219–227. Available online: http://www.tandfonline.com/doi/full/10.1185/03007995.2015.1103215 (accessed on 19 June 2020). [CrossRef]
- Han, X.; Wang, L.; Shi, H.; Zheng, G.; He, J.; Wu, W.; Shi, J.; Wei, G.; Zheng, W.; Sun, J.; et al. Acupuncture combined with methylcobalamin for the treatment of chemotherapy-induced peripheral neuropathy in patients with multiple myeloma. BMC Cancer 2017, 17, 40. Available online: http://bmccancer.biomedcentral.com/articles/10.1186/s12885-016-3037-z (accessed on 19 June 2020). [CrossRef]
- Schloss, J.M.; Colosimo, M.; Airey, C.; Masci, P.; Linnane, A.W.; Vitetta, L. A randomised, placebo-controlled trial assessing the efficacy of an oral B group vitamin in preventing the development of chemotherapy-induced peripheral neuropathy (CIPN). Support Care Cancer 2017, 25, 195–204. Available online: http://link.springer.com/10.1007/s00520-016-3404-y (accessed on 19 June 2020). [CrossRef]
- Woelk, H.; Lehrl, S.; Bitsch, R.; Köpcke, W. Benfotiamine in treatment of alcoholic polyneuropathy: An 8-week randomized controlled study (BAP I Study). Alcohol Alcohol. 1998, 33, 631–638. Available online: http://www.ncbi.nlm.nih.gov/pubmed/9872352 (accessed on 19 June 2020). [CrossRef]
- Peters, T.J.; Kotowicz, J.; Nyka, W.; Kozubski, W.; Kuznetsov, V.; Vanderbist, F.; de Niet, S.; Marcereuil, D.; Coffiner, M. Treatment of alcoholic polyneuropathy with vitamin B complex: A randomised controlled trial. Alcohol Alcohol. 2006, 41, 636–642. Available online: https://academic.oup.com/alcalc/article/41/6/636/157556 (accessed on 19 June 2020). [CrossRef] [PubMed]
- Goldberg, H.; Mibielli, M.A.; Nunes, C.P.; Goldberg, S.W.; Buchman, L.; Mezitis, S.G.; Rzetelna, H.; Oliveira, L.; Geller, M.; Wajnsztajn, F. A double-blind, randomized, comparative study of the use of a combination of uridine triphosphate trisodium, cytidine monophosphate disodium, and hydroxocobalamin, versus isolated treatment with hydroxocobalamin, in patients presenting with compressive neuralgias. J. Pain Res. 2017, 10, 397–404. Available online: https://www.dovepress.com/a-double-blind-randomized-comparative-study-of-the-use-of-a-combinatio-peer-reviewed-article-JPR (accessed on 19 June 2020). [PubMed]
- Negrão, L.; Nunes, P. Uridine monophosphate, folic acid and vitamin B 12 in patients with symptomatic peripheral entrapment neuropathies. Pain Manag. 2016, 6, 25–29. Available online: https://www.futuremedicine.com/doi/10.2217/pmt.15.60 (accessed on 19 June 2020). [CrossRef] [PubMed]
- Singh, P.M.; Dehran, M.; Mohan, V.K.; Trikha, A.; Kaur, M. Analgesic efficacy and safety of medical therapy alone vs combined medical therapy and extraoral glossopharyngeal nerve block in glossopharyngeal neuralgia. Pain Med. 2013, 14, 93–102. Available online: https://academic.oup.com/painmedicine/article-lookup/doi/10.1111/pme.12001 (accessed on 19 June 2020). [CrossRef] [PubMed][Green Version]
- Xu, G.; Lv, Z.W.; Xu, G.; Tang, W.Z. Thiamine, cobalamin, locally injected alone or combination for herpetic itching: A single-center randomized Controlled Trial. Clin. J. Pain 2014, 30, 269–278. Available online: http://content.wkhealth.com/linkback/openurl?sid=WKPTLP:landingpage&an=00002508-201403000-00013 (accessed on 19 June 2020). [CrossRef]
- Xû, G.; Xú, G.; Feng, Y.; Tang, W.; Lv, Z. Transcutaneous electrical nerve stimulation in combination with cobalamin injection for postherpetic neuralgia: A single-center randomized controlled trial. Am. J. Phys. Med. Rehabil. 2014, 93, 287–298. Available online: http://content.wkhealth.com/linkback/openurl?sid=WKPTLP:landingpage&an=00002060-201404000-00003 (accessed on 19 June 2020). [CrossRef]
