Global Vegetable Intake and Supply Compared to Recommendations: A Systematic Review


Abstract
1. Introduction
2. Materials and Methods
2.1. Definitions
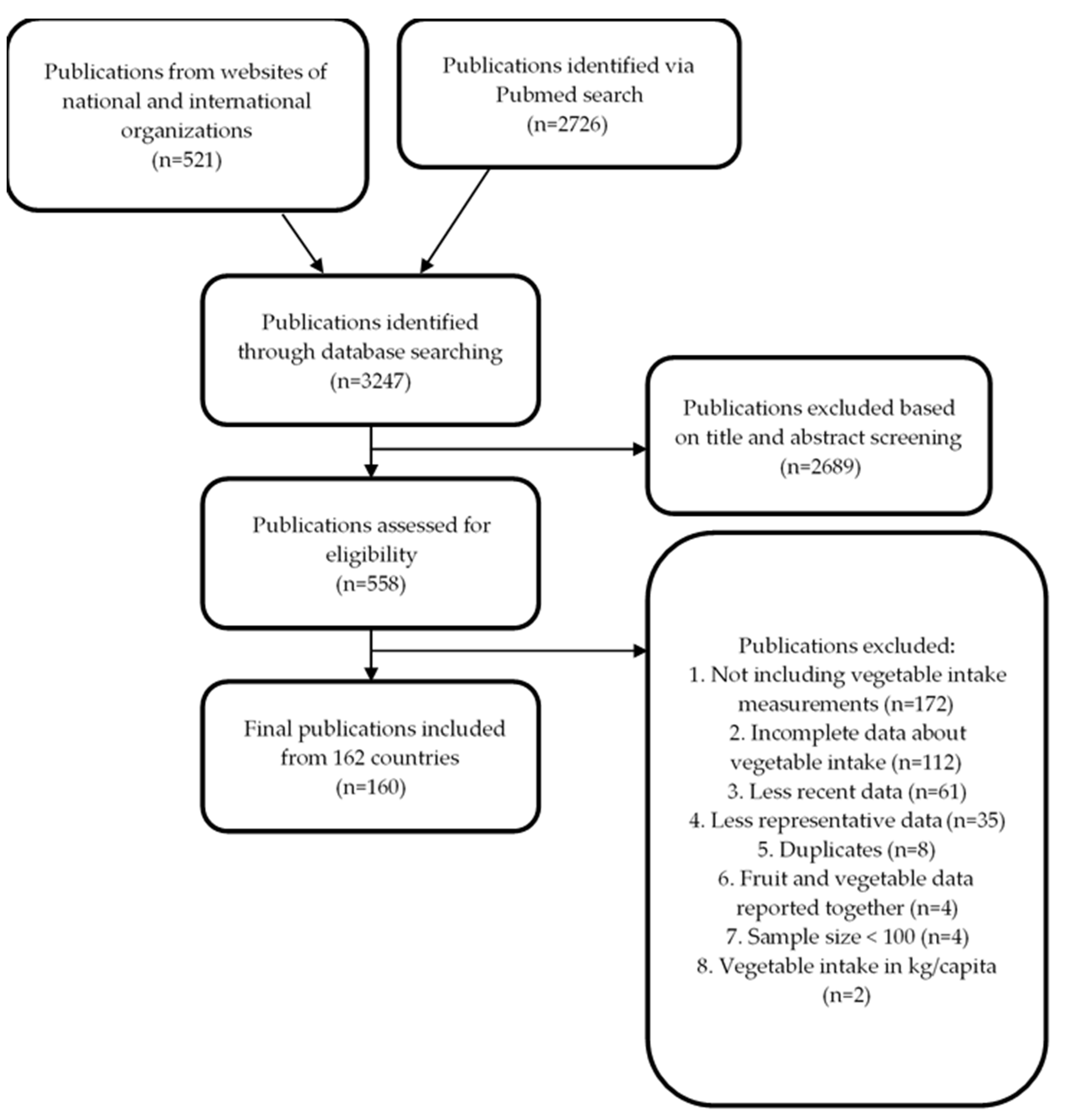
2.2. Search Strategy
- Data from adult populations aged ≥18 years.
- Free living, healthy population. Disabled people, populations with specific diseases or with special dietary needs (pregnant and lactating women, athletes) were excluded.
