Vitamin D Status in Japanese Adults: Relationship of Serum 25-Hydroxyvitamin D with Simultaneously Measured Dietary Vitamin D Intake and Ultraviolet Ray Exposure

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
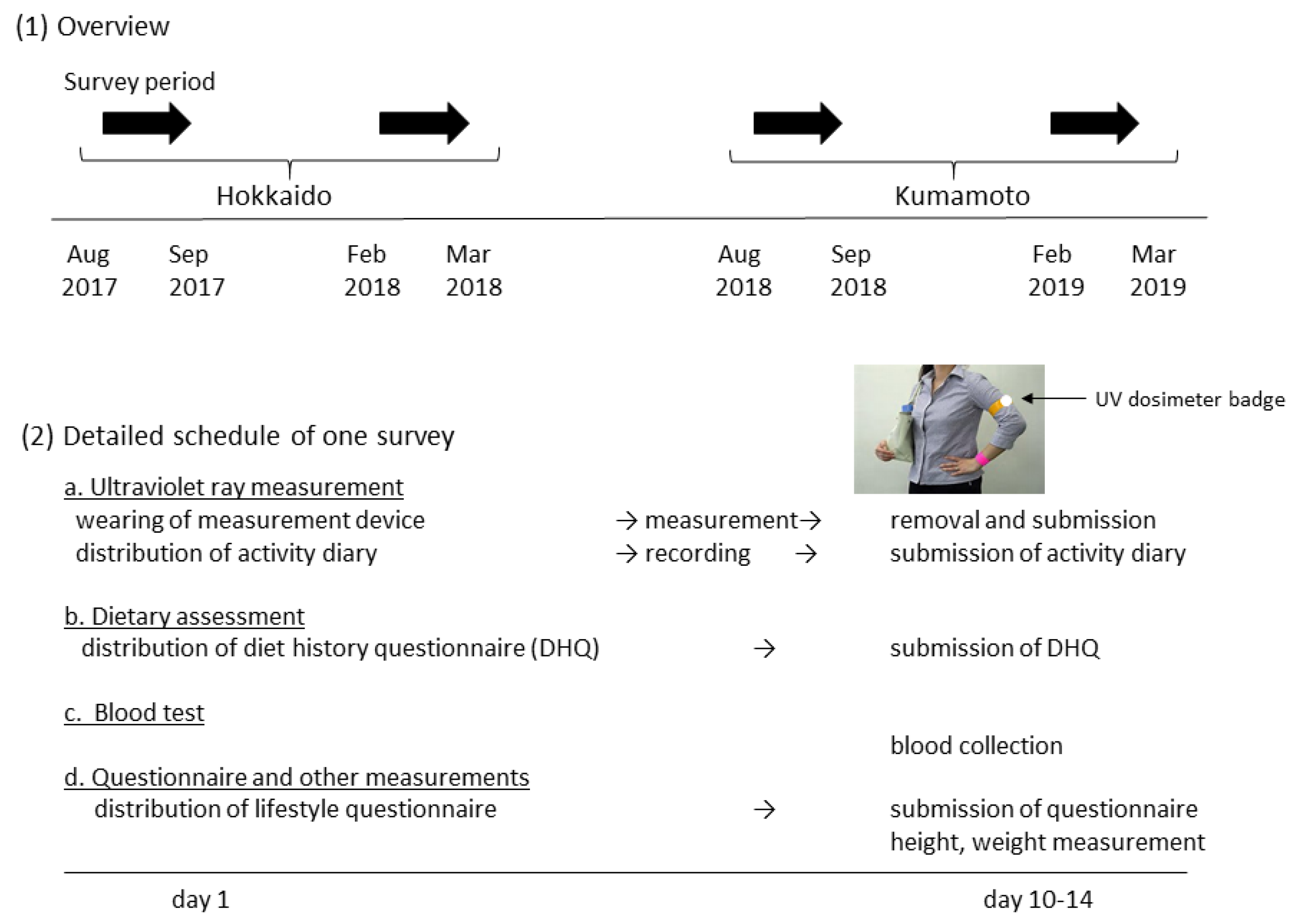
2.2. Measurement Schedule
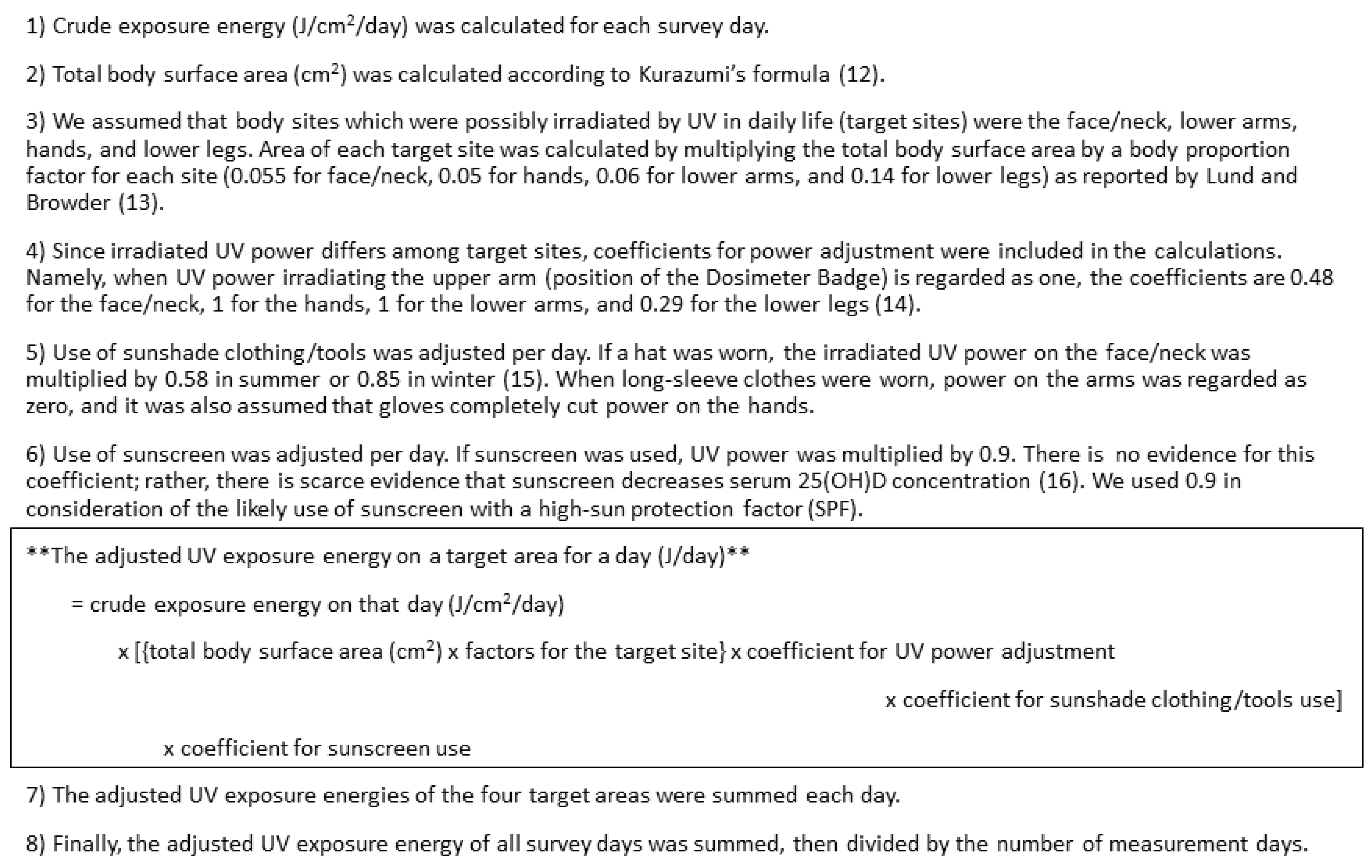
2.3. Ultraviolet Ray Exposure Measurement
2.4. Dietary Assessment
2.5. Blood Tests
2.6. Questionnaire and Other Measurements
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Institute of Medicine (US). Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. In Dietary Reference Intakes for Calcium and Vitamin D; Ross, A.C., Taylor, C.L., Yaktine, A.L., Del Valle, H.B., Eds.; The National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Zhang, Y.; Fang, F.; Tang, J.; Jia, L.; Feng, Y.; Xu, P.; Faramand, A. Association between vitamin D supplementation and mortality: Systematic review and meta-analysis. BMJ 2019, 366, l4673. [Google Scholar] [CrossRef]
- Orkaby, A.R.; Djousse, L.; Manson, J.E. Vitamin D supplements and prevention of cardiovascular disease. Curr. Opin. Cardiol. 2019, 34, 700–705. [Google Scholar] [CrossRef]
- Holick, M.F. The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev. Endocr. Metab. Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef] [PubMed]
- van Schoor, N.M.; Lips, P. Worldwide vitamin D status. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 671–680. [Google Scholar] [CrossRef] [PubMed]
- Kanatani, K.T.; Nakayama, T.; Adachi, Y.; Hamazaki, K.; Onishi, K.; Konishi, Y.; Kawanishi, Y.; Go, T.; Sato, K.; Kurozawa, Y.; et al. High frequency of vitamin D deficiency in current pregnant Japanese women associated with UV avoidance and hypo-vitamin D diet. PLoS ONE 2019, 14, e0213264. [Google Scholar] [CrossRef] [PubMed]
- Mizoue, T.; Kochi, T.; Akter, S.; Eguchi, M.; Kurotani, K.; Tsuruoka, H.; Kuwahara, K.; Ito, R.; Kabe, I.; Nanri, A. Low serum 25-hydroxyvitamin D concentrations are associated with increased likelihood of having depressive symptoms among Japanese workers. J. Nutr. 2015, 145, 541–546. [Google Scholar] [CrossRef] [PubMed]
- Cashman, K.D.; Kiely, M. Recommended dietary intakes for vitamin D: Where do they come from, what do they achieve and how can we meet them? J. Hum. Nutr. Diet. 2014, 27, 434–442. [Google Scholar] [CrossRef]
