The Neuroendocrine Neoplasms of the Digestive Tract: Diagnosis, Treatment and Nutrition

 ,
, 
Abstract
1. Introduction
1.1. NEN Diagnostics
1.2. Types of Hormonally Active Neuroendocrine Neoplasms (NENs)
2. The Treatment of Neuroendocrine Neoplasms
3. The State and Method of Nutrition with Reference to the Risk of Cancer
3.1. Dietary Recommendations for NEN Patients
3.2. The Causes of Diarrhea in NEN Patients and Dietetic Modifications
3.3. Procedures to Follow in the Case of Constipation in NEN Patients
3.4. Nutrition that Takes into Account the Hormone Activity of NEN
3.5. A Diet for NEN Patients under the Risk of Malnutrition and/or Cachexia
4. Dietary Care Taking into Account Pharmacotherapy
5. Summary
5.1. Structure of the Underlying Research
Ethical Approval
Author Contributions
Funding
Conflicts of Interest
References
- Schimmack, S.; Svejda, B.; Lawrence, B.; Kidd, M.; Modlin, I. The diversity and commonalities of gastroenteropancreatic neuroendocrine tumors. Langenbecks Arch. Chir. 2011, 396, 273–298. [Google Scholar] [CrossRef] [PubMed]
- Oronsky, B.; Ma, P.C.; Morgensztern, D.; Carter, C.A. Nothing but NET: A Review of Neuroendocrine Tumors and Carcinomas. Neoplasia 2017, 19, 991–1002. [Google Scholar] [CrossRef] [PubMed]
- Scherübl, H.; Cadiot, G. Early Gastroenteropancreatic Neuroendocrine Tumors: Endoscopic Therapy and Surveillance. Visc. Med. 2017, 33, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Rindi, G.; Wiedenmann, B. Neuroendocrine neoplasms of the gut and pancreas: New insights. Nat. Rev. Endocrinol. 2011, 8, 54–64. [Google Scholar] [CrossRef]
- Öberg, K.; Hellman, P.; Kwekkeboom, D.; Jelic, S. On behalf of the ESMO Guidelines Working Group Neuroendocrine bronchial and thymic tumours: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2010, 21, v220–v222. [Google Scholar] [CrossRef] [PubMed]
- Klöppel, G. Neuroendocrine Neoplasms: Dichotomy, Origin and Classifications. Visc. Med. 2017, 33, 324–330. [Google Scholar] [CrossRef]
- Taal, B.; Visser, O. Epidemiology of Neuroendocrine Tumours. Neuroendocrinology 2004, 80, 3–7. [Google Scholar] [CrossRef]
- Meeker, A.K.; Heaphy, C. Gastroenteropancreatic endocrine tumors. Mol. Cell. Endocrinol. 2014, 386, 101–120. [Google Scholar] [CrossRef]
- Srirajaskanthan, R.; Ahmed, A.; Prachialias, A.; Srinivasan, P.; Heaton, N.; Jervis, N.; Quaglia, A.; Vivian, G.; Ramage, J. ENETS TNM Staging Predicts Prognosis in Small Bowel Neuroendocrine Tumours. ISRN Oncol. 2013, 2013, 420795. [Google Scholar] [CrossRef]
- Cheung, V.T.F.; Khan, M.S. A guide to midgut neuroendocrine tumours (NETs) and carcinoid syndrome. Front. Gastroenterol. 2014, 6, 264–269. [Google Scholar] [CrossRef]
- Jernman, J.; Valimaki, M.J.; Louhimo, J.; Haglund, C.; Arola, J. The Novel WHO 2010 Classification for Gastrointestinal Neuroendocrine Tumours Correlates Well with the Metastatic Potential of Rectal Neuroendocrine Tumours. Neuroendocrinology 2012, 95, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Modlin, I.; Champaneria, M.C.; Chan, A.K.; Kidd, M. A Three-Decade Analysis of 3,911 Small Intestinal Neuroendocrine Tumors: The Rapid Pace of No Progress. Am. J. Gastroenterol. 2007, 102, 1464–1473. [Google Scholar] [CrossRef] [PubMed]
- Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Fearon, K.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN guidelines on nutrition in cancer patients. Clin. Nutr. 2017, 36, 11–48. [Google Scholar] [CrossRef] [PubMed]
- Fearon, K.C.H.; Strasser, F.; Anker, S.; Bosaeus, I.; Bruera, E.; Fainsinger, R.L.; Jatoi, A.; Loprinzi, C.; Macdonald, N.; Mantovani, G.; et al. Definition and classification of cancer cachexia: An international consensus. Lancet Oncol. 2011, 12, 489–495. [Google Scholar] [CrossRef]
- Gallo, M.; Muscogiuri, G.; Pizza, G.; Ruggeri, R.M.; Barrea, L.; Faggiano, A.; Colao, A. On behalf of NIKE Group The management of neuroendocrine tumours: A nutritional viewpoint. Crit. Rev. Food Sci. Nutr. 2017, 59, 1046–1057. [Google Scholar] [CrossRef]
- Lindström, M.; Tohmola, N.; Renkonen, R.; Hamalainen, E.; Schalin-Jäntti, C.; Itkonen, O. Comparison of serum serotonin and serum 5-HIAA LC-MS/MS assays in the diagnosis of serotonin producing neuroendocrine neoplasms: A pilot study. Clin. Chim. Acta 2018, 482, 78–83. [Google Scholar] [CrossRef]
- Tritschler, S.; Erdelkamp, R.; Stief, C.; Hentrich, M. Neuroendokrines Prostatakarzinom. Der Urol. 2017, 56, 1475–1484. [Google Scholar] [CrossRef]
- Koenig, A.; Krug, S.; Mueller, D.; Barth, P.J.; Koenig, U.; Scharf, M.; Ellenrieder, V.; Michl, P.; Moll, R.; Homayunfar, K.; et al. Clinicopathological hallmarks and biomarkers of colorectal neuroendocrine neoplasms. PLoS ONE 2017, 12, e0188876. [Google Scholar] [CrossRef]
- Er, L.-M.; Li, Y.; Wu, M.-L.; Zhao, Q.; Tan, B.-B.; Wang, X.-L.; Wang, S.-J. Expression of IMP3 as a marker for predicting poor outcome in gastroenteropancreatic neuroendocrine neoplasms. Oncol. Lett. 2017, 13, 2391–2396. [Google Scholar] [CrossRef]
- Fottner, C.; Ferrata, M.; Weber, M.M. Hormone secreting gastro-entero-pancreatic neuroendocrine neoplasias (GEP-NEN): When to consider, how to diagnose? Rev. Endocr. Metab. Disord. 2017, 18, 393–410. [Google Scholar] [CrossRef]
- Seymour, N.; Sawh, S.C. Mega-dose intravenous octreotide for the treatment of carcinoid crisis: A systematic review. Can. J. Anesth. 2013, 60, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Sundin, A.; Arnold, R.; Baudin, E.; Cwikla, J.; Eriksson, B.; Fanti, S.; Fazio, N.; Giammarile, F.; Hicks, R.; Kjaer, A.; et al. ENETS Consensus Guidelines for the Standards of Care in Neuroendocrine Tumors: Radiological, Nuclear Medicine and Hybrid Imaging. Neuroendocrinology 2017, 105, 212–244. [Google Scholar] [CrossRef] [PubMed]
- Jin, X.-F.; Spampatti, M.P.; Spitzweg, C.; Auernhammer, C.J. Supportive therapy in gastroenteropancreatic neuroendocrine tumors: Often forgotten but important. Rev. Endocr. Metab. Disord. 2018, 19, 145–158. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Carbonero, R.; Sorbye, H.; Baudin, E.; Raymond, E.; Wiedenmann, B.; Niederle, B.; Sedlackova, E.; Toumpanakis, C.; Anlauf, M.; Cwikla, J.; et al. Consensus Guidelines for High Grade Gastro-Entero-Pancreatic (GEP) Neuroendocrine Tumours and Neuroendocrine Carcinomas (NEC). Neuroendocrinology 2016, 103, 186–194. [Google Scholar] [CrossRef]
- Cavalcanti, M.S.; Gönen, M.; Klimstra, D.S. The ENETS/WHO grading system for neuroendocrine neoplasms of the gastroenteropancreatic system: A review of the current state, limitations and proposals for modifications. Int. J. Endocr. Oncol. 2016, 3, 203–219. [Google Scholar] [CrossRef]
- Niederle, B.; Pape, U.-F.; Costa, F.; Gross, D.; Kelestimur, F.; Knigge, U.; Öberg, K.; Pavel, M.; Perren, A.; Toumpanakis, C.; et al. ENETS Consensus Guidelines Update for Neuroendocrine Neoplasms of the Jejunum and Ileum. Neuroendocrinology 2016, 103, 125–138. [Google Scholar] [CrossRef]
- Inzani, F.; Petrone, G.; Rindi, G. The New World Health Organization Classification for Pancreatic Neuroendocrine Neoplasia. Endocrinol. Metab. Clin. N. Am. 2018, 47, 463–470. [Google Scholar] [CrossRef]
- Ito, T.; Igarashi, H.; Uehara, H.; Berna, M.J.; Jensen, R.T. Causes of Death and Prognostic Factors in Multiple Endocrine Neoplasia Type 1. Medicine 2013, 92, 135–181. [Google Scholar] [CrossRef]
- Kos-Kudła, B.; Blicharz-Dorniak, J.; Strzelczyk, J.; Bałdys-Waligórska, A.; Bednarczuk, T.; Bolanowski, M.; Boratyn-Nowicka, A.; Borowska, M.; Cichocki, A.; Cwikla, J.; et al. Diagnostic and therapeutic guidelines for gastro-entero-pancreatic neuroendocrine neoplasms (recommended by the Polish Network of Neuroendocrine Tumours). Endokrynol Pol. 2017, 68, 79–110. [Google Scholar] [CrossRef]
- Modrzejewski, A.; Śledź, M.; Chęciński, P.; Parafiniuk, M.; Pawlik, A.; Kurzawski, M.; Czerny, B. Carcinoid tumor of the gallbladder: Laparoscopic resection and review of the literature. Videosurgery and other miniinvasive techniques. Surgery 2009, 4, 72–75. [Google Scholar]
- Yao, J.C.; Hassan, M.; Phan, A.; Dagohoy, C.; Leary, C.; Mares, J.E.; Abdalla, E.K.; Fleming, J.B.; Vauthey, J.-N.; Rashid, A.; et al. One Hundred Years After “Carcinoid”: Epidemiology of and Prognostic Factors for Neuroendocrine Tumors in 35,825 Cases in the United States. J. Clin. Oncol. 2008, 26, 3063–3072. [Google Scholar] [CrossRef] [PubMed]
- Pandit, S.; Bhusal, K. Carcinoid Syndrome. In StatPearls [Internet]; 2018. Available online: https://www.ncbi.nlm.nih.gov/books/NBK448096/ (accessed on 1 January 2020).
- Bhattacharya, S. Risk factors for the development and progression of carcinoid heart disease. Am. J. Cardiol. 2011, 107, 1221–1226. [Google Scholar] [CrossRef] [PubMed]
- Sagar, V.M.; Cooper, S.C.; Johnson, J.; Shetty, S.; Shah, T. Gastrointestinal manifestations of neuroendocrine tumours: Their investigation and management. Postgrad. Med. J. 2017, 93, 494–497. [Google Scholar] [CrossRef] [PubMed]
- Gierach, M.; Gierach, J.; Skowrońska, A.; Junik, R. Neuroendocrine tumors—Insulinoma in clinical practice. Postępy Nauk Med. 2013, 12, 906–909. [Google Scholar]
- Epelboym, I.; Mazeh, H. Zollinger-Ellison Syndrome: Classical Considerations and Current Controversies. Oncologist 2013, 19, 44–50. [Google Scholar] [CrossRef]
- Cingam, S.R.; Karanchi, H. Gastrinoma. Copyright© 2018, StatPearls Publishing LLC. Available online: https://www.ncbi.nlm.nih.gov/books/NBK441842/ (accessed on 1 January 2020).
- Sandhu, S.; Jialal, I. VIPoma. Copyright© 2018, StatPearls Publishing LLC. Available online: https://www.ncbi.nlm.nih.gov/books/NBK507698/ (accessed on 1 January 2020).
- John, A.; Schwartz, R.A. Glucagonoma syndrome: A review and update on treatment. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 2016–2022. [Google Scholar] [CrossRef]
- Vinink, A.; Pacak, K.; Feliberti, E.; Perry, R.R. Glucagonoma Syndrome. Copyright 2000–2018, MDText.com, Inc. Available online: https://www.ncbi.nlm.nih.gov/books/NBK279041/ (accessed on 1 January 2020).
- Vinik, A.; Pacak, K.; Feliberti, E.; Perry, R.R. Somatostatinoma. Copyright 2000-2018, MDText.com, Inc. Available online: https://www.ncbi.nlm.nih.gov/books/NBK279034/ (accessed on 1 January 2020).