- Xǔ, G.; Xu, S.; Cheng, C.; Xú, G.; Tang, W.-Z.; Xu, J. Local administration of methylcobalamin and lidocaine for acute ophthalmic herpetic neuralgia: A single-center randomized controlled trial. Pain Pract. 2016, 16, 869–881. Available online: http://doi.wiley.com/10.1111/papr.12328 (accessed on 19 June 2020). [CrossRef]
- Xǔ, G.; Xu, S.; Tang, W.-Z.; Xú, G.; Cheng, C.; Xu, J. Local Injection of Methylcobalamin Combined with Lidocaine for Acute Herpetic Neuralgia. Pain Med. 2015, 17, 572–581. Available online: https://academic.oup.com/painmedicine/article-lookup/doi/10.1093/pm/pnv005 (accessed on 19 June 2020). [CrossRef]
- Bennett, M. The LANSS Pain Scale: The Leeds assessment of neuropathic symptoms and signs. Pain 2001, 92, 147–157. Available online: http://journals.lww.com/00006396-200105000-00017 (accessed on 19 June 2020). [CrossRef]
- Bouhassira, D.; Attal, N.; Alchaar, H.; Boureau, F.; Brochet, B.; Bruxelle, J.; Cunin, G.; Fermanian, J.; Ginies, P.; Grun-Overdyking, A.; et al. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). Pain 2005, 114, 29–36. Available online: http://journals.lww.com/00006396-200503000-00005 (accessed on 19 June 2020). [CrossRef]


{kind=link}
| Study [Reference] | Study Type | Cause of Pain | Intervention Assessed | Main Outcome | Limitations |
|---|---|---|---|---|---|
| Sil et al., 2018 [19] | RCT | Peripheral polyneuropathy | Intramuscular methylcobalamin of two different doses. | There was a significant reduction in pain measured by Leeds assessment of neuropathic signs and symptoms (LANSS) and Douleur Neuropathique 4 (DN4). | No placebo arm. Small population size. |
| Negrao et al., 2014 [20] | Single armed interventional | Peripheral polyneuropathy | Oral capsule containing uridine monophosphate, B12 and folic acid | There was a significant reduction in PainDETECT questionnaire (PDQ) and a reduction in analgesia use. | Open label study design. No placebo group. |
| Prabhoo et al., 2012 [21] | Post-marketing surveillance study | Peripheral polyneuropathy | Oral pregabalin plus methylcobalamin | Reduction in visual analogue scale (VAS) for pain and a reduction in concomitant analgesia use. | Observational study design. Short follow-up. |
| Dongre and Swami. 2013 [22] | Single armed interventional | Peripheral polyneuropathy | Oral pregabalin plus methylcobalamin | Significant reduction in pain measured by VAS and an improvement in sleep disturbance. | No placebo arm. Open label. Short follow-up. |
| Mimenza Alvarado and Navarro.2016 [23] | Non-randomised controlled study | Diabetic peripheral neuropathy | Oral gabapentin, thiamine and cyanocobalamin versus pregabalin alone. | Both groups showed a statistically significant improvement in pain measured by VAS. Both arms experienced less interrupted sleep. There was no difference between arms. | Did not include patients with severe neuropathy. Open label. Non-randomised. No placebo arm. |
| Vasudevan et al., 2014 [24] | RCT | Diabetic peripheral neuropathy | Oral pregabalin alone versus oral pregabalin plus alpha lipoic acid and methylcobalamin | There was a statistically significant reduction in pain measured on numerical rating scale (NRS) in both groups but there was not a difference between arms. | Open label. No placebo arm. Small population size. |
| Talaei et al., 2009 [25] | RCT | Diabetic peripheral neuropathy | Intramuscular B12 versus oral nortriptyline | Both groups showed significant reductions in pain measured by VAS. B12 was superior to nortriptyline. | Poor Jadad score. Open label. No placebo arm. |
| Maladkar et al., 2009 [26] | RCT | Diabetic peripheral neuropathy | Oral methylcobalamin versus epalrestat | There was a significant reduction in prevalence of pain in both groups. Epalrestat outperformed methylcobalamin. | No placebo. No validated quantifier of pain is used, only pain prevalence. |
