The Effects of Different Degrees of Carbohydrate Restriction and Carbohydrate Replacement on Cardiometabolic Risk Markers in Humans—A Systematic Review and Meta-Analysis



Abstract
1. Introduction
2. Methods
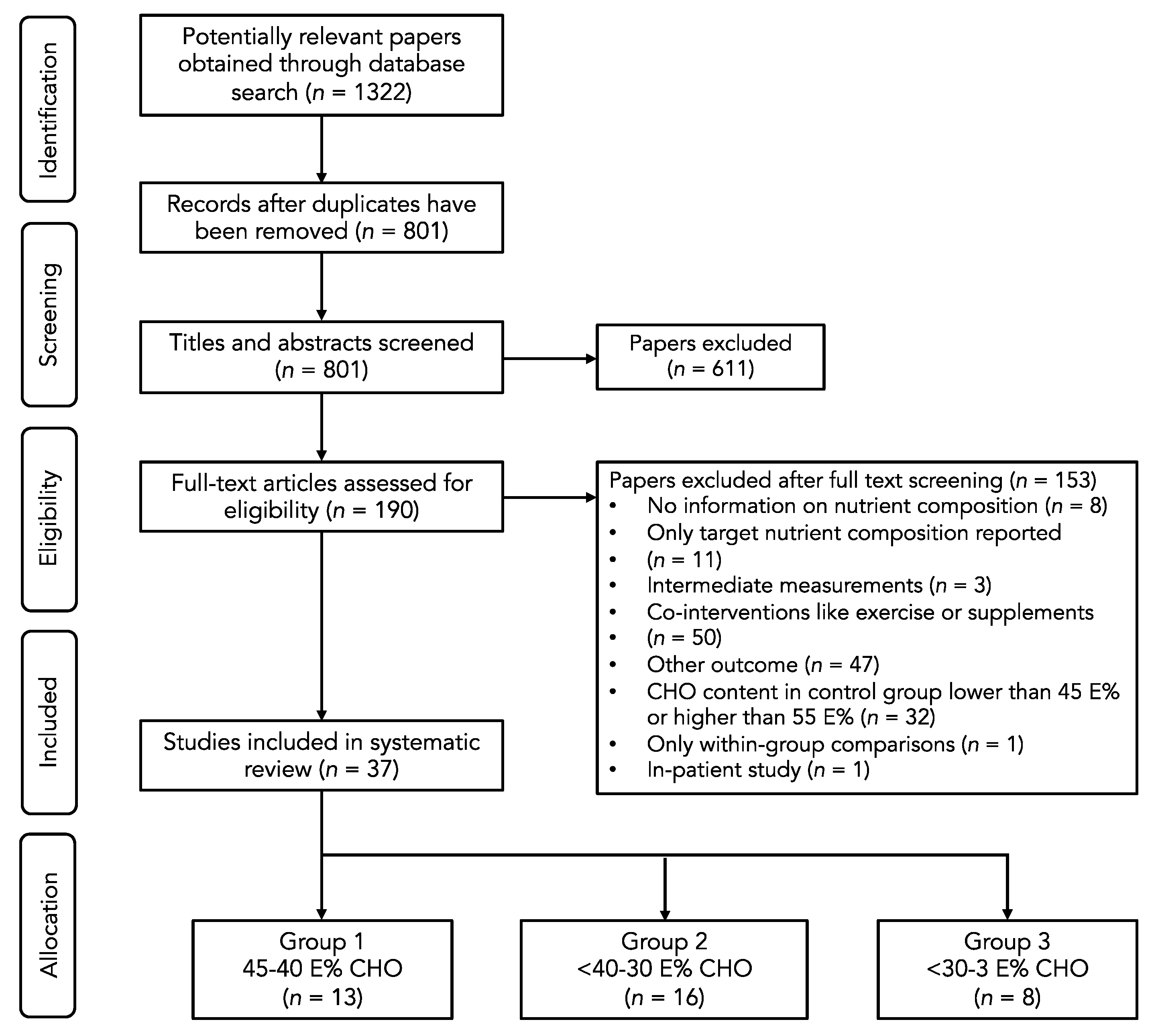
2.1. Search Strategy
2.2. Study Selection
2.3. Data Collection
2.4. Statistical Analyses
3. Results and Discussion
3.1. Group 1: Effects of Moderate-Low CHO Diets (<45–40 E%)
3.2. Group 2: Effects of Low CHO Diets (<40–30 E%)
3.3. Group 3: Effects of Very Low-Carbohydrate Diets (<30–3 E%)
3.4. Effects of the Degree of CHO Restriction
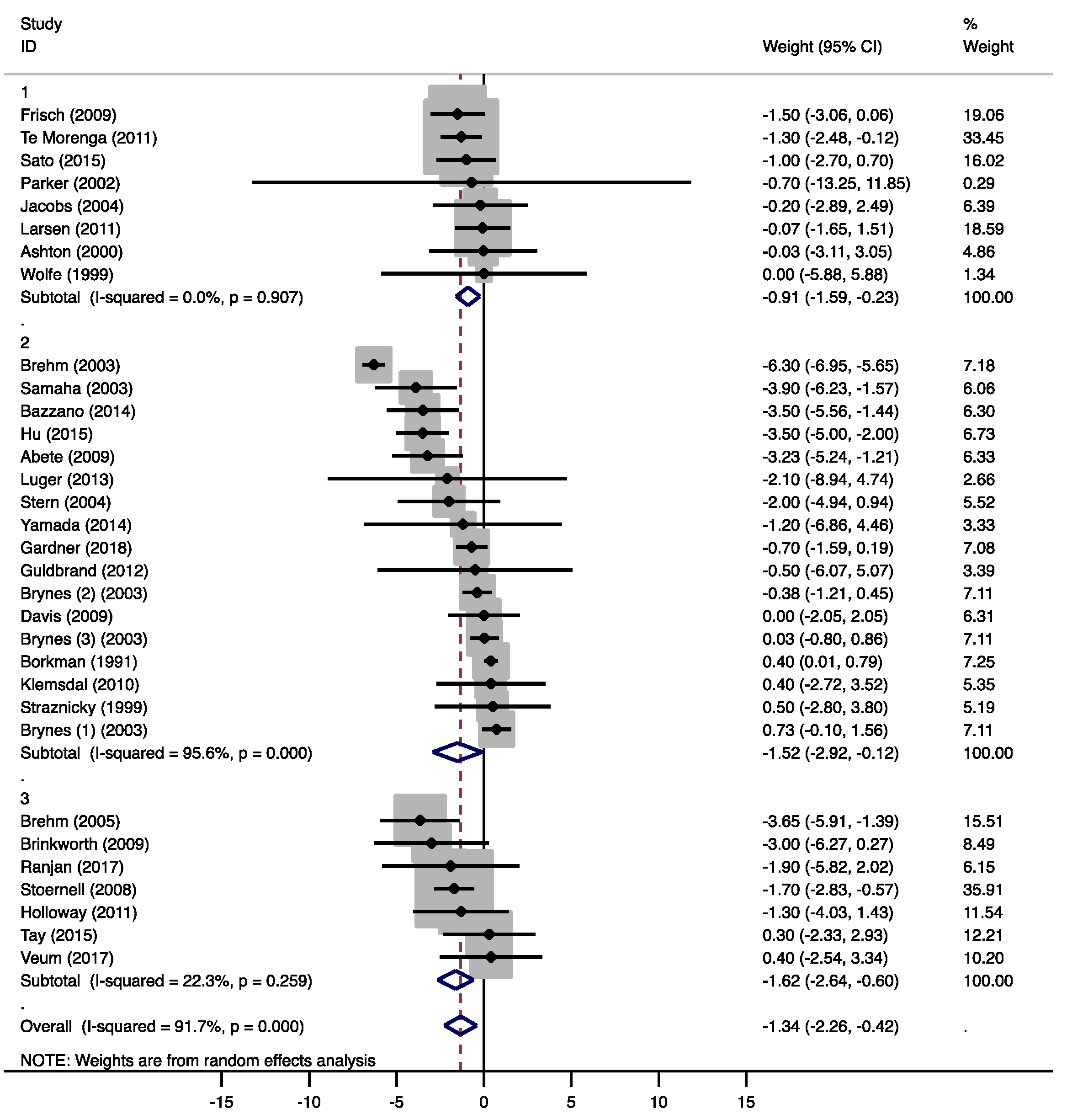
3.4.1. Weight
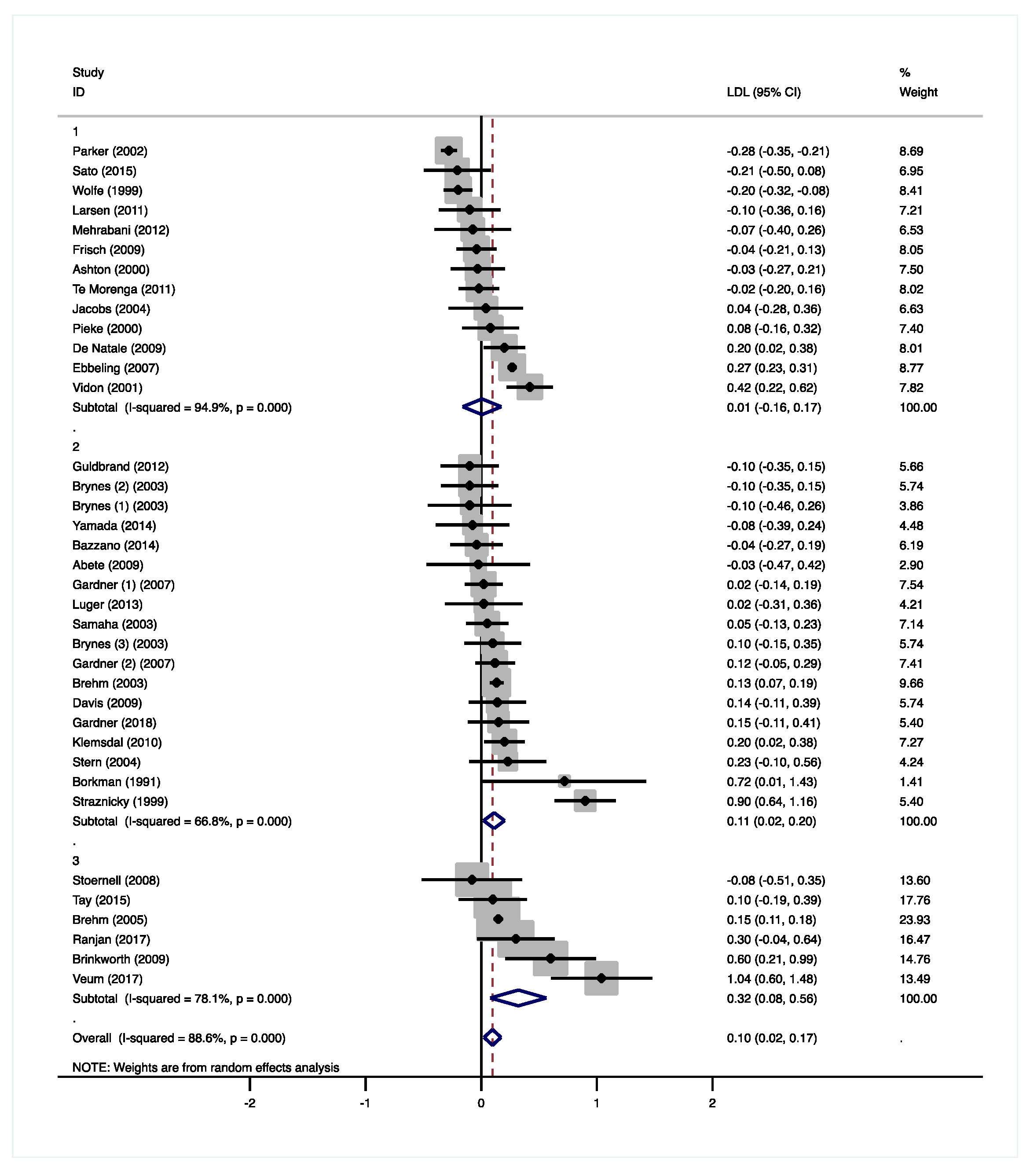
3.4.2. Total Cholesterol and LDL-Cholesterol
3.4.3. HDL Cholesterol
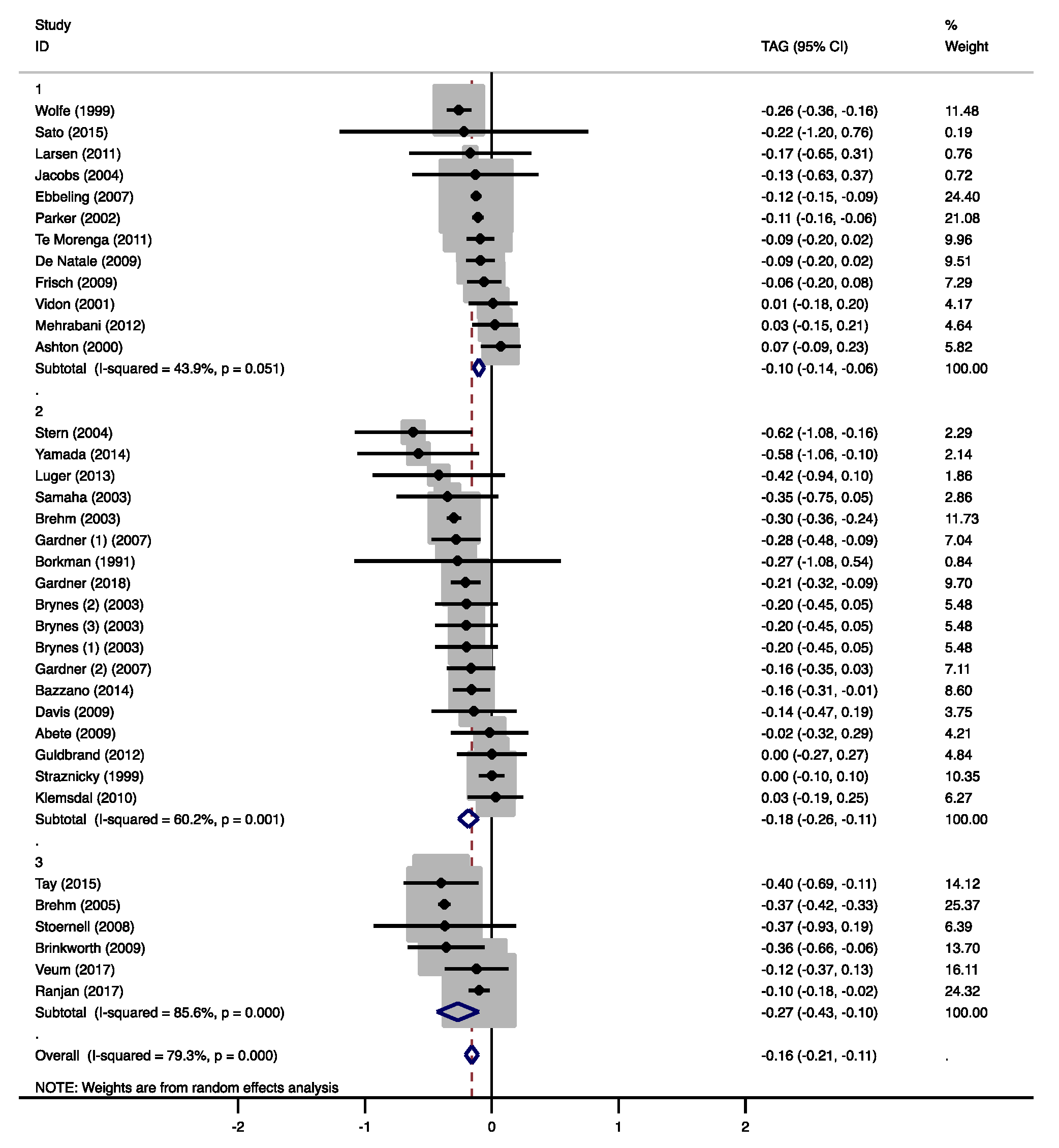
3.4.4. Triacylglycerol
3.4.5. Glucose and Insulin
3.4.6. Blood Pressure
3.5. Subgroup Analysis
4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Arora, S.K.; McFarlane, S.I. The case for low carbohydrate diets in diabetes management. Nutr. Metab. 2005, 2, 16. [Google Scholar] [CrossRef]
- Hall, K.D.; Chung, S.T. Low-carbohydrate diets for the treatment of obesity and type 2 diabetes. Curr. Opin. Clin. Nutr. Metab. Care 2018, 21, 308–312. [Google Scholar] [CrossRef] [PubMed]
- Hu, T.; Bazzano, L.A. The low-carbohydrate diet and cardiovascular risk factors: Evidence from epidemiologic studies. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 337–343. [Google Scholar] [CrossRef]
- Bilsborough, S.A.; Crowe, T.C. Low-carbohydrate diets: What are the potential short- and long-term health implications? Asia Pac. J. Clin. Nutr. 2003, 12, 396–404. [Google Scholar] [PubMed]
- EFSA (European Food Safety Authority). Dietary Reference Values for nutrients. Summary Report. EFSA Supporting Publ. 2017, 14, e15121. [Google Scholar] [CrossRef]
- Brouns, F. Overweight and diabetes prevention: Is a low-carbohydrate-high-fat diet recommendable? Eur. J. Nutr. 2018, 57, 1301–1312. [Google Scholar] [CrossRef] [PubMed]
- Westman, E.C.; Feinman, R.D.; Mavropoulos, J.C.; Vernon, M.C.; Volek, J.S.; Wortman, J.A.; Yancy, W.S.; Phinney, S.D. Low-carbohydrate nutrition and metabolism. Am. J. Clin. Nutr. 2007, 86, 276–284. [Google Scholar] [CrossRef]
- Johnstone, A.M.; Horgan, G.W.; Murison, S.D.; Bremner, D.M.; Lobley, G.E. Effects of a high-protein ketogenic diet on hunger, appetite, and weight loss in obese men feeding ad libitum. Am. J. Clin. Nutr. 2008, 87, 44–55. [Google Scholar] [CrossRef]
- Bergqvist, A.G.C. Long-term monitoring of the ketogenic diet: Do’s and Don’ts. Epilepsy Res. 2012, 100, 261–266. [Google Scholar] [CrossRef]
- Johnston, C.S.; Tjonn, S.L.; Swan, P.D.; White, A.; Hutchins, H.; Sears, B. Ketogenic low-carbohydrate diets have no metabolic advantage over nonketogenic low-carbohydrate diets. Am. J. Clin. Nutr. 2006, 83, 1055–1061. [Google Scholar] [CrossRef]
- Saslow, L.R.; Kim, S.; Daubenmier, J.J.; Moskowitz, J.T.; Phinney, S.D.; Goldman, V.; Murphy, E.J.; Cox, R.M.; Moran, P.; Hecht, F.M. A randomized pilot trial of a moderate carbohydrate diet compared to a very low carbohydrate diet in overweight or obese individuals with type 2 diabetes mellitus or prediabetes. PLoS ONE 2014, 9, e91027. [Google Scholar] [CrossRef] [PubMed]
- Harvey, C.J.D.C.; Schofield, G.M.; Zinn, C.; Thornley, S.J.; Crofts, C.; Merien, F.L.R. Low-carbohydrate diets differing in carbohydrate restriction improve cardiometabolic and anthropometric markers in healthy adults: A randomised clinical trial. Peerj 2019, 7. [Google Scholar] [CrossRef] [PubMed]
- Brown, L.; Rosner, B.; Willett, W.W.; Sacks, F.M. Cholesterol-lowering effects of dietary fiber: A meta-analysis. Am. J. Clin. Nutr. 1999, 69, 30–42. [Google Scholar] [CrossRef] [PubMed]
- Mensink, R.P.; Zock, P.L.; Kester, A.D.; Katan, M.B. Effects of dietary fatty acids and carbohydrates on the ratio of serum total to HDL cholesterol and on serum lipids and apolipoproteins: A meta-analysis of 60 controlled trials. Am. J. Clin. Nutr. 2003, 77, 1146–1155. [Google Scholar] [CrossRef]
- Chandalia, M.; Garg, A.; Lutjohann, D.; von Bergmann, K.; Grundy, S.M.; Brinkley, L.J. Beneficial effects of high dietary fiber intake in patients with type 2 diabetes mellitus. N. Engl. J. Med. 2000, 342, 1392–1398. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. Ann. Intern. Med. 2009, 151, W65–W94. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. Bmj-Brit. Med. J. 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Sato, J.; Kanazawa, A.; Makita, S.; Hatae, C.; Komiya, K.; Shimizu, T.; Ikeda, F.; Tamura, Y.; Ogihara, T.; Mita, T.; et al. A randomized controlled trial of 130 g/day low-carbohydrate diet in type 2 diabetes with poor glycemic control. Clin. Nutr. 2017, 36, 992–1000. [Google Scholar] [CrossRef]
- Larsen, R.N.; Mann, N.J.; Maclean, E.; Shaw, J.E. The effect of high-protein, low-carbohydrate diets in the treatment of type 2 diabetes: A 12 month randomised controlled trial. Diabetologia 2011, 54, 731–740. [Google Scholar] [CrossRef]
- De Natale, C.; Annuzzi, G.; Bozzetto, L.; Mazzarella, R.; Costabile, G.; Ciano, O.; Riccardi, G.; Rivellese, A.A. Effects of a plant-based high-carbohydrate/high-fiber diet versus high-monounsaturated fat/low-carbohydrate diet on postprandial lipids in type 2 diabetic patients. Diabetes Care 2009, 32, 2168–2173. [Google Scholar] [CrossRef] [PubMed]
- Parker, B.; Noakes, M.; Luscombe, N.; Clifton, P. Effect of a high-protein, high-monounsaturated fat weight loss diet on glycemic control and lipid levels in type 2 diabetes. Diabetes Care 2002, 25, 425–430. [Google Scholar] [CrossRef]
- Mehrabani, H.H.; Salehpour, S.; Amiri, Z.; Farahani, S.J.; Meyer, B.J.; Tahbaz, F. Beneficial effects of a high-protein, low-glycemic-load hypocaloric diet in overweight and obese women with polycystic ovary syndrome: A randomized controlled intervention study. J. Am. Coll. Nutr. 2012, 31, 117–125. [Google Scholar] [CrossRef]
- Te Morenga, L.A.; Levers, M.T.; Williams, S.M.; Brown, R.C.; Mann, J. Comparison of high protein and high fiber weight-loss diets in women with risk factors for the metabolic syndrome: A randomized trial. Nutr. J. 2011, 10. [Google Scholar] [CrossRef] [PubMed]
- Frisch, S.; Zittermann, A.; Berthold, H.K.; Gotting, C.; Kuhn, J.; Kleesiek, K.; Stehle, P.; Kortke, H. A randomized controlled trial on the efficacy of carbohydrate-reduced or fat-reduced diets in patients attending a telemedically guided weight loss program. Cardiovasc. Diabetol. 2009, 8. [Google Scholar] [CrossRef] [PubMed]
- Ebbeling, C.B.; Leidig, M.M.; Feldman, H.A.; Lovesky, M.M.; Ludwig, D.S. Effects of a low-glycemic load vs low-fat diet in obese young adults: A randomized trial. JAMA 2007, 297, 2092–2102. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, B.; De Angelis-Schierbaum, G.; Egert, S.; Assmann, G.; Kratz, M. Individual serum triglyceride responses to high-fat and low-fat diets differ in men with modest and severe hypertriglyceridemia. J. Nutr. 2004, 134, 1400–1405. [Google Scholar] [CrossRef] [PubMed]
