Effect of Magnesium Supplementation on Circulating Biomarkers of Cardiovascular Disease

 , , and
, , and
Abstract
1. Introduction
2. Methods
2.1. Study Population
2.2. Intervention
2.3. Blood Biomarker Analysis
2.4. Proteomic Measurements
2.5. Other Covariates
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Del Gobbo, L.C.; Imamura, F.; Wu, J.H.; De Oliveira Otto, M.C.; Chiuve, S.E.; Mozaffarian, D. Circulating and dietary magnesium and risk of cardiovascular disease: A systematic review and meta-analysis of prospective studies. Am. J. Clin. Nutr. 2013, 98, 160–173. [Google Scholar] [CrossRef]
- Misialek, J.R.; Lopez, F.L.; Lutsey, P.L.; Huxley, R.R.; Peacock, J.M.; Chen, L.Y.; Soliman, E.Z.; Agarwal, S.K.; Alonso, A. Serum and dietary magnesium and incidence of atrial fibrillation in whites and in African Americans--Atherosclerosis Risk in Communities (ARIC) Study. Circ. J. 2013, 77, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Burgess, S.; Michaëlsson, K. Serum magnesium levels and risk of coronary artery disease: Medelian randomisation study. BMC Med. 2018, 16, 68. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Drca, N.; Michaëlsson, K. Serum magnesium and calcium levels and risk of atrial fibrillation. Circ. Genom Precis Med. 2019, 12, e002349. [Google Scholar] [CrossRef] [PubMed]
- Arsenault, K.A.; Yusuf, A.M.; Crystal, E.; Healey, J.S.; Morillo, C.A.; Nair, G.M.; Whitlock, R.P. Interventions for preventing post-operative atrial fibrillation in patients undergoing heart surgery. Cochrane Database Syst. Rev. 2013, CD003611. [Google Scholar] [CrossRef] [PubMed]
- Veronese, N.; Demurtas, J.; Pesolillo, G.; Celotto, S.; Barnini, T.; Calusi, G.; Caruso, M.G.; Notarnicola, M.; Reddavide, R.; Stubbs, R.; et al. Magnesium and health outcomes: An umbrella review of systematic reviews and meta-analyses of observational and intervention studies. Eur. J. Nutr. 2020, 59, 263–272. [Google Scholar] [CrossRef]
