Impact of Crocus sativus L. on Metabolic Profile in Patients with Diabetes Mellitus or Metabolic Syndrome: A Systematic Review


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
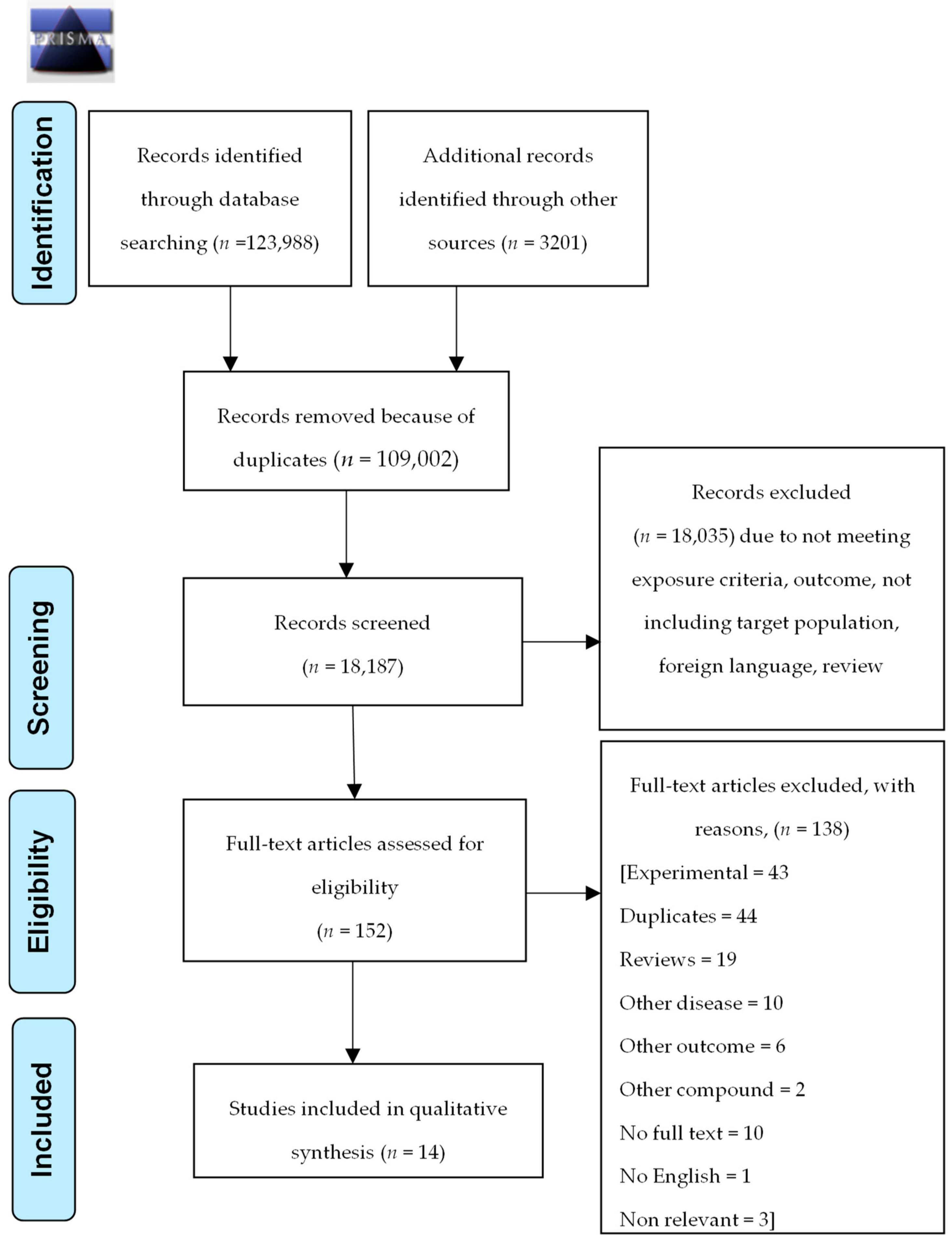
2.1. Literature Search Strategy
2.2. Types of Studies and Eligibility Criteria
2.3. Data Collection and Extraction
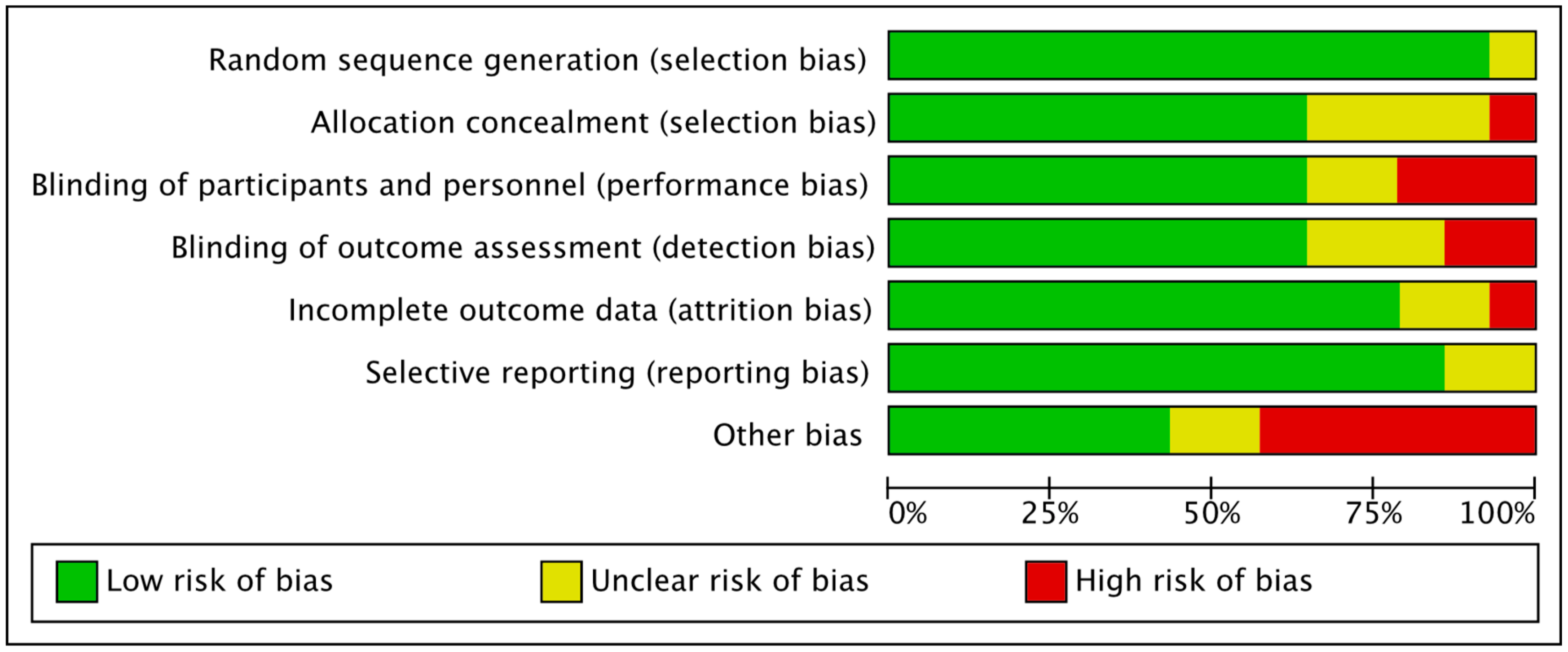
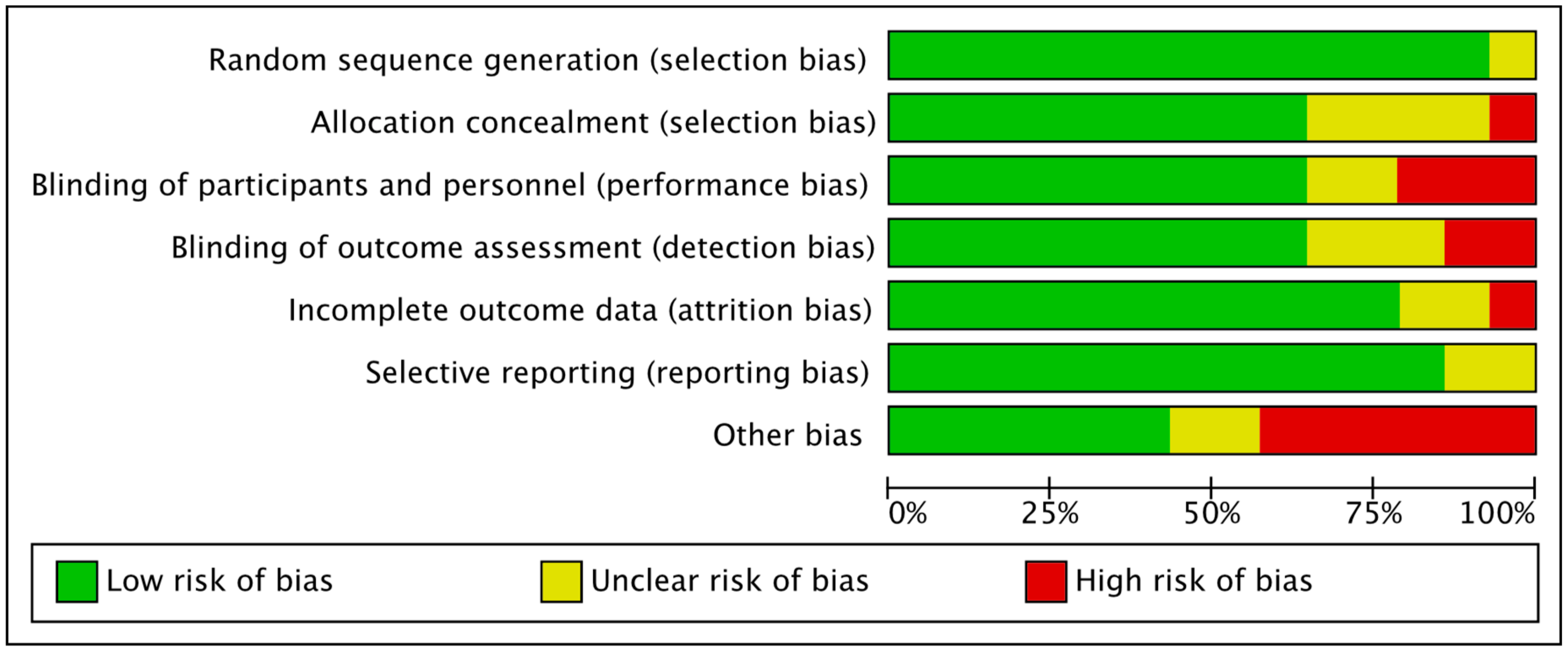
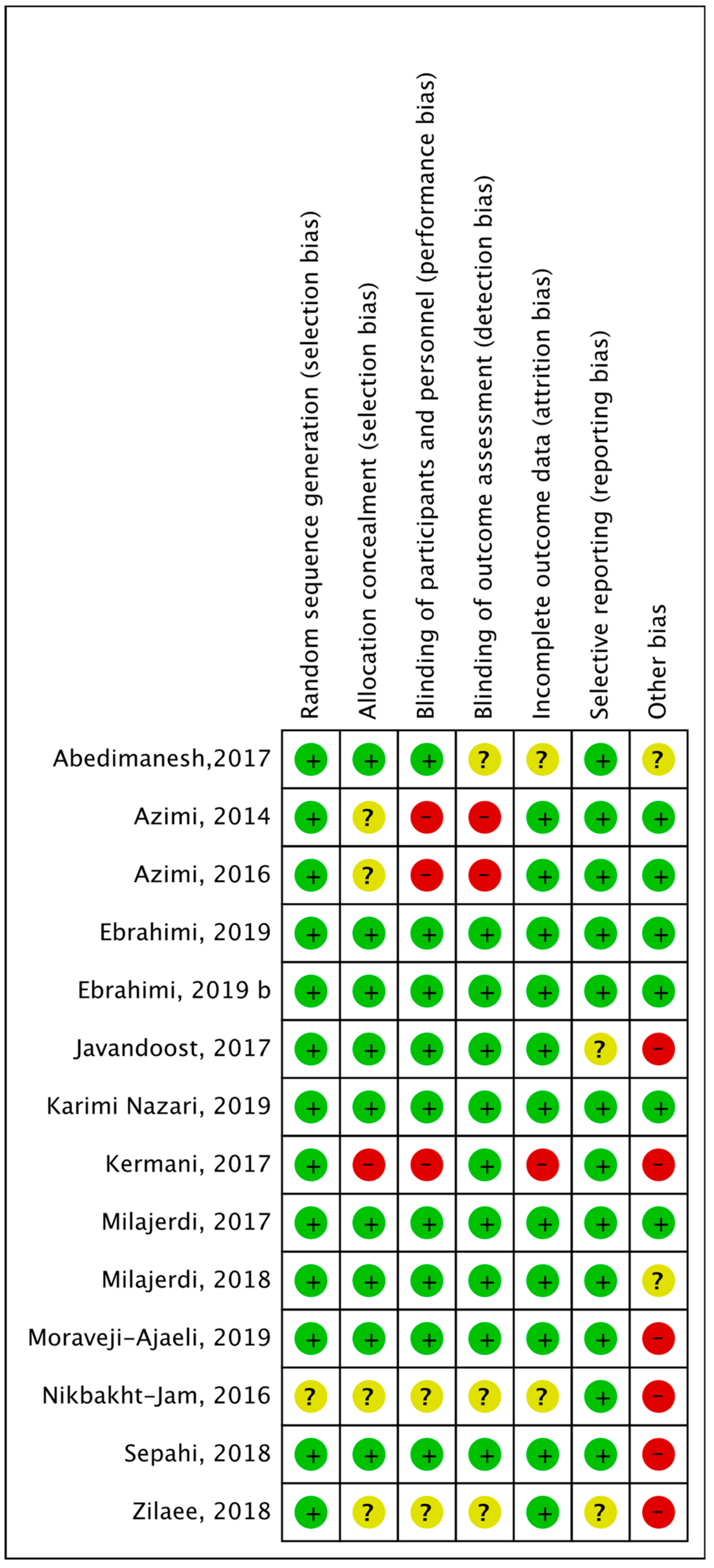
2.4. Study Quality and Risk of Bias Assessment in Included Studies
2.5. Data Synthesis and Analysis
3. Results
3.1. Characteristics of the Studies Included in the Review
3.2. Risk of Bias Assessment
3.3. Glycemic Control
3.4. Lipid Profile
3.5. Other Components of Metabolic Syndrome (MS)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AGEs | advanced glycation end product |
| PPARa | peroxisome proliferator-activated receptor alpha |
| BP | blood pressure |
| CK | creatine kinase |
| DM | Diabetes mellitus |
| FBG | fasting blood glucose |
| HbA1c | Glycatedhaemoglobin |
| HDL-C | high-density cholesterol |
| LDH | levels of lactate dehydrogenase |
| LDL-C | low-density cholesterol |
| MDA | malondialdehyde |
| MS | metabolic syndrome |
| NO | nitric oxide |
| TG | triglycerides |
| SOD | superoxide dismutase |
| t-chol | total serum cholesterol |
| WC | waist circumference |
References
- Didangelos, T.; Karamitsos, D. Chronic diabetic complications. In Diabetologia, Theory and Practice in the Treatment of Diabetes Mellitus, 2nd ed.; Karamitsos, D., Ed.; Siokis, Medical and Scientific Publications: Athens, Greece, 2009; Volume 1, pp. 429–535. [Google Scholar]
- Calcutt, N.A.; Cooper, M.E.; Kern, T.S.; Schmidt, A.M. Therapies for hyperglycaemia-induced diabetic complications: From animal models to clinical trials. Nat. Rev. Drug Discov. 2009, 8, 417–430. [Google Scholar] [CrossRef]
- Trisha, D. Preiodontal disease, the overlooked the diabetes complication. Nephrol. Nurs. J. 2009, 36, 489–495. [Google Scholar]
- Brownlee, M. A radical explanation for glucose-induced β cell dysfunction. J. Clin. Investig. 2003, 112, 1788–1790. [Google Scholar] [CrossRef]
- Seino, Y.; Ueno, S.; Yabe, D.; Suzuki, A. Dietary recommendations for type 2 diabetes patients: Lessons from recent clinical and basic research in Asia. J. Diabetes Investig. 2019, 10, 1405–1407. [Google Scholar] [CrossRef] [PubMed]
- Melnyk, J.P.; Wang, S.; Marcone, M.F. Chemical and biological properties of the world’s most expensive spice: Saffron. Food Res. Int. 2010, 43, 1981–1989. [Google Scholar] [CrossRef]
- Christodoulou, E.; Kadoglou, N.P.; Kostomitsopoulos, N.; Valsami, G. Saffron: A natural product with potential pharmaceutical applications. J. Pharm. Pharmacol. 2015, 67, 1634–1649. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Betti, G.; Hensel, A. Saffron in phytotherapy: Pharmacology and clinical uses. Wien. Med. Wochenschr. 2007, 157, 315. [Google Scholar] [CrossRef]
- Arasteh, A.; Aliyev, A.; Khamnei, S.; Delazar, A.; Mesgari, M.; Mehmannavaz, Y. Crocus sativus on serum glucose, insulin and cholesterol levels in healthy male rats. J. Med. Plants Res. 2010, 4, 397–402. [Google Scholar]
- Shirali, S.; Zahra Bathaie, S.; Nakhjavani, M. Effect of Crocin on the Insulin Resistance and Lipid Profile of Streptozotocin-Induced Diabetic Rats. Phytother. Res. 2013, 27, 1042–1047. [Google Scholar] [CrossRef]
- Rajaei, Z.; Hadjzadeh, M.-A.-R.; Nemati, H.; Hosseini, M.; Ahmadi, M.; Shafiee, S. Antihyperglycemic and Antioxidant Activity of Crocin in Streptozotocin-Induced Diabetic Rats. J. Med. Food 2013, 16, 206–210. [Google Scholar] [CrossRef]
- Asri-Rezaei, S.; Tamaddonfard, E.; Ghasemsoltani-Momtaz, B.; Erfanparast, A.; Gholamalipour, S. Effects of crocin and zinc chloride on blood levels of zinc and metabolic and oxidative parameters in streptozotocin-induced diabetic rats. Avicenna J. Phytomed. 2015, 5, 403–412. [Google Scholar] [PubMed]
