The Impact of Malnutrition on Acute Muscle Wasting in Frail Older Hospitalized Patients

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Assessment of the Nutritional Status
2.1.1. GLIM Criteria
2.1.2. MNA-SF
2.2. Geriatric Assessment
2.3. Assessment of Muscle Strength
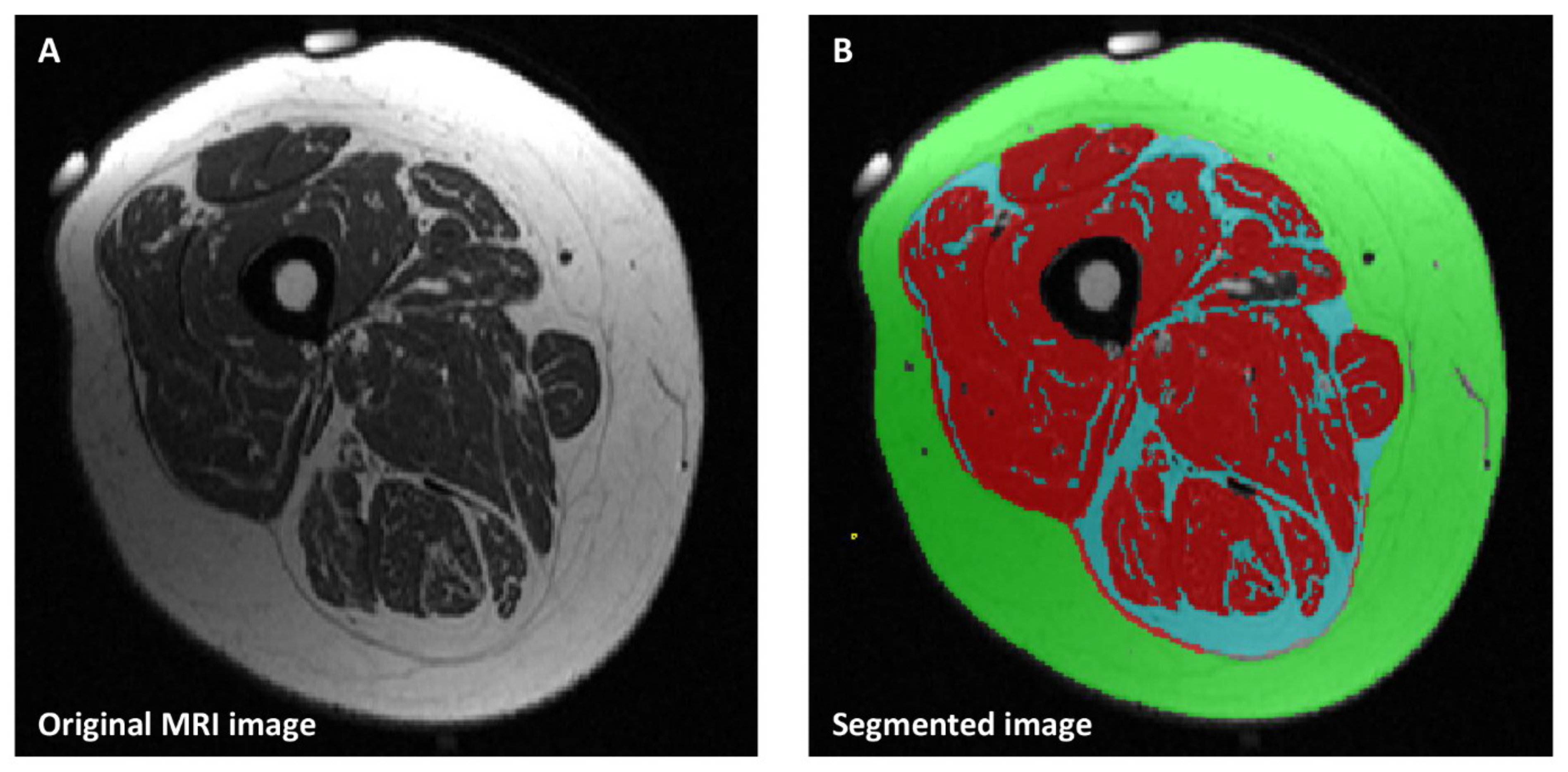
2.4. Mid-Thigh Magnetic Resonance Imaging (MRI) Cross Sectional Area
2.5. Statistical Analysis
3. Results
3.1. Characterization of Study Population
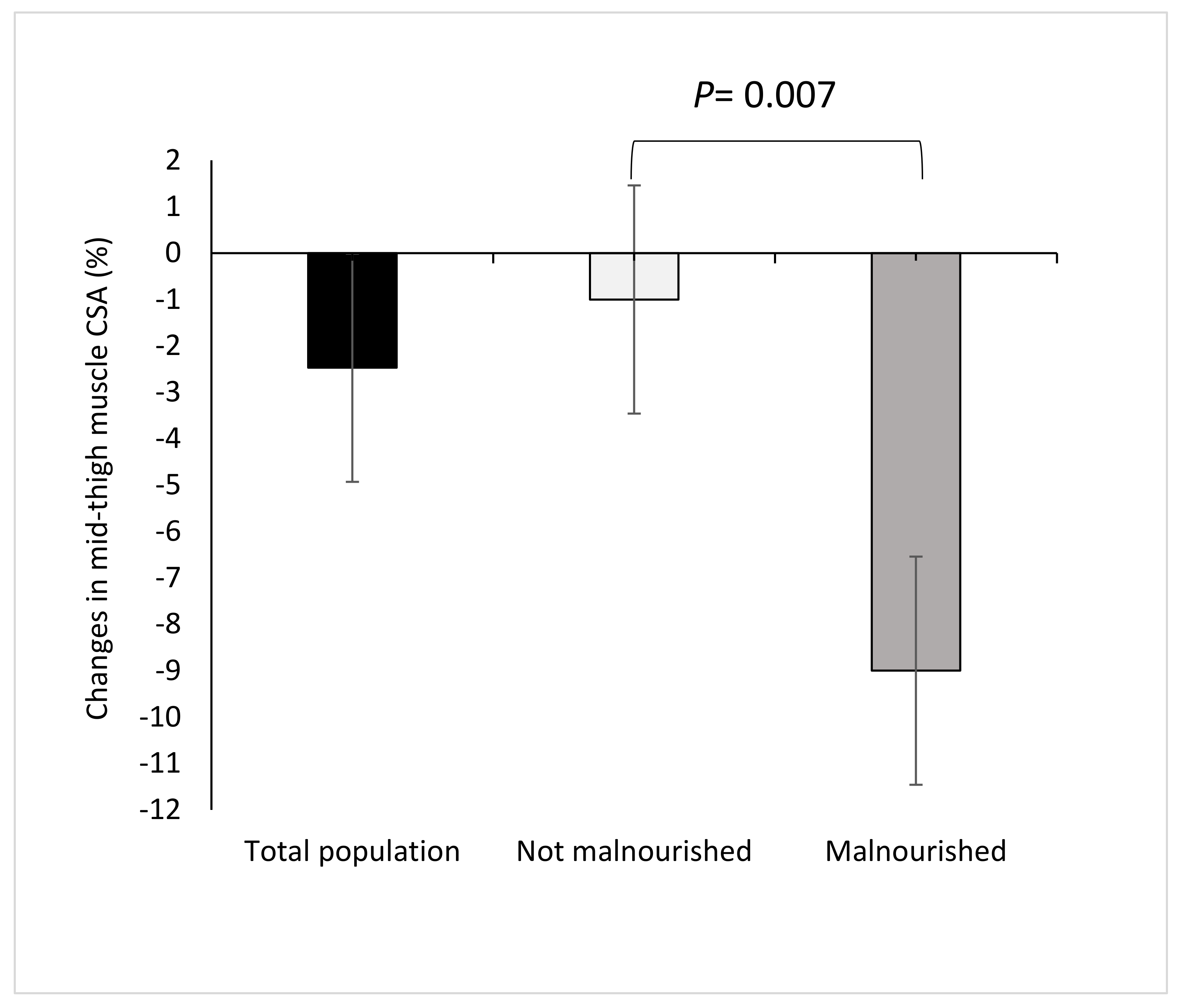
3.2. Changes of MRI-CSA during Follow-Up
3.2.1. GLIM Criteria
3.2.2. MNA-SF
3.3. Functional Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rolland, Y.; Czerwinski, S.; van Kan, G.A.; Morley, J.E.; Cesari, M.; Onder, G.; Woo, J.; Baumgartner, R.; Pillard, F.; Boirie, Y.; et al. Sarcopenia: Its assessment, etiology, pathogenesis, consequences and future perspectives. J. Nutr. Health Aging 2008, 12, 433–450. [Google Scholar] [CrossRef] [PubMed]
- Von Haehling, S.; Morley, J.E.; Anker, S.D. An overview of sarcopenia: Facts and numbers on prevalence and clinical impact. J. Cachexia Sarcopenia Muscle 2010, 1, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Goodpaster, B.H.; Park, S.W.; Harris, T.B.; Kritchevsky, S.B.; Nevitt, M.; Schwartz, A.V.; Simonsick, E.M.; Tylavsky, F.A.; Visser, M.; Newman, A.B. The loss of skeletal muscle strength, mass, and quality in older adults: The health, aging and body composition study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2006, 61, 1059–1064. [Google Scholar] [CrossRef]
- Pierik, V.D.; Meskers, C.G.M.; Van Ancum, J.M.; Numans, S.T.; Verlaan, S.; Scheerman, K.; Kruizinga, R.C.; Maier, A.B. High risk of malnutrition is associated with low muscle mass in older hospitalized patients—A prospective cohort study. BMC Geriatr. 2017, 17, 118. [Google Scholar] [CrossRef]
- Robinson, S.M.; Reginster, J.Y.; Rizzoli, R.; Shaw, S.C.; Kanis, J.A.; Bautmans, I.; Bischoff-Ferrari, H.; Bruyere, O.; Cesari, M.; Dawson-Hughes, B.; et al. Does nutrition play a role in the prevention and management of sarcopenia? Clin. Nutr. 2018, 37, 1121–1132. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.J.; Friedkin, R.J.; Inouye, S.K. Prevalence and outcomes of low mobility in hospitalized older patients. J. Am. Geriatr. Soc. 2004, 52, 1263–1270. [Google Scholar] [CrossRef]
