Dietary Patterns of Nurses on Rotational Shifts Are Marked by Redistribution of Energy into the Nightshift



Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Study Design
2.3. Data Analysis
3. Results
Energy Intake
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Potter, G.; Skene, D.J.; Arendt, J.; Cade, J.; Grant, P.; Hardie, L. Circadian rhythm and sleep disruption: Causes, metabolic consequences, and countermeasures. Endocr. Rev. 2016, 37, 584–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garaulet, M.; Ordovás, J.; Madrid, J. The chronobiology, etiology and pathophysiology of obesity. Int. J. Obes. 2010, 34, 1667–1683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Depner, C.; Stothard, E.; Wright, K. Metabolic consequences of sleep and circadian disorders. Curr. Diab. Rep. 2014, 14, 507. [Google Scholar] [CrossRef] [PubMed]
- Molzof, H.; Wirth, M.; Burch, J.; Shivappa, N.; Hebert, J.; Johnson, R.; Gamble, K. The impact of meal timing on cardiometabolic syndrome indicators in shift workers. Chronobiol. Int. 2017, 34, 337–348. [Google Scholar] [CrossRef] [Green Version]
- Bonham, M.P.; Bonnell, E.K.; Huggins, C.E. Energy intake of shift workers compared to fixed day workers: A systematic review and meta-analysis. Chronobiol. Int. 2017, 33, 1086–1100. [Google Scholar] [CrossRef]
- Shaw, E.; Dorrian, J.; Coates, A.M.; Leung, G.K.W.; Davis, R.; Rosbotham, E.; Warnock, R.; Huggins, C.E.; Bonham, M.P. Temporal pattern of eating in night shift workers. Chronobiol. Int. 2019, 36, 1613–1625. [Google Scholar] [CrossRef]
- Esquirol, Y.; Bongard, V.; Mabile, L.; Jonnier, B.; Soulat, J.; Perret, B. Shift work and metabolic syndrome: Respective impacts of job strain, physical activity, and dietary rhythms. Chronobiol. Int. 2009, 26, 544–559. [Google Scholar] [CrossRef]
- Buysse, D.J. Sleep health: Can we define it? Does it matter? SLEEP 2014, 37, 9–17. [Google Scholar] [CrossRef] [Green Version]
- Johnston, J.D. Physiological responses to food intake throughout the day. Nutr. Res. Rev. 2014, 27, 107–118. [Google Scholar] [CrossRef] [Green Version]
- Bass, J. Circadian topology of metabolism. Nature 2012, 491, 348–356. [Google Scholar] [CrossRef]
- Oike, H.; Oishi, K.; Kobori, M. Nutrients, clock genes, and chrononutrition. Curr. Nutr. Rep. 2014, 3, 204–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, M.; McGinnis, G. Circadian regulation of metabolic homeostasis: Causes and consequences. Nat. Sci. Sleep 2016, 8, 163–180. [Google Scholar] [CrossRef] [Green Version]
- Westerterp-Plantenga, M. Sleep, circadian rhythm and body weight: Parallel developments. Proc. Nutr. Soc. 2016, 75, 431–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lowson, E.; Middleton, B.; Arber, S.; Skene, D.J. Effects of night work on sleep, cortisol and mood of female nurses, their husbands and children. Sleep Biol. Rhythm. 2013, 11, 7–13. [Google Scholar] [CrossRef] [Green Version]
- Thompson, E. Understanding How Night Work Influences the Everyday Family Lives of Nurses, Their Husbands and Children. Ph.D. Thesis, University of Surrey, Guildford, Surrey, UK, 2009; pp. 1–407. [Google Scholar]
- Nutritics, Research Edition (v5.09); Nutritics LTD: Dublin, Ireland, 2018.
- Wrieden, W.; Barton, K. Calculation and Collation of Typical Food Portion Sizes for Adults Aged 19-64 and Older People Aged 65 and Over. Final Technical Report to Food Standards Agency. Available online: http://www.foodbase.org.uk/results.php?f_category_id=&f_report_id=82 (accessed on 10 April 2020).