- Kianbakht, S.; Hajiaghaee, R. Anti-hyperglycemic Effects of Saffron and its Active Constituents, Crocin and Safranal, in Alloxan-Induced Diabetic Rats. J. Med. Plants 2011, 3, 82–89. [Google Scholar]
- Mohajeri, D.; Mousavi, G.; Doustar, Y. Antihyperglycemic and pancreas-protective effects of Crocus sativus L. (saffron) stigma-ethanolic extract on rats with alloxan-induced diabetes. Sci. Alert 2009, 9, 302–310. [Google Scholar] [CrossRef] [Green Version]
- Kang, C.; Lee, H.; Jung, E.-S.; Seyedian, R.; Jo, M.; Kim, J.; Kim, J.-S.; Kim, E. Saffron (Crocus sativus L.) increases glucose uptake and insulin sensitivity in muscle cells via multipathway mechanisms. Food Chem. 2012, 135, 2350–2358. [Google Scholar] [CrossRef] [PubMed]
- Maeda, A.; Kai, K.; Ishii, M.; Ishii, T.; Akagawa, M. Safranal, a novel protein tyrosine phosphatase 1B inhibitor, activates insulin signaling in C2C12 myotubes and improves glucose tolerance in diabetic KK-Ay mice. Mol. Nutr. Food Res. 2014, 58, 1177–1189. [Google Scholar] [CrossRef] [PubMed]
- Xi, L.; Qian, Z.; Xu, G.; Zheng, S.; Sun, S.; Wen, N.; Sheng, L.; Shi, Y.; Zhang, Y. Beneficial impact of crocetin, a carotenoid from saffron, on insulin sensitivity in fructose-fed rats. J. Nutr. Biochem. 2007, 18, 64–72. [Google Scholar] [CrossRef]
- Lee, I.-A.; Lee, J.H.; Baek, N.-I.; Kim, D.-H. Antihyperlipidemic Effect of Crocin Isolated from the Fructus of Gardenia jasminoides and Its Metabolite Crocetin. Biol. Pharm. Bull. 2005, 28, 2106–2110. [Google Scholar] [CrossRef] [Green Version]
- Sheng, L.; Qian, Z.; Zheng, S.; Xi, L. Mechanism of hypolipidemic effect of crocin in rats: Crocin inhibits pancreatic lipase. Eur. J. Pharmacol. 2006, 543, 116–122. [Google Scholar] [CrossRef]
- Xu, G.-L.; Yu, S.-Q.; Gong, Z.-N.; Zhang, S.-Q. Study of the effect of crocin on rat experimental hyperlipemia and the underlying mechanisms. Zhongguo Zhong Yao Za Zhi 2005, 30, 369–372. [Google Scholar]
- Lee, I.-A.; Min, S.-W.; Kim, D. Lactic acid bacteria increases hypolipidemic effect of crocin isolated from fructus of Gardenia jasminoides. J. Microbiol. Biotechnol. 2006, 16, 1084–1089. [Google Scholar]
- Mashmoul, M.; Azlan, A.; Yusof, B.N.M.; Khaza’ai, H.; Mohtarrudin, N.; Boroushaki, M.T. Effects of saffron extract and crocin on anthropometrical, nutritional and lipid profile parameters of rats fed a high fat diet. J. Funct. Foods 2014, 8, 180–187. [Google Scholar] [CrossRef]
- Samarghandian, S.; Azimi-Nezhad, M.; Samini, F. Ameliorative Effect of Saffron Aqueous Extract on Hyperglycemia, Hyperlipidemia, and Oxidative Stress on Diabetic Encephalopathy in Streptozotocin Induced Experimental Diabetes Mellitus. BioMed Res. Int. 2014, 2014, 112, 920857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abe, K.; Saito, H. Effects of saffron extract and its constituent crocin on learning behaviour and long-term potentiation. Phytother. Res. 2000, 14, 149–152. [Google Scholar] [CrossRef]
- Imenshahidi, M.; Razavi, B.M.; Faal, A.; Gholampoor, A.; Mousavi, S.M.; Hosseinzadeh, H. Effects of chronic crocin treatment on desoxycorticosterone acetate (doca)-salt hypertensive rats. Iran. J. Basic Med. Sci. 2014, 17, 9–13. [Google Scholar]
- Imenshahidi, M.; Razavi, M.; Faal, A.; Gholampoor, A.; Mousavi, S.; Hosseinzadeh, H. The effect of chronic administration of safranal on systolic blood pressure in rats. Iran. J. Pharm. Res. 2015, 14, 585–590. [Google Scholar] [CrossRef]
- Imenshahidi, M.; Razavi, B.M.; Faal, A.; Gholampoor, A.; Mousavi, S.M.; Hosseinzadeh, H. The effect of chronic administration of saffron (Crocus sativus) stigma aqueous extract on systolic blood pressure in rats. Jundishapur J. Nat. Pharm. Prod. 2013, 8, 175–179. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Qian, Z. Effects of crocin on cholestane-3beta-5alpha-6beta-triol induced apoptosis and related gene expression of cultured endothelial cells. J. China Pharm. Univ. 2005, 36, 254. [Google Scholar]
- Xu, G.; Gong, Z.; Yu, W.; Gao, L.; He, S.; Qian, Z. Increased Expression Ratio of Bcl-2/Bax Is Associated with Crocin-Mediated Apoptosis in Bovine Aortic Endothelial Cells. Basic Clin. Pharmacol. Toxicol. 2007, 100, 31–35. [Google Scholar] [CrossRef]