- Garbrecht, N.; Anlauf, M.; Schmitt, A.; Henopp, T.; Sipos, B.; Raffel, A.; Eisenberger, C.F.; Knoefel, W.T.; Pavel, M.; Fottner, C.; et al. Somatostatin-producing neuroendocrine tumors of the duodenum and pancreas: Incidence, types, biological behavior, association with inherited syndromes, and functional activity. Endocr. Relat. Cancer 2008, 15, 229–241. [Google Scholar] [CrossRef]
- Falconi, M.; Eriksson, B.; Kaltsas, G.; Bartsch, D.; Capdevila, J.; Caplin, M.; Kos-Kudła, B.; Kwekkeboom, D.; Rindi, G.; Kloppel, G.; et al. ENETS Consensus Guidelines Update for the Management of Patients with Functional Pancreatic Neuroendocrine Tumors and Non-Functional Pancreatic Neuroendocrine Tumors. Neuroendocrinology 2016, 103, 153–171. [Google Scholar] [CrossRef]
- Coriat, R.; Walter, T.; Terris, B.; Couvelard, A.; Ruszniewski, P. Gastroenteropancreatic Well-Differentiated Grade 3 Neuroendocrine Tumors: Review and Position Statement. Oncologist 2016, 21, 1191–1199. [Google Scholar] [CrossRef]
- Watzka, F.M.; Fottner, C.; Miederer, M.; Weber, M.M.; Schad, A.; Lang, H.; Musholt, T.J. Surgical Treatment of NEN of Small Bowel: A Retrospective Analysis. World J. Surg. 2016, 40, 749–758. [Google Scholar] [CrossRef]
- Jiang, S.-H.; Li, J.; Dong, F.; Yang, J.-Y.; Liu, D.-J.; Yang, X.; Wang, Y.-H.; Yang, M.; Fu, X.; Zhang, X.-X.; et al. Increased Serotonin Signaling Contributes to the Warburg Effect in Pancreatic Tumor Cells Under Metabolic Stress and Promotes Growth of Pancreatic Tumors in Mice. Gastroenterology 2017, 153, 277–291.e19. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.S.; Caplin, E.M. Therapeutic management of patients with gastroenteropancreatic neuroendocrine tumours. Endocr. Relat. Cancer 2011, 18, S53–S74. [Google Scholar] [CrossRef] [PubMed]
- Appetecchia, M.; Baldelli, R. Somatostatin analogues in the treatment of gastroenteropancreatic neuroendocrine tumours, current aspects and new perspectives. J. Exp. Clin. Cancer Res. 2010, 29, 19. [Google Scholar] [CrossRef] [PubMed]
- Rinke, A.; Müller, H.-H.; Schade-Brittinger, C.; Klose, K.-J.; Barth, P.; Wied, M.; Mayer, C.; Aminossadati, B.; Pape, U.-F.; Bläker, M.; et al. Placebo-Controlled, Double-Blind, Prospective, Randomized Study on the Effect of Octreotide LAR in the Control of Tumor Growth in Patients With Metastatic Neuroendocrine Midgut Tumors: A Report From the PROMID Study Group. J. Clin. Oncol. 2009, 27, 4656–4663. [Google Scholar] [CrossRef]
- Caplin, M.E.; Pavel, M.; Cwikla, J.; Phan, A.T.; Raderer, M.; Sedlackova, E.; Cadiot, G.; Wolin, E.M.; Capdevila, J.; Wall, L.; et al. Lanreotide in Metastatic Enteropancreatic Neuroendocrine Tumors. N. Engl. J. Med. 2014, 371, 224–233. [Google Scholar] [CrossRef]
- Faivre, S.; Djelloul, S.; Raymond, E. New Paradigms in Anticancer Therapy: Targeting Multiple Signaling Pathways With Kinase Inhibitors. Semin. Oncol. 2006, 33, 407–420. [Google Scholar] [CrossRef]
- Uri, I.; Avniel-Polak, S.; Gross, D.J.; Grozinsky-Glasberg, S. Update in the Therapy of Advanced Neuroendocrine Tumors. Curr. Treat. Options Oncol. 2017, 18, 72. [Google Scholar] [CrossRef]
- Bednarczuk, T.; Bolanowski, M.; Zemczak, A.; Bałdys-Waligórska, A.; Blicharz-Dorniak, J.; Boratyn-Nowicka, A.; Borowska, M.; Cichocki, A.; Ćwikła, J.B.; Falconi, M.; et al. Neuroendocrine neoplasms of the small intestine and appendicitis - principles of conduct (recommended by the Polish Neuroendocrine Tumor Network). Endokrynol. Pol. 2013, 64, 480–493. [Google Scholar]
- Yao, J.C.; Fazio, N.; Singh, S.; Buzzoni, R.; Carnaghi, C.; Wolin, E.; Tomasek, J.; Raderer, M.; Lahner, H.; Voi, M.; et al. Everolimus for the treatment of advanced, non-functional neuroendocrine tumours of the lung or gastrointestinal tract (RADIANT-4): A randomised, placebo-controlled, phase 3 study. Lancet 2015, 387, 968–977. [Google Scholar] [CrossRef]
- Grillo, F.; Florio, T.; Ferraù, F.; Kara, E.; Fanciulli, G.; Faggiano, A.; Colao, A.A.L. Emerging multitarget tyrosine kinase inhibitors in the treatment of neuroendocrine neoplasms. Endocr. Relat. Cancer 2018, 25, R453–R466. [Google Scholar] [CrossRef]
- Raymond, E.; Dahan, L.; Raoul, J.-L.; Bang, Y.-J.; Borbath, I.; Lombard-Bohas, C.; Valle, J.W.; Metrakos, P.; Smisth, D.; Vinik, A.; et al. Sunitinib Malate for the Treatment of Pancreatic Neuroendocrine Tumors. N. Engl. J. Med. 2011, 364, 501–513. [Google Scholar] [CrossRef] [PubMed]
- Pavel, E.M.; Gross, D.J.; Benavent, M.; Perros, P.; Srirajaskanthan, R.; Warner, R.R.P.; Kulke, M.H.; Anthony, L.B.; Kunz, P.L.; Horsch, D.; et al. Telotristat ethyl in carcinoid syndrome: Safety and efficacy in the TELECAST phase 3 trial. Endocr.-Relat. Cancer 2018, 25, 309–322. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.C.; Pavel, M.; Lombard-Bohas, C.; Van Cutsem, E.; Voi, M.; Brandt, U.; He, W.; Chen, D.; Capdevila, J.; De Vries, E.G.; et al. Everolimus for the Treatment of Advanced Pancreatic Neuroendocrine Tumors: Overall Survival and Circulating Biomarkers From the Randomized, Phase III RADIANT-3 Study. J. Clin. Oncol. 2016, 34, 3906–3913. [Google Scholar] [CrossRef]
- Saif, M.W.; Kaley, K.; Brennan, M.; Garcon, M.C.; Rodriguez, G.; Rodriguez, T. A retrospective study of capecitabine/temozolomide (CAPTEM) regimen in the treatment of metastatic pancreatic neuroendocrine tumors (pNETs) afer failing previous therapy. J. Pancreas 2013, 14, 498–501. [Google Scholar]
- Sahu, A.; Jefford, M.; Lai-Kwon, J.; Thai, A.; Hicks, R.J.; Michael, M. CAPTEM in Metastatic Well-Differentiated Intermediate to High Grade Neuroendocrine Tumors: A Single Centre Experience. J. Oncol. 2019, 2019, 9032753. [Google Scholar] [CrossRef]
- Pavel, M.; O’Toole, D.; Costa, F.; Capdevila, J.; Gross, D.; Kianmanesh, R.; Krenning, E.; Knigge, U.; Salazar, R.; Pape, U.-F.; et al. ENETS Consensus Guidelines Update for the Management of Distant Metastatic Disease of Intestinal, Pancreatic, Bronchial Neuroendocrine Neoplasms (NEN) and NEN of Unknown Primary Site. Neuroendocrinology 2016, 103, 172–185. [Google Scholar] [CrossRef]
- Kaderli, R.M.; Spanjol, M.; Kollár, A.; Bütikofer, L.; Gloy, V.; Dumont, R.A.; Seiler, C.A.; Christ, E.R.; Radojewski, P.; Briel, M.; et al. Therapeutic Options for Neuroendocrine Tumors. JAMA Oncol. 2019, 5, 480. [Google Scholar] [CrossRef]
- Liu, T.; Liao, J.; Dang, J.; Li, G. Treatments for patients with advanced neuroendocrine tumors: A network meta-analysis. Ther. Adv. Med. Oncol. 2019, 11. [Google Scholar] [CrossRef]
- Berardi, R.; Rinaldi, S.; Torniai, M.; Morgese, F.; Partelli, S.; Caramanti, M.; Onofri, A.; Polenta, V.; Pagliaretta, S.; Falconi, M.; et al. Gastrointestinal neuroendocrine tumors: Searching the optimal treatment strategy—A literature review. Crit. Rev. Oncol. 2016, 98, 264–274. [Google Scholar] [CrossRef]
- Shachar, S.S.; Williams, G.R. The Obesity Paradox in Cancer-Moving Beyond BMI. Cancer Epidemiol. Biomark. Prev. 2017, 26, 13–16. [Google Scholar] [CrossRef]
- Sharpless, N.E.; DePinho, R.A. p53: Good cop/bad cop. Cell 2002, 110, 9–12. [Google Scholar] [CrossRef]
- Fontana, L.; Klein, S. Aging, Adiposity, and Calorie Restriction. JAMA 2007, 297, 986. [Google Scholar] [CrossRef] [PubMed]
- Surh, Y.-J. Cancer chemoprevention with dietary phytochemicals. Nat. Rev. Cancer 2003, 3, 768–780. [Google Scholar] [CrossRef] [PubMed]
- Go, V.; Srihari, P.; Burns, L.A.K. Nutrition and Gastroenteropancreatic Neuroendocrine Tumors. Endocrinol. Metab. Clin. N. Am. 2010, 39, 827–837. [Google Scholar] [CrossRef]
- Barrea, L.; Altieri, B.; Muscogiuri, G.; Laudisio, D.; Annunziata, G.; Colao, A.; Faggiano, A.; Savastano, S. Impact of Nutritional Status on Gastroenteropancreatic Neuroendocrine Tumors (GEP-NET) Aggressiveness. Nutrients 2018, 10, 1854. [Google Scholar] [CrossRef]
- Wang, X.; Ouyang, Y.; Liu, J.; Zhu, M.; Zhao, G.; Bao, W.; Hu, F.B. Fruit and vegetable consumption and mortality from all causes, cardiovascular disease, and cancer: Systematic review and dose-response meta-analysis of prospective cohort studies. BMJ 2014, 349, g4490. [Google Scholar] [CrossRef]
- De Pergola, G.; Silvestris, F. Obesity as a Major Risk Factor for Cancer. J. Obes. 2013, 2013, 1–11. [Google Scholar] [CrossRef]
- Herrera-Martínez, A.D.; Hofland, J.; Hofland, L.J.; Brabander, T.; Eskens, F.A.L.M.; Moreno, M.A.G.; Luque, R.M.; Castaño, J.P.; De Herder, W.W.; Feelders, R.A. Targeted Systemic Treatment of Neuroendocrine Tumors: Current Options and Future Perspectives. Drugs 2018, 79, 21–42. [Google Scholar] [CrossRef]
- Altieri, B.; Barrea, L.; Modica, R.; Muscogiuri, G.; Savastano, S.; Colao, A.; Faggiano, A. Nutrition and neuroendocrine tumors: An update of the literature. Rev. Endocr. Metab. Disord. 2018, 19, 159–167. [Google Scholar] [CrossRef]
- Longo, V.D.; Fontana, L. Calorie restriction and cancer prevention: Metabolic and molecular mechanisms. Trends Pharmacol. Sci. 2010, 31, 89–98. [Google Scholar] [CrossRef]
- Turati, F.; Rossi, M.; Pelucchi, C.; Levi, F.; La Vecchia, C. Fruit and vegetables and cancer risk: A review of southern European studies. Br. J. Nutr. 2015, 113, S102–S110. [Google Scholar] [CrossRef] [PubMed]
- Promotion. USDoHaHSOoDPaH. 2015–2020 Dietary Guidelines for Americans. Available online: https://health.gov/dietaryguidelines/?_ga=2.93506781.1509651194.1526503567-2137365160.1526503567 (accessed on 1 January 2020).
- Blanchard, C.M.; Courneya, K.S.; Stein, K. Cancer Survivors’ Adherence to Lifestyle Behavior Recommendations and Associations With Health-Related Quality of Life: Results From the American Cancer Society’s SCS-II. J. Clin. Oncol. 2008, 26, 2198–2204. [Google Scholar] [CrossRef] [PubMed]
- Dietary Guidelines Advisory Committee; US Department of Health and Human Services; US Department of Agriculture. Dietary Guidelines for Americans 2005; US Government Printing Office: Washington, DC, USA, 2005.