- National or population-based surveys/studies. In case these were not available, baseline data or data from a control group, belonging to a healthy general population, of controlled trials were included.
- Surveys/Studies conducted from the year 2000 onwards and published until June 2019.
- Sample size of participants ≥100.
- Surveys/Studies in which vegetable intake in adults at individual level were included (therefore, studies estimating vegetable intake per capita or at household level were excluded)
2.3. Data Extraction
2.4. Quality Assessment of the Data
2.5. Data Analysis
- For the conversion of medians and ranges into means [61]:
- 2.
- For conversion of median and 25th and 75th percentiles into means [62]:
- 3.
- For mean and SE into 95% CIs [63]:
- 4.
- For mean and SD into 95% CIs [63]:
- 5.
- For 25th and 75th percentiles into 95% CI [62], first a conversion was made into SD and then into 95% CI following the equation above (4):
- 6.
- For 5th and 95th into 95% CI [62], first a conversion was made into SD and then into 95% CI following the equation above (4):
2.6. Vegetable Supply Data
3. Results
3.1. Data Availability, Representativeness and Dietary Assessment Methodology
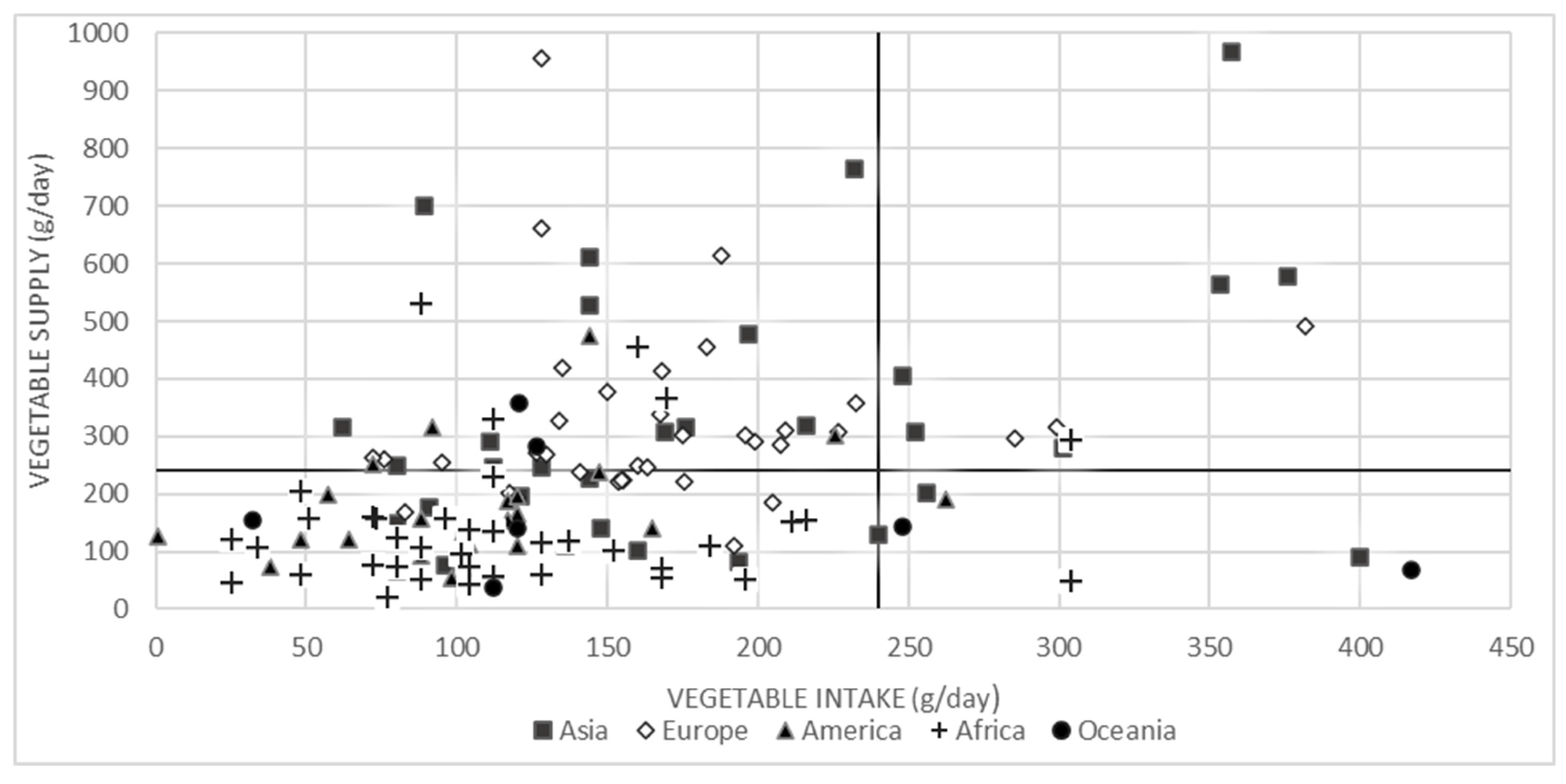
3.2. Global Vegetable Intake and Supply
3.3. Asia
3.4. Europe
3.5. America
3.6. Oceania
3.7. Africa
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Darfour-Oduro, S.A.; Buchner, D.M.; Andrade, J.E.; Grigsby-Toussaint, D.S. A comparative study of fruit and vegetable consumption and physical activity among adolescents in 49 Low-and-Middle-Income Countries. Sci. Rep. 2018, 8, 1623. [Google Scholar] [CrossRef]
- Diet, nutrition and the prevention of chronic diseases. World Health Organ. Tech. Rep. Ser. 2003, 916. i–viii, 1–149, backcover.
- Riordan, F.; Ryan, K.; Perry, I.J.; Schulze, M.B.; Andersen, L.F.; Geelen, A.; Van’t Veer, P.; Eussen, S.; Dagnelie, P.; Wijckmans-Duysens, N.; et al. A systematic review of methods to assess intake of fruits and vegetables among healthy European adults and children: A DEDIPAC (DEterminants of DIet and Physical Activity) study. Public Health Nutr. 2017, 20, 417–448. [Google Scholar] [CrossRef] [PubMed]
- Riley, L.; Guthold, R.; Cowan, M.; Savin, S.; Bhatti, L.; Armstrong, T.; Bonita, R. The World Health Organization STEPwise Approach to Noncommunicable Disease Risk-Factor Surveillance: Methods, Challenges, and Opportunities. Am. J. Public Health 2016, 106, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Health Organization, W. Global Health Risks. Mortality and Burden Och Disease Attributable to Selected Major Risks; Health Organization: Geneva, Switzerland, 2009; pp. 1–63. [Google Scholar]
- Dauchet, L.; Amouyel, P.; Hercberg, S.; Dallongeville, J. Fruit and vegetable consumption and risk of coronary heart disease: A meta-analysis of cohort studies. J. Nutr. 2006, 136, 2588–2593. [Google Scholar] [CrossRef]
- Joshipura, K.J.; Hu, F.B.; Manson, J.E.; Stampfer, M.J.; Rimm, E.B.; Speizer, F.E.; Colditz, G.; Ascherio, A.; Rosner, B.; Spiegelman, D.; et al. The effect of fruit and vegetable intake on risk for coronary heart disease. Ann. Intern. Med. 2001, 134, 1106–1114. [Google Scholar] [CrossRef]
- Oyebode, O.; Gordon-Dseagu, V.; Walker, A.; Mindell, J.S. Fruit and vegetable consumption and all-cause, cancer and CVD mortality: Analysis of Health Survey for England data. J. Epidemiol. Commun. Health 2014, 68, 856–862. [Google Scholar] [CrossRef] [PubMed]
- Lock, K.; Pomerleau, J.; Causer, L.; Altmann, D.R.; McKee, M. The global burden of disease attributable to low consumption of fruit and vegetables: Implications for the global strategy on diet. Bull World Health Organ 2005, 83, 100–108. [Google Scholar]
- He, F.J.; Nowson, C.A.; Lucas, M.; MacGregor, G.A. Increased consumption of fruit and vegetables is related to a reduced risk of coronary heart disease: Meta-analysis of cohort studies. J. Hum. Hypertens. 2007, 21, 717. [Google Scholar] [CrossRef]
- He, F.J.; Nowson, C.A.; MacGregor, G.A. Fruit and vegetable consumption and stroke: Meta-analysis of cohort studies. Lancet 2006, 367, 320–326. [Google Scholar] [CrossRef]
- Hu, D.; Huang, J.; Wang, Y.; Zhang, D.; Qu, Y. Fruits and Vegetables Consumption and Risk of Stroke. Meta-Anal. Prospect. Cohort Stud. 2014, 45, 1613–1619. [Google Scholar] [CrossRef]
- Crowe, F.; W Roddam, A.; J Key, T.; N Appleby, P.; Overvad, K.; Jakobsen, M.; Tjønneland, A.; Hansen, L.; Boeing, H.; Weikert, C.; et al. Fruit and Vegetable Intake and Mortality from Ischaemic Heart Disease: Results from the European Prospective Investigation into Cancer and Nutrition (EPIC)-Heart Study. Eur. Heart J. 2011, 32, 1235–1243. [Google Scholar] [CrossRef] [PubMed]
- Borgi, L.; Muraki, I.; Satija, A.; Willett, W.C.; Rimm, E.B.; Forman, J.P. Fruit and Vegetable Consumption and the Incidence of Hypertension in Three Prospective Cohort Studies. Hypertension 2016, 67, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Li, F.; Wang, L.; Zhang, D. Fruit and Vegetables Consumption and Risk of Hypertension: A Meta-Analysis. J. Clin. Hypertens. (Greenwich Conn,) 2016, 18, 468–476. [Google Scholar] [CrossRef] [PubMed]
- Bhupathiraju, S.N.; Wedick, N.M.; Pan, A.; Manson, J.E.; Rexrode, K.M.; Willett, W.C.; Rimm, E.B.; Hu, F.B. Quantity and variety in fruit and vegetable intake and risk of coronary heart disease. Am. J. Clin. Nutr. 2013, 98, 1514–1523. [Google Scholar] [CrossRef]
- Dauchet, L.; Amouyel, P.; Dallongeville, J. Fruit and vegetable consumption and risk of stroke: A meta-analysis of cohort studies. Neurology 2005, 65, 1193–1197. [Google Scholar] [CrossRef]
- Zhan, J.; Liu, Y.J.; Cai, L.B.; Xu, F.R.; Xie, T.; He, Q.Q. Fruit and vegetable consumption and risk of cardiovascular disease: A meta-analysis of prospective cohort studies. Crit. Rev. Food Sci. Nutr. 2017, 57, 1650–1663. [Google Scholar] [CrossRef]