- Leech, R.M.; Timperio, A.; Livingstone, K.M.; Worsley, A.; McNaughton, S.A. Temporal eating patterns: Associations with nutrient intakes, diet quality, and measures of adiposity. Am. J. Clin. Nutr. 2017, 106, 1121–1130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Naimi, S.; Hampton, S.; Richard, P.; Tzung, C.; Morgan, L. Postprandial metabolic profiles following meals and snacks eaten during simulated night and day shift work. Chronobiol. Int. 2004, 21, 937–947. [Google Scholar] [CrossRef]
- Hibi, M.; Masumoto, A.; Naito, Y.; Kiuchi, K.; Yoshimoto, Y.; Matsumoto, M.; Katashima, M.; Oka, J.; Ikemoto, S. Nighttime snacking reduces whole body fat oxidation and increases LDL cholesterol in healthy young women. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2013, 304, R94–R101. [Google Scholar] [CrossRef] [Green Version]
- Costa, G.; Ghirlanda, G.; Tarondi, G.; Minors, D.; Waterhouse, J. Evaluation of a rapidly rotating shift system for tolerance of nurses to nightwork. Int. Arch. Occup. Environ. Health 1994, 65, 305–311. [Google Scholar] [CrossRef]
- Wehrens, S.; Christou, S.; Isherwood, C.; Middleton, B.; Gibbs, M.; Archer, S.; Skene, D.J.; Johnston, J.D. Meal timing regulates the human circadian system. Curr. Biol. 2017, 27, 1768–1775.e3. [Google Scholar] [CrossRef] [Green Version]
- Almoosawi, S.; Vingeliene, S.; Karagounis, L.; Pot, G. Chrono-nutrition: A review of current evidence from observational studies on global trends in time-of-day of energy intake and its association with obesity. Proc. Nutr. Soc. 2016, 75, 487–500. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Lauren, S.; Chang, B.P.; Shechter, A. Objective food intake in night and day shift workers: A laboratory study. Clocks Sleep 2019, 1, 43–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonnell, E.K.; Huggins, C.E.; Huggins, C.T.; McCaffrey, T.A.; Palermo, C.; Bonham, M.P. Influences