- Nordic Council of Ministers. Nordic Nutrition Recommendations 2012 5th Edition. Available online: http://norden.diva-portal.org/smash/get/diva2:704251/FULLTEXT01.pdf (accessed on 1 November 2019).
- Ministry of Health, Labour and Welfare. Dietary Reference Intakes for Japanese, 2015; Daiichi Shuppan Publishing Co., Ltd.: Tokyo, Japan, 2014. [Google Scholar]
- Grandahl, K.; Mortensen, O.S.; Sherman, D.Z.; Køster, B.; Lund, P.A.; Ibler, K.S.; Eriksen, P. Solar UV exposure among outdoor workers in Denmark measured with personal UV-B dosimeters: Technical and practical feasibility. Biomed. Eng. Online 2017, 16, 119. [Google Scholar] [CrossRef]
- Kurazumi, Y.; Horikoshi, T.; Tsuchikawa, T.; Matsubara, N. The body surface area for Japanese. Jpn. J. Biometeor. 1994, 31, 5–29. [Google Scholar]
- Lund, C.C.; Browder, N.C. The estimation of areas of burns. Surg. Gynecol. Obste. 1944, 79, 352–358. [Google Scholar]
- Eto, N.; Asakura, K.; Nishiwaki, Y. Relationships between solar ultraviolet exposure levels at different sites around the body. Toho J. Med. 2019, in press. [Google Scholar]
- Backes, C.; Religi, A.; Moccozet, L.; Vuilleumier, L.; Vernez, D.; Bulliard, J.L. Facial exposure to ultraviolet radiation: Predicted sun protection effectiveness of various hat styles. Photodermatol. Photoimmunol. Photomed. 2018, 34, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Neale, R.E.; Khan, S.R.; Lucas, R.M.; Waterhouse, M.; Whiteman, D.C.; Olsen, C.M. The effect of sunscreen on vitamin D: A review. Br. J. Dermatol. 2019, 18, 907–915. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S.; Murakami, K.; Sasaki, S.; Okubo, H.; Hirota, N.; Notsu, A.; Fukui, M.; Date, C. Comparison of relative validity of food group intakes estimated by comprehensive and brief-type self-administered diet history questionnaires against 16 d dietary records in Japanese adults. Public Health Nutr. 2011, 14, 1200–1211. [Google Scholar] [CrossRef]
- Kobayashi, S.; Honda, S.; Murakami, K.; Sasaki, S.; Okubo, H.; Hirota, N.; Notsu, A.; Fukui, M.; Date, C. Both comprehensive and brief self-administered diet history questionnaires satisfactorily rank nutrient intakes in Japanese adults. J. Epidemiol. 2012, 22, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Shiraishi, M.; Haruna, M.; Matsuzaki, M.; Murayama, R.; Kitanaka, S.; Sasaki, S. Validity of a self-administered diet history questionnaire for estimating vitamin D intakes of Japanese pregnant women. Matern. Child Nutr. 2015, 11, 525–536. [Google Scholar] [CrossRef] [PubMed]
- The Council for Science and Technology. Standard Tables of Food Composition in Japan, Fifth Revised and Enlarged edition-2010; Official Gazette Cooperation: Tokyo, Japan, 2010. [Google Scholar]
- Willett, W.C.; Howe, G.R.; Kushi, L.H. Adjustment for total energy intake in epidemiologic studies. Am. J. Clin. Nutr. 1997, 65 (Suppl. 4), 1220S–1228S. [Google Scholar] [CrossRef]
- Kobayashi, E.; Sato, Y.; Umegaki, K.; Chiba, T. The Prevalence of Dietary Supplement Use among College Students: A Nationwide Survey in Japan. Nutrients 2017, 9, 1250. [Google Scholar] [CrossRef]
- Kobayashi, E.; Nishijima, C.; Sato, Y.; Umegaki, K.; Chiba, T. The Prevalence of Dietary Supplement Use Among Elementary, Junior High, and High School Students: A Nationwide Survey in Japan. Nutrients 2018, 10, 1176. [Google Scholar] [CrossRef]
- Masumoto, S.; Sato, M.; Maeno, T.; Ichinohe, Y. Factors associated with the use of dietary supplements and over-the-counter medications in Japanese elderly patients. BMC Fam. Pract. 2018, 19, 20. [Google Scholar] [CrossRef]
- Fitzpatrick, T.B. The validity and practicality of sun-reactive skin types I through VI. Arch. Dermatol. 1988, 124, 869–871. [Google Scholar] [CrossRef] [PubMed]
- Murase, N.; Katsumura, T.; Ueda, C.; Inoue, S.; Shimomitsu, T. Validity and reliability of Japanese version of International Physical Activity Questionnaire. J. Health Welf. Stat. 2002, 49, 1–9. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Jiang, C.Q.; Chan, Y.H.; Xu, L.; Jin, Y.L.; Zhu, T.; Zhang, W.S.; Cheng, K.K.; Lam, T.H. Smoking and serum vitamin D in older Chinese people: Cross-sectional analysis based on the Guangzhou Biobank Cohort Study. BMJ Open 2016, 6, e010946. [Google Scholar] [CrossRef]
- Statistics Bureau, Ministry of Internal Affairs and Communications, Japan. Statistical Handbook of Japan, 2019. Available online: https://www.stat.go.jp/english/data/handbook/index.html (accessed on 1 November 2019).
- Cashman, K.D.; Hill, T.R.; Lucey, A.J.; Taylor, N.; Seamans, K.M.; Muldowney, S.; Fitzgerald, A.P.; Flynn, A.; Barnes, M.S.; Horigan, G.; et al. Estimation of the dietary requirement for vitamin D in healthy adults. Am. J. Clin. Nutr. 2008, 88, 1535–1542. [Google Scholar] [CrossRef]
- Cashman, K.D.; Wallace, J.M.; Horigan, G.; Hill, T.R.; Barnes, M.S.; Lucey, A.J.; Bonham, M.P.; Taylor, N.; Duffy, E.M.; Seamans, K.; et al. Estimation of the dietary requirement for vitamin D in free-living adults >=64 y of age. Am. J. Clin. Nutr. 2009, 89, 1366–1374. [Google Scholar] [CrossRef]
- MacLaughlin, J.; Holick, M.F. Aging decreases the capacity of human skin to produce vitamin D3. J. Clin. Investig. 1985, 76, 1536–1538. [Google Scholar] [CrossRef]
- Cheng, T.Y.; Millen, A.E.; Wactawski-Wende, J.; Beresford, S.A.; LaCroix, A.Z.; Zheng, Y.; Goodman, G.E.; Thornquist, M.D.; Neuhouser, M.L. Vitamin D intake determines vitamin d status of postmenopausal women, particularly those with limited sun exposure. J. Nutr. 2014, 144, 681–689. [Google Scholar] [CrossRef][Green Version]
- Ohta, H.; Kuroda, T.; Onoe, Y.; Orito, S.; Ohara, M.; Kume, M.; Harada, A.; Tsugawa, N.; Okano, T.; Sasaki, S. The impact of lifestyle factors on serum 25-hydroxyvitamin D levels: A cross-sectional study in Japanese women aged 19–25 years. J. Bone Miner Metab. 2009, 27, 682–688. [Google Scholar] [CrossRef]
- Hyppönen, E.; Boucher, B.J. Adiposity, Vitamin D Requirements, and Clinical Implications for Obesity-Related Metabolic Abnormalities. Nutr. Rev. 2018, 76, 678–692. [Google Scholar] [CrossRef]
- Aloia, J.F.; Patel, M.; Dimaano, R.; Li-Ng, M.; Talwar, S.A.; Mikhail, M.; Pollack, S.; Yeh, J.K. Vitamin D intake to attain a desired serum 25-hydroxyvitamin D concentration. Am. J. Clin. Nutr. 2008, 87, 1952–1958. [Google Scholar] [CrossRef] [PubMed]
- Olds, W.J.; McKinley, A.R.; Moore, M.R.; Kimlin, M.G. In vitro model of vitamin D3 (cholecalciferol) synthesis by UV radiation: Dose-response relationships. J. Photochem. Photobiol. B 2008, 93, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Callegari, E.T.; Garland, S.M.; Gorelik, A.; Reavley, N.J.; Wark, J.D. Predictors and correlates of serum 25-hydroxyvitamin D concentrations in young women: Results from the Safe-D study. Br. J. Nutr. 2017, 118, 263–272. [Google Scholar] [CrossRef]
- Scragg, R.K.R.; Stewart, A.W.; McKenzie, R.L.; Reeder, A.I.; Liley, J.B.; Allen, M.W. Sun exposure and 25-hydroxyvitamin D3 levels in a community sample: Quantifying the association with electronic dosimeters. J. Expo. Sci. Environ. Epidemiol. 2017, 27, 471–477. [Google Scholar] [CrossRef]
- O’Sullivan, F.; Laird, E.; Kelly, D.; van Geffen, J.; van Weele, M.; McNulty, H.; Hoey, L.; Healy, M.; McCarroll, K.; Cunningham, C.; et al. Ambient UVB dose and sun enjoyment are important predictors of vitamin D status in an older population. J. Nutr. 2017, 147, 858–868. [Google Scholar] [CrossRef]
- Kimlin, M.G.; Olds, W.J.; Moore, M.R. Location and vitamin D synthesis: Is the hypothesis validated by geophysical data? J. Photochem. Photobiol. B 2007, 86, 234–239. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Seasona | n (%) or Mean, SD | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Study Area | Sex | ||||||||
| Hokkaido (lat.43° N, n = 54) | Kumamoto (lat.33° N, n = 53) | Men (n = 53) | Women (n = 54) | ||||||
| <Background> | |||||||||
| Age 20s | S, W | 11 | (20.4) | 9 | (17.0) | 9 | (17.0) | 11 | (20.4) |
| 30s | S, W | 9 | (16.7) | 11 | (20.8) | 11 | (20.8) | 9 | (16.7) |
| 40s | S, W | 12 | (22.2) | 12 | (22.6) | 12 | (22.6) | 12 | (22.2) |
| 50s | S, W | 12 | (22.2) | 11 | (20.8) | 11 | (20.8) | 12 | (22.2) |
| 60s | S, W | 10 | (18.5) | 10 | (18.9) | 10 | (18.9) | 10 | (18.5) |
| Height (cm) | S | 162.8 | 7.5 | 165.0 | 8.0 | 169.8 | 5.6 | 158.1 | 4.6 |
| Weight (kg) | S | 61.9 | 11.9 | 63.0 | 15.2 | 69.3 | 13.2 | 55.7 | 10.3 |
| BMI (kg/m2) | S | 23.2 | 3.8 | 23.0 | 4.2 | 24.0 | 3.9 | 22.3 | 3.9 |
| Skin typeb | |||||||||
| II | S | 14 | (25.9) | 18 | (34.0) | 11 | (20.8) | 21 | (38.9) |
| III | S | 27 | (50.0) | 25 | (47.2) | 28 | (52.8) | 24 | (44.4) |
| IV | S | 13 | (24.1) | 10 | (18.9) | 14 | (26.4) | 9 | (16.7) |
| <Blood test> | |||||||||
| 25(OH)D3 (ng/mL) | S | 22.3 | 6.7 | 20.0 | 6.7 | 24.1 | 6.8 | 18.3 | 5.5 |
| W | 15.6 | 6.6 | 13.7 | 4.3 | 15.6 | 5.4 | 13.7 | 5.7 | |
| Vitamin D status | |||||||||
| sufficient (20≤25(OH)D3) | S | 32 | (59.3) | 24 | (45.3) | 38 | (71.7) | 18 | (33.3) |
| insufficient (12≤25(OH)D3<20) | S | 20 | (37.0) | 23 | (43.4) | 14 | (26.4) | 29 | (53.7) |
| deficient (25(OH)D3<12) | S | 2 | (3.7) | 6 | (11.3) | 1 | (1.9) | 7 | (13.0) |
| sufficient (20≤25(OH)D3) | W | 15 | (27.8) | 4 | (7.6) | 12 | (22.6) | 7 | (13.0) |
| insufficient (12≤25(OH)D3<20) | W | 21 | (38.9) | 27 | (50.9) | 26 | (49.1) | 22 | (40.7) |
| deficient (25(OH)D3<12) | W | 18 | (33.3) | 22 | (41.5) | 15 | (28.3) | 25 | (46.3) |
| PTH intact (pg/mL) | S | 45.4 | 15.4 | 52.5 | 19.0 | 47.4 | 15.1 | 50.5 | 19.7 |
| W | 48.3 | 16.7 | 55.8 | 18.7 | 51.2 | 18.1 | 52.8 | 18.1 | |
| <Dietary intake> | |||||||||
| Energy (kcal) | S | 1804 | 699 | 1954 | 537 | 2071 | 559 | 1690 | 635 |
| W | 1776 | 497 | 1845 | 471 | 1968 | 449 | 1656 | 469 | |
| Vitamin D (μg/1000kcal) | S | 2.8 | 1.8 | 2.9 | 1.3 | 2.6 | 1.5 | 3.1 | 1.6 |