- Kaiser, K.A.; Brown, A.W.; Bohan Brown, M.M.; Shikany, J.M.; Mattes, R.D.; Allison, D.B. Increased fruit and vegetable intake has no discernible effect on weight loss: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2014, 100, 567–576. [Google Scholar] [CrossRef]
- Tapsell, L.C.; Dunning, A.; Warensjo, E.; Lyons-Wall, P.; Dehlsen, K. Effects of vegetable consumption on weight loss: A review of the evidence with implications for design of randomized controlled trials. Am. J. Clin. Nutr. 2014, 54, 1529–1538. [Google Scholar] [CrossRef]
- Ledoux, T.A.; Hingle, M.D.; Baranowski, T. Relationship of fruit and vegetable intake with adiposity: A systematic review. Obes. Rev. 2011, 12, e143–e150. [Google Scholar] [CrossRef]
- Carter, P.; Gray, L.J.; Troughton, J.; Khunti, K.; Davies, M.J. Fruit and vegetable intake and incidence of type 2 diabetes mellitus: Systematic review and meta-analysis. BMJ (Clin. res. ed.) 2010, 341. [Google Scholar] [CrossRef]
- Harding, A.H.; Wareham, N.J.; Bingham, S.A.; Khaw, K.; Luben, R.; Welch, A.; Forouhi, N.G. Plasma vitamin C level, fruit and vegetable consumption, and the risk of new-onset type 2 diabetes mellitus: The European prospective investigation of cancer--Norfolk prospective study. Arch. Intern. Med. 2008, 168, 1493–1499. [Google Scholar] [CrossRef] [PubMed]
- Villegas, R.; Shu, X.O.; Gao, Y.T.; Yang, G.; Elasy, T.; Li, H.; Zheng, W. Vegetable but not fruit consumption reduces the risk of type 2 diabetes in Chinese women. J. Nutr. 2008, 138, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Bazzano, L.A.; Li, T.Y.; Joshipura, K.J.; Hu, F.B. Intake of fruit, vegetables, and fruit juices and risk of diabetes in women. Diabetes Care 2008, 31, 1311–1317. [Google Scholar] [CrossRef] [PubMed]
- Montonen, J.; Jarvinen, R.; Heliovaara, M.; Reunanen, A.; Aromaa, A.; Knekt, P. Food consumption and the incidence of type II diabetes mellitus. Eur. J. Clin. Nutr. 2005, 59, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Serdula, M.; Janket, S.J.; Cook, N.R.; Sesso, H.D.; Willett, W.C.; Manson, J.E.; Buring, J.E. A prospective study of fruit and vegetable intake and the risk of type 2 diabetes in women. Diabetes Care 2004, 27, 2993–2996. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S.; Mokdad, A.H. Fruit and vegetable consumption and diabetes mellitus incidence among U.S. adults. Prev. Med. 2001, 32, 33–39. [Google Scholar] [CrossRef]
- Meyer, K.A.; Kushi, L.H.; Jacobs, D.R., Jr.; Slavin, J.; Sellers, T.A.; Folsom, A.R. Carbohydrates, dietary fiber, and incident type 2 diabetes in older women. J. Clin. Nutr. 2000, 71, 921–930. [Google Scholar] [CrossRef]
- Hirayama, F.; Lee, A.H.; Binns, C.W.; Zhao, Y.; Hiramatsu, T.; Tanikawa, Y.; Nishimura, K.; Taniguchi, H. Do vegetables and fruits reduce the risk of chronic obstructive pulmonary disease? A case–control study in Japan. Prev. Med. 2009, 49, 184–189. [Google Scholar] [CrossRef]
- Hosseini, B.; Berthon, B.S.; Wark, P.; Wood, L.G. Effects of Fruit and Vegetable Consumption on Risk of Asthma, Wheezing and Immune Responses: A Systematic Review and Meta-Analysis. Nutrients 2017, 9. [Google Scholar] [CrossRef]
- Soerjomataram, I.; Oomen, D.; Lemmens, V.; Oenema, A.; Benetou, V.; Trichopoulou, A.; Coebergh, J.W.; Barendregt, J.; de Vries, E. Increased consumption of fruit and vegetables and future cancer incidence in selected European countries. Eur. J. Cancer 2010, 46, 2563–2580. [Google Scholar] [CrossRef] [PubMed]
- Leenders, M.; Siersema, P.D.; Overvad, K.; Tjonneland, A.; Olsen, A.; Boutron-Ruault, M.C.; Bastide, N.; Fagherazzi, G.; Katzke, V.; Kuhn, T.; et al. Subtypes of fruit and vegetables, variety in consumption and risk of colon and rectal cancer in the European Prospective Investigation into Cancer and Nutrition. Int. J. Cancer 2015, 137, 2705–2714. [Google Scholar] [CrossRef] [PubMed]
- Benetou, V.; Orfanos, P.; Lagiou, P.; Trichopoulos, D.; Boffetta, P.; Trichopoulou, A. Vegetables and fruits in relation to cancer risk: Evidence from the Greek EPIC cohort study. Cancer Epidemiol. Biomark. Prev. 2008, 17, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Linseisen, J.; Rohrmann, S.; Miller, A.B.; Bueno-de-Mesquita, H.B.; Buchner, F.L.; Vineis, P.; Agudo, A.; Gram, I.T.; Janson, L.; Krogh, V.; et al. Fruit and vegetable consumption and lung cancer risk: Updated information from the European Prospective Investigation into Cancer and Nutrition (EPIC). Int. J. Cancer 2007, 121, 1103–1114. [Google Scholar] [CrossRef]
- Gonzalez, C.A.; Pera, G.; Agudo, A.; Bueno-de-Mesquita, H.B.; Ceroti, M.; Boeing, H.; Schulz, M.; Del Giudice, G.; Plebani, M.; Carneiro, F.; et al. Fruit and vegetable intake and the risk of stomach and oesophagus adenocarcinoma in the European Prospective Investigation into Cancer and Nutrition (EPIC-EURGAST). Int. J. Cancer 2006, 118, 2559–2566. [Google Scholar] [CrossRef]
- Takachi, R.; Inoue, M.; Sugawara, Y.; Tsuji, I.; Tsugane, S.; Ito, H.; Matsuo, K.; Tanaka, K.; Tamakoshi, A.; Mizoue, T.; et al. Fruit and vegetable intake and the risk of overall cancer in Japanese: A pooled analysis of population-based cohort studies. J. Epidemiol. 2017, 27, 152–162. [Google Scholar] [CrossRef]
- Wang, M.; Qin, S.; Zhang, T.; Song, X.; Zhang, S. The effect of fruit and vegetable intake on the development of lung cancer: A meta-analysis of 32 publications and 20 414 cases. Eur. J. Clin. Nutr. 2015, 69, 1184. [Google Scholar] [CrossRef]
- Li, M.; Fan, Y.; Zhang, X.; Hou, W.; Tang, Z. Fruit and vegetable intake and risk of type 2 diabetes mellitus: Meta-analysis of prospective cohort studies. BMJ Open 2014, 4, e005497. [Google Scholar] [CrossRef]
- Appleton, K.M.; Hemingway, A.; Saulais, L.; Dinnella, C.; Monteleone, E.; Depezay, L.; Morizet, D.; Armando Perez-Cueto, F.J.; Bevan, A.; Hartwell, H. Increasing vegetable intakes: Rationale and systematic review of published interventions. Eur. J. Nutr. 2016, 55, 869–896. [Google Scholar] [CrossRef]
- Liu, R.H. Health-promoting components of fruits and vegetables in the diet. Adv. Nutr. 2013, 4, 384S–392S. [Google Scholar] [CrossRef]
- Slavin, J.L.; Lloyd, B. Health Benefits of Fruits and Vegetables. Adv. Nutr. 2012, 3, 506–516. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Sheehy, T.; Kolonel, L. Sources of vegetables, fruits, and vitamins A, C and E among five ethnic groups: Results from the Multiethnic Cohort Study. Eur. J. Clin. Nutr. 2014, 68, 384–391. [Google Scholar] [CrossRef] [PubMed]
- Flood-Obbagy, J.E.; Rolls, B.J. The effect of fruit in different forms on energy intake and satiety at a meal. Appetite 2009, 52, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Van Duyn, M.A.S.; Pivonka, E. Overview of the Health Benefits of Fruit and Vegetable Consumption for the Dietetics Professional: Selected Literature. J. Am. Diet. Assoc. 2000, 100, 1511–1521. [Google Scholar] [CrossRef]
- Pem, D.; Jeewon, R. Fruit and Vegetable Intake: Benefits and Progress of Nutrition Education Interventions- Narrative Review Article. Iran. J. Public Health 2015, 44, 1309–1321. [Google Scholar] [PubMed]
- Loef, M.; Walach, H. Fruit, vegetables and prevention of cognitive decline or dementia: A systematic review of cohort studies. J. Nutr. Health Aging 2012, 16, 626–630. [Google Scholar]
- World Health Organization. Food and Agriculture Organization of the United Nations. Diet, Nutrition, and the Prevention of Chronic Diseases: Report of a Joint WHO/FAO Expert Consultation; World Health Organization: Geneva, Switzerland, 2003; p. 149. [Google Scholar]
- Micha, R.; Khatibzadeh, S.; Shi, P.; Andrews, K.G.; Engell, R.E.; Mozaffarian, D. Global, regional and national consumption of major food groups in 1990 and 2010: A systematic analysis including 266 country-specific nutrition surveys worldwide. BMJ Open 2015, 5. [Google Scholar] [CrossRef]
- Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [CrossRef]
- Miller, V.; Yusuf, S.; Chow, C.K.; Dehghan, M.; Corsi, D.J.; Lock, K.; Popkin, B.; Rangarajan, S.; Khatib, R.; Lear, S.A.; et al. Availability, affordability, and consumption of fruits and vegetables in 18 countries across income levels: Findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet Glob. Health 2016, 4, e695–e703. [Google Scholar] [CrossRef]
- Hall, J.N.; Moore, S.; Harper, S.B.; Lynch, J.W. Global variability in fruit and vegetable consumption. Am. J. Prev. Med. 2009, 36, 402–409. [Google Scholar] [CrossRef]
- Agudo, A. Measuring Intake of fruit and Vegetables [electronic resource] / Antonio Agudo; World Health Organization: Geneva, Switzerland.
- Food-Based Dietary Guidelines. Available online: http://www.fao.org/nutrition/education/food-dietary-guidelines/home/en/ (accessed on 15 March 2018).
- Research, W.C.R.F.A.I.f.C. Food, Nutrition, Physical Activity, and the Prevention of Cancer: A Global Perspective; American Institute for Cancer Research: Washington, DC, USA, 2007. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339. [Google Scholar] [CrossRef] [PubMed]
- Nag, O.S. The Regions Of Europe. 13 March. Available online: https://www.worldatlas.com/articles/the-four-european-regions-as-defined-by-the-united-nations-geoscheme-for-europe.html (accessed on 13 March 2018).
- Sawe, B.E. What Is The United Nations Geoscheme? Available online: https://www.worldatlas.com/articles/what-is-the-united-nations-geoscheme.html (accessed on 13 March 2018).
- EFSA. The EFSA Comprehensive European Food Consumption Database. Available online: https://www.efsa.europa.eu/en/food-consumption/comprehensive-database (accessed on 20 June 2019).
- Hilger, J.; Friedel, A.; Herr, R.; Rausch, T.; Roos, F.; Wahl, D.A.; Pierroz, D.D.; Weber, P.; Hoffmann, K. A systematic review of vitamin D status in populations worldwide. Br. J. Nutr. 2014, 111, 23–45. [Google Scholar] [CrossRef] [PubMed]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed]
- Barde, M.P.; Barde, P.J. What to use to express the variability of data: Standard deviation or standard error of mean? Perspect. Clin. Res. 2012, 3, 113–116. [Google Scholar] [CrossRef] [PubMed]
- (UNICEF), U.N.C.s.F. The State of the World’s Children 2015: Executive Summary. Reimagine the Future. Innovation for Every Child; UNICEF: New York, NY, USA, 2014. [Google Scholar]
- Food Balance Sheets. Available online: http://www.fao.org/economic/ess/fbs/en/ (accessed on 15 July 2019).
- Introduction. In Food Balance Sheets- A Handbook; FAO, Ed.; FAO: Rome, Italy, 2001. [Google Scholar]
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT–Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef]
- Herforth, A.; Arimond, M.; Alvarez-Sanchez, C.; Coates, J.; Christianson, K.; Muehlhoff, E. A Global Review of Food-Based Dietary Guidelines. Adv. Nutr. 2019, 10, 590–605. [Google Scholar] [CrossRef]
- Institute of Medicine (US) and National Research Council (US) Committee on Childhood Obesity Prevention Actions for Local Governments. Actions for Healthy Eating. In Local Government Actions to Prevent Childhood Obesity; Parker L, B.A., Sanchez, E., Eds.; National Academies Press (US): Washington, DC, USA, 2009. [Google Scholar]
- Pomerleau, J.; Lock, K.; Knai, C.; McKee, M. Interventions designed to increase adult fruit and vegetable intake can be effective: A systematic review of the literature. J. Nutr. 2005, 135, 2486–2495. [Google Scholar] [CrossRef]
- Conner, T.S.; Brookie, K.L.; Carr, A.C.; Mainvil, L.A.; Vissers, M.C.M. Let them eat fruit! The effect of fruit and vegetable consumption on psychological well-being in young adults: A randomized controlled trial. PLoS ONE 2017, 12, e0171206. [Google Scholar] [CrossRef]
- Plaete, J.; Crombez, G.; Van der Mispel, C.; Verloigne, M.; Van Stappen, V.; De Bourdeaudhuij, I. Effect of the Web-Based Intervention MyPlan 1.0 on Self-Reported Fruit and Vegetable Intake in Adults Who Visit General Practice: A Quasi-Experimental Trial. J. Med. Internet Res. 2016, 18, e47. [Google Scholar] [CrossRef]
- Mason-D’Croz, D.; Bogard, J.R.; Sulser, T.B.; Cenacchi, N.; Dunston, S.; Herrero, M.; Wiebe, K. Gaps between fruit and vegetable production, demand, and recommended consumption at global and national levels: An integrated modelling study. Lancet. Planet. Health 2019, 3, e318–e329. [Google Scholar] [CrossRef]
- Ishangulyyev, R.; Kim, S.; Lee, S.H. Understanding Food Loss and Waste-Why Are We Losing and Wasting Food? Foods 2019, 8, 297. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Continent | Region | Number of countries in the Region | Vegetable intake per Region (g/day) | Vegetable Supply per Region (g/day) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Countries with Data (n) | Weighted Mean | Range | Countries with Vegetable Intake ≥240 g/day (%) | Countries with Data (n) | Weighted Mean | Range | % of Vegetable Supply Consumed | |||
| Asia | West | 11 | 11 | 144 | 89–256 | 9 | 9 | 545 | 202–765 | 26 1 |
| East | 8 | 6 | 349 | 80–357 | 67 | 6 | 882 | 149–969 | 40 1 | |
| Southeast | 13 | 11 | 153 | 91–400 | 27 | 10 | 190 | 92–577 | 80 4 | |
| South | 8 | 7 | 81 | 62–304 | 29 | 6 | 264 | 75–315 | 31 3 | |
| Europe | East | 13 | 12 | 270 | 83–382 | 25 | 12 | 323 | 109–956 | 84 2 |
| North | 17 | 10 | 132 | 72–227 | 0 | 10 | 270 | 192–339 | 49 | |
| South | 17 | 9 | 167 | 128–240 | 11 | 8 | 453 | 221–662 | 37 | |
| West | 9 | 6 | 123 | 95–207 | 0 | 6 | 269 | 239–379 | 46 | |
| America | Central | 7 | 2 | 56 | 1–88 | 0 | 2 | 145 | 127–156 | 39 |
| South | 12 | 8 | 156 | 48–263 | 13 | 8 | 148 | 64–197 | 106 3 | |
| Caribbean | 29 | 14 | 104 | 38–163 | 0 | 9 | 102 | 53–252 | 102 1 | |
| North | 6 | 4 | 108 | 92–226 | 0 | 4 | 277 | 153–474 | 39 | |
| Oceania | Australasia | 5 | 3 | 126 | 23–127 | 0 | 2 | 295 | 283–357 | 43 |
| Melanesia | 7 | 3 | 73 | 64–248 | 33 | 2 | 71 | 37–142 | 103 1 | |
| Micronesia | 8 | 5 | 122 | 32–216 | 0 | 1 | 155 | 155–155 | 78 | |
| Polynesia | 12 | 7 | 196 | 72–417 | 14 | 2 | 110 | 67–140 | 178 1 | |
| Africa | North | 11 | 5 | 122 | 88–170 | 0 | 4 | 434 | 230–531 | 28 |
| East | 20 | 14 | 98 | 28–304 | 7 | 10 | 86 | 48–206 | 114 5 | |
| Central | 9 | 6 | 103 | 25–304 | 17 | 6 | 134 | 21–294 | 77 4 | |
| West | 17 | 14 | 123 | 25–216 | 7 | 14 | 122 | 46–331 | 101 6 | |
| South | 5 | 5 | 135 | 88–168 | 0 | 5 | 114 | 54–119 | 118 4 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalmpourtzidou, A.; Eilander, A.; Talsma, E.F. Global Vegetable Intake and Supply Compared to Recommendations: A Systematic Review. Nutrients 2020, 12, 1558. https://doi.org/10.3390/nu12061558
Kalmpourtzidou A, Eilander A, Talsma EF. Global Vegetable Intake and Supply Compared to Recommendations: A Systematic Review. Nutrients. 2020; 12(6):1558. https://doi.org/10.3390/nu12061558
Chicago/Turabian StyleKalmpourtzidou, Aliki, Ans Eilander, and Elise F. Talsma. 2020. "Global Vegetable Intake and Supply Compared to Recommendations: A Systematic Review" Nutrients 12, no. 6: 1558. https://doi.org/10.3390/nu12061558
APA StyleKalmpourtzidou, A., Eilander, A., & Talsma, E. F. (2020). Global Vegetable Intake and Supply Compared to Recommendations: A Systematic Review. Nutrients, 12(6), 1558. https://doi.org/10.3390/nu12061558