- Nielsen, F.H. Magnesium deficiency and increased inflammation: Current perspectives. J. Inflamm. Res. 2018, 11, 25–34. [Google Scholar] [CrossRef]
- Morais, J.B.; Severo, J.S.; Santos, L.R.; De Sousa Melo, S.R.; De Oliveira Santos, R.; De Oliveira, A.R.; Cruz, K.J.; Do Nascimento Marreiro, D. Role of magnesium in oxidative stress in individuals with obesity. Biol. Trace Elem. Res. 2017, 176, 20–26. [Google Scholar] [CrossRef]
- Barbagallo, M.; Dominguez, L.J.; Galioto, A.; Pineo, A.; Belvedere, M. Oral magnesium supplementation improves vascular function in elderly diabetic patients. Magnes. Res. 2010, 23, 131–137. [Google Scholar]
- Lindsey, M.L.; Mayr, M.; Gomes, A.V.; Delles, C.; Arrell, D.K.; Murphy, A.M.; Lange, R.A.; Costello, C.E.; Jin, Y.F.; Laskowitz, D.T.; et al. Transformative impact of proteomics on cardiovascular health and disease: A scientific statement from the American Heart Association. Circulation 2015, 132, 852–872. [Google Scholar] [CrossRef]
- Chacko, S.A.; Sul, J.; Song, Y.; Li, X.; LeBlanc, J.; You, Y.; Butch, A.; Liu, S. Magnesium supplementation, metabolic and inflammatory markers, and global genomic and proteomic profiling: A randomized, double-blind, controlled, crossover trial in overweight individuals. Am. J. Clin. Nutr. 2011, 93, 463–473. [Google Scholar] [CrossRef] [PubMed]
- Lutsey, P.L.; Chen, L.Y.; Eaton, A.; Jaeb, M.; Rudser, K.D.; Neaton, J.D.; Alonso, A. A pilot randomized trial of oral magnesium supplementation on supraventricular arrhythmias. Nutrients 2018, 10, 884. [Google Scholar] [CrossRef] [PubMed]
- Assarsson, E.; Lundberg, M.; Holmquist, G.; Björkesten, J.; Bucht Thorsen, S.; Ekman, D.; Eriksson, A.; Rennel Dickens, E.; Ohlsson, S.; Edfeldt, G.; et al. Homogenous 96-plex PEA immunoassay exhibiting high sensitivity, specificity, and excellent scalability. PLoS ONE 2014, 9, e95192. [Google Scholar] [CrossRef] [PubMed]