| W | 3.1 | 1.8 | 2.9 | 1.0 | 2.7 | 1.3 | 3.2 | 1.5 | |
| Fish (g/1000kcal) | S | 28.5 | 21.8 | 26.3 | 12.4 | 25.7 | 16.9 | 29.0 | 18.5 |
| W | 30.2 | 20.1 | 25.6 | 10.7 | 26.1 | 14.2 | 29.7 | 18.0 | |
| <Ultraviolet ray exposure> | |||||||||
| Exposure time (min/day) | S | 58.3 | 58.7 | 11.6 | 9.7 | 37.8 | 54.6 | 32.6 | 41.2 |
| W | 22.5 | 18.1 | 14.9 | 13.2 | 20.1 | 20.0 | 17.4 | 11.4 | |
| Exposure energy (J/day) | S | 494 | 598 | 144 | 162 | 407 | 594 | 236 | 291 |
| W | 104 | 93 | 99 | 118 | 105 | 118 | 99 | 93 | |
| <Lifestyle factors> | |||||||||
| Smoking | |||||||||
| Never | S | 27 | (50.0) | 33 | (62.3) | 20 | (37.7) | 40 | (74.1) |
| Past | S | 12 | (22.2) | 14 | (26.4) | 16 | (30.2) | 10 | (18.5) |
| Current | S | 15 | (27.8) | 6 | (11.3) | 17 | (32.1) | 4 | (7.4) |
| Occupation | |||||||||
| Manager | S | 2 | (3.7) | 4 | (7.5) | 6 | (11.3) | 0 | (0.0) |
| Professional | S | 7 | (13.0) | 21 | (39.6) | 10 | (18.9) | 18 | (33.3) |
| Clerical | S | 18 | (33.3) | 21 | (39.6) | 24 | (45.3) | 15 | (27.8) |
| Service and sales | S | 7 | (13.0) | 1 | (1.9) | 4 | (7.5) | 4 | (7.4) |
| Agricultural, forestry and fisheries | S | 7 | (13.0) | 0 | (0.0) | 3 | (5.7) | 4 | (7.4) |
| Craft and related trades | S | 4 | (7.4) | 0 | (0.0) | 3 | (5.7) | 1 | (1.9) |
| Othersc | S | 9 | (16.7) | 6 | (11.3) | 3 | (5.7) | 12 | (22.2) |
| Physical activity (Mets x minutes) | S | 496 | 741 | 164 | 153 | 368 | 654 | 296 | 455 |
| Sunscreen used | |||||||||
| Face | S | 13 | (24.1) | 22 | (41.5) | 1 | (1.9) | 34 | (63.0) |
| W | 11 | (20.4) | 17 | (32.1) | 0 | (0.0) | 28 | (51.9) | |
| Neck | S | 7 | (13.0) | 14 | (26.4) | 1 | (1.9) | 20 | (37.0) |
| W | 3 | (5.6) | 3 | (5.7) | 0 | (0.0) | 6 | (11.1) | |
| Arm | S | 6 | (11.1) | 12 | (22.6) | 1 | (1.9) | 17 | (31.5) |
| W | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | |
| Hand | S | 6 | (11.1) | 10 | (18.9) | 1 | (1.9) | 15 | (27.8) |
| W | 2 | (3.7) | 1 | (1.9) | 0 | (0.0) | 3 | (5.6) | |
| Anye | S | 13 | (24.1) | 22 | (41.5) | 1 | (1.9) | 34 | (63.0) |
| W | 11 | (20.4) | 17 | (32.1) | 0 | (0.0) | 28 | (51.9) | |
| Sunshade clothing/tools used | |||||||||
| Hat | S | 18 | (33.3) | 7 | (13.2) | 8 | (15.1) | 17 | (31.5) |
| W | 27 | (50.0) | 5 | (9.4) | 18 | (34.0) | 14 | (25.9) | |
| Parasol | S | 6 | (11.1) | 22 | (41.5) | 3 | (5.7) | 25 | (46.3) |
| W | 2 | (3.7) | 0 | (0.0) | 1 | (1.9) | 1 | (1.9) | |