- Xu, G.-L.; Qian, Z.-Y.; Yu, S.-Q.; Gong, Z.-N.; Shen, X.-C. Evidence of crocin against endothelial injury induced by hydrogen peroxide in vitro. J. Asian Nat. Prod. Res. 2006, 8, 79–85. [Google Scholar] [CrossRef]
- Ma, S.; Liu, B.; Zhou, S.; Xu, X.; Yang, Q.; Zhou, J. Pharmacological studies of glycosides of saffron crocus (Crocus sativus).II.Effects on blood coagulation, platelet aggregation and thromobosis. Zhong Cao Yao 1999, 30, 196–198. [Google Scholar]
- He, S.-Y.; Qian, Z.-Y.; Tang, F.-T.; Wen, N.; Xu, G.-L.; Sheng, L. Effect of crocin on experimental atherosclerosis in quails and its mechanisms. Life Sci. 2005, 77, 907–921. [Google Scholar] [CrossRef] [PubMed]
- He, S.-Y.; Qian, Z.-Y.; Wen, N.; Tang, F.-T.; Xu, G.-L.; Zhou, C.-H. Influence of crocetin on experimental atherosclerosis in hyperlipidamic-diet quails. Eur. J. Pharmacol. 2007, 554, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Khori, V.; Rakhshan, E.; Mirabbas, A. A study of the role of nitric oxide in the mechanism of action of hydroalcoholic extract of saffron (Crocus sativus) on the electrophysiological properties of the rabbit atrioventricular node. In Proceedings of the II International Symposium on Saffron Biology and Technology, Masshad, Iran, 28–30 October 2016; pp. 351–358. [Google Scholar]
- Boskabady, M.H.; Shafei, M.N.; Shakiba, A.; Sefidi, H.S. Effect of aqueous-ethanol extract from Crocus sativus (saffron) on guinea-pig isolated heart. Phytother. Res. 2008, 22, 330–334. [Google Scholar] [CrossRef] [PubMed]
- Du, P.; Qian, Z.Y.; Shen, X.C.; Rao, S.Y.; Wen, N. Effectiveness of crocin against myocardial injury. Chin. New Drugs J. 2005, 14, 1424. [Google Scholar]
- Zhang, R.; Zhi-Yu, Q.; Xiao-Yuan, H.; Zhen, C.; Jun-Ling, Y.; Hamid, A. Comparison of the effects of crocetin and crocin on myocardial injury in rats. Chin. J. Nat. Med. 2009, 7, 223–227. [Google Scholar] [CrossRef]
- Goyal, S.N.; Arora, S.; Sharma, A.K.; Joshi, S.; Ray, R.; Bhatia, J.; Kumari, S.; Arya, D.S. Preventive effect of crocin of Crocus sativus on hemodynamic, biochemical, histopathological and ultrastuctural alterations in isoproterenol-induced cardiotoxicity in rats. Phytomedicine 2010, 17, 227–232. [Google Scholar] [CrossRef]
- EElsherbiny, N.M.; Salama, M.F.; Said, E.; El-Sherbiny, M.; Al-Gayyar, M.M. Crocin protects against doxorubicin-induced myocardial toxicity in rats through down-regulation of inflammatory and apoptic pathways. Chem. Biol. Interact. 2016, 247, 39–48. [Google Scholar] [CrossRef]
- Farshid, A.A.; Tamaddonfard, E.; Moradi-Arzeloo, M.; Mirzakhani, N. The effects of crocin, insulin and their co-administration on the heart function and pathology in streptozotocin-induced diabetic rats. Avicenna J. Phytomed. 2016, 6, 658–670. [Google Scholar]
- Feidantsis, K.; Mellidis, K.; Galatou, E.; Sinakos, Z.; Lazou, A. Treatment with crocin improves cardiac dysfunction by normalizing autophagy and inhibiting apoptosis in STZ-induced diabetic cardiomyopathy. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 952–961. [Google Scholar] [CrossRef]
- Cai, J.; Yi, F.F.; Bian, Z.Y.; Shen, D.F.; Yang, L.; Yan, L.; Tang, Q.-Z.; Yang, X.-C.; Li, H. Crocetin protects against cardiac hypertrophy by blocking MEK-ERK1/2 signalling pathway. J. Cell. Mol. Med. 2009, 13, 909–925. [Google Scholar] [CrossRef] [Green Version]
- Didangelos, T.; Doupis, J.; Veves, A. Oxidative Stress in Diabetes Mellitus and Possible Interventions. In Studies in Diabetes; Obrosova, I., Stevens, M.J., Yorek, M.A., Eds.; Springer New York: New York, NY, USA, 2014; pp. 237–261. [Google Scholar]