- Pieke, B.; von Eckardstein, A.; Gulbahce, E.; Chirazi, A.; Schulte, H.; Assmann, G.; Wahrburg, U. Treatment of hypertriglyceridemia by two diets rich either in unsaturated fatty acids or in carbohydrates: Effects on lipoprotein subclasses, lipolytic enzymes, lipid transfer proteins, insulin and leptin. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1286–1296. [Google Scholar] [CrossRef] [PubMed]
- Vidon, C.; Boucher, P.; Cachefo, A.; Peroni, O.; Diraison, F.; Beylot, M. Effects of isoenergetic high-carbohydrate compared with high-fat diets on human cholesterol synthesis and expression of key regulatory genes of cholesterol metabolism. Am. J. Clin. Nutr. 2001, 73, 878–884. [Google Scholar] [CrossRef]
- Ashton, E.L.; Pomeroy, S.; Foster, J.E.; Kaye, R.S.; Nestel, P.J.; Ball, M. Diet high in monounsaturated fat does not have a different effect on arterial elasticity than a low-fat, high-carbohydrate diet. J. Am. Diet. Assoc. 2000, 100, 537–542. [Google Scholar] [CrossRef]
- Wolfe, B.M.; Piche, L.A. Replacement of carbohydrate by protein in a conventional-fat diet reduces cholesterol and triglyceride concentrations in healthy normolipidemic subjects. Clin. Investig. Med. 1999, 22, 140–148. [Google Scholar]
- Harris, W.S. n-3 fatty acids and serum lipoproteins: Human studies. Am. J. Clin. Nutr. 1997, 65, 1645S–1654S. [Google Scholar] [CrossRef] [PubMed]
- Yamada, Y.; Uchida, J.; Izumi, H.; Tsukamoto, Y.; Inoue, G.; Watanabe, Y.; Irie, J.; Yamada, S. A non-calorie-restricted low-carbohydrate diet is effective as an alternative therapy for patients with type 2 diabetes. Intern. Med. 2014, 53, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Luger, M.; Holstein, B.; Schindler, K.; Kruschitz, R.; Ludvik, B. Feasibility and efficacy of an isocaloric high-protein vs. standard diet on insulin requirement, body weight and metabolic parameters in patients with type 2 diabetes on insulin therapy. Exp. Clin. Endocrinol. Diabetes 2013, 121, 286–294. [Google Scholar] [CrossRef]
- Guldbrand, H.; Dizdar, B.; Bunjaku, B.; Lindstrom, T.; Bachrach-Lindstrom, M.; Fredrikson, M.; Ostgren, C.J.; Nystrom, F.H. In type 2 diabetes, randomisation to advice to follow a low-carbohydrate diet transiently improves glycaemic control compared with advice to follow a low-fat diet producing a similar weight loss. Diabetologia 2012, 55, 2118–2127. [Google Scholar] [CrossRef]
- Davis, N.J.; Tomuta, N.; Schechter, C.; Isasi, C.R.; Segal-Isaacson, C.J.; Stein, D.; Zonszein, J.; Wylie-Rosett, J. Comparative study of the effects of a 1-year dietary intervention of a low-carbohydrate diet versus a low-fat diet on weight and glycemic control in type 2 diabetes. Diabetes Care 2009, 32, 1147–1152. [Google Scholar] [CrossRef]
- Klemsdal, T.O.; Holme, I.; Nerland, H.; Pedersen, T.R.; Tonstad, S. Effects of a low glycemic load diet versus a low-fat diet in subjects with and without the metabolic syndrome. Nutr. Metab. Cardiovasc. Dis. 2010, 20, 195–201. [Google Scholar] [CrossRef]
- Brynes, A.E.; Mark Edwards, C.; Ghatei, M.A.; Dornhorst, A.; Morgan, L.M.; Bloom, S.R.; Frost, G.S. A randomised four-intervention crossover study investigating the effect of carbohydrates on daytime profiles of insulin, glucose, non-esterified fatty acids and triacylglycerols in middle-aged men. Br. J. Nutr. 2003, 89, 207–218. [Google Scholar] [CrossRef]
