Validation of a Semi-Quantitative Food-Frequency Questionnaire for Dutch Pregnant Women from the General Population Using the Method or Triads

 ,
, 
 and
and
Abstract
1. Introduction
2. Materials and Methods
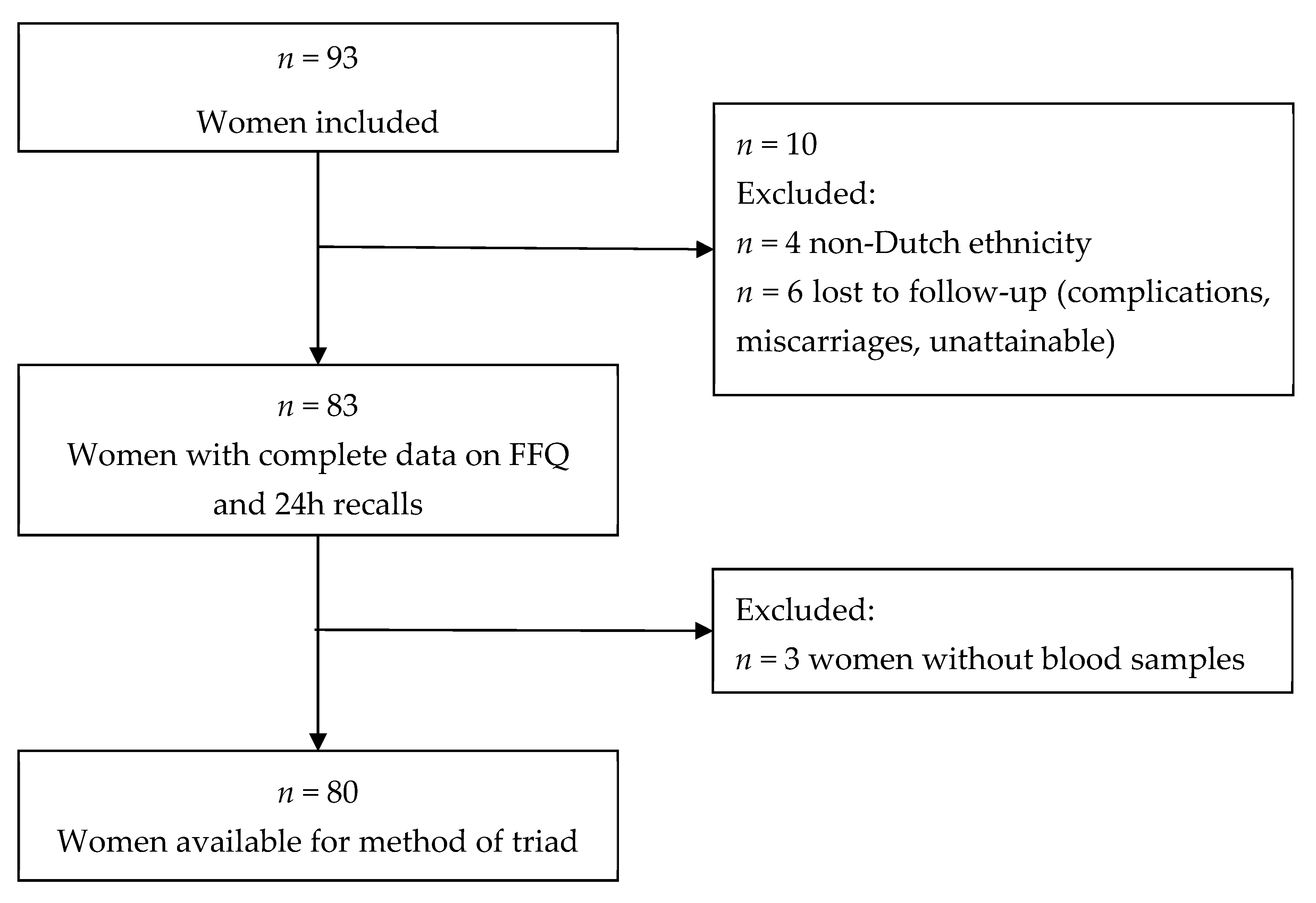
2.1. Study Design and Participants
2.2. Food-Frequency Questionnaire
2.3. 24 Hour-recalls
2.4. Biomarkers
2.5. Statistical Analysis
3. Results
3.1. Evaluation of the FFQ Against 24 h-Recalls
3.2. Evaluation of the FFQ Against 24 h-recalls and Biomarkers: the Method of Triads
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gillman, M.W. Developmental origins of health and disease. N. Engl. J. Med. 2005, 353, 1848–1850. [Google Scholar] [CrossRef] [PubMed]
- Bouwland-Both, M.I.; Steegers-Theunissen, R.P.; Vujkovic, M.; Lesaffre, E.M.; Mook-Kanamori, D.O.; Hofman, A.; Lindemans, J.; Russcher, H.; Jaddoe, V.W.; Steegers, E.A. A periconceptional energy-rich dietary pattern is associated with early fetal growth: The generation r study. BJOG 2013, 120, 435–445. [Google Scholar] [CrossRef] [PubMed]
- Parisi, F.; Rousian, M.; Steegers-Theunissen, R.P.M.; Koning, A.H.J.; Willemsen, S.P.; de Vries, J.H.M.; Cetin, I.; Steegers, E.A.P. Early first trimester maternal ‘high fish and olive oil and low meat’ dietary pattern is associated with accelerated human embryonic development. Eur. J. Clin. Nutr. 2018, 72, 1655–1662. [Google Scholar] [CrossRef] [PubMed]
- Timmermans, S.; Steegers-Theunissen, R.P.; Vujkovic, M.; den Breeijen, H.; Russcher, H.; Lindemans, J.; Mackenbach, J.; Hofman, A.; Lesaffre, E.E.; Jaddoe, V.V.; et al. The mediterranean diet and fetal size parameters: The generation r study. Br. J. Nutr. 2012, 108, 1399–1409. [Google Scholar] [CrossRef]
- Oostingh, E.C.; Hall, J.; Koster, M.P.H.; Grace, B.; Jauniaux, E.; Steegers-Theunissen, R.P.M. The impact of maternal lifestyle factors on periconception outcomes: A systematic review of observational studies. Reprod. Biomed. Online 2019, 38, 77–94. [Google Scholar] [CrossRef]
- Jen, V.; Erler, N.S.; Tielemans, M.J.; Braun, K.V.; Jaddoe, V.W.; Franco, O.H.; Voortman, T. Mothers’ intake of sugar-containing beverages during pregnancy and body composition of their children during childhood: The generation r study. Am. J. Clin. Nutr. 2017, 105, 834–841. [Google Scholar] [CrossRef]