| Long sleeves | S | 13 | (24.1) | 10 | (18.9) | 9 | (17.0) | 14 | (25.9) |
| W | 52 | (96.3) | 53 | (100.0) | 52 | (98.1) | 53 | (98.2) | |
| Gloves | S | 11 | (20.4) | 12 | (22.7) | 5 | (9.4) | 18 | (33.3) |
| W | 35 | (64.9) | 14 | (26.4) | 25 | (47.2) | 24 | (44.5) | |
| Combinationf | S | 24 | (44.4) | 24 | (45.3) | 12 | (22.6) | 36 | (66.7) |
| W | 37 | (68.5) | 17 | (32.1) | 28 | (52.8) | 26 | (48.2) | |
| Season | Variable | Unit, Category (Ref) | Model 1time | Model 2time | ||||
|---|---|---|---|---|---|---|---|---|
| Regression Coefficient | 95%CI | p Value | Regression Coefficient | 95%CI | p Value | |||
| Summer | VD intake | μg/1000kcal | 1.00 | (0.34, 1.67) | 0.004 | 0.88 | (0.14, 1.62) | 0.020 |
| UV exposure time | min | 0.059 | (0.034, 0.083) | <0.001 | 0.047 | (0.014, 0.079) | 0.005 | |
| Sex | women (vs men) | −5.94 | <0.001 | −5.39 | 0.001 | |||
| Area | Kumamoto (vs Hokkaido) | 0.34 | 0.77 | −0.17 | 0.90 | |||
| Age | years | 0.08 | 0.08 | |||||
| Smoking | past smoker (vs nonsmoker) | −0.12 | 0.93 | |||||
| current smoker (vs nonsmoker) | −0.76 | 0.62 | ||||||
| Skin typea | III (vs II) | −0.46 | 0.71 | |||||
| IV (vs II) | 0.25 | 0.87 | ||||||
| Sunscreen useb | user (vs nonuser) | −1.67 | 0.29 | |||||
| Sunshade clothing/tools usec | user (vs nonuser) | 0.53 | 0.70 | |||||
| Physical activityd | Mets x min | 0.00 | 0.93 | |||||
| Winter | VD intake | μg/1000kcal | 1.88 | (1.25, 2.52) | <0.001 | 1.70 | (1.09, 2.32) | <0.001 |
| UV exposure time | min | 0.067 | (0.0097, 0.125) | 0.022 | 0.041 | (−0.016, 0.099) | 0.16 | |
| Sex | women (vs men) | −2.65 | 0.005 | −1.90 | 0.10 | |||
| Area | Kumamoto (vs Hokkaido) | −1.05 | 0.26 | −0.73 | 0.45 | |||
| Age | years | 0.12 | 0.001 | |||||
| Smoking | past smoker (vs nonsmoker) | −0.92 | 0.42 | |||||
| current smoker (vs nonsmoker) | 0.61 | 0.63 | ||||||
| Skin typea | III (vs II) | 0.42 | 0.69 | |||||
| IV (vs II) | −0.27 | 0.83 | ||||||
| Sunscreen useb | user (vs nonuser) | −1.27 | 0.33 | |||||
| Sunshade clothing/tools usec | user (vs nonuser) | 1.11 | 0.24 | |||||
| Season | Variable | Unit, Category (Ref) | Model 1energy | Model 2energy | ||||
|---|---|---|---|---|---|---|---|---|
| Regression Coefficient | 95%CI | p Value | Regression Coefficient | 95%CI | p Value | |||
| Summer | VD intake | μg/1000kcal | 1.10 | (0.41, 1.79) | 0.002 | 0.81 | (0.083, 1.55) | 0.029 |
| UV exposure energya | J/day | 0.004 | (0.0020, 0.0069) | 0.001 | 0.004 | (0.001, 0.007) | 0.012 | |