- Gardner, C.D.; Trepanowski, J.F.; Del Gobbo, L.C.; Hauser, M.E.; Rigdon, J.; Ioannidis, J.P.A.; Desai, M.; King, A.C. Effect of Low-Fat vs Low-Carbohydrate Diet on 12-Month Weight Loss in Overweight Adults and the Association With Genotype Pattern or Insulin Secretion: The DIETFITS Randomized Clinical Trial. JAMA 2018, 319, 667–679. [Google Scholar] [CrossRef]
- Bazzano, L.A.; Hu, T.; Reynolds, K.; Yao, L.; Bunol, C.; Liu, Y.; Chen, C.S.; Klag, M.J.; Whelton, P.K.; He, J. Effects of low-carbohydrate and low-fat diets: A randomized trial. Ann. Intern. Med. 2014, 161, 309–318. [Google Scholar] [CrossRef]
- Abete, I.; Parra, D.; De Morentin, B.M.; Alfredo Martinez, J. Effects of two energy-restricted diets differing in the carbohydrate/protein ratio on weight loss and oxidative changes of obese men. Int. J. Food Sci. Nutr. 2009, 60, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Gardner, C.D.; Kiazand, A.; Alhassan, S.; Kim, S.; Stafford, R.S.; Balise, R.R.; Kraemer, H.C.; King, A.C. Comparison of the Atkins, Zone, Ornish, and LEARN diets for change in weight and related risk factors among overweight premenopausal women: The A TO Z Weight Loss Study: A randomized trial. JAMA 2007, 297, 969–977. [Google Scholar] [CrossRef] [PubMed]
- Brehm, B.J.; Seeley, R.J.; Daniels, S.R.; D’Alessio, D.A. A randomized trial comparing a very low carbohydrate diet and a calorie-restricted low fat diet on body weight and cardiovascular risk factors in healthy women. J. Clin. Endocrinol. Metab. 2003, 88, 1617–1623. [Google Scholar] [CrossRef] [PubMed]
- Stern, L.; Iqbal, N.; Seshadri, P.; Chicano, K.L.; Daily, D.A.; McGrory, J.; Williams, M.; Gracely, E.J.; Samaha, F.F. The effects of low-carbohydrate versus conventional weight loss diets in severely obese adults: One-year follow-up of a randomized trial. Ann. Intern. Med. 2004, 140, 778–785. [Google Scholar] [CrossRef] [PubMed]
- Samaha, F.F.; Iqbal, N.; Seshadri, P.; Chicano, K.L.; Daily, D.A.; McGrory, J.; Williams, T.; Williams, M.; Gracely, E.J.; Stern, L. A low-carbohydrate as compared with a low-fat diet in severe obesity. N. Engl. J. Med. 2003, 348, 2074–2081. [Google Scholar] [CrossRef]
- Hu, T.; Yao, L.; Reynolds, K.; Whelton, P.K.; Niu, T.; Li, S.; He, J.; Bazzano, L.A. The Effects of a Low-Carbohydrate Diet vs. a Low-Fat Diet on Novel Cardiovascular Risk Factors: A Randomized Controlled Trial. Nutrients 2015, 7, 7978–7994. [Google Scholar] [CrossRef]
- Straznicky, N.E.; O’Callaghan, C.J.; Barrington, V.E.; Louis, W.J. Hypotensive effect of low-fat, high-carbohydrate diet can be independent of changes in plasma insulin concentrations. Hypertension 1999, 34, 580–585. [Google Scholar] [CrossRef]
- Borkman, M.; Campbell, L.V.; Chisholm, D.J.; Storlien, L.H. Comparison of the effects on insulin sensitivity of high carbohydrate and high fat diets in normal subjects. J. Clin. Endocrinol. Metab. 1991, 72, 432–437. [Google Scholar] [CrossRef]
- Ranjan, A.; Schmidt, S.; Damm-Frydenberg, C.; Holst, J.J.; Madsbad, S.; Norgaard, K. Short-term effects of a low carbohydrate diet on glycaemic variables and cardiovascular risk markers in patients with type 1 diabetes: A randomized open-label crossover trial. Diabetes Obes. Metab. 2017, 19, 1479–1484. [Google Scholar] [CrossRef]
- Tay, J.; Luscombe-Marsh, N.D.; Thompson, C.H.; Noakes, M.; Buckley, J.D.; Wittert, G.A.; Yancy, W.S., Jr.; Brinkworth, G.D. Comparison of low- and high-carbohydrate diets for type 2 diabetes management: A randomized trial. Am. J. Clin. Nutr. 2015, 102, 780–790. [Google Scholar] [CrossRef]