- Holm, S. A simple sequentially rejective multiple test procedure. Scand. J. Statist 1979, 6, 65–70. [Google Scholar]
- Salaminia, S.; Sayehmiri, F.; Angha, P.; Sayehmiri, K.; Motedayen, M. Evaluating the effect of magnesium supplementation and cardiac arrhythmias after acture coronary syndrome: A systematic review and meta-analysis. BMC Cardiovasc. Disord 2018, 18, 129. [Google Scholar] [CrossRef]
- Joris, P.J.; Plat, J.; Bakker, S.J.; Mensink, R.P. Effects of long-term magnesium supplementation on endothelial function and cardiometabolic risk markers: A randomized controlled trial in overweight/obese adults. Sci. Rep. 2017, 7, 106. [Google Scholar] [CrossRef]
- Ordway, G.A.; Garry, D.J. Myoglobin: An essential hemoprotein in striated muscle. J. Exp. Biol. 2004, 207, 3441–3446. [Google Scholar] [CrossRef]
- Schneider, P.; MacKay, F.; Steiner, V.; Hofmann, K.; Bodmer, J.L.; Holler, N.; Ambrose, C.; Lawton, P.; Bixler, S.; Acha-Orbea, H.; et al. BAFF, a novel ligand of the tumor necrosis family, stimulates B cell growth. J. Exp. Med. 1999, 189, 1747–1756. [Google Scholar] [CrossRef]
- Schmitz, J.; Owyang, A.; Oldham, E.; Song, Y.; Murphy, E.; McClanahan, T.K.; Zurawski, G.; Moshrefi, M.; Qin, J.; Li, X.; et al. IL-33, an interleukin-1-like cytokine that signals via the IL-1 receptor-related protein ST2 and induces T helper type 2-associated cytokines. Immunity 2005, 23, 479–490. [Google Scholar] [CrossRef]
- Tominaga, K.; Yoshimoto, T.; Torigoe, K.; Kurimoto, M.; Matsui, K.; Hada, T.; Okamura, H.; Nakanishi, K. IL-12 synergizes with IL-18 or IL-1beta for IFN-gamma production from human T cells. Int. Immunol. 2000, 12, 151–160. [Google Scholar] [CrossRef]
- Halleen, J.M.; Ylipahkala, H.; Alatalo, S.L.; Janckila, A.J.; Heikkinen, J.E.; Suominen, H.; Cheng, S.; Väänänen, H.K. Serum tartrate-resistant acid phosphatase 5b, but not 5a, correlates with other markers of bone turnover and bone mineral density. Calcif. Tissue Int. 2002, 71, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Pascual-Figal, D.A.; Januzzi, J.L. The biology of ST2: The International ST2 Consensus Panel. Am. J. Cardiol. 2015, 115, 3B–7B. [Google Scholar] [CrossRef] [PubMed]
- Seshacharyulu, P.; Ponnusamy, M.P.; Haridas, D.; Jain, M.; Ganti, A.K.; Batra, S.K. Targeting the EGFR signaling pathway in cancer therapy. Expert. Opin. Ther. Targets 2012, 16, 15–31. [Google Scholar] [CrossRef] [PubMed]
- Steinbacher, T.; Kummer, D.; Ebnet, K. Junctional adhesion molecule-A: Functional diversity through molecular promiscuity. Cell Mol. Life Sci. 2018, 75, 1393–1409. [Google Scholar] [CrossRef] [PubMed]
- Lertkiatmongkol, P.; Liao, D.; Mei, H.; Hu, Y.; Newman, P.J. Endothelial functions of platelet/endothelial cell adhesion molecule-1 (CD31). Curr. Opin. Hematol. 2016, 23, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Précourt, L.P.; Amre, D.; Denis, M.C.; Lavoie, J.C.; Delvin, E.; Seidman, E.; Levy, E. The three-gene paraoxonase family: Physiologic roles, actions and regulation. Atherosclerosis 2011, 214. [Google Scholar] [CrossRef]
- Zhang, X.; Del Gobbo, L.C.; Hruby, A.; Rosanoff, A.; He, K.; Dai, Q.; Costello, R.B.; Zhang, W.; Song, Y. The circulating concentration and 24-h urine excretion of magnesium dose- and time-dependently respond to oral magnesium supplementation in a meta-analysis of randomized controlled trials. J. Nutr. 2016, 146, 595–602. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Magnesium (400 mg Daily) | Placebo | |
|---|---|---|
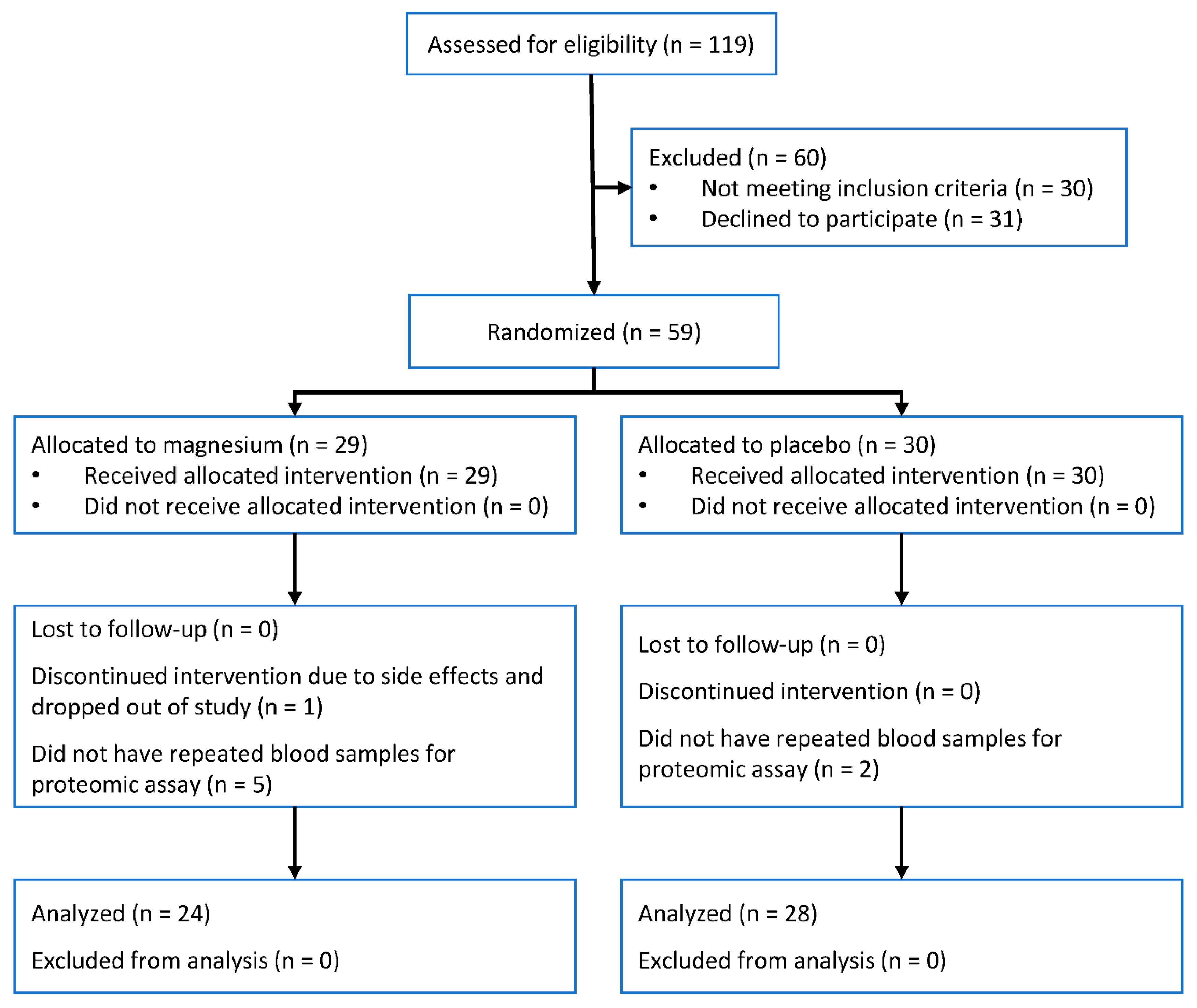
| N | 24 | 28 |
| Age, years | 62 (5) | 62 (6) |
| Women, n (%) | 21 (88) | 17 (61) |
| Non-white, n (%) | 2 (8) | 1 (4) |
| Body mass index, kg/m2 | 28.3 (5.1) | 27.8 (4.2) |
| Systolic blood pressure, mmHg | 118 (15) | 119 (17) |
| Diastolic blood pressure, mmHg | 73 (8) | 71 (8) |
| Serum magnesium, mmol/L | 0.86 (0.06) | 0.84 (0.05) |
| Hypomagnesemia, n (%) * | 2 (8.3) | 2 (7.1) |