- Azimi, P.; Ghiasvand, R.; Feizi, A.; Hariri, M.; Abbasi, B. Effects of cinnamon, cardamom, saffron, and ginger consumption on markers of glycemic control, lipid profile, oxidative stress, and inflammation in type 2 diabetes patients. Rev. Diabet. Stud. RDS 2014, 11, 258–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azimi, P.; Ghiasvand, R.; Feizi, A.; Hosseinzadeh, J.; Bahreynian, M.; Hariri, M.; Khosravi-Boroujeni, H. Effect of cinnamon, cardamom, saffron and ginger consumption on blood pressure and a marker of endothelial function in patients with type 2 diabetes mellitus: A randomized controlled clinical trial. Blood Press. 2016, 25, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi, F.; Aryaeian, N.; Pahlavani, N.; Abbasi, D.; Hosseini, A.F.; Fallah, S.; Moradi, N.; Heydari, I. The effect of saffron (Crocus sativus L.) supplementation on blood pressure, and renal and liver function in patients with type 2 diabetes mellitus: A double-blinded, randomized clinical trial. Avicenna J. Phytomed. 2019, 9, 322–333. [Google Scholar] [PubMed]
- Ebrahimi, F.; Sahebkar, A.; Aryaeian, N.; Pahlavani, N.; Fallah, S.; Moradi, N.; Abbas, D.; Hosseini, A.F. Effects of saffron supplementation on inflammation and metabolic responses in type 2 diabetic patients: A randomized, double-blind, placebo-controlled trial. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 2107–2115. [Google Scholar] [CrossRef] [Green Version]
- Milajerdi, A.; Jazayeri, S.; Bitarafan, V.; Hashemzadeh, N.; Shirzadi, E.; Derakhshan, Z.; Mahmoodi, M.; Rayati, A.; Djazayeri, A.; Akhondzadeh, S. The effect of saffron (Crocus sativus L.) hydro-alcoholic extract on liver and renal functions in type 2 diabetic patients: A double-blinded randomized and placebo control trial. J. Nutr. Intermed. Metab. 2017, 9, 6–11. [Google Scholar] [CrossRef]
- Milajerdi, A.; Jazayeri, S.; Hashemzadeh, N.; Shirzadi, E.; Derakhshan, Z.; Djazayeri, A.; Akhondzadeh, S. The effect of saffron (Crocus sativus L.) hydroalcoholic extract on metabolic control in type 2 diabetes mellitus: A triple-blinded randomized clinical trial. J. Res. Med Sci. 2018, 23, 16. [Google Scholar] [CrossRef]
- Moravej Aleali, A.; Amani, R.; Shahbazian, H.; Namjooyan, F.; Latifi, S.M.; Cheraghian, B. The effect of hydroalcoholic Saffron (Crocus sativus L.) extract on fasting plasma glucose, HbA1c, lipid profile, liver, and renal function tests in patients with type 2 diabetes mellitus: A randomized double-blind clinical trial. Phytother. Res. 2019, 33, 1648–1657. [Google Scholar] [CrossRef]
- Sepahi, S.; Mohajeri, S.A.; Hosseini, S.M.; Khodaverdi, E.; Shoeibi, N.; Namdari, M.; Tabassi SA, S. Effects of Crocin on diabetic maculopathy: A placebo-controlled randomized clinical trial. Am. J. Ophthalmol. 2018, 190, 89–98. [Google Scholar] [CrossRef]
- Javandoost, A.; Afshari, A.; Nikbakht-Jam, I.; Khademi, M.; Eslami, S.; Nosrati, M.; Foroutan-Tanha, M.; Sahebkar, A.; Tavalaie, S.; Ghayour-Mobarhan, M.; et al. Effect of crocin, a carotenoid from saffron, on plasma cholesteryl ester transfer protein and lipid profile in subjects with metabolic syndrome: A double blind randomized clinical trial. ARYA Atheroscler. 2017, 13, 245–252. [Google Scholar]
- Kermani, T.; Kazemi, T.; Molki, S.; Ilkhani, K.; Sharifzadeh, G.; Rajabi, O. The efficacy of crocin of saffron (Crocus sativus L.) on the components of metabolic syndrome: A randomized controlled clinical trial. J. Res. Pharm. Pract. 2017, 6, 228–232. [Google Scholar]
- Nikbakht-Jam, I.; Khademi, M.; Nosrati, M.; Eslami, S.; Foroutan-Tanha, M.; Sahebkar, A.; Tavalaie, S.; Ghayour-Mobarhan, M.; Ferns, G.A.A.; Hadizadeh, F.; et al. Effect of crocin extracted from saffron on pro-oxidant–anti-oxidant balance in subjects with metabolic syndrome: A randomized, placebo-controlled clinical trial. Eur. J. Integr. Med. 2016, 8, 307–312. [Google Scholar] [CrossRef]
- Zilaee, M.; Soukhtanloo, M.; Ghayour-Mobarhan, M.; Shemshian, M.; Salehi, M.; Ferns, G.A. Effect of saffron on serum leptin levels in patients with metabolic syndrome, a double-blind, randomized and placebo-controlled trial study. Prog. Nutr. 2018, 20, 140–144. [Google Scholar]
- Karimi-Nazari, E.; Nadjarzadeh, A.; Masoumi, R.; Marzban, A.; Mohajeri, S.A.; Ramezani-Jolfaie, N.; Salehi-Abargouei, A. Effect of saffron (Crocus sativus L.) on lipid profile, glycemic indices and antioxidant status among overweight/obese prediabetic individuals: A double-blinded, randomized controlled trial. Clin. Nutr. ESPEN 2019, 34, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Abedimanesh, N.; Bathaie, S.Z.; Abedimanesh, S.; Motlagh, B.; Separham, A.; Ostadrahimi, A. Saffron and crocin improved appetite, dietary intakes and body composition in patients with coronary artery disease. J. Cardiovasc. Thorac. Res. 2017, 9, 200–208. [Google Scholar] [CrossRef] [Green Version]
- Gout, B.; Bourges, C.; Paineau-Dubreuil, S. Satiereal, a Crocus sativus L. extract, reduces snacking and increases satiety in a randomized placebo-controlled study of mildly overweight, healthy women. Nutr. Res. 2010, 30, 305–313. [Google Scholar] [CrossRef]
- Pourmasoumi, M.; Hadi, A.; Najafgholizadeh, A.; Kafeshani, M.; Sahebkar, A. Clinical evidence on the effects of saffron (Crocus sativus L.) on cardiovascular risk factors: A systematic review meta-analysis. Pharmacol. Res. 2019, 139, 348–359. [Google Scholar] [CrossRef]
- Alavizadeh, S.H.; Hosseinzadeh, H. Bioactivity assessment and toxicity of crocin: A comprehensive review. Food Chem. Toxicol. 2014, 64, 65–80. [Google Scholar] [CrossRef]
- Razavi, B.M.; Hosseinzadeh, H. Saffron: A promising natural medicine in the treatment of metabolic syndrome. J. Sci. Food Agric. 2017, 97, 1679–1685. [Google Scholar] [CrossRef]
- Tome-Carneiro, J.; Visioli, F. Polyphenol-based nutraceuticals for the prevention and treatment of cardiovascular disease: Review of human evidence. Phytomedicine 2016, 23, 1145–1174. [Google Scholar] [CrossRef]
- Bjelakovic, G.; Nikolova, D.; Gluud, L.L.; Simonetti, R.G.; Gluud, C. Mortality in randomized trials of antioxidant supplements for primary and secondary prevention: Systematic review and meta-analysis. JAMA 2007, 297, 842–857. [Google Scholar] [CrossRef]
- Moyer, M.W. The myth of antioxidants. Sci. Am. 2013, 308, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Yabe, D.; Seino, Y.; Fukushima, M.; Seino, S. β cell dysfunction versus insulin resistance in the pathogenesis of type 2 diabetes in East Asians. Curr. Diabetes Rep. 2015, 15, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Study (Year) | Sample | Gender (Males) | Age (Years) | Study Design | Condition | Intervention/Groups | Duration | Outcome | Assessment of Diet | Assessment of Physical Activity |
|---|---|---|---|---|---|---|---|---|---|---|
| Abedimanesh 2017 [57] | 75 | 14/13/12 | 56.04 ± 7.55 53.36 ± 5.94 56.32 ± 5.91 | Randomized Double blind placebo controlled | Coronary artery disease (17% DM) | Saffron aqueous extract (30 mg) vs. Crocin (30 mg) vs. Placebo | 8 weeks | FBG, t-chol, HDL-c, LDL-c, TG, WC | Yes | No |
| Azimi 2014 [44] | 208 | 17/16/15/16/15 | 54.33 ± 0.5 | Parallel Randomized Single Blind Placebo controlled | DM-2 | 3 gl of Black tea + 3 g cardamom vs. 3 gl black tea + 3 g cinnamon 3 gl Black tea + 3 g ginger vs. 3 gl black tea + 1 g saffron vs. 3 gl black tea (control) | 8 weeks | FBG, t-chol, TG, LDL-c, HDL-c, HbA1c, | Yes | Yes |
| Azimi 2016 [45] | 208 | 17/16/15/16/15 | 54.33 ± 0.5 | Parallel Randomized Single Blind Placebo controlled | DM-2 | 3 gl of black tea + 3 g cardamom vs. 3 gl black tea + 3 g cinnamon vs. 3 gl black tea + 3 g ginger vs. 3 gl black tea + 1 g saffron vs. 3 gl black tea (control) | 8 weeks | WC, SBP, DBP | Yes | Yes |
| Ebrahimi 2019 [46] | 90 | 36 | 55.2 ± 7.3 53 ± 10.6 | Prospective DoubleBlind Placebo Controlled Randomized | DM-2 | Saffron 100 mg vs. placebo 100 mg maltodextrin | 12 weeks | SBP, DBP | Yes | Yes |
| Ebrahimi 2019b [47] | 90 | 36 | 55.2 ± 7.3 53 ± 10.6 | Prospective Double Blind Placebo Controlled Randomized | DM-2 | Saffron 100 mg vs. placebo 100 mg maltodextrin | 12 weeks | FBG, HbA1c, TG, t-chol, HDL-c, LDL-c, WC | Yes | Yes |
| Javandoost 2017 [52] | 44 | 18 | 44.50 (24.75–51.50) 33.10 (29.85–35.42) | Double blind randomized placebo controlled | MS | 30 mg crocin vs. placebo | 8 weeks | FBG, TG, HDL-c, LDL-c, t-chol | No | No |