| Sex | women (vs men) | −5.52 | <0.001 | −5.80 | <0.001 | |||
| Area | Kumamoto (vs Hokkaido) | −0.85 | 0.46 | −1.41 | 0.23 | |||
| Age | years | 0.12 | 0.005 | |||||
| Smoking | past smoker (vs nonsmoker) | 0.02 | 0.99 | |||||
| current smoker (vs nonsmoker) | −1.01 | 0.51 | ||||||
| Skin typeb | III (vs II) | −0.51 | 0.69 | |||||
| IV (vs II) | 0.15 | 0.93 | ||||||
| Physical activityc | Mets x min | 0.00 | 0.90 | |||||
| Winter | VD intake | μg/1000kcal | 1.94 | (1.29, 2.58) | <0.001 | 1.75 | (1.13, 2.36) | <0.001 |
| UV exposure energy | J/day | 0.005 | (−0.004, 0.013) | 0.29 | 0.004 | (−0.005, 0.012) | 0.37 | |
| Sex | women (vs men) | −2.83 | 0.003 | −2.66 | 0.007 | |||
| Area | Kumamoto (vs Hokkaido) | −1.53 | 0.10 | −1.58 | 0.08 | |||
| Age | years | 0.14 | <0.001 | |||||
| Smoking | past smoker (vs nonsmoker) | −0.72 | 0.53 | |||||
| current smoker (vs nonsmoker) | 0.61 | 0.63 | ||||||
| Skin typeb | III (vs II) | 0.59 | 0.57 | |||||
| IV (vs II) | −0.08 | 0.95 | ||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asakura, K.; Etoh, N.; Imamura, H.; Michikawa, T.; Nakamura, T.; Takeda, Y.; Mori, S.; Nishiwaki, Y. Vitamin D Status in Japanese Adults: Relationship of Serum 25-Hydroxyvitamin D with Simultaneously Measured Dietary Vitamin D Intake and Ultraviolet Ray Exposure. Nutrients 2020, 12, 743. https://doi.org/10.3390/nu12030743
Asakura K, Etoh N, Imamura H, Michikawa T, Nakamura T, Takeda Y, Mori S, Nishiwaki Y. Vitamin D Status in Japanese Adults: Relationship of Serum 25-Hydroxyvitamin D with Simultaneously Measured Dietary Vitamin D Intake and Ultraviolet Ray Exposure. Nutrients. 2020; 12(3):743. https://doi.org/10.3390/nu12030743
Chicago/Turabian StyleAsakura, Keiko, Norihito Etoh, Haruhiko Imamura, Takehiro Michikawa, Takahiro Nakamura, Yuki Takeda, Sachie Mori, and Yuji Nishiwaki. 2020. "Vitamin D Status in Japanese Adults: Relationship of Serum 25-Hydroxyvitamin D with Simultaneously Measured Dietary Vitamin D Intake and Ultraviolet Ray Exposure" Nutrients 12, no. 3: 743. https://doi.org/10.3390/nu12030743
APA StyleAsakura, K., Etoh, N., Imamura, H., Michikawa, T., Nakamura, T., Takeda, Y., Mori, S., & Nishiwaki, Y. (2020). Vitamin D Status in Japanese Adults: Relationship of Serum 25-Hydroxyvitamin D with Simultaneously Measured Dietary Vitamin D Intake and Ultraviolet Ray Exposure. Nutrients, 12(3), 743. https://doi.org/10.3390/nu12030743