- Steenweg-de Graaff, J.; Tiemeier, H.; Steegers-Theunissen, R.P.; Hofman, A.; Jaddoe, V.W.; Verhulst, F.C.; Roza, S.J. Maternal dietary patterns during pregnancy and child internalising and externalising problems. The generation r study. Clin. Nutr. 2014, 33, 115–121. [Google Scholar] [CrossRef]
- Shaheen, S.O.; Northstone, K.; Newson, R.B.; Emmett, P.M.; Sherriff, A.; Henderson, A.J. Dietary patterns in pregnancy and respiratory and atopic outcomes in childhood. Thorax 2009, 64, 411–417. [Google Scholar] [CrossRef]
- de Rooij, S.R.; Painter, R.C.; Holleman, F.; Bossuyt, P.M.; Roseboom, T.J. The metabolic syndrome in adults prenatally exposed to the dutch famine. Am. J. Clin. Nutr. 2007, 86, 1219–1224. [Google Scholar] [CrossRef]
- Vujkovic, M.; Steegers, E.A.; Looman, C.W.; Ocke, M.C.; van der Spek, P.J.; Steegers-Theunissen, R.P. The maternal mediterranean dietary pattern is associated with a reduced risk of spina bifida in the offspring. BJOG 2009, 116, 408–415. [Google Scholar] [CrossRef]
- Obermann-Borst, S.A.; Vujkovic, M.; de Vries, J.H.; Wildhagen, M.F.; Looman, C.W.; de Jonge, R.; Steegers, E.A.; Steegers-Theunissen, R.P. A maternal dietary pattern characterised by fish and seafood in association with the risk of congenital heart defects in the offspring. BJOG 2011, 118, 1205–1215. [Google Scholar] [CrossRef] [PubMed]
- Han, S.; Crowther, C.A.; Middleton, P.; Heatley, E. Different types of dietary advice for women with gestational diabetes mellitus. Cochrane Database Syst. Rev. 2013, 3, CD009275. [Google Scholar]
- Tielemans, M.J.; Garcia, A.H.; Peralta Santos, A.; Bramer, W.M.; Luksa, N.; Luvizotto, M.J.; Moreira, E.; Topi, G.; de Jonge, E.A.; Visser, T.L.; et al. Macronutrient composition and gestational weight gain: A systematic review. Am. J. Clin. Nutr. 2016, 103, 83–99. [Google Scholar] [CrossRef] [PubMed]
- Timmermans, S.; Steegers-Theunissen, R.P.; Vujkovic, M.; Bakker, R.; den Breeijen, H.; Raat, H.; Russcher, H.; Lindemans, J.; Hofman, A.; Jaddoe, V.W.; et al. Major dietary patterns and blood pressure patterns during pregnancy: The generation r study. Am. J. Obstet. Gynecol. 2011, 205, 337. [Google Scholar] [CrossRef] [PubMed]
- Hillesund, E.R.; Overby, N.C.; Engel, S.M.; Klungsoyr, K.; Harmon, Q.E.; Haugen, M.; Bere, E. Associations of adherence to the new nordic diet with risk of preeclampsia and preterm delivery in the norwegian mother and child cohort study (moba). Eur. J. Epidemiol. 2014, 29, 753–765. [Google Scholar] [CrossRef] [PubMed]