on dietary choices during day versus night shift in shift workers: A mixed methods study. Nutrients 2017, 9, 193. [Google Scholar] [CrossRef] [PubMed]
- Morris, C.; Purvis, T.; Mistretta, J.; Scheer, F. Effects of the internal circadian system and circadian misalignment on glucose tolerance in chronic shift workers. J. Clin. Endocrinol. Metab. 2015, 101, 1066–1074. [Google Scholar] [CrossRef]
- Scheer, F.; Hilton, M.; Mantzoros, C.; Shea, S. Adverse metabolic and cardiovascular consequences of circadian misalignment. Proc. Natl. Acad. Sci. USA 2009, 106, 4453–4458. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
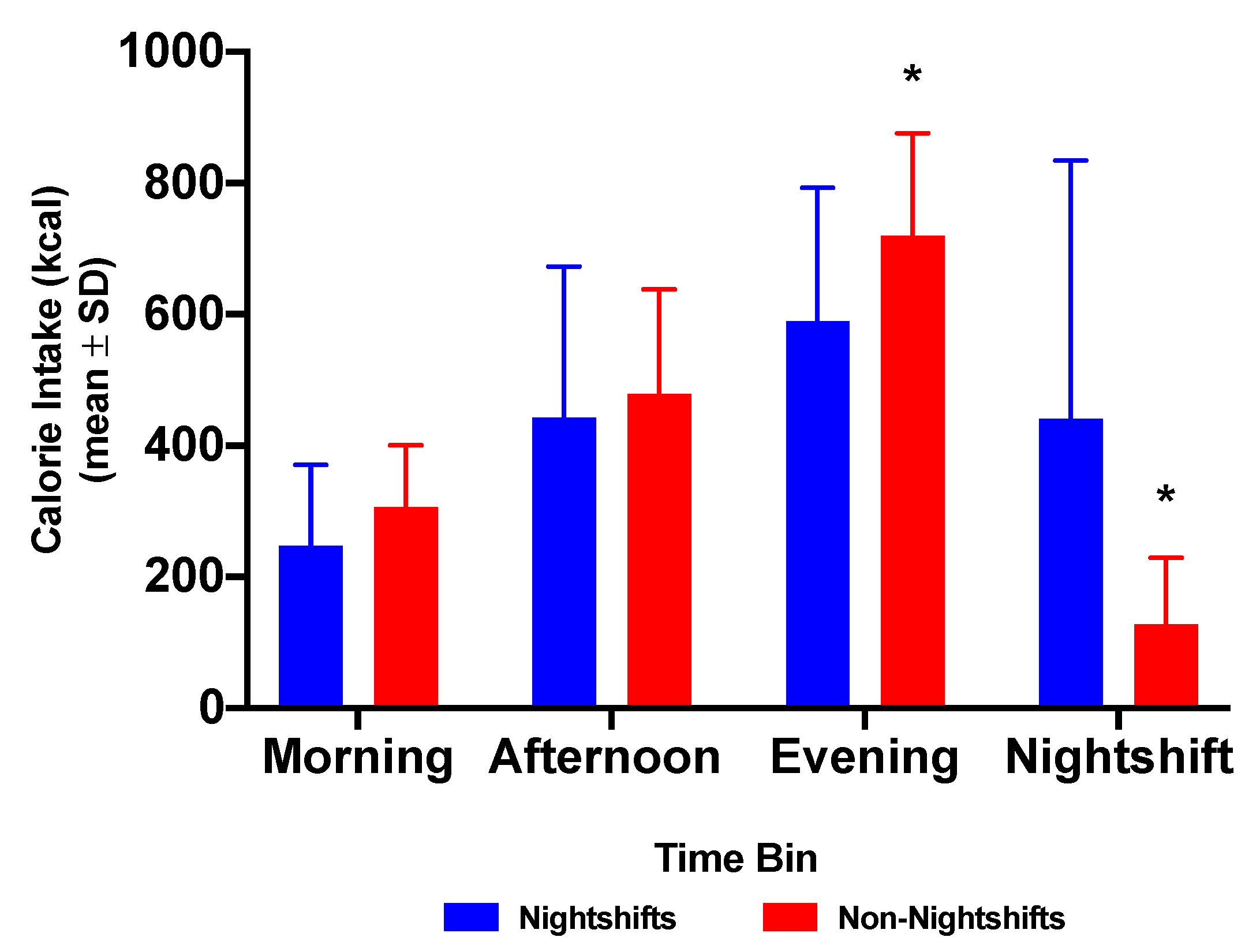
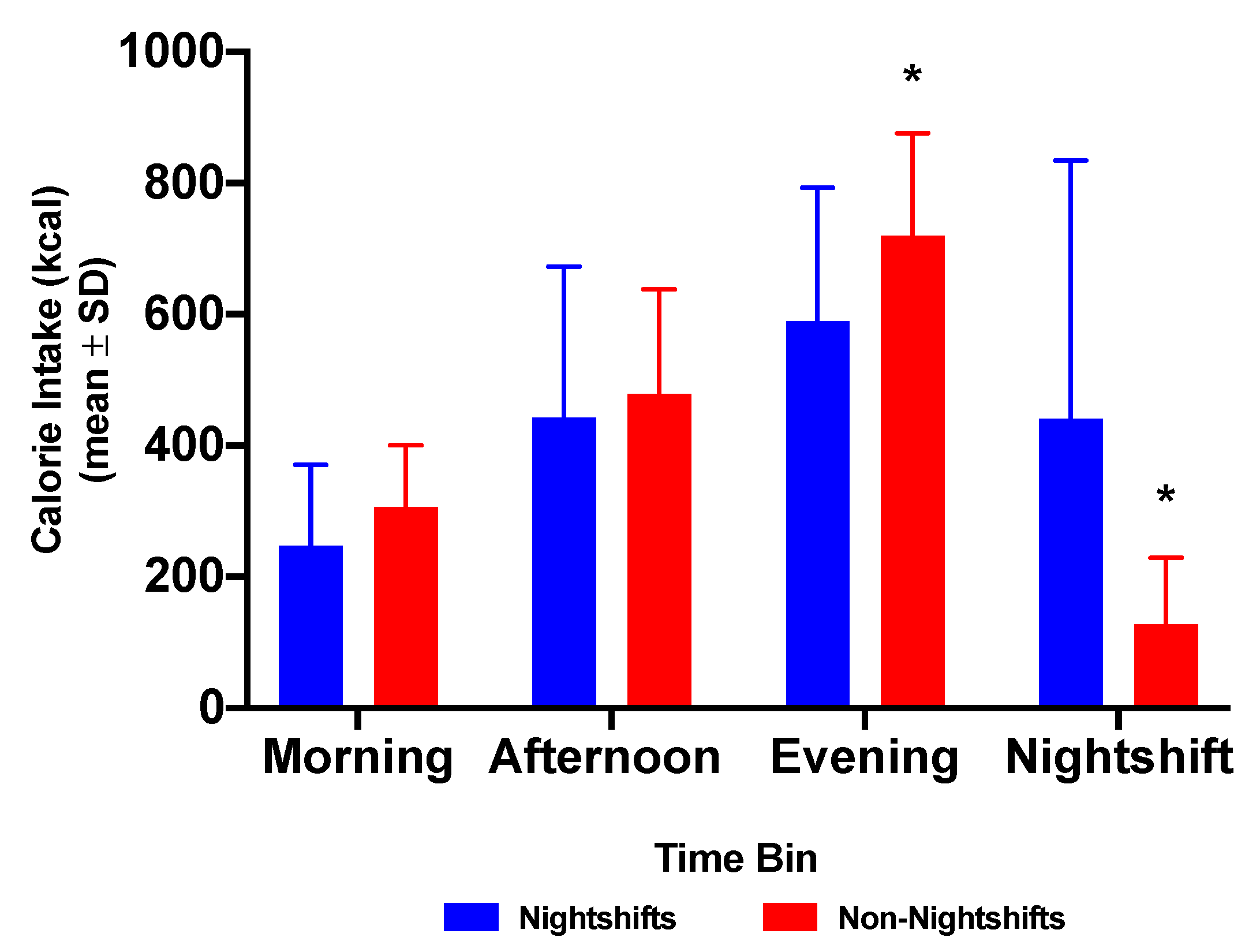
| Dietary Intake Nights vs. Non-Nights | Nightshifts | Non-Nightshifts | p Value | |
| Total daily energy, kcal | 1566.5 ± 557.2 | 1551.1 ± 327.4 | 0.919 | |