- Van Ancum, J.M.; Scheerman, K.; Jonkman, N.H.; Smeenk, H.E.; Kruizinga, R.C.; Meskers, C.G.M.; Maier, A.B. Change in muscle strength and muscle mass in older hospitalized patients: A systematic review and meta-analysis. Exp. Gerontol. 2017, 92, 34–41. [Google Scholar] [CrossRef]
- Pourhassan, M.; Norman, K.; Muller, M.J.; Dziewas, R.; Wirth, R. Impact of Sarcopenia on One-Year Mortality among Older Hospitalized Patients with Impaired Mobility. J. Frailty Aging 2018, 7, 40–46. [Google Scholar] [CrossRef]
- Kortebein, P.; Ferrando, A.; Lombeida, J.; Wolfe, R.; Evans, W.J. Effect of 10 days of bed rest on skeletal muscle in healthy older adults. JAMA 2007, 297, 1772–1774. [Google Scholar] [CrossRef]
- Vanderwee, K.; Clays, E.; Bocquaert, I.; Gobert, M.; Folens, B.; Defloor, T. Malnutrition and associated factors in elderly hospital patients: A Belgian cross-sectional, multi-centre study. Clin. Nutr. 2010, 29, 469–476. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Landi, F.; Topinkova, E.; Michel, J.P. Understanding sarcopenia as a geriatric syndrome. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Vandewoude, M.F.; Alish, C.J.; Sauer, A.C.; Hegazi, R.A. Malnutrition-sarcopenia syndrome: Is this the future of nutrition screening and assessment for older adults? J. Aging Res. 2012, 2012, 651570. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T.; Jensen, G.L.; Correia, M.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. Clin. Nutr. 2019, 38, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, M.J.; Bauer, J.M.; Ramsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.; Charlton, K.E.; Maggio, M.; et al. Validation of the Mini Nutritional Assessment short-form (MNA-SF): A practical tool for identification of nutritional status. J. Nutr. Health Aging 2009, 13, 782–788. [Google Scholar] [CrossRef]
- Mahoney, F.I.; Barthel, D.W. FUNCTIONAL EVALUATION: THE BARTHEL INDEX. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- van Kan, G.A.; Rolland, Y.M.; Morley, J.E.; Vellas, B. Frailty: Toward a clinical definition. J. Am. Med. Dir. Assoc. 2008, 9, 71–72. [Google Scholar] [CrossRef]