- Brehm, B.J.; Spang, S.E.; Lattin, B.L.; Seeley, R.J.; Daniels, S.R.; D’Alessio, D.A. The role of energy expenditure in the differential weight loss in obese women on low-fat and low-carbohydrate diets. J. Clin. Endocrinol. Metab. 2005, 90, 1475–1482. [Google Scholar] [CrossRef] [PubMed]
- Veum, V.L.; Laupsa-Borge, J.; Eng, O.; Rostrup, E.; Larsen, T.H.; Nordrehaug, J.E.; Nygard, O.K.; Sagen, J.V.; Gudbrandsen, O.A.; Dankel, S.N.; et al. Visceral adiposity and metabolic syndrome after very high-fat and low-fat isocaloric diets: A randomized controlled trial. Am. J. Clin. Nutr. 2017, 105, 85–99. [Google Scholar] [CrossRef]
- Brinkworth, G.D.; Noakes, M.; Buckley, J.D.; Keogh, J.B.; Clifton, P.M. Long-term effects of a very-low-carbohydrate weight loss diet compared with an isocaloric low-fat diet after 12 mo. Am. J. Clin. Nutr. 2009, 90, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Stoernell, C.K.; Tangney, C.C.; Rockway, S.W. Short-term changes in lipoprotein subclasses and C-reactive protein levels of hypertriglyceridemic adults on low-carbohydrate and low-fat diets. Nutr. Res. 2008, 28, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Holloway, C.J.; Cochlin, L.E.; Emmanuel, Y.; Murray, A.; Codreanu, I.; Edwards, L.M.; Szmigielski, C.; Tyler, D.J.; Knight, N.S.; Saxby, B.K.; et al. A high-fat diet impairs cardiac high-energy phosphate metabolism and cognitive function in healthy human subjects. Am. J. Clin. Nutr. 2011, 93, 748–755. [Google Scholar] [CrossRef] [PubMed]
- Chokkalingam, K.; Jewell, K.; Norton, L.; Littlewood, J.; van Loon, L.J.; Mansell, P.; Macdonald, I.A.; Tsintzas, K. High-fat/low-carbohydrate diet reduces insulin-stimulated carbohydrate oxidation but stimulates nonoxidative glucose disposal in humans: An important role for skeletal muscle pyruvate dehydrogenase kinase 4. J. Clin. Endocrinol. Metab. 2007, 92, 284–292. [Google Scholar] [CrossRef]
- Johnston, B.C.; Kanters, S.; Bandayrel, K.; Wu, P.; Naji, F.; Siemieniuk, R.A.; Ball, G.D.; Busse, J.W.; Thorlund, K.; Guyatt, G.; et al. Comparison of weight loss among named diet programs in overweight and obese adults: A meta-analysis. JAMA 2014, 312, 923–933. [Google Scholar] [CrossRef]
- Mansoor, N.; Vinknes, K.J.; Veierod, M.B.; Retterstol, K. Effects of low-carbohydrate diets v. low-fat diets on body weight and cardiovascular risk factors: A meta-analysis of randomised controlled trials. Br. J. Nutr. 2016, 115, 466–479. [Google Scholar] [CrossRef]
- Hamdy, O.; Tasabehji, M.W.; Elseaidy, T.; Tomah, S.; Ashrafzadeh, S.; Mottalib, A. Fat Versus Carbohydrate-Based Energy-Restricted Diets for Weight Loss in Patients With Type 2 Diabetes. Curr. Diabetes Rep. 2018, 18, 128. [Google Scholar] [CrossRef]
- Mensink, R.P. Effects of Saturated Fatty Acids on Serum Lipids and Lipoproteins: A Systematic Review and Regression Analysis; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Fielding, C.J.; Havel, R.J.; Todd, K.M.; Yeo, K.E.; Schloetter, M.C.; Weinberg, V.; Frost, P.H. Effects of dietary cholesterol and fat saturation on plasma lipoproteins in an ethnically diverse population of healthy young men. J. Clin. Investig. 1995, 95, 611–618. [Google Scholar] [CrossRef]
- Pasiakos, S.M.; Lieberman, H.R.; Fulgoni, V.L., 3rd. Higher-protein diets are associated with higher HDL cholesterol and lower BMI and waist circumference in US adults. J. Nutr. 2015, 145, 605–614. [Google Scholar] [CrossRef] [PubMed]
- Scherer, P.E.; Hill, J.A. Obesity, Diabetes, and Cardiovascular Diseases: A Compendium. Circ. Res. 2016, 118, 1703–1705. [Google Scholar] [CrossRef] [PubMed]