| Morning energy 07:00–12:00 h, kcal | 246.8 ± 123.7 | 305.9 ± 94.7 | 0.053 | |
| Morning energy, % TDEI | 15.8 ± 9.0 | 19.7 ± 4.6 | 0.034 | |
| Afternoon energy 12:00–17:00 h, kcal | 443.4 ± 230.4 | 478.6 ± 159.4 | 0.538 | |
| Afternoon energy, % TDEI | 28.3 ± 13.5 | 30.5 ± 6.9 | 0.844 | |
| Evening energy 17:00–21:00 h, kcal | 588.7 ± 203.7 | 719.3 ± 156.9 | 0.055 | |
| Evening energy, % TDEI | 38.8% ± 11.9% | 46.4% ± 7.5% | 0.044 * | |
| Nightshift energy 21:00–07:00 h, kcal | 466.5 ± 419.1 | 126.8 ± 102.0 | 0.001 * | |
| Nightshift energy 21:00–07:00 h, % TDEI | 29.8% ± 5.1% | 8.2% ± 5.2% | 0.0001 * | |
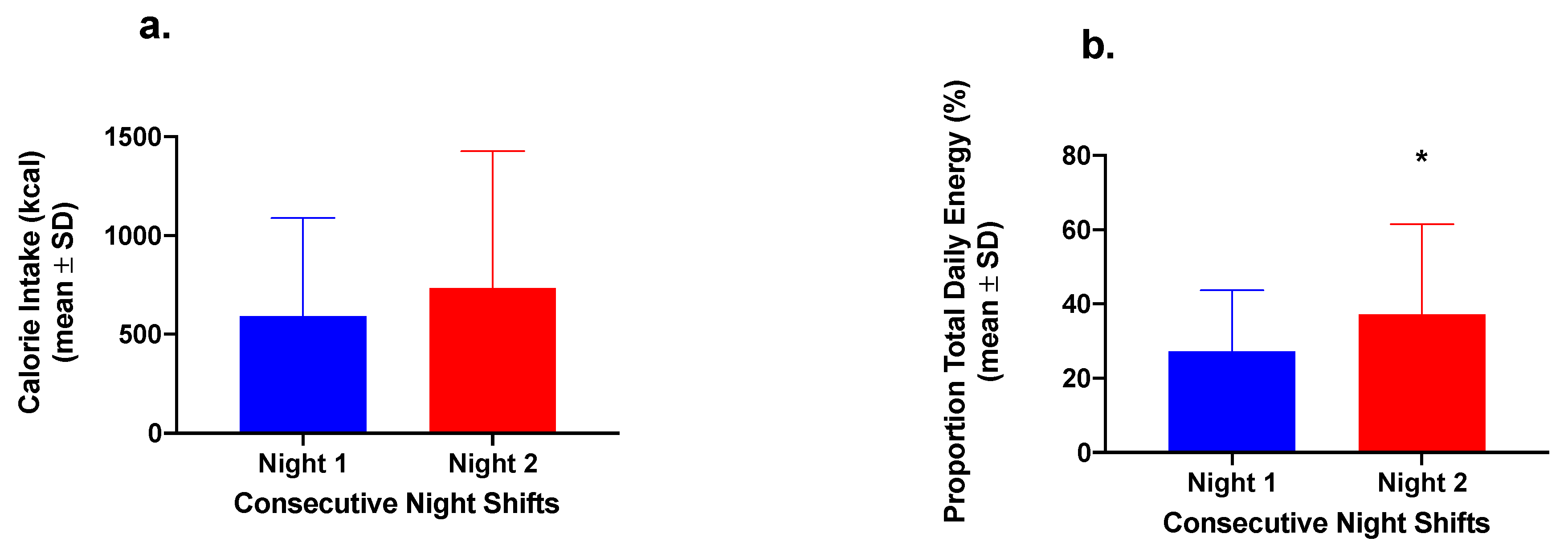
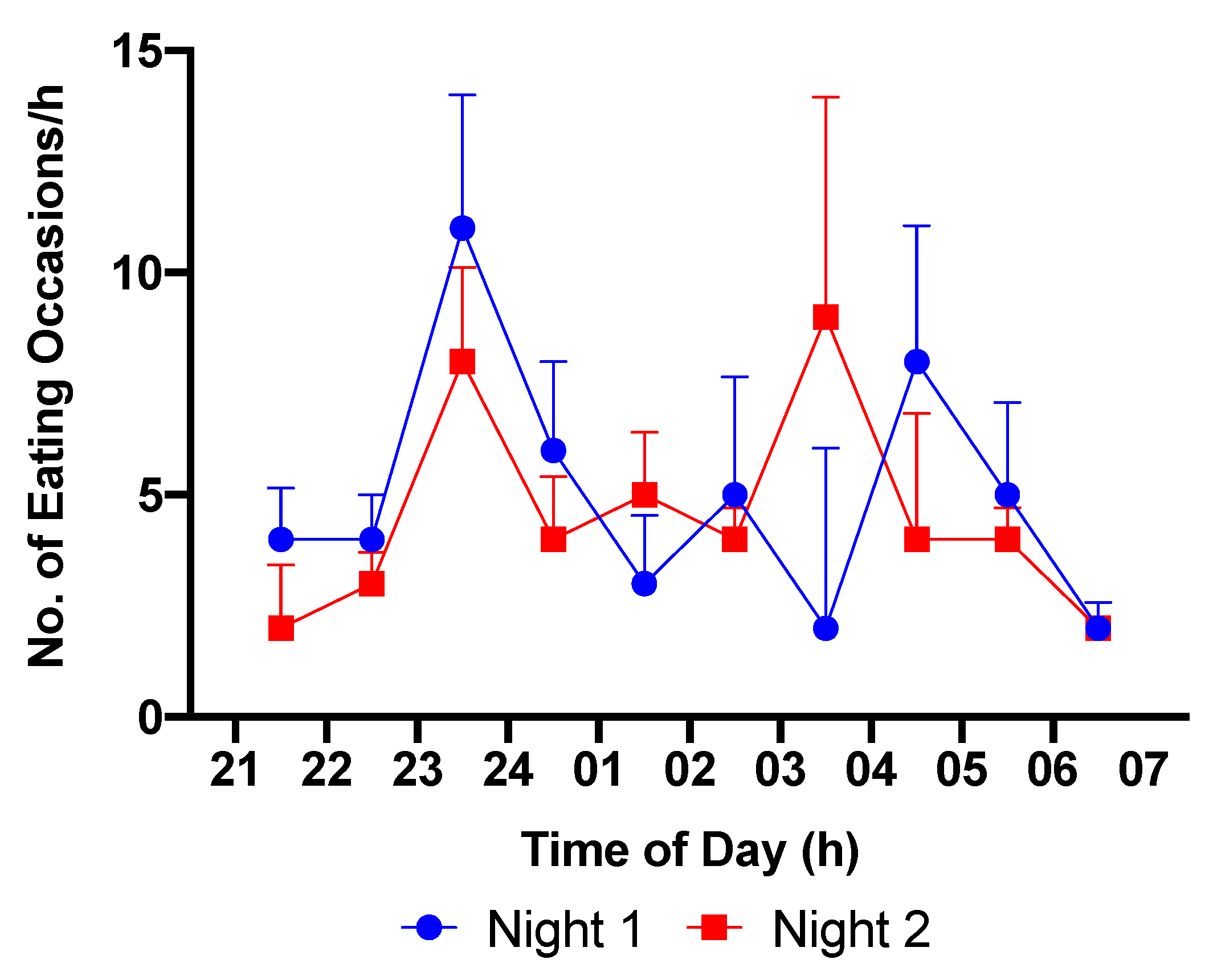
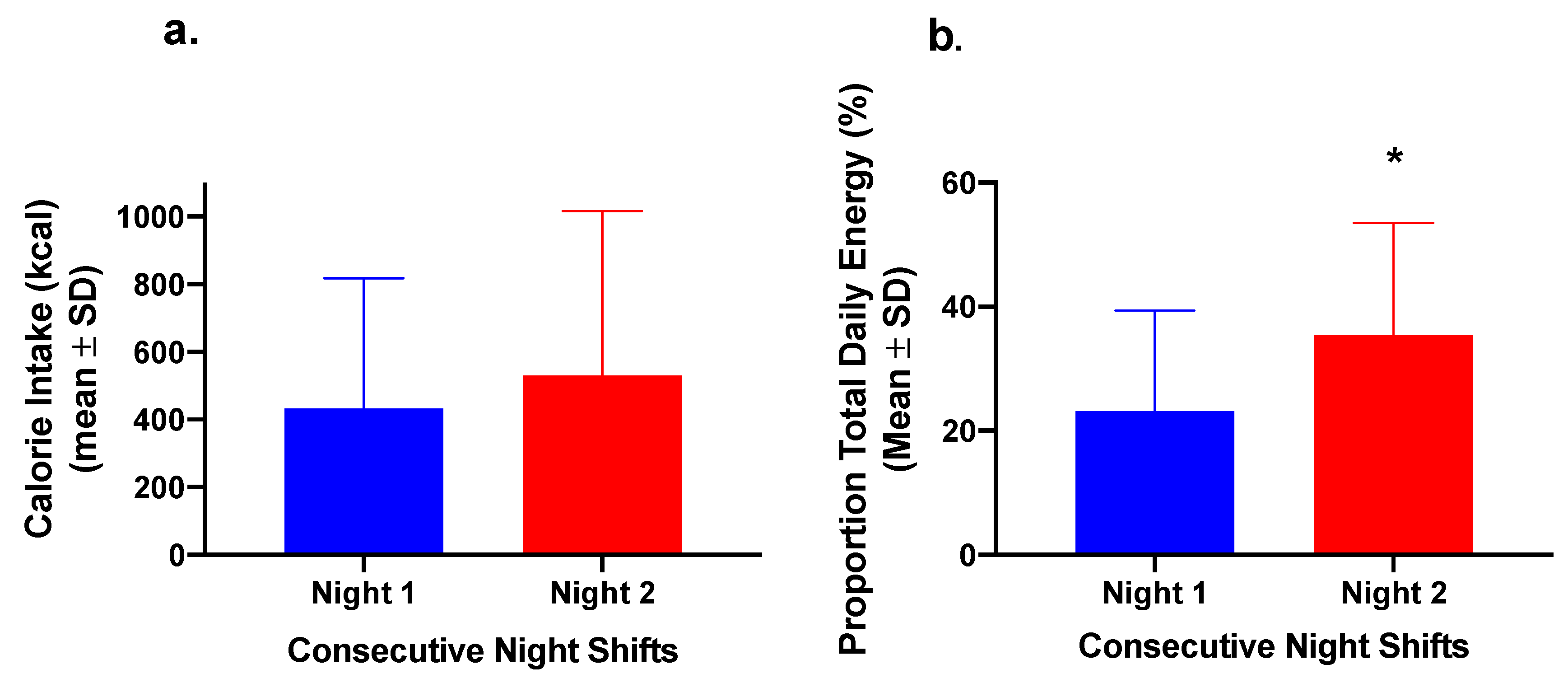
| 2-Night Group Dietary Intake Over Nightshifts | Night 1 | Night 2 | p value | |
| 2-Night Group (n = 8) energy, kcal | 591.5 ± 497.4 | 734.8 ± 692.0 | 0.276 | |
| 2-Night Group (n = 8) energy, %TDEI | 27.3% ± 16.5% | 42.3% ± 18.2% | 0.037 * | |