- Willett, W. Nutritional Epidemiology, 3rd ed.; Oxford University Press: New York, NY, USA, 2013. [Google Scholar]
- Ocke, M.C.; Kaaks, R.J. Biochemical markers as additional measurements in dietary validity studies: Application of the method of triads with examples from the european prospective investigation into cancer and nutrition. Am. J. Clin. Nutr. 1997, 65, 1240S–1245S. [Google Scholar] [CrossRef]
- Kaaks, R.J. Biochemical markers as additional measurements in studies of the accuracy of dietary questionnaire measurements: Conceptual issues. Am. J. Clin. Nutr. 1997, 65, 1232s–1239s. [Google Scholar] [CrossRef]
- Verkleij-Hagoort, A.C.; de Vries, J.H.; Stegers, M.P.; Lindemans, J.; Ursem, N.T.; Steegers-Theunissen, R.P. Validation of the assessment of folate and vitamin b12 intake in women of reproductive age: The method of triads. Eur. J. Clin. Nutr. 2007, 61, 610–615. [Google Scholar] [CrossRef]
- Roza, A.M.; Shizgal, H.M. The harris benedict equation reevaluated: Resting energy requirements and the body cell mass. Am. J. Clin. Nutr. 1984, 40, 168–182. [Google Scholar] [CrossRef]
- Jaddoe, V.W.; van Duijn, C.M.; Franco, O.H.; van der Heijden, A.J.; van Iizendoorn, M.H.; de Jongste, J.C.; van der Lugt, A.; Mackenbach, J.P.; Moll, H.A.; Raat, H.; et al. The generation r study: Design and cohort update 2012. Eur. J. Epidemiol. 2012, 27, 739–756. [Google Scholar] [CrossRef]
- Klipstein-Grobusch, K.; den Breeijen, J.H.; Goldbohm, R.A.; Geleijnse, J.M.; Hofman, A.; Grobbee, D.E.; Witteman, J.C. Dietary assessment in the elderly: Validation of a semiquantitative food frequency questionnaire. Eur. J. Clin. Nutr. 1998, 52, 588–596. [Google Scholar] [CrossRef] [PubMed]
- Donders-Engelen, M.; van der Heijden, L. Maten, Gewichten en Codenummers 2003; Department of Human Nutrition, Wageningen UR: Wageningen, The Netherlands, 2003. [Google Scholar]
- Netherlands Nutrition Centre. Dutch Food Composition Database 2006 (Nevo-Table 2006); Netherlands Nutrition Centre (Voedingscentrum): Den Haag, The Netherlands, 2006. [Google Scholar]
- Willett, W.C.; Howe, G.R.; Kushi, L.H. Adjustment for total energy intake in epidemiologic studies. Am. J. Clin. Nutr. 1997, 65, 1220S–1228S. [Google Scholar] [CrossRef] [PubMed]