- Malmstrom, T.K.; Miller, D.K.; Simonsick, E.M.; Ferrucci, L.; Morley, J.E. SARC-F: A symptom score to predict persons with sarcopenia at risk for poor functional outcomes. J. Cachexia Sarcopenia Muscle 2016, 7, 28–36. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Gandevia, S.C. Spinal and supraspinal factors in human muscle fatigue. Physiol. Rev. 2001, 81, 1725–1789. [Google Scholar] [CrossRef]
- Deutz, N.E.P.; Ashurst, I.; Ballesteros, M.D.; Bear, D.E.; Cruz-Jentoft, A.J.; Genton, L.; Landi, F.; Laviano, A.; Norman, K.; Prado, C.M. The Underappreciated Role of Low Muscle Mass in the Management of Malnutrition. J. Am. Med. Dir. Assoc. 2019, 20, 22–27. [Google Scholar] [CrossRef]
- Prado, C.M.; Purcell, S.A.; Alish, C.; Pereira, S.L.; Deutz, N.E.; Heyland, D.K.; Goodpaster, B.H.; Tappenden, K.A.; Heymsfield, S.B. Implications of low muscle mass across the continuum of care: A narrative review. Ann. Med. 2018, 50, 675–693. [Google Scholar] [CrossRef] [PubMed]
- Verlaan, S.; Van Ancum, J.M.; Pierik, V.D.; Van Wijngaarden, J.P.; Scheerman, K.; Meskers, C.G.M.; Maier, A.B. Muscle Measures and Nutritional Status at Hospital Admission Predict Survival and Independent Living of Older Patients—The EMPOWER Study. J. Frailty Aging 2017, 6, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Cerri, A.P.; Bellelli, G.; Mazzone, A.; Pittella, F.; Landi, F.; Zambon, A.; Annoni, G. Sarcopenia and malnutrition in acutely ill hospitalized elderly: Prevalence and outcomes. Clin. Nutr. 2015, 34, 745–751. [Google Scholar] [CrossRef]
- Perez-Zepeda, M.U.; Sgaravatti, A.; Dent, E. Sarcopenia and post-hospital outcomes in older adults: A longitudinal study. Arch. Gerontol. Geriatr. 2017, 69, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Van Ancum, J.M.; Scheerman, K.; Pierik, V.D.; Numans, S.T.; Verlaan, S.; Smeenk, H.E.; Slee-Valentijn, M.; Kruizinga, R.C.; Meskers, C.G.M.; Maier, A.B. Muscle Strength and Muscle Mass in Older Patients during Hospitalization: The EMPOWER Study. Gerontology 2017, 63, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Koopman, R.; van Loon, L.J. Aging, exercise, and muscle protein metabolism. J. Appl. Physiol. 2009, 106, 2040–2048. [Google Scholar] [CrossRef]
- Cawood, A.L.; Elia, M.; Stratton, R.J. Systematic review and meta-analysis of the effects of high protein oral nutritional supplements. Ageing Res. Rev. 2012, 11, 278–296. [Google Scholar] [CrossRef]