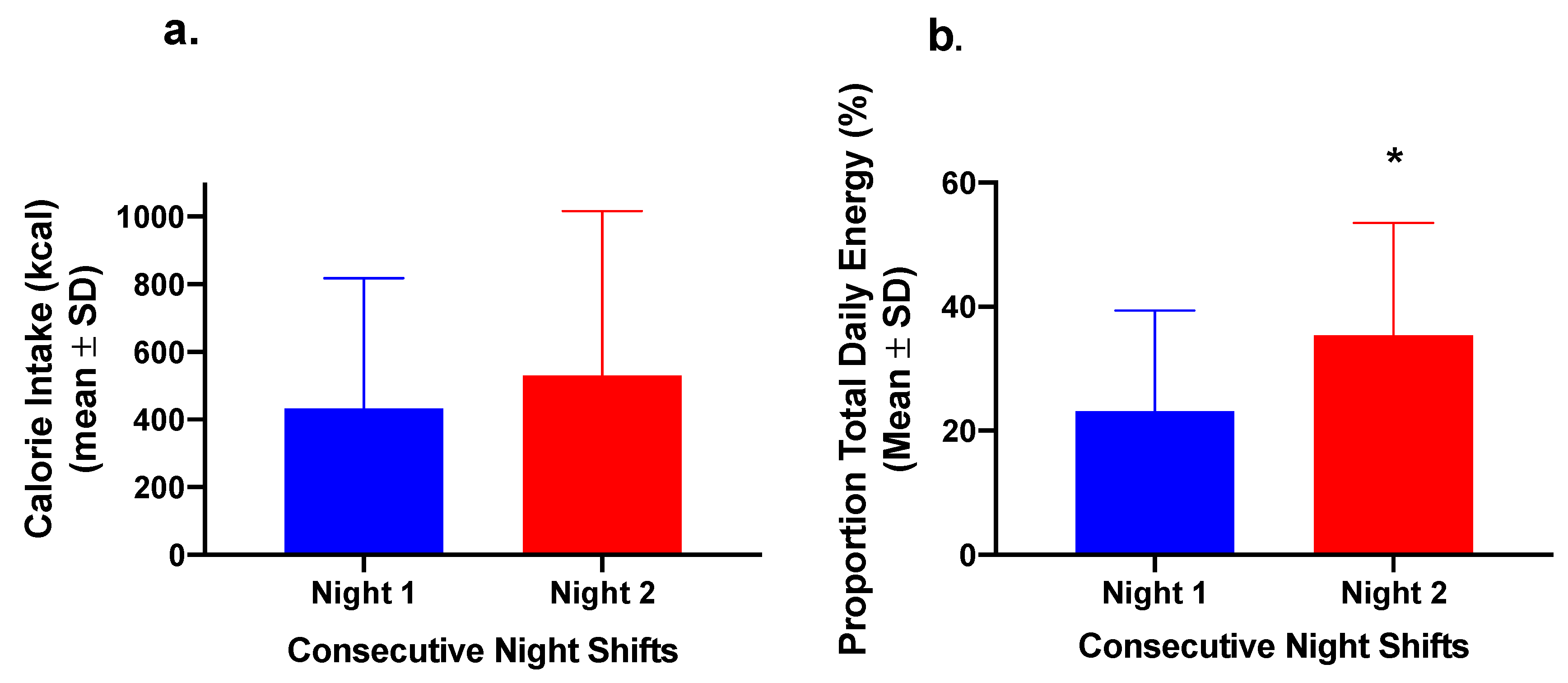
| All Group (n = 20) 2-Night energy, kcals | 440.5 ± 373.3 | 483.4 ± 487.0 | 0.138 | |
| All Group (n = 20) 2-Night energy, %TDEI | 26.0% ± 15.7% | 33.5% ± 20.2% | 0.008 * | |
| All Group (n = 20) 2-Night CHO, kcal | 212.8 ± 177.6 | 264.1 ± 228.6 | 0.188 | |
| All Group (n = 20) 2-Night CHO, %CHO energy | 25.4% ± 16.6% | 38.1% ± 30.2% | 0.070 | |
| All Group (n = 20) 2-Night FAT, kcal | 169.2 ± 160.0 | 157.6 ± 200.1 | 0.686 | |
| All Group (n = 20) 2-Night FAT, %FAT energy | 23.7% ± 17.2% | 31.7% ± 29.3% | 0.149 | |
| All Group (n = 20) 2-Night PRO, kcal | 57.6 ± 51.1 | 65.4 ± 69.5 | 0.455 | |
| All Group (n = 20) 2-Night PRO, %PRO energy | 20.5% ± 17.2% | 28.9% ± 23.8% | 0.126 | |
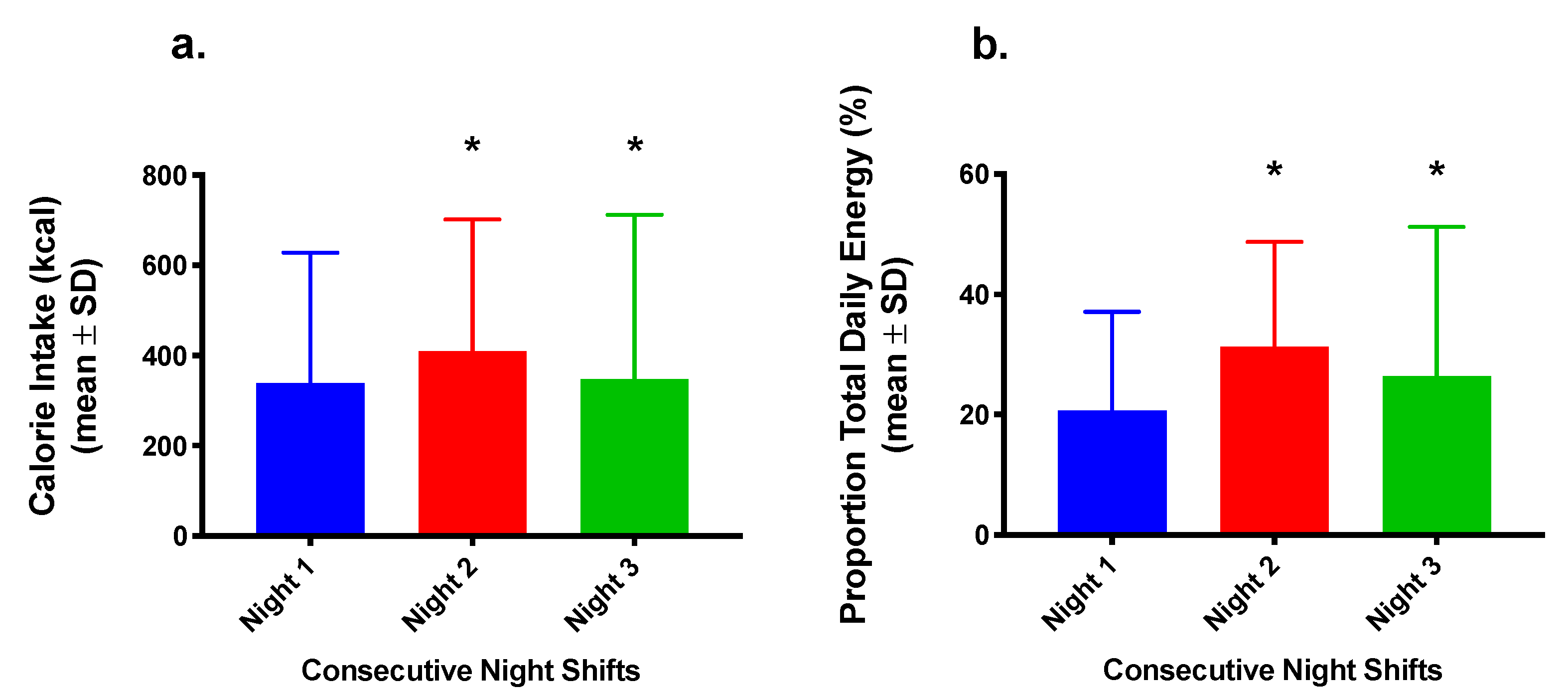
| 3-Night Group Dietary Intake Over Nightshifts | Night 1 | Night 2 | Night 3 | p value |