- Steenweg-de Graaff, J.C.; Tiemeier, H.; Basten, M.G.; Rijlaarsdam, J.; Demmelmair, H.; Koletzko, B.; Hofman, A.; Jaddoe, V.W.; Verhulst, F.C.; Roza, S.J. Maternal lc-pufa status during pregnancy and child problem behavior: The generation r study. Pediatr. Res. 2015, 77, 489–497. [Google Scholar] [CrossRef] [PubMed]
- Rosner, B.; Willett, W.C. Interval estimates for correlation coefficients corrected for within-person variation: Implications for study design and hypothesis testing. Am. J. Epidemiol. 1988, 127, 377–386. [Google Scholar] [CrossRef]
- McNaughton, S.A.; Hughes, M.C.; Marks, G.C. Validation of a ffq to estimate the intake of pufa using plasma phospholipid fatty acids and weighed foods records. Br. J. Nutr. 2007, 97, 561–568. [Google Scholar] [CrossRef]
- Swierk, M.; Williams, P.G.; Wilcox, J.; Russell, K.G.; Meyer, B.J. Validation of an australian electronic food frequency questionnaire to measure polyunsaturated fatty acid intake. Nutrition 2011, 27, 641–646. [Google Scholar] [CrossRef][Green Version]
- Parra, M.S.; Schnaas, L.; Meydani, M.; Perroni, E.; Martinez, S.; Romieu, I. Erythrocyte cell membrane phospholipid levels compared against reported dietary intakes of polyunsaturated fatty acids in pregnant mexican women. Public Health Nutr. 2002, 5, 931–937. [Google Scholar] [CrossRef]
- Parker, G.; McClure, G.; Hegarty, B.D.; Smith, I.G. The validity of a food frequency questionnaire as a measure of pufa status in pregnancy. BMC Pregnancy Childbirth 2015, 15, 60. [Google Scholar] [CrossRef]
- Arab, L. Biomarkers of fat and fatty acid intake. J. Nutr. 2003, 133 (Suppl. S3), 925s–932s. [Google Scholar] [CrossRef]
- van ’t Veer, P.; Kardinaal, A.F.; Bausch-Goldbohm, R.A.; Kok, F.J. Biomarkers for validation. Eur. J. Clin. Nutr. 1993, 47 (Suppl. S2), S58–S63. [Google Scholar]
- Cade, J.; Thompson, R.; Burley, V.; Warm, D. Development, validation and utilisation of food-frequency questionnaires—A review. Public Health Nutr. 2002, 5, 567–587. [Google Scholar] [CrossRef] [PubMed]
- Freedman, L.S.; Commins, J.M.; Moler, J.E.; Arab, L.; Baer, D.J.; Kipnis, V.; Midthune, D.; Moshfegh, A.J.; Neuhouser, M.L.; Prentice, R.L.; et al. Pooled results from 5 validation studies of dietary self-report instruments using recovery biomarkers for energy and protein intake. Am. J. Epidemiol. 2014, 180, 172–188. [Google Scholar] [CrossRef] [PubMed]
- Subar, A.F.; Freedman, L.S.; Tooze, J.A.; Kirkpatrick, S.I.; Boushey, C.; Neuhouser, M.L.; Thompson, F.E.; Potischman, N.; Guenther, P.M.; Tarasuk, V.; et al. Addressing current criticism regarding the value of self-report dietary data. J. Nutr. 2015, 145, 2639–2645. [Google Scholar] [CrossRef]