- Bauer, J.M.; Verlaan, S.; Bautmans, I.; Brandt, K.; Donini, L.M.; Maggio, M.; McMurdo, M.E.T.; Mets, T.; Seal, C.; Wijers, S.L.; et al. Effects of a Vitamin D and Leucine-Enriched Whey Protein Nutritional Supplement on Measures of Sarcopenia in Older Adults, the PROVIDE Study: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Am. Med. Dir. Assoc. 2015, 16, 740–747. [Google Scholar] [CrossRef]
- Bourdel-Marchasson, I.; Joseph, P.A.; Dehail, P.; Biran, M.; Faux, P.; Rainfray, M.; Emeriau, J.P.; Canioni, P.; Thiaudiere, E. Functional and metabolic early changes in calf muscle occurring during nutritional repletion in malnourished elderly patients. Am. J. Clin. Nutr. 2001, 73, 832–838. [Google Scholar] [CrossRef]
- Landi, F.; Liperoti, R.; Russo, A.; Giovannini, S.; Tosato, M.; Capoluongo, E.; Bernabei, R.; Onder, G. Sarcopenia as a risk factor for falls in elderly individuals: Results from the ilSIRENTE study. Clin. Nutr. 2012, 31, 652–658. [Google Scholar] [CrossRef]
- Van Ancum, J.M.; Pijnappels, M.; Jonkman, N.H.; Scheerman, K.; Verlaan, S.; Meskers, C.G.M.; Maier, A.B. Muscle mass and muscle strength are associated with pre- and post-hospitalization falls in older male inpatients: A longitudinal cohort study. BMC Geriatr. 2018, 18, 116. [Google Scholar] [CrossRef] [PubMed]
- Green, J.; Forster, A.; Young, J. A test-retest reliability study of the Barthel Index, the Rivermead Mobility Index, the Nottingham Extended Activities of Daily Living Scale and the Frenchay Activities Index in stroke patients. Disabil. Rehabil. 2001, 23, 670–676. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| GLIM Criteria | ||||
|---|---|---|---|---|
| All (n = 41) | Malnourished (n = 7; 17%) | Non-Malnourished (n = 34; 83%) | p Value | |
| Gender | ||||
| Female (number, %) | 30 (73) | 4 (57) | 26 (77) | 0.361 |
| Male (number, %) | 11 (27) | 3 (43) | 8 (23) | |
| Age (y) | 82.4 ± 6.6 | 81.1 ± 8.0 | 82.6 ± 6.3 | 0.660 |
| Height (m) | 1.61 ± 0.1 | 1.67 ± 0.1 | 1.60 ± 0.1 | 0.036 |
| Actual body weight (kg) | 73.9 ± 16.8 | 66.5 ± 13.1 | 75.4 ± 17.2 | 0.150 |
| BMI (kg/m2) | 28.4 ± 6.4 | 23.5 ± 3.8 | 29.4 ± 6.4 | 0.006 |
| Weight loss in 6 months (kg) | 2.2 ± 3.1 | 5.8 ± 3.0 | 1.4 ± 2.6 | 0.006 |
| CRP (mg/dl) | 2.5 ± 5.5 | 2.5 ± 1.9 | 2.5 ± 6.0 | 0.969 |