| Trippe et al., 2016 [27] | Single armed interventional | Diabetic peripheral neuropathy | Oral L-methylfolate, methylcobalamin and pyridoxal-5-phosphate | There was a significant reduction in pain captured by VAS and NTSS6. There was an improved quality of life with a focus on pain. | No placebo group. Open label. Adverse events were not reported. |
| Kuwabara et al., 1999 [14] | Single armed interventional | Uraemic diabetic peripheral neuropathy | Intravenous B12 | Neuropathic pain grading score was not improved to a significant degree. | Small study size. No placebo arm. Open label. |
| Han et al., 2017 [28] | RCT | Chemotherapy induced peripheral neuropathy | Acupuncture plus intramuscular methylcobalamin initially then oral methylcobalamin versus methylcobalamin intramuscularly then orally alone. | Both treatment groups showed a significant reduction in pain measured by VAS. Although improvement was greater in the acupuncture group, it was not significant. | Open label. No placebo arm. Poor Jadad score. |
| Schloss et al., 2017 [29] | RCT | Chemotherapy induced peripheral neuropathy | Placebo versus oral capsule of thiamine, riboflavin, niacin, pantothenic acid, pyridoxine, folate (B9), cyanocobalamin, biotin, choline and inositol | The vitamin capsule did not decrease the incidence of pain compared with placebo. | This study was underpowered. Small study size. |
| Woelk et al., 1998 [30] | RCT | Alcohol-related polyneuropathy | Three treatment groups of capsules containing (A) B1, (B) B1, B6 and B12, (C) placebo | There was a significant improvement in pain assessed using McGill pain questionnaire in all three groups, with no differences between arms. | This is a high-quality study with few limitations. It does not assess B12 monotherapy. |
| Peters et al., 2006 [31] | RCT | Alcohol-related polyneuropathy | Three treatment arms: (A) B1, B2, B6, B12; (B) Regimen A plus folate; (C) Placebo | Groups A and B showed a greater reduction in pain measured by McGill pain questionnaire than with placebo. There is no additional benefit with addition of folate. | This is a high-quality study with few limitations. It does not assess B12 monotherapy. |
| Goldberg et al., 2017 [32] | RCT | Degenerative orthopaedic alteration with neural compression | Oral cytidine monophosphate disodium uridine triphosphate trisodium and hydroxocobalamin versus oral hydroxocobalamin alone. | Both arms had a statistically significant reduction in pain measured by VAS, but the improvement was greater in the arm inclusive of nucleosides. | Short follow-up. No placebo arm. |
| Negrao et al., 2016 [33] | Single armed interventional | Peripheral entrapment neuropathy | Oral uridine monophosphate, folic acid and vitamin B12 | There was a significant reduction in pain assessed by PDQ score and a reduction in concomitant use of analgesics. | No placebo arm. Open label. Did not include severe neuropathies. A very small dose of B12 is used. Small study size. |
| Huang et al., 2019 [12] | Single armed interventional | Piriformis syndrome | Intravenous mannitol plus oral B1, B2 and B12 | There was a significant reduction in pain evaluated by NRS and LRS. | Small study size. No placebo arm. Open label. |
| Singh et al., 2013 [34] | RCT | Glossopharyngeal neuropathy | Standard medical therapy (combination of oral methylcobalamin, tramadol and gabapentin) versus standard medical therapy plus extraoral glossopharyngeal nerve block | Pain measured by numerical pain scale and brief pain inventory significantly reduced in both groups. There were no significant differences between groups at the end of follow-up. | Poor Jadad score. No placebo group. Open label. |
| Xu et al., 2013 [13] | Post-herpetic neuralgia | RCT | Subcutaneous methylcobalamin versus subcutaneous lidocaine versus oral methylcobalamin | Pain intensity measured on NRS was improved in both methylcobalamin arms, but significantly more so in the subcutaneous methylcobalamin arm. The impact of pain upon quality of life was reduced in the subcutaneous methylcobalamin group but not in the other arms. | Small study size. No placebo arm. Short follow-up. |
| Xu et al., 2014 [35] | Post-herpetic neuralgia | RCT | Subcutaneous thiamine versus subcutaneous cobalamin versus a combination of the two and finally a group receiving subcutaneous lidocaine. | Pain measured by zoster brief pain inventory was significantly reduced only in the arms containing cobalamin. | Small study size. Short follow-up. No placebo group. |
| Xu et al., 2014 [36] | Post-herpetic neuralgia | RCT | Transcutaneous electrical nerve stimulation and cobalamin injection versus transcutaneous electrical nerve stimulation plus lidocaine injection. | No significant differences were identified between the two groups. Both groups showed a significantly improved quality of life and reduced pain measured by zoster brief pain inventory. | Small study size. No placebo arm. |
| Xu et al., 2016 [37] | Acute ophthalmic herpetic neuralgia | RCT | Lidocaine and methylcobalamin subcutaneously locally versus intramuscularly | Whilst the intramuscular group showed a statistically significant reduction in pain measured by NRS, this was short-lived and tapered off after 14 days. The subcutaneous locally delivered treatment showed a decrease in pain severity a year later. | No placebo arm. Small study size. |
| Xu et al., 2015 [38] | Truncal post-herpetic neuralgia | RCT | Lidocaine and methylcobalamin subcutaneously locally versus intramuscularly | There was a more significant reduction in pain measured by NRS and improvement in quality of life in those receiving local subcutaneous injection over the intramuscular group. | No placebo arm. |
| Study [Reference] | Randomisation | Blinding | Withdrawals | Jadad Score (/5) | Risk of Bias | ||
|---|---|---|---|---|---|---|---|
| Described | Appropriate Method | Described | Appropriate Method | Accounted for | |||
| Sil A, 2018 [19] | * | * | * | 3 | Low | ||
| Goldberg H, 2017 [32] | * | * | * | * | 4 | Low | |
| Han X, 2017 [28] | * | * | 2 | High | |||
| Schloss JM, 2017 [29] | * | * | * | * | * | 5 | Low |
| Mimenza Alvarado A, 2016 [23] | * | * | * | * | 4 | Low | |
| Xu G, 2015 [38] | * | * | * | * | * | 5 | Low |
| Xu G, 2016 [37] | * | * | * | * | * | 5 | Low |
| Vasudevan D, 2014 [24] | * | * | * | 3 | Low | ||
| Xu G, 2014 [36] | * | * | * | * | * | 5 | Low |
| Xu G, 2014 [35] | * | * | * | * | * | 5 | Low |
| Xu G, 2013 [13] | * | * | * | * | * | 5 | Low |
| Singh PM, 2013 [34] | * | * | 2 | High | |||
| Talaei A, 2009 [25] | * | * | 2 | High | |||
| Maladkar M, 2009 [26] | * | * | * | 3 | Low | ||
| Peters TJ, 2006 [31] | * | * | * | * | * | 5 | Low |
| Woelk H, 1998 [30] | * | * | * | * | 4 | Low | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Julian, T.; Syeed, R.; Glascow, N.; Angelopoulou, E.; Zis, P. B12 as a Treatment for Peripheral Neuropathic Pain: A Systematic Review. Nutrients 2020, 12, 2221. https://doi.org/10.3390/nu12082221
Julian T, Syeed R, Glascow N, Angelopoulou E, Zis P. B12 as a Treatment for Peripheral Neuropathic Pain: A Systematic Review. Nutrients. 2020; 12(8):2221. https://doi.org/10.3390/nu12082221
Chicago/Turabian StyleJulian, Thomas, Rubiya Syeed, Nicholas Glascow, Efthalia Angelopoulou, and Panagiotis Zis. 2020. "B12 as a Treatment for Peripheral Neuropathic Pain: A Systematic Review" Nutrients 12, no. 8: 2221. https://doi.org/10.3390/nu12082221
APA StyleJulian, T., Syeed, R., Glascow, N., Angelopoulou, E., & Zis, P. (2020). B12 as a Treatment for Peripheral Neuropathic Pain: A Systematic Review. Nutrients, 12(8), 2221. https://doi.org/10.3390/nu12082221