- McRae, M.P. Dietary Fiber Intake and Type 2 Diabetes Mellitus: An Umbrella Review of Meta-analyses. J. Chiropr. Med. 2018, 17, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Churuangsuk, C.; Kherouf, M.; Combet, E.; Lean, M. Low-carbohydrate diets for overweight and obesity: A systematic review of the systematic reviews. Obes. Rev. 2018, 19, 1700–1718. [Google Scholar] [CrossRef]
- Naude, C.E.; Schoonees, A.; Senekal, M.; Young, T.; Garner, P.; Volmink, J. Low carbohydrate versus isoenergetic balanced diets for reducing weight and cardiovascular risk: A systematic review and meta-analysis. PLoS ONE 2014, 9, e100652. [Google Scholar] [CrossRef]
- Nordmann, A.J.; Nordmann, A.; Briel, M.; Keller, U.; Yancy, W.S., Jr.; Brehm, B.J.; Bucher, H.C. Effects of low-carbohydrate vs low-fat diets on weight loss and cardiovascular risk factors: A meta-analysis of randomized controlled trials. Arch. Intern. Med. 2006, 166, 285–293. [Google Scholar] [CrossRef]
- Van Zuuren, E.J.; Fedorowicz, Z.; Kuijpers, T.; Pijl, H. Effects of low-carbohydrate- compared with low-fat-diet interventions on metabolic control in people with type 2 diabetes: A systematic review including GRADE assessments. Am. J. Clin. Nutr. 2018, 108, 300–331. [Google Scholar] [CrossRef]
- Bueno, N.B.; de Melo, I.S.; de Oliveira, S.L.; da Rocha Ataide, T. Very-low-carbohydrate ketogenic diet v. low-fat diet for long-term weight loss: A meta-analysis of randomised controlled trials. Br. J. Nutr. 2013, 110, 1178–1187. [Google Scholar] [CrossRef]
- Bansal, S.; Buring, J.E.; Rifai, N.; Mora, S.; Sacks, F.M.; Ridker, P.M. Fasting compared with nonfasting triglycerides and risk of cardiovascular events in women. JAMA 2007, 298, 309–316. [Google Scholar] [CrossRef]
- McKeown, N.M.; Meigs, J.B.; Liu, S.; Saltzman, E.; Wilson, P.W.F.; Jacques, P.F. Carbohydrate nutrition, insulin resistance, and the prevalence of the metabolic syndrome in the Framingham Offspring Cohort. Diabetes Care 2004, 27, 538–546. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Characteristics | Diet Changes | Diet Effect | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author And Year | Study Design | LCD vs. MCD | Duration | Participants | kcal | CHO | Fat | Prot | Weight (kg) | TC (mmol/L) | LDL−C | HDL−C | TAG | Glucose (mmol/L) | Insulin (mU/mL) | Systolic/ |
| (mmol/L) | (mmol/L) | (mmol/L) | Diastolic BP (mmHg) | |||||||||||||
| Sato [19] | Parallel | Isocaloric | 6 months | 62 participants with T2D | −277 | −7.3 | 5.6 | 2.7 | ↓ −1.0 | = | = | = | ||||
| 2017 | ||||||||||||||||
| Larsen [20] 2011 | Parallel | Isocaloric with ER | 12 months | 99 participants with T2D | 75 | −5.2 | −0.7 | 6.6 | = | = | = | = | = | =/= | ||
| Parker [22] 2002 | Parallel | Isocaloric with ER | 3 months | 46 participants with T2D | 244 | −12 | 0.9 | 12 | = | ↓ −0.3 | ↓ −0.3 | = | = | = | = | =/= |
| Mehrabani [23] 2012 | Parallel | Isocaloric | 12 weeks | 49 overweight/ | −143 | −11 | −3.1 | 15 | = | = | = | = | = | ↓ −2.6 | ||
| obese women with PCOS | ||||||||||||||||
| Te Morenga [24] 2011 | Parallel | Isocaloric with ER | 2 months | 74 overweight/ | 214 | −9 | 4 | 6 | ↓ −1.3 | = | = | = | = | = | = | =/ |
| obese women | ↓ −3.7 | |||||||||||||||
| Frisch [25] 2009 | Parallel | Isocaloric with ER | 12 months | 200 overweight participants | −64 | −4.3 | 2.5 | 1.4 | = | = | = | = | = | = | ↓ −4.0/= | |
| Ebbeling [26] 2007 | Parallel | Isocaloric | 18 months | 73 obese participants | 154 | −13 | 12 | −0.3 | = | ↑ 0.3 | ↑ 0.3 | = | = | = | =/= | |