| 3-Night Group (n = 12) energy, kcal | 326.0 ± 280.9 | 383.7 ± 294.6 | 338.7 ± 350.4 | 0.0001 **/0.549 |
| 3-Night Group (n = 12) energy, %TDEI | 21.0% ± 16.1% | 28.2% ± 18.3% | 25.7% ± 23.8% | 0.004 **/0.224 |
| 3-Night Group (n = 12) CHO, kcal | 175.5 ± 148.2 | 226.2 ± 147.5 | 161.4 ± 127.6 | 0.001 **/0.236 |
| 3-Night Group (n = 12) CHO, %CHO energy | 22.5% ± 16.4% | 36.8% ± 34.6% | 28.1% ± 28.0% | 0.002 **/0.204 |
| 3-Night Group (n = 12) FAT, kcal | 118.8 ± 119.4 | 113.3 ± 112.9 | 74.5 ± 68.9 | 0.014 **/0.380 |
| 3-Night Group (n = 12) FAT, %FAT energy | 20.0% ± 17.4% | 27.5% ± 31.0% | 15.8% ± 15.0% | 0.008 **/0.246 |
| 3-Night Group (n = 12) PRO, kcal | 44.5 ± 39.3 | 50.3 ± 33.6 | 34.6 ± 30.3 | 0.024 **/0.390 |
| 3-Night Group (n = 12) PRO, %PRO energy | 19.5% ± 19.2% | 24.4% ± 14.3% | 18.2% ± 19.6% | 0.040 **/0.557 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flanagan, A.; Lowson, E.; Arber, S.; Griffin, B.A.; Skene, D.J. Dietary Patterns of Nurses on Rotational Shifts Are Marked by Redistribution of Energy into the Nightshift. Nutrients 2020, 12, 1053. https://doi.org/10.3390/nu12041053
Flanagan A, Lowson E, Arber S, Griffin BA, Skene DJ. Dietary Patterns of Nurses on Rotational Shifts Are Marked by Redistribution of Energy into the Nightshift. Nutrients. 2020; 12(4):1053. https://doi.org/10.3390/nu12041053
Chicago/Turabian StyleFlanagan, Alan, Elizabeth Lowson, Sara Arber, Bruce A. Griffin, and Debra J. Skene. 2020. "Dietary Patterns of Nurses on Rotational Shifts Are Marked by Redistribution of Energy into the Nightshift" Nutrients 12, no. 4: 1053. https://doi.org/10.3390/nu12041053
APA StyleFlanagan, A., Lowson, E., Arber, S., Griffin, B. A., & Skene, D. J. (2020). Dietary Patterns of Nurses on Rotational Shifts Are Marked by Redistribution of Energy into the Nightshift. Nutrients, 12(4), 1053. https://doi.org/10.3390/nu12041053