- Özoğul, F.; Hamed, I. The importance of lactic acid bacteria for the prevention of bacterial growth and their biogenic amines formation: A review. Crit. Rev. Food Sci. Nutr. 2017, 58, 1660–1670. [Google Scholar] [CrossRef] [PubMed]
- Jiang, W.; Xu, Y.; Li, C.; Dong, X.; Wang, N. Biogenic amines in commercially produced Yulu, a Chinese fermented fish sauce. Food Addit. Contam. Part B 2013, 7, 25–29. [Google Scholar] [CrossRef]
- Fan, P.; Song, P.; Li, L.; Huang, C.; Chen, J.; Yang, W.; Qiao, S.; Wu, G.; Zhang, G.; Ma, X. Roles of Biogenic Amines in Intestinal Signaling. Curr. Protein Pept. Sci. 2017, 18, 532–540. [Google Scholar] [CrossRef]
- Tuberoso, C.; Serreli, G.; Montoro, P.; D’Urso, G.; Congiu, F.; Kowalczyk, A. Biogenic amines and other polar compounds in long aged oxidized Vernaccia di Oristano white wines. Food Res. Int. 2018, 111, 97–103. [Google Scholar] [CrossRef]
- Martin, I.S.M.; Brachero, S.; Vilar, E.G. Histamine intolerance and dietary management: A complete review. Allergol. Immunopathol. 2016, 44, 475–483. [Google Scholar] [CrossRef]
- Wüthrich, B. Allergic and intolerance reactions to wine. Allergol. Sel. 2018, 2, 80–88. [Google Scholar] [CrossRef]
- Riederer, P.; Müller, T. Use of monoamine oxidase inhibitors in chronic neurodegeneration. Expert Opin. Drug Metab. Toxicol. 2017, 13, 233–240. [Google Scholar] [CrossRef]
- Schink, M.; Konturek, P.C.; Tietz, E.; Dieterich, W.; Pinzer, T.C.; Wirtz, S.; Neurath, M.F.; Zopf, Y. Microbial Patterns in Patients with Histamine Intolerance. J. Physiol. Pharmacol. 2018, 69, 579–593. [Google Scholar]
- Latorre-Moratalla, M.; Comas-Basté, O.; Bover-Cid, S.; Vidal-Carou, M.C. Tyramine and histamine risk assessment related to consumption of dry fermented sausages by the Spanish population. Food Chem. Toxicol. 2017, 99, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Ercan, S.Ş.; Bozkurt, H.; Soysal, Ç. Significance of Biogenic Amines in Foods and Their Reduction Methods. J. Food Sci. Eng. 2013, 3, 395–410. [Google Scholar] [CrossRef]
- Franke, G.; Cwiková, O. Biogenic amines in smear ripened cheeses. Potravin. Slovak J. Food Sci. 2019, 13, 378–384. [Google Scholar] [CrossRef]
- Naraev, B.G.; Halland, M.; Halperin, D.M.; Purvis, A.J.; O’dorisioT, M.; Halfdanarson, T.R. Management of Diarrhea in Patients With Carcinoid Syndrome. Pancreas 2019, 48, 961–972. [Google Scholar] [CrossRef]
- Clement, D.S.V.M.; Tesselaar, M.E.T.; E Van Leerdam, M.; Srirajaskanthan, R.; Ramage, J. Nutritional and vitamin status in patients with neuroendocrine neoplasms. World J. Gastroenterol. 2019, 25, 1171–1184. [Google Scholar] [CrossRef]
- Laing, E.; Kiss, N.; Michael, M.; Gough, K.; Krishnasamy, M.; Whyand, T.; Auer, B. Investigating Nutrition-Related Complications and Quality of Life in Patients With Gastroenteropancreatic Neuroendocrine Tumors: Protocol for a Mixed-Methods Prospective Study. JMIR Res. Protoc. 2018, 7, e11228. [Google Scholar] [CrossRef]
- Hutton, J.L.; Martin, L.; Field, C.J.; Wismer, W.V.; Bruera, E.D.; Watanabe, S.M.; Baracos, V.E. Dietary patterns in patients with advanced cancer: Implications for anorexia-cachexia therapy. Am. J. Clin. Nutr. 2006, 84, 1163–1170. [Google Scholar] [CrossRef]
- Shaw, C.; Taylor, L. Treatment-Related Diarrhea in Patients with Cancer. Clin. J. Oncol. Nurs. 2012, 16, 413–417. [Google Scholar] [CrossRef]
- Jones, L.W.; Demark-Wahnefried, W. Diet, exercise, and complementary therapies after primary treatment for cancer. Lancet Oncol. 2006, 7, 1017–1026. [Google Scholar] [CrossRef]
- Paris, S.; García, M.; Trufero, M.; Sorrosal, L.; Gracia, C.; Alaminos, L.; Sanz-París, A.; Martinez-García, M.; Trufero, J.M.; Lambea, J.; et al. Oligomeric Enteral Nutrition in Undernutrition, due to Oncology Treatment-Related Diarrhea. Systematic Review and Proposal of An Algorithm of Action. Nutrients 2019, 11, 1888. [Google Scholar] [CrossRef]
- Thompson, K.L.; Elliott, L.; Fuchs-Tarlovsky, V.; Levin, R.; Voss, A.C.; Piemonte, T. Oncology Evidence-Based Nutrition Practice Guideline for Adults. J. Acad. Nutr. Diet. 2017, 117, 297–310.e47. [Google Scholar] [CrossRef] [PubMed]
- Wedlake, L.J.; Shaw, C.; Whelan, K.; Andreyev, H.J.N. Systematic review: The efficacy of nutritional interventions to counteract acute gastrointestinal toxicity during therapeutic pelvic radiotherapy. Aliment. Pharmacol. Ther. 2013, 37, 1046–1056. [Google Scholar] [CrossRef] [PubMed]
- Mardas, M.; Madry, R.; Stelmach-Mardas, M. Link between diet and chemotherapy related gastrointestinal side effects. Contemp. Oncol. 2017, 21, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Grabenbauer, G.G.; Holger, G. Management of radiation and chemotherapy related acute toxicity in gastrointestinal cancer. Best Pract. Res. Clin. Gastroenterol. 2016, 30, 655–664. [Google Scholar] [CrossRef] [PubMed]
- De Hosson, L.D.; Stelwagen, J.; Bouma, G.; Sijtema, B.; Huitema, S.; Van Faassen, H.J.R.; De Bock, G.H.; A De Groot, D.J.; E Campmans-Kuijpers, M.J.; Kema, I.P.; et al. Towards optimal personalized diet and vitamin supplementation in NET patients. Endocr. Relat. Cancer 2018, 25, L23–L26. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.R.; Lee, J.H.; Lee, J.H.; Na, G.Y.; Lee, K.-H.; Lee, Y.-B.; Jung, G.-H.; Kim, O.Y. Low-FODMAP formula improves diarrhea and nutritional status in hospitalized patients receiving enteral nutrition: A randomized, multicenter, double-blind clinical trial. Nutr. J. 2015, 14, 116. [Google Scholar] [CrossRef] [PubMed]
- Gibson, R.; Keefe, D.M.K. Cancer chemotherapy-induced diarrhoea and constipation: Mechanisms of damage and prevention strategies. Support. Care Cancer 2006, 14, 890–900. [Google Scholar] [CrossRef]
- Vandeputte, D.; Falony, G.; Vieira-Silva, S.; Wang, J.; Sailer, M.; Theis, S.; Verbeke, K.; Raes, J. Prebiotic inulin-type fructans induce specific changes in the human gut microbiota. Gut 2017, 66, 1968–1974. [Google Scholar] [CrossRef]
- Riezzo, G.; Orlando, A.; D’Attoma, B.; Linsalata, M.; Martulli, M.; Russo, F. Randomised double blind placebo controlled trial on Lactobacillus reuteri DSM 17938: Improvement in symptoms and bowel habit in functional constipation. Benef. Microbes 2018, 9, 51–60. [Google Scholar] [CrossRef]
- Wołkowicz, T.; Januszkiewicz, A.; Szych, J. Microbiome of the digestive tract and its dysbiosis as an important factor affecting the health condition of the human body. Med. Dośw. Mikrobiol. 2014, 66, 223–235. [Google Scholar]
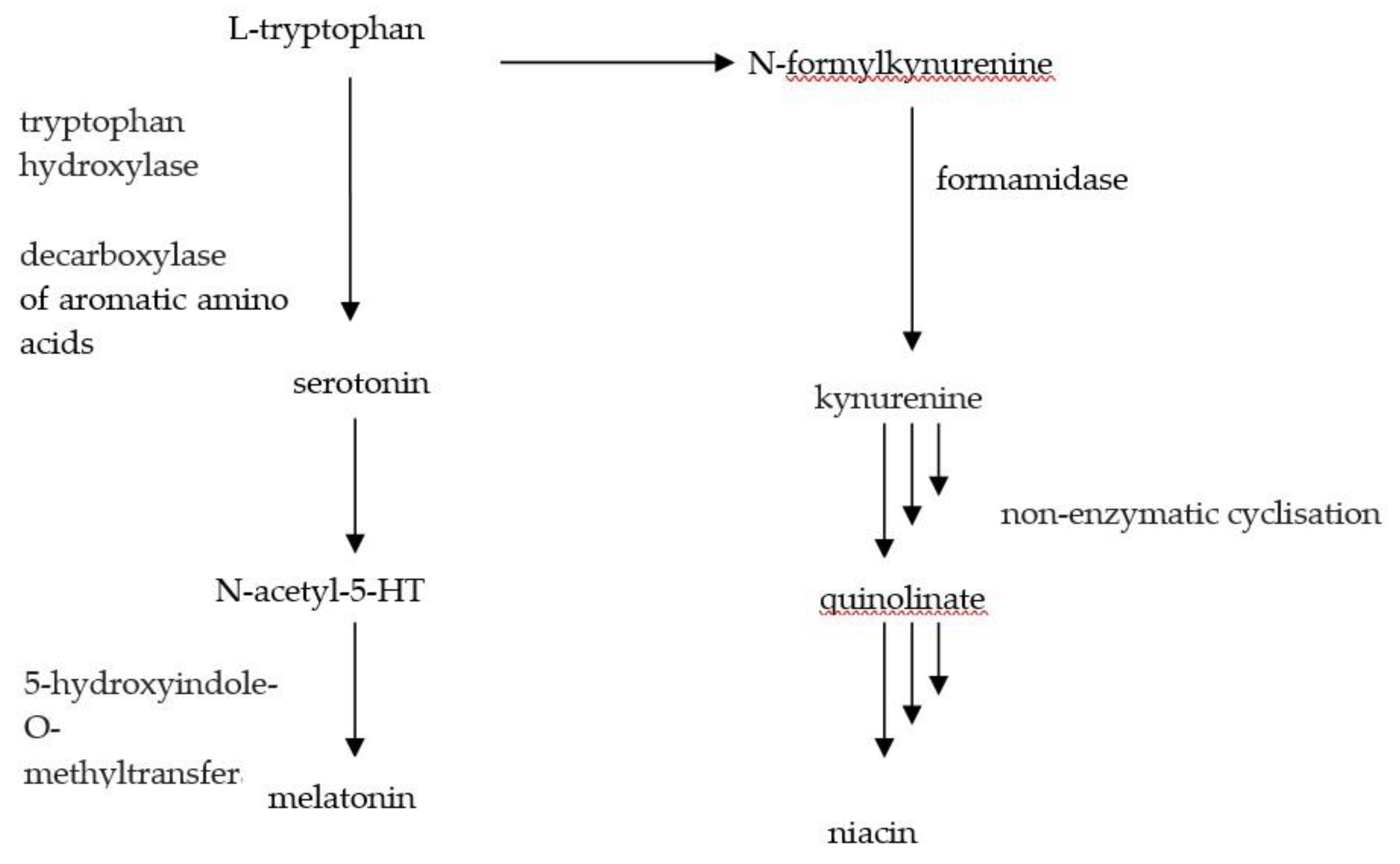
- Bouma, G.; van Faassen, M.; Kats-Ugurlu, G.; Vries de, E.G.E.; Kema, I.P.; Walenkamp, A.M.E. Niacin (Vitamin B-3) supplementation in patients with serotonin-producing neuroendocrine tumor. Neuroendocrinology 2016, 103, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Shah, G.M.; Shah, R.G.; Veillette, H.; Kirkland, J.B.; Pasieka, J.L.; Warner, R.R.P. Biochemical Assessment of Niacin Deficiency Among Carcinoid Cancer Patients. Am. J. Gastroenterol. 2005, 100, 2307–2314. [Google Scholar] [CrossRef] [PubMed]
- Brennan, G.T.; Saif, M.W. Pancreatic Enzyme Replacement Therapy: A Concise Review. J. Pancreas 2019, 20, 126–129. [Google Scholar]
- Qureshi, S.A.; Burch, N.; Druce, M.; Hattersley, A.; Khan, S.; Gopalakrishnan, K.; Darby, C.; Wong, J.L.H.; Davies, L.; Fletcher, S.; et al. Screening for malnutrition in patients with gastro-entero-pancreatic neuroendocrine tumours: A cross-sectional study. BMJ Open 2016, 6, e010765. [Google Scholar] [CrossRef] [PubMed]
- Arends, J.; Bodoky, G.; Bozzetti, F.; Fearon, K.; Muscaritoli, M.; Selga, G.; Schueren, M.V.B.-D.V.D.; Von Meyenfeldt, M.; Zürcher, G.; Fietkau, R.; et al. ESPEN Guidelines on Enteral Nutrition: Non-surgical oncology. Clin. Nutr. 2006, 25, 245–259. [Google Scholar] [CrossRef]
- Elting, L.S.; Cooksley, C.; Chambers, M.; Cantor, S.B.; Manzullo, E.; Rubenstein, E.B. The burdens of cancer therapy. Cancer 2003, 98, 1531–1539. [Google Scholar] [CrossRef]
- Borre, M.; Dam, G.A.; Knudsen, A.W.; Grønbæk, H. Nutritional status and nutritional risk in patients with neuroendocrine tumors. Scand. J. Gastroenterol. 2018, 53, 284–292. [Google Scholar] [CrossRef]
- Robbins, H.L.; Symington, M.; Mosterman, B.; Goodby, J.; Davies, L.; Dimitriadis, G.K.; Kaltsas, G.A.; Randeva, H.S.; Weickert, M.O. Supplementation of Vitamin D Deficiency in Patients with Neuroendocrine Tumors Using Over-the-Counter Vitamin D3 Preparations. Nutr. Cancer 2018, 70, 748–754. [Google Scholar] [CrossRef]
- Lavriv, D.S.; Neves, P.; Ravasco, P. Should omega-3 fatty acids be used for adjuvant treatment of cancer cachexia? Clin. Nutr. ESPEN 2018, 25, 18–25. [Google Scholar] [CrossRef]
- Keshet, R.; Erez, A. Arginine and the metabolic regulation of nitric oxide synthesis in cancer. Dis. Model. Mech. 2018, 11, dmm033332. [Google Scholar] [CrossRef]
- Maasberg, S.; Knappe-Drzikova, B.; Vonderbeck, D.; Jann, H.; Weylandt, K.; Grieser, C.; Pascher, A.; Schefold, J.C.; Pavel, M.; Wiedenmann, B.; et al. Malnutrition Predicts Clinical Outcome in Patients with Neuroendocrine Neoplasia. Neuroendocrinology 2015, 104, 11–25. [Google Scholar] [CrossRef] [PubMed]
- Lamarca, A.; McCallum, L.; Nuttall, C.; Barriuso, J.; Backen, A.; Frizziero, M.; Leon, R.; Mansoor, W.; McNamara, M.G.; Hubner, R.A.; et al. Somatostatin analogue-induced pancreatic exocrine insufficiency in patients with neuroendocrine tumors: Results of a prospective observational study. Expert Rev. Gastroenterol. Hepatol. 2018, 12, 723–731. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| (A) Proposed dietary care solutions for patients with NEN according to the patient’s nutritional status (BMI). | ||
| Nutritional status (BMI) | Symptoms | Dietary care solutions |
| >30 Obesity, visceral fat accumulation | No persistent bothersome symptoms | Anti-neoplastic diet (based on the high quantity and diversity of plant products) or Mediterranean and additionally reduction diet [69,70,71,74,75,76,77,78,79] Regular physical activity adjusted to the patient’s capabilities [77,78,79]. |
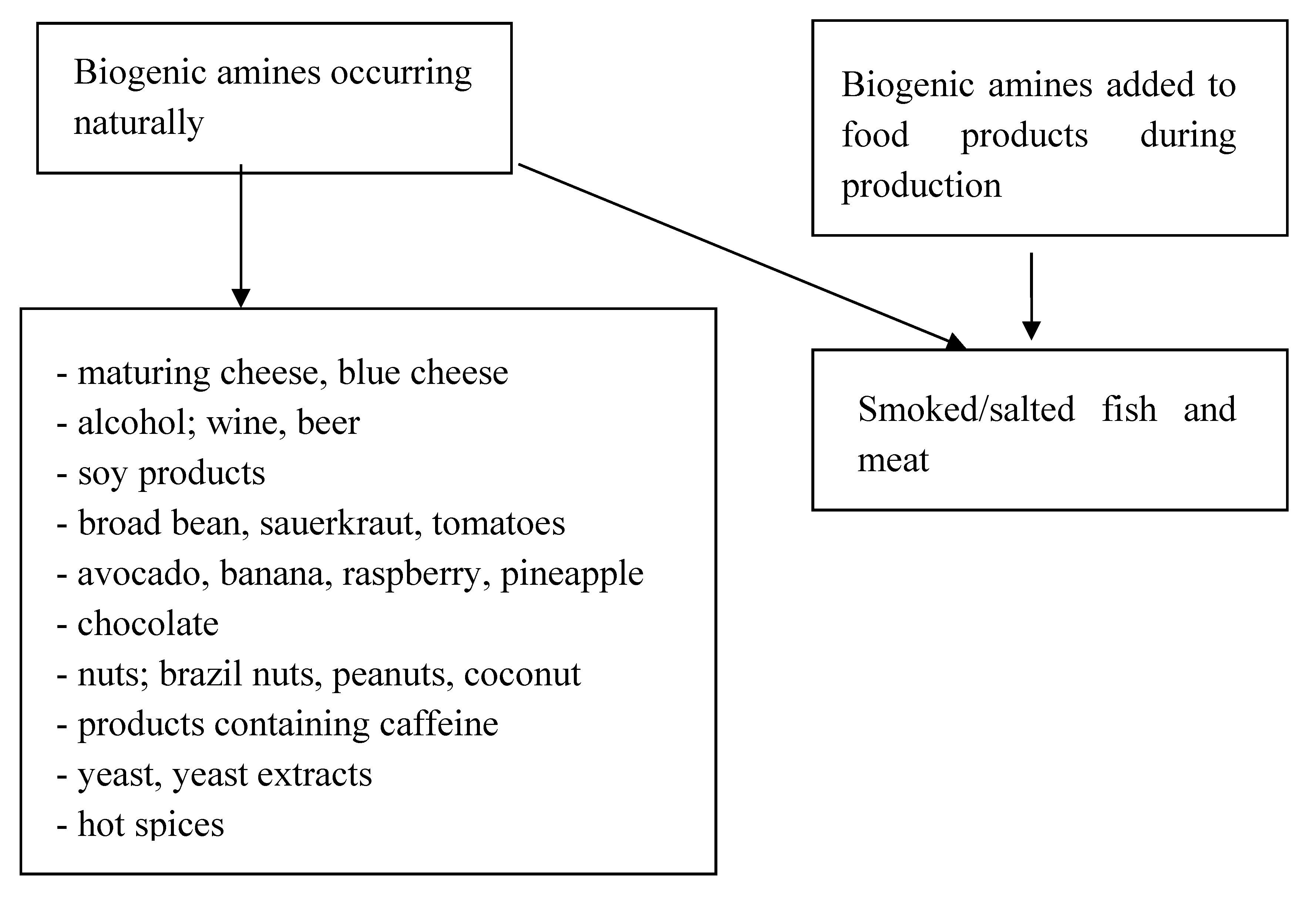
| Severe diarrhea with progressing reduction of body mass | Consider supplementation, especially with omega 3 [94,116]; diet that includes a reduced amount of fiber, legumes and brassicas until symptoms decline [15,80,94]; Elimination of biogenic amines [87,88,92]; Electrolyte supplementation [91]; Potassium supplementation (hypokalemia) [15]; Avoid hot, very spicy, fatty and large meal portions [66]; Consume meals that include proteins, mainly lean poultry, cottage cheese, eggs and yoghurt; Carbohydrates: rice and finely ground oats, pumpkin, carrot, bananas, apples [66]; Exclude lactose, saccharose, fructose and glucose [15,66,93]. | |
| Constipation | Anti-neoplastic, Mediterranean diet [69,70,71,74,75,76,77,78,79] high in fiber with inulin [15,102], consider probiotics therapy: Lactobacillus acidophilus and Bifidobacterium lactis [106]; Increased supply of liquids (mineral water with lemon, aloe, additionally drank in the morning) [34]; Regular physical activity, physiotherapeutic massage [74,75,76]. | |
| Disturbed carbohydrate metabolism | Low glycemic index diet with limited amounts of fruit (glucose, fructose, saccharose), supplemented with MUFA and PUFA [66,67,68,69,70,71,72,73,117]; Regular physical activity [77,78,79]. | |
| * 26–29.9 overweight Visceral Fat accumulation <26 | No chronic, irritating symptoms | Anti-neoplastic, Mediterranean diet. Perhaps consider a reduction diet if the patient’s diet did not decrease recently due to the intense course of the disease [69,70,71,74,75,76,77,78,79]; Regular physical activity [77,78,79]. |
| Irritating diarrhea with progressing reduction of body mass | Procedures the same as in the case of diarrhea >30 BMI. | |
| Constipation | Procedures the same as in the case of constipation >30 BMI. | |
| Disturbed carbohydrate metabolism | Procedures the same as in the case of disturbed carbohydrate metabolism >30 BMI. | |
| 26–22/23 ** | No chronic, irritating symptoms | Anti-neoplastic, Mediterranean diet according to needs of the body [69,70,71,74,75,76,77,78,79] Regular physical activity [77,78,79]. |
| Irritating diarrhea with progressing reduction of body mass | Procedures the same as in the case of diarrhea >30 BMI. | |
| Constipation | Procedures the same as in the case of constipation >30 BMI. | |
| Disturbed carbohydrate metabolism | Procedures the same as in the case of disturbed carbohydrate metabolism >30 BMI. | |
| <22/23 ** At the risk of malnutrition | No chronic, irritating symptoms | Anti-neoplastic, Mediterranean diet [69,70,71,74,75,76,77,78,79] Stimulation of tissue reconstruction, e.g., through the incorporation of industrial diet preparations that additionally feature arginine [117]. |