- Conrad, J.; Nothlings, U. Innovative approaches to estimate individual usual dietary intake in large-scale epidemiological studies. Proc. Nutr. Soc. 2017, 76, 213–219. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable (Unit) | Value * |
|---|---|
| Age (years) | 31.8 ± 4.0 |
| Gestational age at enrollment (weeks) | 15.6 (8.4–20.4) |
| Weight (kg) | 66.0 (53.2–87.2) |
| Height (m) | 1.72 ± 0.1 |
| Body mass index (kg/m2) | 22.0 (18.4–29.7) |
| Basal metabolic rate (kcal) [20] | 1756 (1632–1916) |
| Educational level | |
| Low | 1 (1.2%) |
| Medium | 7 (8.4%) |
| High | 75 (90.4%) |
| Vegetarian diet | |
| No | 78 (94.0%) |
| No meat and no fish | 2 (2.4%) |
| No meat | 3 (3.6%) |
| Parity | |
| Nulliparous | 50 (60.2%) |
| Multiparous | 33 (39.8%) |
| Smoking | |
| No | 72 (86.7%) |
| Yes, until pregnancy was known | 7 (8.4%) |
| Yes, continued | 4 (4.8%) |
| Folic acid supplement use | |
| No | 2 (2.4%) |
| When pregnancy was known | 24 (28.9%) |
| Later in pregnancy | 3 (3.6%) |
| Preconceptionally | 54 (65.1) |
| Biomarker concentrations at median 19.8 weeks (90% range 13.4–23.9) of gestation | |
| Serum folate (nmol/L) | 30.6 ± 8.9 |
| Red blood cell folate (nmol/L) | 1479.7 ± 301.5 |
| Serum vitamin B12 (pmol/L) | 247.0 ± 74.1 |
| Plasma saturated fatty acids (mg/L) | 688.6 ± 117.5 |
| Plasma monounsaturated fatty acids (mg/L) | 217.3 ± 37.3 |
| Plasma polyunsaturated fatty acids (mg/L) | 709.4 ± 113.9 |
| Plasma linoleic acid (mg/L) | 349.0 ± 59.4 |
| Estimated Nutrient Intakes (Median (90% Range)) | Pearson’s Correlation Coefficients | Intraclass Correlation Coefficients | ||||||
|---|---|---|---|---|---|---|---|---|
| FFQ | 24 h-Recalls | p- Value | Crude | Energy- Adjusted † | De-Attenuated ‡ | Crude | Energy Adjusted | |
| Energy (kcal/d) | 2099 (1344–2995) | 2123 (1528–2830) | 0.76 | 0.23 * | - | 0.30 | 0.36 * | - |
| Total protein (g/d) | 74.7 (48.3–109.0) | 77.9 (56.0–105.6) | 0.31 | 0.25 * | 0.46 ** | 0.39 | 0.39 ** | 0.62 ** |
| Vegetable protein (g/d) | 32.3 (20.5–53.1) | 32.7 (19.7–48.0) | 0.43 | 0.52 ** | 0.65 ** | 0.74 | 0.62 ** | 0.79 ** |
| Animal protein (g/d) | 43.7 (23.4–62.9) | 44.9 (24.4–65.7) | 0.15 | 0.27 * | 0.46 ** | 0.46 | 0.42 ** | 0.62 ** |