| Karimi Nazari2019 [56] | 80 | 27 | 57.95 ± 8.18 57.9 ± 8.7 | Double blind randomized placebo controlled | Prediabetes | 15 mg saffron vs. placebo | 8 weeks | FBG, TG, HDL-c, LDL-c, t-chol | Yes | Yes |
| Kermani 2017 [53] | 48 | 7 | 53.8 ± 9.2 50.9 ± 8.8 | Double blind Randomized placebo controlled | MS | 100 mg crocin vs. placebo | 6 weeks | FBG, TG, HDL-c, LDL-c, t-chol, SBP, DBP, WC | No | No |
| Milajerdi 2017 [48] | 54 | 12 | 54.57 ± 6.96 55.42 ± 7.58 | Double blind Randomized placebo controlled | DM-2 | 30 mg saffron vs. placebo | 8 weeks | WC, SBP, DBP (does not report full data) | Yes | Yes |
| Milajerdi 2018 [49] | 54 | 12 | 54.57 ± 6.96 55.42 ± 7.58 | Triple blind randomized placebo controlled | DM-2 | 30 mg saffron vs. placebo | 8 weeks | FBG, t-chol, TG, HDL-c, LDL-c, HbA1c | Yes | Yes |
| Moravej Aleali 2019 [50] | 64 | 19 | 52.4 ± 13 53.5 ± 9.9 | Double blind Randomized placebo controlled | DM-2 | 30 mg saffron vs. placebo | 3 months | FBG, t-chol, TG, HDL-c, LDL-c, HbA1c, | Yes | No |
| Nikbakht-Jam 2016 [54] | 60 | 25 | 38.97 ± 13.33 43.46 ± 12.77 | Double blind Randomized placebo controlled | MS (DM 16%) | 30 mg crocin vs. placebo | 8 weeks | FBG, t-chol, TG, HDL-c, LDL | No | No |
| Zilaee 2018 [55] | 76 | 9 | 42.19 ± 11.52 43.60 ± 9.05 | Double blind Randomized placebo controlled | MS | 100 mg saffron vs. placebo | 12 weeks | LDL-c, HDL-c, TG, t-chol, WC | No | Yes (self-reported) |
| Sepahi 2018 [51] | 60 | 29 | 53.31 ± 6.6 56.09 ± 4.3 57.17 ± 2.9 | Double masked Randomized phase 2 placebo controlled | DM-1:10 DM-2:50 | Crocin 5 mg vs. crocin 15 mg vs. placebo | 3 months | FBG, HbA1c HDL-c, LDL-c, TG, t-Chol | No | No |
| Study Name, Year | Intervention Group | Control Group | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Post-Intervention | Baseline | Post-Intervention | ||||||||
| N | Mean | SD | Mean | SD | N | Mean | SD | Mean | SD | p | |
| Abedimanesh 2017 # [57] | 25 | 107.25 | 44.14 | 100.85 | 26.49 | 25 | 123.11 | 59.31 | 117.63 | 56.48 | NS |
| Azimi 2014 # [44] | 42 | 358.35 | 4.3 | 356.66 | 4.39 | 39 | 355.28 | 11.86 | 353.23 | 11.96 | NS |
| Ebrahimi 2019b [47] | 40 | 166.7 | 53.7 | 162.1 | 52.7 | 40 | 160.9 | 51.9 | 147.7 | 51.8 | NS |
| Karimi Nazari 2019 [56] | 36 | 118.11 | 3.55 | 109.14 | 6.23 | 39 | 119.15 | 4.03 | 118.87 | 6.27 | 0.005 |
| Javandoost 2017 [52] | 21 | 94.08 | 16.49 | 91 | 20.67 | 22 | 102.75 | 27.5 | 103.83 | 23.77 | NS |
| Kermani 2017 # [53] | 24 | 110 | 42.16 | 111.2 | 35.6 | 24 | 124.4 | 47.7 | 129.3 | 75 | NS |
| Milajerdi 2018 [49] | 26 | 164.36 | 40.88 | 128.84 | 31.86 | 26 | 159.64 | 38.38 | 153.76 | 41.23 | <0.001 |
| Moravej Aleali 2019 [50] | 32 | 173.2 | 73.9 | 147.9 | 53.5 | 32 | 177.1 | 60.1 | 188.5 | 74.7 | 0.013 |
| Nikbakht-Jam 2016 # [54] | 30 | 102.34 | 36.88 | 104.52 | 49.2 | 30 | 101.31 | 29.08 | 103.31 | 25.18 | NS |
| Sepahi 2018 [51] | 55 | 176.6 | 64.17 | 155.39 | 55.49 | 23 | 175.15 | 7.38 | 169.45 | 7.61 | NS |
| Study Name, Year | Intervention Group | Control Group | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Post-Intervention | Baseline | Post-Intervention | ||||||||
| N | Mean | SD | Mean | SD | N | Mean | SD | Mean | SD | p | |
| Azimi 2014 # [44] | 42 | 7.73 | 0.07 | 7.74 | 0.07 | 39 | 7.5 | 0.1 | 7.51 | 0.1 | NS |
| Ebrahimi 2019b [47] | 40 | 8.01 | 1.4 | 7.69 | 1.49 | 40 | 7.38 | 1.53 | 7.34 | 1.48 | NS |
| Karimi Nazari 2019 [56] | 36 | 5.85 | 0.12 | 5.7 | 0.11 | 39 | 5.88 | 0.11 | 5.92 | 0.12 | <0.005 |
| Milajerdi 2018 [49] | 26 | 6.37 | 1.3 | 6.75 | 1.28 | 26 | 6.83 | 1.36 | 7.25 | 1.65 | NS |
| Moravej Aleali 2019 [50] | 32 | 8.9 | 2 | 8.2 | 1.8 | 32 | 8.8 | 1.8 | 8.3 | 1.4 | NS |
| Sepahi 2018 [51] | 23 | 8.17 | 0.11 | 7.29 | 0.12 | 23 | 8.15 | 0.22 | 8.03 | 0.14 | 0.024 * |
| Study Name, Year | Intervention Group | Control Group | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Post-Intervention | Baseline | Post-Intervention | ||||||||
| N | Mean | SD | Mean | SD | N | Mean | SD | Mean | SD | p | |
| Azimi 2014 # [44] | 42 | 395 | 212 | 394.3 | 2.22 | 39 | 338.92 | 8.78 | 334.92 | 8.87 | 0.004 |
| Ebrahimi 2019b [47] | 40 | 143.7 | 36.6 | 152.8 | 31.4 | 40 | 147 | 32.5 | 155.1 | 37.2 | NS |
| Karimi Nazari 2019 [56] | 36 | 186.67 | 17.22 | 184.54 | 17.45 | 39 | 192.69 | 13.57 | 190.88 | 14.6 | NS |
| Javandoost 2017 [52] | 22 | 232.18 | 66.52 | 220.09 | 55.6 | 22 | 209.19 | 38.41 | 199.95 | 50.1 | NS |
| Kermani 2017 # [53] | 24 | 230.1 a | 42.3 | 204.5 a | 41.2 | 24 | 232.2 b | 49.7 | 208.6 b | 41 | NS |
| Milajerdi 2018 [49] | 26 | 179.04 | 35.29 | 166.96 | 25.8 | 26 | 181.44 | 33.19 | 169.28 | 25.57 | NS |
| Moravej Aleali 2019 [50] | 32 | 169.3 | 38.8 | 152.9 | 32.1 | 32 | 152.21 | 31.5 | 164.2 | 43.5 | 0.014 |
| Nikbakht-Jam 2016 # [54] | 30 | 224.48 | 60.83 | 210.52 | 52.68 | 30 | 212.76 | 37.82 | 210.9 | 50.3 | NS |
| Sepahi 2018 [51] | 55 | 196.54 | 55.2 | 199.02 | 49.5 | 23 | 189.45 | 7.24 | 190.85 | 7.17 | NS |
| Zilaee 2018 # [55] | 30 | 199.15 | 27.3 | 96.88 | 37.73 | 31 | 177.16 | 33.34 | 167.36 | 37.03 | NS |
| Study Name, Year | Intervention Group | Control Group | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Post-Intervention | Baseline | Post-Intervention | ||||||||
| N | Mean | SD | Mean | SD | N | Mean | SD | Mean | SD | p | |
| Abedimanesh 2017 # [57] | 25 | 94.1 | 35.4 | 89.2 | 32.34 | 25 | 81.31 | 28.47 | 83.21 | 26.23 | NS |
| Azimi 2014 # [44] | 42 | 229.57 | 2.64 | 228.28 | 2.63 | 39 | 208.64 | 6.06 | 205.94 | 5.51 | 0.01 |
| Ebrahimi 2019b [47] | 40 | 82.7 | 25.7 | 89.5 | 23.9 | 40 | 84.5 | 26.6 | 90.7 | 30.5 | NS |
| Karimi Nazari 2019 [56] | 36 | 114.75 | 13.25 | 113.55 | 12.77 | 39 | 120.31 | 12.69 | 117.72 | 11.34 | NS |
| Javandoost 2017 [52] | 21 | 162.67 | 66.78 | 131.25 | 54.66 | 22 | 130.92 | 39.8 | 116.17 | 70.5 | NS |
| Kermani 2017 # [53] | 24 | 146.3 | 25.4 | 139.1 | 25.8 | 24 | 147.2 | 44.9 | 127.5 | 32.1 | NS |
| Milajerdi 2018 [49] | 26 | 83.79 | 29.48 | 85.9 | 32.04 | 26 | 95.9 | 36.16 | 82.94 | 26.95 | NS |
| Moravej Aleali 2019 [50] | 32 | 87.7 | 26.1 | 72.9 | 26.2 | 32 | 81.2 | 25.4 | 82.9 | 40.5 | 0.014 |
| Nikbakht-Jam 2016 # [54] | 30 | 152.29 a | 56.93 | 123.52 a | 48.06 | 30 | 138.45 | 36.76 | 125.76 | 52.16 | NS |
| Sepahi 2018 [51] | 55 | 120.99 | 43.15 | 118.54 | 46.13 | 23 | 113.85 | 6.02 | 110.45 | 5.31 | NS |
| Zilaee 2018 # [55] | 30 | 120.03 | 30.01 | 97.65 | 25.88 | 31 | 125.16 | 22.33 | 113 | 26.56 | 0.03 |
| Study Name, Year | Intervention Group | Control Group | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Post-Intervention | Baseline | Post-Intervention | ||||||||
| N | Mean | SD | Mean | SD | N | Mean | SD | Mean | SD | p | |
| Abedimanesh 2017 # [57] | 25 | 42.35 | 6.74 | 45.7 | 9.06 | 25 | 45.84 | 6.52 | 47.84 | 8.33 | NS |
| Azimi2014 # [44] | 42 | 53.97 | 0.71 | 54.76 | 0.74 | 39 | 50.38 | 1.38 | 51.53 | 1.52 | 0.001 |
| Ebrahimi 2019b [47] | 40 | 41.8 | 8.4 | 42.2 | 9.4 | 40 | 44.35 | 10.1 | 44.9 | 11.3 | NS |
| Karimi Nazari 2019 [56] | 36 | 49.97 | 11.62 | 50.25 | 11.15 | 39 | 52.2 | 8.8 | 52 | 9.8 | NS |
| Javandoost 2017 [52] | 21 | 38.25 a | 11.33 | 48.92 a | 12.5 | 22 | 38.17 b | 10.7 | 52.5 b | 15.06 | NS |
| Kermani 2017 # [53] | 24 | 40.3 | 8.4 | 40 | 7.8 | 24 | 38.4 | 6.8 | 38.6 | 7.3 | NS |
| Milajerdi 2018 [49] | 26 | 58.83 | 8.47 | 63.33 | 5.11 | 26 | 60.95 | 7.17 | 6.17 | 7.08 | NS |
| Moravej Aleali 2019 [50] | 32 | 45.1 | 9.1 | 48.2 | 10.6 | 32 | 38.3 | 9.6 | 43 | 11.1 | NS |
| Nikbakht-Jam 2016 # [54] | 30 | 38.59 | 10.14 | 49.25 | 11.5 | 30 | 38.93 | 9.18 | 51.24 | 10.44 | NS |
| Sepahi 2018 [51] | 55 | 43.57 | 11.53 | 42.94 | 10.3 | 23 | 43.95 | 0.94 | 44.35 | 0.85 | NS |
| Zilaee 2018 # [55] | 30 | 39.03 | 5.34 | 43 | 9.97 | 31 | 39.13 | 8 | 43.46 | 6.5 | NS |
| Study Name, Year | Intervention Group | Control Group | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Post-Intervention | Baseline | Post-Intervention | |||||||||
| N | Mean | SD | Mean | SD | N | Mean | SD | Mean | SD | p | ||
| Abedimanesh 2017 # [57] | 25 | 200.05 | 74.08 | 193.05 | 60.44 | 25 | 182.37 | 87.27 | 192.32 | 101 | NS | |
| Azimi 2014 # [44] | 42 | 391.88 | 3.91 | 390.71 | 3.82 | 39 | 386.54 | 13.28 | 382.48 | 12.72 | NS | |
| Ebrahimi 2019b [47] | 40 | 165.8 | 121.8 | 175 | 98.1 | 40 | 170.4 | 63.5 | 168 | 58.3 | NS | |
| Karimi Nazari 2019 [56] | 36 | 101.5 | 20.34 | 100.22 | 17.63 | 39 | 108.94 | 18.2 | 107.84 | 15.97 | NS | |
| Javandoost 2017 [52] | 21 | 155.58 | 73.74 | 163.25 | 99.58 | 22 | 164.33 | 84.8 | 153.67 | 75.29 | NS | |
| Kermani 2017 # [53] | 24 | 218.1a | 80 | 173.8a | 97.5 | 24 | 232.4 | 83.2 | 197.5 | 82.9 | NS | |
| Milajerdi 2018 [49] | 26 | 146.54 | 41.86 | 127 | 37.61 | 26 | 137.96 | 40.71 | 128.2 | 38.5 | NS | |
| Moravej Aleali 2019 [50] | 32 | 166.4 | 87.7 | 156.4 | 73.2 | 32 | 187.2 | 137.1 | 191.8 | 135.3 | NS | |
| Nikbakht-Jam 2016 # [54] | 30 | 153.17 | 67.06 | 147 | 72.52 | 30 | 165.47 | 76.73 | 153.9 | 89.9 | NS | |
| Sepahi 2018 [51] | 55 | 199.65 | 112.24 | 196.32 | 97.6 | 23 | 203.75 | 9.32 | 200.7 | 8.09 | NS | |
| Zilaee2018 # [55] | 30 | 139,76 | 70,14 | 96,88 | 37,73 | 31 | 139 | 73,52 | 107,6 | 43,98 | NS | |
| Study Name, Year | Intervention Group | Control Group | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Post-Intervention | Baseline | Post-Intervention | ||||||||
| N | Mean | SD | Mean | SD | N | Mean | SD | Mean | SD | p | |
| Azimi 2016 # [45] | 42 | 139.08 | 0.2 | 139 | 0.1 | 39 | 136.9 | 0.2 | 137.2 | 0.2 | NS |
| Ebrahimi 2019 [46] | 40 | 132.7 | 21.3 | 124.5 | 13.2 | 40 | 127.4 | 15.3 | 128.3 | 12.4 | 0.005 |
| Kermani 2017 # [53] | 24 | 129.3 | 16.9 | 126.8 | 19.4 | 24 | 131 | 14 | 131.8 | 13.5 | NS |
| Study Name, Year | Intervention Group | Control Group | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Post-Intervention | Baseline | Post-Intervention | ||||||||
| N | Mean | SD | Mean | SD | N | Mean | SD | Mean | SD | p | |
| Azimi 2016# [45] | 42 | 94.06 | 0.1 | 94.02 | 0.1 | 39 | 92.7 | 0.1 | 93.9 | 0.1 | NS |
| Ebrahimi 2019 [46] | 40 | 79.5 | 10.8 | 76.7 | 9.9 | 40 | 79.7 | 11.1 | 75.9 | 14 | NS |
| Kermani 2017 # [53] | 24 | 81.1 | 12.8 | 80.9 | 14.5 | 24 | 85 | 20.6 | 84.1 | 13.4 | NS |
| Study Name, Year | Intervention Group | Control Group | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Post-Intervention | Baseline | Post-Intervention | ||||||||
| N | Mean | SD | Mean | SD | N | Mean | SD | Mean | SD | p | |
| Abedimanesh 2017 # [57] | 25 | 95 | 12.85 | 92.68 | 13.03 | 25 | 92.84 | 9.13 | 91.42 | 8.94 | NS |
| Azimi 2016 # [45] | 42 | 102.26 | 1.5 | 102.02 | 1.5 | 39 | 100.92 | 1.4 | 100.66 | 1.4 | NS |
| Ebrahimi 2019b [47] | 40 | 104.31 | 7.85 | 100.02 | 7.32 | 40 | 102.95 | 7.94 | 104.33 | 7.42 | <0.001 |
| Kermani2017 # [53] | 24 | 103.9 | 9.5 | 103.2 | 9 | 24 | 101.5 | 8.1 | 105.9 | 15.7 | NS |
| Zilaee 2018 # [55] | 32 | 105.76 | 9.01 | 103 | 9.02 | 32 | 103.36 | 12.09 | 101.03 | 12.69 | NS |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giannoulaki, P.; Kotzakioulafi, E.; Chourdakis, M.; Hatzitolios, A.; Didangelos, T. Impact of Crocus sativus L. on Metabolic Profile in Patients with Diabetes Mellitus or Metabolic Syndrome: A Systematic Review. Nutrients 2020, 12, 1424. https://doi.org/10.3390/nu12051424
Giannoulaki P, Kotzakioulafi E, Chourdakis M, Hatzitolios A, Didangelos T. Impact of Crocus sativus L. on Metabolic Profile in Patients with Diabetes Mellitus or Metabolic Syndrome: A Systematic Review. Nutrients. 2020; 12(5):1424. https://doi.org/10.3390/nu12051424
Chicago/Turabian StyleGiannoulaki, Parthena, Evangelia Kotzakioulafi, Michail Chourdakis, Apostolos Hatzitolios, and Triantafyllos Didangelos. 2020. "Impact of Crocus sativus L. on Metabolic Profile in Patients with Diabetes Mellitus or Metabolic Syndrome: A Systematic Review" Nutrients 12, no. 5: 1424. https://doi.org/10.3390/nu12051424
APA StyleGiannoulaki, P., Kotzakioulafi, E., Chourdakis, M., Hatzitolios, A., & Didangelos, T. (2020). Impact of Crocus sativus L. on Metabolic Profile in Patients with Diabetes Mellitus or Metabolic Syndrome: A Systematic Review. Nutrients, 12(5), 1424. https://doi.org/10.3390/nu12051424