| Irritating diarrhea with progressing reduction of body mass | Incorporation of oligomeric formula of enteral nutrition in patients with diarrhea and progressing malnutrition [97,98]; Potentially–full parenteral nutrition [101]; Diets with reduced osmolarity [100]; Electrolyte supplementation [91]; Incorporate multi-element supplementation that includes omega-3 [95]. | |
| Cachexia | Enteral nutrition and parenteral nutrition, omega-3 supplementation [102], multi-element supplementation [89,95]. | |
| (B) Proposed solutions for the dietary care of patients with NEN taking into account NEN hormone activity | ||
| NEN | Symptoms | Nutrition |
| Carcinoid | Increased metabolism of tryptophan into serotonin/spastic diarrhea | Supplementation of niacin deficiency (vitamin PP), supplementation 25–50 mg/day [16]; Include the consumption of fish, meat, bran and the seeds of legumes [106,107]; Regular physical activity after the earlier analysis of the heart using echocardiography [72]. |
| Gastrinoma | Increased gastric acid synthesis and inactivation of pancreatic enzymes. Disorders of digestion and/or absorption of fatty acids = fatty diarrhea | Consume meals that include fats, mainly lean poultry, cottage cheese, eggs and yoghurt; Carbohydrates: rice and finely ground oats, pumpkin, carrot, bananas, apples; Limit fats or include pancreas enzymes’ substitution [88,89]; Regular physical activity [72]. |
| Somatostatinoma | Inhibition of the exocrine pancreatic function/steatorrhea | Procedures the same as in the case of gastrinoma. |
| Vipoma | Water and electrolyte secretion by the digestive tract and inhibition of stomach acid secretion/secretory diarrhea | Special care for hydration and electrolyte management [91]. |
| Glucagonoma | Disturbed carbohydrate metabolism; glucagon overproduction; impaired fasting glucose/impaired glucose tolerance/diabetes | Low glycemic index diet with the limitation of fruit; Prevention of long fasts between meals during the night break; Regular physical activity [72]. |
| Insulinoma | Disturbed carbohydrate metabolism insulin overproduction/hypoglicemia | In the case of frequent hypoglycemia in insulinoma, the supply of carbohydrates with a high glycemic index, e.g., fruit juice [34,35,36,37,38,39,40,41]; Prevention of long fasts between meals during the night break. |
| (C) Sample pharmacotherapy of NEN patients taking into account interactions with food | ||
| Medicine | Influence | Food |
| Everolimus, sunitinib [66] | P450 (CYP) 3A4 inhibition | Exclude for the diet: grapefruit, camomile, cranberry, garlic, ginseng, green tea extract, pepper, resveratrol and soy |
| Sorafenib | Inhibitors of tyrosine kinase | High fat meals |
| Capecytabine | is unstable under strongly acidic conditions | should be administered with a meal (up to 30 min after a meal) |
| Temozolomide [66] | CYP P450 inhibition through stomach pH | Not to be supplied together with food (on empty stomach) |
| Long-acting somatostatin analogues [110,119] | Exocrine pancreatic insufficiency | Include the substitution of pancreatic enzymes |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pobłocki, J.; Jasińska, A.; Syrenicz, A.; Andrysiak-Mamos, E.; Szczuko, M. The Neuroendocrine Neoplasms of the Digestive Tract: Diagnosis, Treatment and Nutrition. Nutrients 2020, 12, 1437. https://doi.org/10.3390/nu12051437
Pobłocki J, Jasińska A, Syrenicz A, Andrysiak-Mamos E, Szczuko M. The Neuroendocrine Neoplasms of the Digestive Tract: Diagnosis, Treatment and Nutrition. Nutrients. 2020; 12(5):1437. https://doi.org/10.3390/nu12051437
Chicago/Turabian StylePobłocki, Jakub, Anna Jasińska, Anhelli Syrenicz, Elżbieta Andrysiak-Mamos, and Małgorzata Szczuko. 2020. "The Neuroendocrine Neoplasms of the Digestive Tract: Diagnosis, Treatment and Nutrition" Nutrients 12, no. 5: 1437. https://doi.org/10.3390/nu12051437
APA StylePobłocki, J., Jasińska, A., Syrenicz, A., Andrysiak-Mamos, E., & Szczuko, M. (2020). The Neuroendocrine Neoplasms of the Digestive Tract: Diagnosis, Treatment and Nutrition. Nutrients, 12(5), 1437. https://doi.org/10.3390/nu12051437