| Protein | Difference in Change in Protein (NPX Units) | 95% CI | p-Value | |
|---|---|---|---|---|
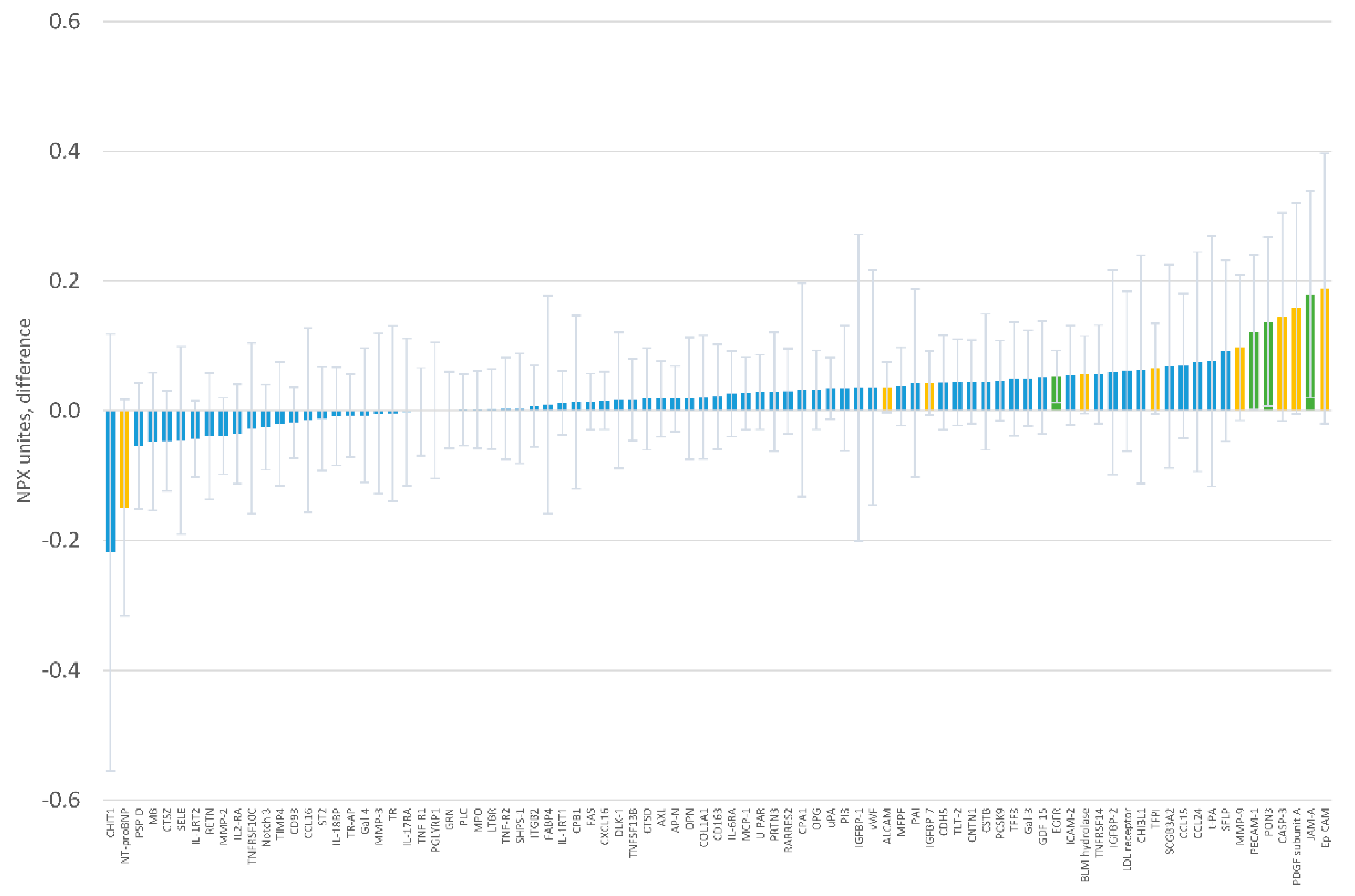
| MB | Myoglobin | −0.319 | −0.550, −0.088 | 0.008 |
| TR-AP | Tartrate-resistant acid phosphatase type 5 | −0.187 | −0.328, −0.045 | 0.011 |
| TNFSF13B | Tumor necrosis factor ligand superfamily member 13B | −0.181 | −0.332, −0.031 | 0.019 |
| ST2 | ST2 protein | −0.198 | −0.363, −0.032 | 0.020 |
| IL-1RT1 | Interleukin-1 receptor type 1 | −0.144 | −0.273, −0.015 | 0.029 |
| Protein | Difference in Protein Levels (NPX Units) | 95% CI | p-Value | |
|---|---|---|---|---|
| EGFR | Epidermal growth factor receptor | 0.053 | 0.013, 0.093 | 0.011 |
| JAM-A | Junctional adhesion molecule A | 0.180 | 0.020, 0.339 | 0.028 |
| PON3 | Paraoxonase 3 | 0.137 | 0.039, 0.007 | 0.039 |
| PECAM-1 | Platelet endothelial cell adhesion molecule | 0.121 | 0.002, 0.241 | 0.046 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alonso, A.; Chen, L.Y.; Rudser, K.D.; Norby, F.L.; Rooney, M.R.; Lutsey, P.L. Effect of Magnesium Supplementation on Circulating Biomarkers of Cardiovascular Disease. Nutrients 2020, 12, 1697. https://doi.org/10.3390/nu12061697
Alonso A, Chen LY, Rudser KD, Norby FL, Rooney MR, Lutsey PL. Effect of Magnesium Supplementation on Circulating Biomarkers of Cardiovascular Disease. Nutrients. 2020; 12(6):1697. https://doi.org/10.3390/nu12061697
Chicago/Turabian StyleAlonso, Alvaro, Lin Y. Chen, Kyle D. Rudser, Faye L. Norby, Mary R. Rooney, and Pamela L. Lutsey. 2020. "Effect of Magnesium Supplementation on Circulating Biomarkers of Cardiovascular Disease" Nutrients 12, no. 6: 1697. https://doi.org/10.3390/nu12061697
APA StyleAlonso, A., Chen, L. Y., Rudser, K. D., Norby, F. L., Rooney, M. R., & Lutsey, P. L. (2020). Effect of Magnesium Supplementation on Circulating Biomarkers of Cardiovascular Disease. Nutrients, 12(6), 1697. https://doi.org/10.3390/nu12061697