| Total MNA-SF, Median (IQR) | 8 (10–12) | 9 (7–9) | 11 (9–12) | 0.010 |
| Barthel Index on admission, Median (IQR) | 55 (40–67) | 35 (35–45) | 60 (40–70) | 0.005 |
| Walking, Median (IQR) | 5 (5–10) | 5 (5–5) | 10 (5–10) | 0.025 |
| Frail Simple scale score, Median (IQR) | 3 (2–3) | 3 (3–4) | 3 (2–3) | 0.006 |
| SARC-F scores, Median (IQR) | 6 (4–7) | 5 (3–8) | 6 (4–7) | 0.747 |
| CCI score, Median (IQR) | 2 (1–3) | 1 (1–3) | 2 (1–2) | 0.959 |
| Mobility Status | ||||
| Mobile (number, %) | 19 (46) | 0 (0) | 19 (56) | 0.010 |
| Immobile (number, %) | 22 (54) | 7 (100) | 15 (44) | |
| Length of hospital stay | 16 (14–18) | 16 (14–17) | 16 (14–18) | 0.577 |
| Time between MRI scans | 14 (11–14) | 14 (11–14) | 13 (11–14) | 0.667 |
| MNA-SF All (n = 41) | GLIM Criteria All (n = 41) | ||||
|---|---|---|---|---|---|
| Mid-thigh MRI cross sectional area (cm2) | Malnourished (n = 5, 12%) | At risk (n = 22, 54%) | Normal (n = 14, 34%) | Malnourished (n = 7, 17%) | Non-malnourished (n = 34, 83%) |
| Muscle area T0 | 68.1 ± 15.2 | 82.6 ± 19.7 | 83.5 ± 15.9 | 78.9 ± 21.0 | 81.6 ± 17.9 |
| Muscle area T1 | 62.1 ± 11.1 † | 80.8 ± 21.2 a | 83.1 ± 16.6 bb | 71.9 ± 20.8 †† | 80.8 ± 19.2 |
| Changes in muscle area | −6.0 ± 4.3 | −1.8 ± 6.0 | −0.4 ± 5.2 b | −7.0 ± 4.7 | −0.7 ± 5.3 c |
| Subcutaneous fat area T0 | 77.1 ± 48.0 | 77.6 ± 43.0 | 112.4 ± 64.4 | 63.8 ± 28.6 | 94.7 ± 55.8 c |
| Subcutaneous fat area T1 | 70.0 ± 41.8 | 75.5 ± 40.9 | 106.6 ± 59.2 | 56.9 ± 27.4 | 91.3 ± 51.0 c |
| Changes in subcutaneous fat area | −7.1 ± 9.4 | −2.1 ± 12.0 | −5.7 ± 19.7 | −6.8 ± 7.8 | −3.4 ± 15.8 |
| Intermuscular fat area T0 | 9.4 ± 2.6 | 18.2 ± 8.8 | 21.1 ± 10.7 bb | 14.2 ± 6.5 | 18.9 ± 9.9 |
| Intermuscular fat area T1 | 9.5 ± 2.6 | 17.3 ± 8.8 | 21.0 ± 13.1 | 12.0 ± 5.1 | 18.7 ± 11.0 c |
| Changes in intermuscular fat area | 0.1 ± 0.9 | −0.9 ± 3.2 | −0.1 ± 3.8 | −2.2 ± 2.7 | −0.2 ± 3.2 |
| GlIM Criteria | p Value | ||
|---|---|---|---|
| Functional Status | Malnourished (n = 7, 17%) | Non-Malnourished (n = 34, 83%) | |
| Handgrip strength (kg), T0 | 17.3 ± 5.7 | 20.3 ± 8.7 | 0.268 |
| Handgrip strength (kg), T1 | 15.4 ± 4.2 | 20.8 ± 8.8 | 0.024 |
| Changes in Handgrip strength (kg) | −1.8 ± 4.3 | 0.5 ± 2.4 | 0.207 |
| Knee extension strength (kg), T0 | 12.4 ± 4.6 | 17.5 ± 6.8 | 0.030 |
| Knee extension strength (kg), T1 | 10.9 ± 4.7 | 17.2 ± 7.0 | 0.022 |
| Changes in Knee extension strength (kg) | −1.5 ± 2.2 | −0.3 ± 3.1 | 0.289 |
| Activity of daily living | |||
| Barthel Index, Median (IQR); T0 | 35 (35–45) | 60 (40–70) | 0.005 |
| Barthel Index, Median (IQR); T1 | 55 (50–75) † | 75 (65–85) † | 0.028 |
| Changes in Barthel Index, Median (IQR) | 20 (10–30) | 15 (10–20) | 0.584 |
| Beta Coefficient | SE | p Value | |
|---|---|---|---|
| Changes in absolute mid-thigh muscle mass area | |||
| Age | 0.085 | 0.137 | 0.838 |
| Gender | −1.506 | 2.861 | 0.747 |
| Body weight on admission | 0.150 | 0.074 | 0.325 |
| Weight loss in last 6 months | 0.012 | 0.299 | 0.110 |
| Malnutrition based on GLIM criteria | −6.271 | 2.088 | 0.005 |
| Changes in body weight during hospital stay | 0.323 | 0.155 | 0.044 |
| Mid-thigh muscle mass area on admission | −0.178 | 0.078 | 0.864 |
| Mobility based on Barthel Index | 0.344 | 0.255 | 0.079 |
| Frail Simple scale score | −1.224 | 1.314 | 0.101 |
| C-reactive protein | −0.240 | 0.177 | 0.130 |
| Charlson Comorbidity Index | 1.629 | 0.889 | 0.284 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pourhassan, M.; Rommersbach, N.; Lueg, G.; Klimek, C.; Schnatmann, M.; Liermann, D.; Janssen, G.; Wirth, R. The Impact of Malnutrition on Acute Muscle Wasting in Frail Older Hospitalized Patients. Nutrients 2020, 12, 1387. https://doi.org/10.3390/nu12051387
Pourhassan M, Rommersbach N, Lueg G, Klimek C, Schnatmann M, Liermann D, Janssen G, Wirth R. The Impact of Malnutrition on Acute Muscle Wasting in Frail Older Hospitalized Patients. Nutrients. 2020; 12(5):1387. https://doi.org/10.3390/nu12051387
Chicago/Turabian StylePourhassan, Maryam, Nikola Rommersbach, Gero Lueg, Christiane Klimek, Mirja Schnatmann, Dieter Liermann, Gregor Janssen, and Rainer Wirth. 2020. "The Impact of Malnutrition on Acute Muscle Wasting in Frail Older Hospitalized Patients" Nutrients 12, no. 5: 1387. https://doi.org/10.3390/nu12051387
APA StylePourhassan, M., Rommersbach, N., Lueg, G., Klimek, C., Schnatmann, M., Liermann, D., Janssen, G., & Wirth, R. (2020). The Impact of Malnutrition on Acute Muscle Wasting in Frail Older Hospitalized Patients. Nutrients, 12(5), 1387. https://doi.org/10.3390/nu12051387