| De Natale [21] 2009 | Cross− | Isocaloric | 4 weeks | 18 participants with T2D | −12 | −7 | 7 | 0 | = | ↑ 0.2 | ↑ 0.2 | ↑ 0.1 | = | |||
| over | ||||||||||||||||
| Jacobs [27] 2004 | Cross−over | Isocaloric | 3 weeks | 14 non−obese men with elevated TAGs | 48 | −11 | 11 | −0.3 | = | = | = | = | = | |||
| Pieke [28] 2000 | Cross−over | Isocaloric | 3 weeks | 19 non−obese men with elevated TAGs | 81 | −14 | 12 | 1.6 | ↓ −0.2 | = | ↑ 0.1 | ↓ −0.9 | = | |||
| Vidon [29] 2001 | Cross−over | Isocaloric | 3 weeks | 7 healthy participants | −14 | 13 | 1.1 | ↑ 0.6 | ↑ 0.4 | ↑ 0.2 | = | ↑ 0.6 | ↑ 2.6 | |||
| Ashton [30] 2000 | Cross−over | Isocaloric | 3 weeks | 28 healthy participants | 300 | −14 | 16 | 0.8 | = | = | = | ↓ −0.1 | = | =/= | ||
| Wolfe [31] 1999 | Cross−over | Isocaloric | 4 weeks | 10 healthy participants | 23 | −10 | 0 | 10 | = | ↓ −0.3 | ↓ −0.2 | = | ↓ −0.3 | |||
| Study Characteristics | Diet Changes | Diet Effect | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author And Year | Study Design | LCD vs. MCD | Duration | Participants | kcal | CHO | Fat | Prot | Weight (kg) | TC (mmol/L) | LDL−C | HDL−C | TAG | Glucose (mmol/L) | Insulin (mU/mL) | Systolic/ |
| (mmol/L) | (mmol/L) | (mmol/L) | Diastolic BP (mmHg) | |||||||||||||
| Yamada [33] 2014 | Parallel | Ad libitum vs. ER | 6 months | 24 participants with T2D | 24 | −21 | 13 | 8.7 | = | = | = | = | = | =/= | ||
| Luger [34] | Parallel | Isocaloric | 12 weeks | 42 participants with T2D | 44 | −13 | 6.7 | 5.9 | = | = | = | = | = | =/= | ||
| 2013 | ||||||||||||||||
| Guldbrand [35] 2012 | Parallel | Isocaloric with ER | 24 months | 61 participants with T2D | −189 | −9 | 6 | 4 | = | = | = | = | = | =/= | ||
| Davis [36] | Parallel | Isocaloric | 12 months | 105 participants with T2D | −288 | −19 | 16 | 3.7 | = | = | = | ↑ 0.1 | = | =/= | ||
| 2009 | ||||||||||||||||
| Klemsdal [37] 2010 | Parallel | Isocaloric with ER | 12 months | 164 participants with at least one MetS symptom | −8.1 | 5 | 2.5 | = | = | = | = | = | = | = | =/ | |
| ↓ −2.9 | ||||||||||||||||
| Gardner [39] 2018 | Parallel | Isocaloric | 12 months | 609 overweight participants | −94 | −18 | 15 | 1.9 | = | ↑ 0.2 | ↑ 0.1 | ↓ −0.2 | = | = | =/= | |
| Bazzano [40] 2014 | Parallel | Isocaloric with ER | 12 months | 148 obese participants | −43 | −22 | 13 | 5.3 | ↓ −3.5 | = | = | ↑ 0.2 | ↓ −0.2 | = | = | =/= |
| Abete [41] 2009 | Parallel | Isocaloric with ER | 8 weeks | 19 obese men | −19 | 4.2 | 11 | ↓ −3.2 | = | = | = | = | = | = | =/= | |
| Gardner [42] 2007 (1) | Parallel | Ad libitum vs. ER | 12 months | 311 overwight/obse woman | 92 | −9.4 | 9.2 | −0.4 | ↓ −3.1 | = | = | ↓ −0.3 | = | = | ↓ −4.3/= | |
| Gardner [42] 2007 (2) | Parallel | Isocaloric | 12 months | 311 overwight/obse woman | 56 | −16 | 13 | 2.0 | = | = | ↑ 0.2 | = | = | = | ↓ −5.7/↓ −3.7 | |
| Brehm [43] 2003 | Parallel | Ad libitum vs. ER | 6 months | 42 obese men | 154 | −23 | 18 | 4.0 | ↓ −6.3 | = | = | = | ↓ −0.3 | = | = | =/= |
| Stern [44] 2004 | Parallel | Ad libitum vs. ER | 12 months | 87 obse participants +/− T2D | −413 | −16 | 25 | 0.7 | = | = | = | ↑ 0.1 | ↓ −0.6 | =/= | ||
| Samaha [45] 2003 | Parallel | Ad libitum vs. ER | 6 months | 132 obse participants +/− T2D and MetS | −188 | −12 | 8.0 | 5.0 | ↓ −3.9 | = | = | = | ↓ −0.4 | ↓ −0.5 | ↓ −7.0 | =/= |
| Hu [46] | Parallel | Isocaloric with ER | 12 months | 148 healthy participants | −43 | −22 | 13 | 5.3 | ↓ −3.5 | |||||||
| 2015 | ||||||||||||||||