| Total fat (g/d) § | 87.1 (53.0–140.2) | 80.1 (49.9–120.1) | 0.05 | 0.28 * | 0.42 ** | 0.41 | 0.43 ** | 0.58 ** |
| SFA (g/d) § | 28.4 (14.9–48.9) | 31.0 (17.0–48.6) | 0.19 | 0.40 ** | 0.60 ** | 0.60 | 0.57 ** | 0.75 ** |
| MUFA (g/d) § | 30.2 (17.2–49.2) | 30.0 (16.0–45.4) | 0.02 | 0.25 * | 0.33 ** | 0.38 | 0.40 * | 0.47 ** |
| PUFA (g/d) § | 19.5 (10.6–33.7) | 14.2 (7.9–22.6) | <0.001 | 0.42 ** | 0.54 ** | 0.69 | 0.59 ** | 0.69 ** |
| Total carbohydrates (g/d) | 248.3 (148.2–358.0) | 266.7 (183.2–398.4) | 0.02 | 0.32 ** | 0.43 ** | 0.42 | 0.49 ** | 0.60 ** |
| Mono- and disaccharides (g/d) | | 134.6 (72.2–213.7) | 128.8 (81.1–253.4) | 0.75 | 0.44 ** | 0.58 ** | 0.50 | 0.61 ** | 0.74 ** |
| Polysaccharides (g/d) | 112.1 (68.7–165.5) | 131.8 (86.3–193.3) | <0.001 | 0.33 ** | 0.41 ** | 0.55 | 0.5 ** | 0.58 ** |
| Fiber (g/d) | 24.5 (12.5–42.4) | 23.8 (13.4–37.3) | 0.66 | 0.63 ** | 0.65 ** | 0.88 | 0.77 ** | 0.77 ** |
| Calcium (mg/d) | 1145 (516–2035) | 1189 (779–1657) | 0.71 | 0.45 ** | 0.60 ** | 0.68 | 0.59 ** | 0.74 ** |
| Phosphor (g/d) | 1535 (894–2285) | 1531 (1080–2200) | 0.78 | 0.42 ** | 0.62 ** | 0.60 | 0.58 ** | 0.76 ** |
| Total iron (mg/d) | 12.2 (7.5–18.8) | 11.9 (8.1–17.3) | 0.93 | 0.47 ** | 0.45 ** | 0.62 | 0.64 ** | 0.61 ** |
| Retinol equivalents (mg/d) § | 877 (380–1351) | 671 (293–1844) | 0.01 | 0.37 ** | 0.17 | 0.62 | 0.52 ** | 0.22 |
| Vitamin B1 (mg/d) § | 1.2 (0.6–1.9) | 1.3 (0.8–2.5) | 0.16 | 0.34 ** | 0.24 * | 0.60 | 0.5 ** | 0.35 * |
| Vitamin B2 (mg/d) | 1.5 (0.8–2.5) | 1.7 (0.9–2.4) | 0.007 | 0.47 ** | 0.58 ** | 0.61 | 0.64 ** | 0.72 ** |
| Vitamin B6 (mg/d) § | 1.9 (1.0–3.2) | 1.9 (1.1–3.4) | 0.40 | 0.49 ** | 0.55 ** | 0.59 | 0.65 ** | 0.67 ** |
| Vitamin B12 (µg/d) § | 3.1 (1.7–4.9) | 3.3 (1.6–7.0) | 0.20 | 0.24 * | 0.24 * | 0.46 | 0.37 * | 0.33 * |
| Folate equivalents (µg/d) § | 178 (117–305) | 213 (114–402) | 0.001 | 0.43 ** | 0.58 ** | 0.62 | 0.59 ** | 0.67 ** |
| Vitamin E (mg/d) | 17.2 (9.0–28.8) | 14.2 (6.8–21.9) | <0.001 | 0.18 | 0.23 * | 0.27 | 0.29 | 0.37 * |
| Vitamin C (mg/d) | | 101.8 (46.6–215.1) | 120.7 (41.6–260.1) | 0.01 | 0.52 ** | 0.44 ** | 0.65 | 0.68 ** | 0.59 ** |
| Fatty Acids (Plasma Phospholipids) | |||||||
|---|---|---|---|---|---|---|---|
| Serum Folate | RBC Folate | Serum Vitamin B12 | Saturated Fatty Acids | Mono- Unsaturated Fatty Acids | Poly- Unsaturated Fatty Acids | Linoleic Acid | |
| n = 80 | n = 77 | n = 80 | n = 78 | n = 78 | n = 78 | n = 78 | |
