Effects of Supplementing the Usual Diet with a Daily Dose of Walnuts for Two Years on Metabolic Syndrome and Its Components in an Elderly Cohort

 , , , ,
, , , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
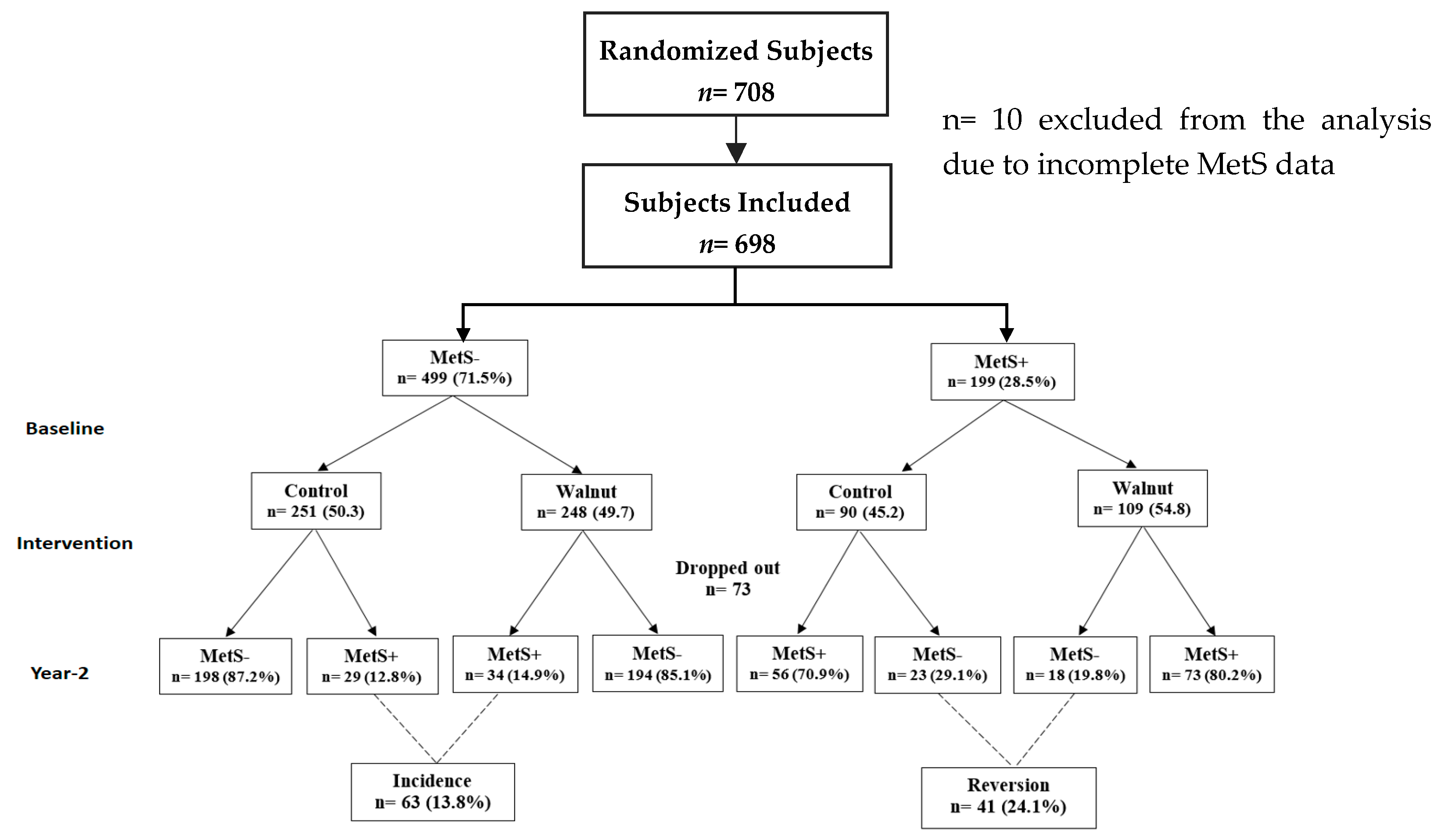
2.1. Study Design and Intervention
2.2. Measurements
2.3. Determination of MetS
2.4. Compliance and Retention
2.5. