Association between Non-Alcoholic Fatty Liver Disease and Dietary Habits, Stress, and Health-Related Quality of Life in Korean Adults

Abstract
1. Introduction
2. Materials and Methods
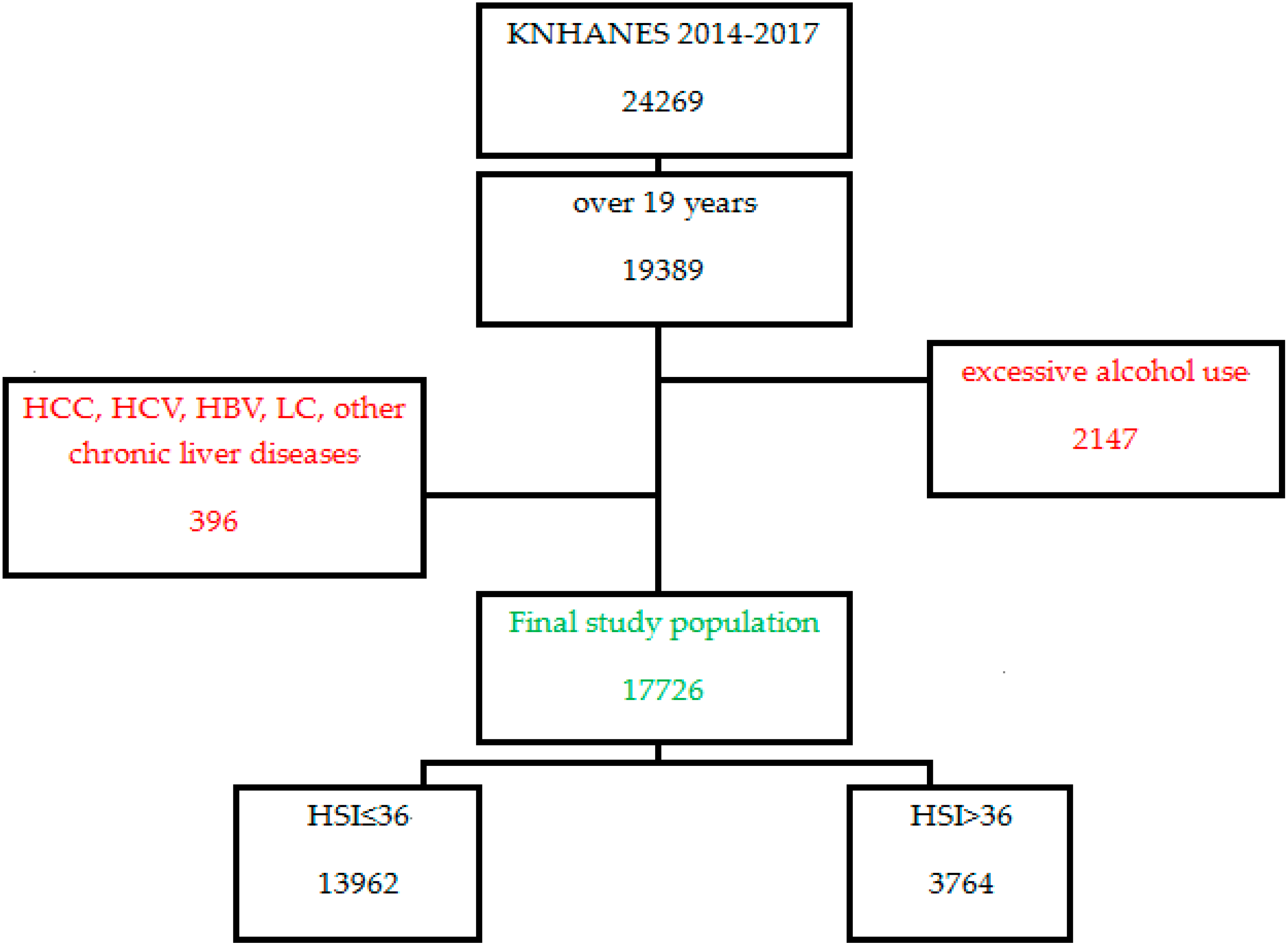
2.1. Study Design
2.2. Anthropometric Measurements
2.3. Sociodemographic and Lifestyle Variables
2.4. Statistical Analysis
3. Results
4. Discussion
Funding
Conflicts of Interest
References
- Hassan, K.; Bhalla, V.; El Regal, M.E.; A-Kader, H.H. Nonalcoholic fatty liver disease: A comprehensive review of a growing epidemic. World J. Gastroenterol. WJG 2014, 20, 12082. [Google Scholar] [CrossRef]
- Sozio, M.S.; Liangpunsakul, S.; Crabb, D. The role of lipid metabolism in the pathogenesis of alcoholic and nonalcoholic hepatic steatosis. In Seminars in Liver Disease; Thieme Medical Publishers: New York, NY, USA, 2010. [Google Scholar]
- Jun, D.W. The role of diet in non-alcoholic fatty liver disease. Korean J. Gastroenterol. 2013, 61, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Singal, A.K.; Hasanin, M.; Kaif, M.; Wiesner, R.; Kuo, Y.F. Nonalcoholic steatohepatitis is the most rapidly growing indication for simultaneous liver kidney transplantation in the United States. Transplantation 2016, 100, 607–612. [Google Scholar] [CrossRef]
- Yasutake, K.; Kohjima, M.; Kotoh, K.; Nakashima, M.; Nakamuta, M.; Enjoji, M. Dietary habits and behaviors associated with nonalcoholic fatty liver disease. World J. Gastroenterol. WJG 2014, 20, 1756. [Google Scholar] [CrossRef] [PubMed]
- Toshimitsu, K.; Matsuura, B.; Ohkubo, I.; Niiya, T.; Furukawa, S.; Hiasa, Y.; Kawamura, M.; Ebihara, K.; Onji, M. Dietary habits and nutrient intake in non-alcoholic steatohepatitis. Nutrition 2007, 23, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Abdelmalek, M.F.; Suzuki, A.; Guy, C.; Unalp-Arida, A.; Colvin, R.; Johnson, R.J.; Diehl, A.M. Nonalcoholic Steatohepatitis Clinical Research Network Increased fructose consumption is associated with fibrosis severity in patients with nonalcoholic fatty liver disease. Hepatology 2010, 51, 1961–1971. [Google Scholar] [CrossRef]
- Fuse, Y.; Hirao, A.; Kuroda, H.; Otsuka, M.; Tahara, Y.; Shibata, S. Differential roles of breakfast only (one meal per day) and a bigger breakfast with a small dinner (two meals per day) in mice fed a high-fat diet with regard to induced obesity and lipid metabolism. J. Circadian Rhythm. 2012, 10, 4. [Google Scholar] [CrossRef]
- Stunkard, A.J.; Grace, W.J.; Wolff, H.G. The night-eating syndrome: A pattern of food intake among certain obese patients. Am. J. Med. 1955, 19, 78–86. [Google Scholar] [CrossRef]
- Summerbell, C.D.; Moody, R.C.; Shanks, J.; Stock, M.J.; Geissler, C. Relationship between feeding pattern and body mass index in 220 free-living people in four age groups. Eur. J. Clin. Nutr. 1996, 50, 513–519. [Google Scholar]
- Timlin, M.T.; Pereira, M.A. Breakfast frequency and quality in the etiology of adult obesity and chronic diseases. Nutr. Rev. 2007, 65, 268–281. [Google Scholar] [CrossRef]
- Wyatt, H.R.; Grunwald, G.K.; Mosca, C.L.; Klem, M.L.; Wing, R.R.; Hill, J.O. Long-term weight loss and breakfast in subjects in the National Weight Control Registry. Obes. Res. 2002, 10, 78–82. [Google Scholar] [CrossRef] [PubMed]
- Lei, S.; Liu, Z.W.; Li, Y.; Gong, C.; Zhang, H.; Song, L.J.; Huang, C.Y.; Li, M. The prevalence of nonalcoholic fatty liver disease and its association with lifestyle/dietary habits among university faculty and staff in Chengdu. Biomed. Environ. Sci. 2012, 25, 383–391. [Google Scholar]
- Chung, G.E. Dietary patterns are associated with the prevalence of nonalcoholic fatty liver disease in Korean adults. Nutrition 2019, 62, 32–38. [Google Scholar] [CrossRef]
- Chang, J.H.; Lee, H.S.; Kang, E.H. A study on dietary habits, nutrient intakes and dietary quality in adults of a health screening and promotion center according to non-alcoholic fatty liver disease. J. Nutr. Health 2014, 47, 330–341. [Google Scholar] [CrossRef][Green Version]
- Chung, G.E.; Youn, J.; Kim, Y.S.; Lee, J.E.; Yang, S.Y.; Lim, J.H.; Song, J.H.; Doo, E.Y.; Kim, J.S. Non-Alcoholic Fatty Liver Disease and Its Association with Depression in Korean General Population. J. Korean Med. Sci. 2019, 34. [Google Scholar] [CrossRef]
- Surdea-Blaga, T.; Dumitraşcu, D. Depression and anxiety in nonalcoholic steatohepatitis: Is there any association? Rom. J. Intern. Med. Rev. Roum. Med. Interne 2011, 49, 273–280. [Google Scholar]
- Russ, T.C.; Kivimäki, M.; Morling, J.R.; Starr, J.M.; Stamatakis, E.; Batty, G.D. Association between psychological distress and liver disease mortality: A meta-analysis of individual study participants. Gastroenterology 2015, 148, 958–966. [Google Scholar] [CrossRef]
- Nagaraja, A.S.; Sadaoui, N.C.; Dorniak, P.L.; Lutgendorf, S.K.; Sood, A.K. SnapShot: Stress and disease. Cell Metab. 2016, 23, 388.e1. [Google Scholar] [CrossRef]
- Lundberg, U. Stress hormones in health and illness: The roles of work and gender. Psychoneuroendocrinology 2005, 30, 1017–1021. [Google Scholar] [CrossRef]
- Schneiderman, N.; Ironson, G.; Siegel, S.D. Stress and health: Psychological, behavioral, and biological determinants. Annu. Rev. Clin. Psychol. 2005, 1, 607–628. [Google Scholar] [CrossRef]
- Björntorp, P. Visceral fat accumulation: The missing link between psychosocial factors and cardiovascular disease? J. Inter. Med. 1991, 230, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Yudkin, J.S.; Kumari, M.; Humphries, S.E.; Mohamed-Ali, V. Inflammation, obesity, stress and coronary heart disease: Is interleukin-6 the link? Atherosclerosis 2000, 148, 209–214. [Google Scholar] [CrossRef]
- Dan, A.A.; Kallman, J.B.; Wheeler, A.; Younoszai, Z.; Collantes, R.; Bodini, S.; Gerber, L.; Younossi, Z.M. Health-related quality of life in patients with non-alcoholic fatty liver disease. Aliment. Pharmacol. Ther. 2007, 26, 815–820. [Google Scholar] [CrossRef] [PubMed]
- Assimakopoulos, K.; Karaivazoglou, K.; Tsermpini, E.E.; Diamantopoulou, G.; Triantos, C. Quality of life in patients with nonalcoholic fatty liver disease: A systematic review. J. Psychosom. Res. 2018, 112, 73–80. [Google Scholar] [CrossRef]
- David, K.; Kowdley, K.V.; Unalp, A.; Kanwal, F.; Brunt, E.M.; Schwimmer, J.B. Quality of life in adults with nonalcoholic fatty liver disease: Baseline data from the nonalcoholic steatohepatitis clinical research network. Hepatology 2009, 49, 1904–1912. [Google Scholar] [CrossRef]
- Kennedy-Martin, T.; Bae, J.P.; Paczkowski, R.; Freeman, E. Health-related quality of life burden of nonalcoholic steatohepatitis: A robust pragmatic literature review. J. Patient Rep. Outcomes 2018, 2, 28. [Google Scholar] [CrossRef]
- Tsuchiya, A.; Ikeda, S.; Ikegami, N.; Nishimura, S.; Sakai, I.; Fukuda, T.; Hamashima, C.; Hisashige, A.; Tamura, M. Estimating an EQ-5D population value set: The case of Japan. Health Econ. 2002, 11, 341–353. [Google Scholar] [CrossRef]
- Balestroni, G.; Bertolotti, G. EuroQol-5D (EQ-5D): An instrument for measuring quality of life. Monaldi Arch. Chest Dis. 2012, 78, 155–159. [Google Scholar] [CrossRef]
- Dolan, P.; Gudex, C.; Kind, P.; Williams, A. A Social Tariff for EuroQol: Results from a UK General Population Survey; University of York, Center for Health Economics: Heslington, UK, 1995. [Google Scholar]
- Luo, N.; Johnson, J.A.; Shaw, J.W.; Feeny, D.; Coons, S.J. Self-reported health status of the general adult US population as assessed by the EQ-5D and Health Utilities Index. Med. Care 2005, 43, 1078–1086. [Google Scholar] [CrossRef]
- Han, M.A.; Ryu, S.Y.; Park, J.; Kang, M.; Park, J.K.; Kim, K.S. Health-related Quality of Life Assessment by the EuroQol-5D in Some Rural Adults. J. Prev. Med. Public Health 2008, 41, 173–180. [Google Scholar] [CrossRef]
- Jo, M.-W.; Yun, S.C.; Lee, S.I. Estimating quality weights for EQ-5D health states with the time trade-off method in South Korea. Value Health 2008, 11, 1186–1189. [Google Scholar] [CrossRef] [PubMed]
- Kang, E.J.; Shin, H.S.; Park, H.J.; Jo, M.W.; Kim, N.Y. A valuation of health status using EQ-5D. Korean J. Health Econ. Policy 2006, 12, 19–43. [Google Scholar]
- Papagianni, M.; Sofogianni, A.; Tziomalos, K. Non-invasive methods for the diagnosis of nonalcoholic fatty liver disease. World J. Hepatol. 2015, 7, 638. [Google Scholar] [CrossRef] [PubMed]
- Bateman, R.M.; Sharpe, M.D.; Jagger, J.E.; Ellis, C.G.; Solé-Violán, J.; López-Rodríguez, M.; Herrera-Ramos, E.; Ruíz-Hernández, J.; Borderías, L.; Horcajada, J.; et al. Development, external validation, and comparative assessment of a new diagnostic score for hepatic steatosis. Am. J. Gastroenterol. 2014, 109, 1404. [Google Scholar]
- Shen, Y.N.; Yu, M.X.; Gao, Q.; Li, Y.Y.; Huang, J.J.; Sun, C.M.; Qiao, N.; Zhang, H.X.; Wang, H.; Lu, Q.; et al. External validation of non-invasive prediction models for identifying ultrasonography-diagnosed fatty liver disease in a Chinese population. Medicine 2017, 96, e7610. [Google Scholar] [CrossRef]
- Zhang, Z.; Wang, G.; Kang, K.; Wu, G.; Wang, P. Diagnostic accuracy and clinical utility of a new noninvasive index for hepatic steatosis in patients with hepatitis B virus infection. Sci. Rep. 2016, 6, 32875. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, D.; Kim, H.J.; Lee, C.H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.H.; Cho, S.H.; Sung, M.W.; et al. Hepatic steatosis index: A simple screening tool reflecting nonalcoholic fatty liver disease. Dig. Liver Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef]
- Lee, J.; Ha, J.; Jo, K.; Lim, D.J.; Lee, J.M.; Chang, S.A.; Kang, M.I.; Cha, B.Y.; Kim, M.H. Male-specific association between subclinical hypothyroidism and the risk of non-alcoholic fatty liver disease estimated by hepatic steatosis index: Korea National Health and Nutrition Examination Survey 2013 to 2015. Sci. Rep. 2018, 8, 1–7. [Google Scholar] [CrossRef]
- Kweon, S.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.H.; Oh, K. Data resource profile: The Korea national health and nutrition examination survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Chen, L.D.; Huang, J.F.; Chen, Q.S.; Lin, G.F.; Zeng, H.X.; Lin, X.F.; Lin, X.J.; Lin, L.; Lin, Q.C. Validation of fatty liver index and hepatic steatosis index for screening of non-alcoholic fatty liver disease in adults with obstructive sleep apnea hypopnea syndrome. Chin. Med. J. 2019, 132, 2670–2676. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, H.E.; Arendt, B.M.; Noureldin, S.A.; Therapondos, G.; Guindi, M.; Allard, J.P. A cross-sectional study assessing dietary intake and physical activity in Canadian patients with nonalcoholic fatty liver disease vs healthy controls. J. Acad. Nutr. Diet. 2014, 114, 1181–1194. [Google Scholar] [CrossRef] [PubMed]
- Kris-Etherton, P.M.; Pearson, T.A.; Wan, Y.; Hargrove, R.L.; Moriarty, K.; Fishell, V.; Etherton, T.D. High.–monounsaturated fatty acid diets lower both plasma cholesterol and triacylglycerol concentrations. Am. J. Clin. Nutr. 1999, 70, 1009–1015. [Google Scholar] [CrossRef] [PubMed]
- Zelber-Sagi, S.; Nitzan-Kaluski, D.; Goldsmith, R.; Webb, M.; Blendis, L.; Halpern, Z.; Oren, R. Long term nutritional intake and the risk for non-alcoholic fatty liver disease (NAFLD): A population based study. J. Hepatol. 2007, 47, 711–717. [Google Scholar] [CrossRef] [PubMed]
- Ganji, S.H.; Kashyap, M.L.; Kamanna, V.S. Niacin inhibits fat accumulation, oxidative stress, and inflammatory cytokine IL-8 in cultured hepatocytes: Impact on non-alcoholic fatty liver disease. Metabolism 2015, 64, 982–990. [Google Scholar] [CrossRef] [PubMed]
- Ullah, R.; Rauf, N.; Nabi, G.; Ullah, H.; Shen, Y.; Zhou, Y.D.; Fu, J. Role of nutrition in the pathogenesis and prevention of non-alcoholic fatty liver disease: Recent updates. Int. J. Biol. Sci. 2019, 15, 265. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.Y.; Tzeng, Y.H.; Chai, C.Y.; Hsieh, A.T.; Chen, J.R.; Chang, L.S.; Yang, S.S. Soy protein retards the progression of non-alcoholic steatohepatitis via improvement of insulin resistance and steatosis. Nutrition 2011, 27, 943–948. [Google Scholar] [CrossRef]
- Trovato, F.M.; Martines, G.F.; Brischetto, D.; Catalano, D.; Musumeci, G.; Trovato, G.M. Fatty liver disease and lifestyle in youngsters: Diet, food intake frequency, exercise, sleep shortage and fashion. Liver Int. 2016, 36, 427–433. [Google Scholar] [CrossRef]
- Koot, B.G.; van der Baan-Slootweg, O.H.; Tamminga-Smeulders, C.L.; Rijcken, T.H.; Korevaar, J.C.; van Aalderen, W.M.; Jansen, P.L.; Benninga, M.A. Lifestyle intervention for non-alcoholic fatty liver disease: Prospective cohort study of its efficacy and factors related to improvement. Arch. Dis. Child. 2011, 96, 669–674. [Google Scholar] [CrossRef]
- Nseir, W.; Hellou, E.; Assy, N. Role of diet and lifestyle changes in nonalcoholic fatty liver disease. World J. Gastroenterol. WJG 2014, 20, 9338. [Google Scholar]
- Cho, S.; Dietrich, M.; Brown, C.J.; Clark, C.A.; Block, G. The effect of breakfast type on total daily energy intake and body mass index: Results from the Third National Health and Nutrition Examination Survey (NHANES III). J. Am. Coll. Nutr. 2003, 22, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Song, W.O.; Chun, O.K.; Obayashi, S.; Cho, S.; Chung, C.E. Is consumption of breakfast associated with body mass index in US adults? J. Am. Diet. Assoc. 2005, 105, 1373–1382. [Google Scholar] [CrossRef] [PubMed]
- Moreno, L.A.; Rodriguez, G. Dietary risk factors for development of childhood obesity. Curr. Opin. Clin. Nutr. Metab. Care 2007, 10, 336–341. [Google Scholar] [CrossRef]
- Baratta, F.; Pastori, D.; Polimeni, L.; Bucci, T.; Ceci, F.; Calabrese, C.; Ernesti, I.; Pannitteri, G.; Violi, F.; Angelico, F.; et al. Adherence to mediterranean diet and non-alcoholic fatty liver disease: Effect on insulin resistance. Am. J. Gastroenterol. 2017, 112, 1832–1839. [Google Scholar] [CrossRef] [PubMed]
- De Souza Marinho, T.; Ornellas, F.; Barbosa-da-Silva, S.; Mandarim-de-Lacerda, C.A.; Aguila, M.B. Beneficial effects of intermittent fasting on steatosis and inflammation of the liver in mice fed a high-fat or a high-fructose diet. Nutrition 2019, 65, 103–112. [Google Scholar] [CrossRef]
- Hotamisligil, G.S.; Shargill, N.S.; Spiegelman, B.M. Adipose expression of tumor necrosis factor-alpha: Direct role in obesity-linked insulin resistance. Science 1993, 259, 87–91. [Google Scholar] [CrossRef]
- Czech, B.; Neumann, I.D.; Müller, M.; Reber, S.O.; Hellerbrand, C. Effect of chronic psychosocial stress on nonalcoholic steatohepatitis in mice. Int. J. Clin Exp. Pathol. 2013, 6, 1585. [Google Scholar] [PubMed]
- Zhang, S.; Ma, C.; Wang, X.; Wang, Q.; Song, W.; Li, C.; Zhai, C.; Qi, Y.; Fan, S.; Cheng, F. Impact of chronic psychological stress on nonalcoholic fatty liver disease. Int. J. Clin. Exp. Med. 2019, 12, 7991–7998. [Google Scholar]
- Stewart, K.E.; Levenson, J.L. Psychological and psychiatric aspects of treatment of obesity and nonalcoholic fatty liver disease. Clin. Liver Dis. 2012, 16, 615–629. [Google Scholar] [CrossRef] [PubMed]
- Tapper, E.B.; Sengupta, N.; Hunink, M.G.; Afdhal, N.H.; Lai, M. Cost-effective evaluation of nonalcoholic fatty liver disease with NAFLD fibrosis score and vibration controlled transient elastography. Am. J. Gastroenterol. 2015, 110, 1298–1304. [Google Scholar] [CrossRef]
- Cortesi, P.; Scalone, L.; Ciampichini, R.; Cozzolino, P.; Cesana, G.; Mantovani, L.; Okolicsanyi, S.; Ciaccio, A.; Rota, M.; Gentiluomo, M.; et al. Health related quality of life in the major liver conditions. Hepatology 2013, 58 (Suppl. 1), 1210A. [Google Scholar]
- Fontaine, K.; Barofsky, I. Obesity and health-related quality of life. Obes. Rev. 2001, 2, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Swallen, K.C.; Reither, E.N.; Haas, S.A.; Meier, A.M. Overweight, obesity, and health-related quality of life among adolescents: The National Longitudinal Study of Adolescent Health. Pediatrics 2005, 115, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Hassan, M.K.; Joshi, A.V.; Madhavan, S.S.; Amonkar, M.M. Obesity and health-related quality of life: A cross-sectional analysis of the US population. Int. J. Obes. 2003, 27, 1227–1232. [Google Scholar] [CrossRef]
- Jia, H.; Lubetkin, E.I. The impact of obesity on health-related quality-of-life in the general adult US population. J. Public Health 2005, 27, 156–164. [Google Scholar] [CrossRef]
- Ford, E.S.; Li, C. Metabolic syndrome and health-related quality of life among US adults. Ann. Epidemiol. 2008, 18, 165–171. [Google Scholar] [CrossRef]
- Kim, M.H.; Cho, Y.S.; Uhm, W.S.; Kim, S.; Bae, S.C. Cross-cultural adaptation and validation of the Korean version of the EQ-5D in patients with rheumatic diseases. Qual. Life Res. 2005, 14, 1401–1406. [Google Scholar] [CrossRef]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.F.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef]
- Nam, H.; Kim, K.; Kwon, S.; Koh, K.; Poul, K.; Ko, K.W.; Kind, P. EQ-5D Korean Valuation Study Using Time Trade Off Method; ScienceOpen, Inc.: Burlington, MA, USA, 2011. [Google Scholar]


{kind=link}
| Total (17,726) | HSI ≤ 36 | HSI > 36 | p-Value a | ||
|---|---|---|---|---|---|
| Sex | Male | 7986 (50.6) | 6004 (47.5) | 1982 (61.3) | <0.0001 |
| Female | 9740 (49.4) | 7958 (52.5) | 1782 (38.7) | ||
| Age | years | 43.93 ± 0.25 | 43.59 ± 0.27 | 45.1 ± 0.34 | <0.0001 |
| Educational level | ≤Elementary | 4129 (17.3) | 3360 (18.1) | 769 (14.5) | <0.0001 |
| Middle | 2064 (11.2) | 1623 (11.3) | 441 (10.8) | ||
| High | 5010 (31) | 3868 (30.7) | 1142 (32.3) | ||
| ≥College | 5753 (35.9) | 4515 (35.5) | 1238 (37.4) | ||
| Smoking | 2905 (19.5) | 2110 (18.1) | 795 (24.4) | <0.0001 | |
| Exercise | 6956 (42) | 5495 (42.1) | 1461 (41.7) | <0.0001 | |
| Alcohol | 8790 (54.1) | 6860 (53.5) | 1930 (56) | <0.0001 | |
| Stress | 4637 (28.2) | 3496 (26.9) | 1141(32.7) | <0.0001 | |
| Breakfast frequency | 5–7/week | 10,153 (60.2) | 8129 (61.1) | 2024 (57) | 0.002 |
| 3–4/week | 1702 (12.3) | 1332 (12.2) | 370 (12.6) | ||
| 1–2/week | 1603 (12.2) | 1234 (11.7) | 369 (14.2) | ||
| Rare | 1908 (15.2) | 1475 (15) | 433 (16.2) | ||
| Lunch frequency | 5–7/week | 13,933 (90.4) | 11,074 (90.8) | 2859 (89) | 0.047 |
| 3–4/week | 917 (6.3) | 708 (6.2) | 209 (7) | ||
| 1–2/week | 261 (1.7) | 198 (1.6) | 63 (2.1) | ||
| Rare | 255 (1.5) | 190 (1.4) | 65 (2) | ||
| Dinner frequency | 5–7/week | 13,980 (90.1) | 11,079 (90.1) | 2901 (90.1) | 0.783 |
| 3–4/week | 1106 (8.1) | 859 (8) | 247 (8.3) | ||
| 1–2/week | 218 (1.5) | 180 (1.6) | 38 (1.3) | ||
| Rare | 62 (0.4) | 52 (0.4) | 10 (0.3) | ||
| Companion for breakfast | 7120 (42.3) | 5692 (42.8) | 1428 (40.4) | 0.002 | |
| Companion for lunch | 10,343 (69.1) | 8234 (69.3) | 2109 (68) | 0.042 | |
| Companion for dinner | 11,676 (77) | 9240 (76.8) | 2436 (77.7) | 0.485 | |
| WC | 81.09 ± 0.13 | 77.84 ± 0.12 | 92.98 ± 0.17 | <0.0001 | |
| BMI | 23.66 ± 0.04 | 22.37 ± 0.03 | 28.3 ± 0.06 | <0.0001 | |
| Fasting glucose | 99.28 ± 0.23 | 96.71 ± 0.2 | 108.38 ± 0.6 | <0.0001 | |
| HbA1c | 5.61 ± 0.01 | 5.52 ± 0.01 | 5.92 ± 0.02 | <0.0001 | |
| TC | 190.3 ± 0.38 | 187.96 ± 0.38 | 198.54 ± 0.82 | <0.0001 | |
| HDL-C | 51.11 ± 0.14 | 52.63 ± 0.15 | 45.8 ± 0.2 | <0.0001 | |
| TG | 134.18 ± 1.23 | 120.86 ± 1.32 | 180.56 ± 2.56 | <0.0001 | |
| LDL-C | 119.07 ± 0.82 | 114.85 ± 1 | 124.47 ± 1.27 | <0.0001 | |
| Stress | 0.28 ± 0.004 | 0.27 ± 0.005 | 0.33 ± 0.01 | <0.0001 | |
| EQ-5D | 0.95 ± 0.001 | 0.96 ± 0.001 | 0.95 ± 0.002 | <0.0001 | |
| Characteristics | OR | (95% CI) | p-Value a | |
|---|---|---|---|---|
| Sex | Male | 1.747 | (1.609–1.898) | <0.0001 |
| Female | 1 | Reference | ||
| Age | 1.047 | (1.025–1.069) | <0.0001 | |
| Educational level | ≤Elementary | 0.762 | (0.678–0.856) | 0.003 |
| Middle | 0.903 | (0.788–1.034) | 0.190 | |
| High | 0.998 | (0.897–1.11) | 0.660 | |
| ≥College | 1 | Reference | ||
| Smoking | 1.349 | (1.221–1.49) | <0.0001 | |
| Exercise | 0.892 | (0.821–0.97) | <0.0001 | |
| Drinking | 1.057 | (0.966–1.156) | <0.0001 | |
| Breakfast frequency | 5–7/week | 1 | Reference | |
| 3–4/week | 1.104 | (0.952–1.28) | 0.545 | |
| 1–2/week | 1.301 | (1.123–1.508) | 0.245 | |
| Rare | 1.165 | (1.016–1.337) | 0.029 | |
| Lunch frequency | 5–7/week | 1 | Reference | |
| 3–4/week | 1.153 | (0.946–1.406) | 0.312 | |
| 1–2/week | 1.330 | (0.943–1.876) | 0.791 | |
| Rare | 1.415 | (1.005–1.992) | 0.046 | |
| Dinner frequency | 5–7/week | 1 | Reference | |
| 3–4/week | 1.034 | (0.878–1.218) | 0.692 | |
| 1–2/week | 0.833 | (0.548–1.267) | 0.897 | |
| Rare | 0.882 | (0.407–1.912) | 0.751 | |
| Eating out | ≥2/day | 1.250 | (1.006–1.552) | |
| 1/day | 1.103 | (0.906–1.343) | ||
| 5–6/week | 0.899 | (0.739–1.094) | ||
| 3–4/week | 0.971 | (0.78–1.208) | ||
| 1–2/week | 1.008 | (0.833–1.22) | ||
| 1–3/month | 1.064 | (0.868–1.304) | ||
| Rare | 1 | Reference | ||
| Companion for breakfast | Yes | 1 | Reference | |
| No | 1.008 | (0.903–1.126) | 0.001 | |
| Companion for lunch | Yes | 1 | Reference | |
| No | 1.029 | (0.932–1.136) | 0.018 | |
| Companion for dinner | Yes | 1 | Reference | |
| No | 0.958 | (0.857–1.07) | 0.335 | |
| WC | 1.237 | (1.227–1.247) | <0.0001 | |
| BMI | 2.389 | (2.309–2.471) | <0.0001 | |
| Fasting glucose | 1.021 | (1.018–1.023) | <0.0001 | |
| HbA1c | 1.829 | (1.707–1.96) | <0.0001 | |
| TC | 1.008 | (1.006–1.009) | <0.0001 | |
| HDL-C | 0.948 | (0.944–0.952) | <0.0001 | |
| TG | 1.004 | (1.003–1.005) | <0.0001 | |
| LDL-C | 1.008 | (1.005–1.011) | <0.0001 | |
| Stress recognition | 1.316 | (1.203–1.44) | <0.0001 | |
| EQ-5D | 2.255 | (1.533–3.317) | <0.0001 |
| OR | (95% CI) | p-Value a | ||
|---|---|---|---|---|
| Breakfast frequency | 5–7/week | 1 | Reference | |
| 3–4/week | 1.052 | 0.890–1.243 | 0.925 | |
| 1–2/week | 1.246 | 1.053–1.474 | 0.076 | |
| Rare | 1.042 | 0.890–1.221 | 0.609 | |
| Lunch frequency | 5–7/week | 1 | Reference | |
| 3–4/week | 1.116 | 0.903–1.378 | 0.399 | |
| 1–2/week | 1.291 | 0.907–1.836 | 0.891 | |
| Rare | 1.333 | 0.940–1.890 | 0.107 | |
| Dinner frequency | 5–7/week | 1 | Reference | |
| 3–4/week | 1.025 | 0.852–1.233 | 0.313 | |
| 1–2/week | 0.861 | 0.563–1.317 | 0.568 | |
| Rare | 0.653 | 0.278–1.533 | 0.327 | |
| Stress | 1.314 | 1.175–1.469 | <0.0001 | |
| EQ-5D | 3.028 | 1.893–4.844 | <0.0001 | |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, A.L. Association between Non-Alcoholic Fatty Liver Disease and Dietary Habits, Stress, and Health-Related Quality of Life in Korean Adults. Nutrients 2020, 12, 1555. https://doi.org/10.3390/nu12061555
Han AL. Association between Non-Alcoholic Fatty Liver Disease and Dietary Habits, Stress, and Health-Related Quality of Life in Korean Adults. Nutrients. 2020; 12(6):1555. https://doi.org/10.3390/nu12061555
Chicago/Turabian StyleHan, A Lum. 2020. "Association between Non-Alcoholic Fatty Liver Disease and Dietary Habits, Stress, and Health-Related Quality of Life in Korean Adults" Nutrients 12, no. 6: 1555. https://doi.org/10.3390/nu12061555
APA StyleHan, A. L. (2020). Association between Non-Alcoholic Fatty Liver Disease and Dietary Habits, Stress, and Health-Related Quality of Life in Korean Adults. Nutrients, 12(6), 1555. https://doi.org/10.3390/nu12061555