| Brynes [38] 2003 (1) | Cross−over | Isocaloric | 24 weeks | 17 men with at least one cardiac risk factor | 449 | −11 | 11 | −2.0 | = | = | = | = | = | = | = | |
| Brynes [38] 2003 (2) | Cross−over | Isocaloric | 24 weeks | 17 men with at least one cardiac risk factor | 736 | −11 | 14 | −3.0 | = | = | = | = | = | = | = | |
| Brynes [38] 2003 (3) | Cross−over | Isocaloric | 24 weeks | 17 men with at least one cardiac risk factor | 239 | −15 | 14 | −1.0 | = | = | = | = | = | = | = | |
| Straznicky [47] 1999 | Cross−over | Isocaloric | 2 weeks | 148 healthy men | 449 | −18 | 22 | −2.9 | = | ↑ 1.1 | ↑ 0.9 | ↑ 0.2 | = | ↑ 0.3 | = | ↑ 7.0/ ↑ 3.0 |
| Borkman [48] 1991 | Cross−over | Isocaloric | 3 weeks | 8 healthy participants | 287 | −24 | 30 | −6.1 | = | = | = | ↑ 0.3 | = | |||
| Study Characteristics | Diet Changes | Diet Effect | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author And Year | Study Design | LCD vs. MCD | Duration | Participants | kcal | CHO | Fat | Prot | Weight (kg) | TC (mmol/L) | LDL−C (mmol/L) | HDL−C (mmol/L) | TAG (mmol/L) | Glucose (mmol/L) | Insulin (μU/mL) | Systolic/ Diastolic BP (mmHg) |
| Tay [50] 2015 | Parallel | Isocaloric with ER | 12 months | 77 participants with T2D | −37 | −32 | 26 | 7.2 | = | = | ↑ 0.1 | ↓ −0.4 | = | = | =/= | |
| Brehm [51] 2005 | Parallel | Ad libitum vs. ER | 4 months | 40 obese women | 119 | −21 | 19 | 2.0 | ↓ −3.7 | = | = | ↑ 0.1 | = | =/= | ||
| Veum [52] 2017 | Parallel | Isocaloric | 12 weeks | 38 men with abdominal obesity | 245 | −39 | 40 | −0.6 | = | ↑ 1.1 | ↑ 1.0 | ↑ 0.2 | = | ↑ 0.3 | = | =/= |
| Brinkworth [53] 2009 | Parallel | Isocaloric with ER | 12 months | 107 participants with abdominal obesity and at least one MetS symptom | 20 | −38 | 29 | 11 | = | ↑ 0.6 | ↑ 0.6 | ↑ 0.2 | ↓ −0.4 | = | = | =/= |
| Stoernell [54] 2008 | Parallel | Isocaloric | 8 weeks | 23 participants with elevated TAGs | −145 | −27 | 21 | 2.0 | = | = | = | = | = | |||
| Ranjan [49] 2017 | Cross− over | Isocaloric | 1 week | 10 participants with T2D | −160 | −40 | 31 | 9.2 | = | = | = | = | = | = | =/= | |
| Holloway [55] 2011 | Cross− over | Isocaloric | 5 days | 16 healthy men | −31 | −45 | 47 | −2.0 | ↓ −3.1 | = | = | |||||
| Chokkalingam [56] 2007 | Cross− over | Isocaloric | 6 days | 10 healthy men | 215 | −42 | 44 | 0 | = | = | ||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fechner, E.; Smeets, E.T.H.C.; Schrauwen, P.; Mensink, R.P. The Effects of Different Degrees of Carbohydrate Restriction and Carbohydrate Replacement on Cardiometabolic Risk Markers in Humans—A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 991. https://doi.org/10.3390/nu12040991
Fechner E, Smeets ETHC, Schrauwen P, Mensink RP. The Effects of Different Degrees of Carbohydrate Restriction and Carbohydrate Replacement on Cardiometabolic Risk Markers in Humans—A Systematic Review and Meta-Analysis. Nutrients. 2020; 12(4):991. https://doi.org/10.3390/nu12040991
Chicago/Turabian StyleFechner, Eva, Ellen T.H.C. Smeets, Patrick Schrauwen, and Ronald P. Mensink. 2020. "The Effects of Different Degrees of Carbohydrate Restriction and Carbohydrate Replacement on Cardiometabolic Risk Markers in Humans—A Systematic Review and Meta-Analysis" Nutrients 12, no. 4: 991. https://doi.org/10.3390/nu12040991
APA StyleFechner, E., Smeets, E. T. H. C., Schrauwen, P., & Mensink, R. P. (2020). The Effects of Different Degrees of Carbohydrate Restriction and Carbohydrate Replacement on Cardiometabolic Risk Markers in Humans—A Systematic Review and Meta-Analysis. Nutrients, 12(4), 991. https://doi.org/10.3390/nu12040991