| Sample correlations | |||||||
| rQM | 0.24 | 0.09 | 0.33 | 0.01 | −0.17 | −0.02 | 0.16 |
| (95% CI) | (−0.01, 0.47) | (−0.19, 0.37) | (0.08, 0.54) | (−0.19, 0.21) | (−0.36, 0.05) | (−0.21, 019) | (−0.02, 0.33) |
| rRM | 0.14 | 0.05 | 0.07 | 0.09 | −0.12 | −0.08 | 0.13 |
| (95% CI) | (−0.07, 0.37) | (−0.20, 0.30) | (−0.15, 0.27) | (−0.10, 0.29) | (−0.35, 0.10) | (−0.30, 0.14) | (−0.10, 0.36) |
| rQR | 0.43 | 0.41 | 0.24 | 0.41 | 0.24 | 0.42 | 0.36 |
| (95% CI) | (0.22, 0.59) | (0.19, 0.58) | (0.07, 0.41) | (0.18, 0.62) | (−0.01, 0.46) | (0.17, 0.62) | (0.10, 0.59) |
| Validity coefficient * | |||||||
| ρQT | 0.86 | 0.86 | 1.00 | 0.22 | 0.58 | 0.33 | 0.67 |
| (95% CI) | (0.36, 1.00) | (0.18, 1.00) | (0.42, 1.00) | (0.12, 1.00) | (0.13, 1.00) | (0.13, 1.00) | (0.20, 1.00) |
| Range † | 0.24–0.86 | 0.09–0.86 | 0.33–1.00 | 0.01–0.22 | −0.17–0.58 | −0.02–0.33 | 0.16–0.67 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Voortman, T.; Steegers-Theunissen, R.P.M.; Bergen, N.E.; Jaddoe, V.W.V.; Looman, C.W.N.; Kiefte-de Jong, J.C.; Schalekamp-Timmermans, S. Validation of a Semi-Quantitative Food-Frequency Questionnaire for Dutch Pregnant Women from the General Population Using the Method or Triads. Nutrients 2020, 12, 1341. https://doi.org/10.3390/nu12051341
Voortman T, Steegers-Theunissen RPM, Bergen NE, Jaddoe VWV, Looman CWN, Kiefte-de Jong JC, Schalekamp-Timmermans S. Validation of a Semi-Quantitative Food-Frequency Questionnaire for Dutch Pregnant Women from the General Population Using the Method or Triads. Nutrients. 2020; 12(5):1341. https://doi.org/10.3390/nu12051341
Chicago/Turabian StyleVoortman, Trudy, Régine P. M. Steegers-Theunissen, Nienke E. Bergen, Vincent W. V. Jaddoe, Caspar W. N. Looman, Jessica C. Kiefte-de Jong, and Sarah Schalekamp-Timmermans. 2020. "Validation of a Semi-Quantitative Food-Frequency Questionnaire for Dutch Pregnant Women from the General Population Using the Method or Triads" Nutrients 12, no. 5: 1341. https://doi.org/10.3390/nu12051341
APA StyleVoortman, T., Steegers-Theunissen, R. P. M., Bergen, N. E., Jaddoe, V. W. V., Looman, C. W. N., Kiefte-de Jong, J. C., & Schalekamp-Timmermans, S. (2020). Validation of a Semi-Quantitative Food-Frequency Questionnaire for Dutch Pregnant Women from the General Population Using the Method or Triads. Nutrients, 12(5), 1341. https://doi.org/10.3390/nu12051341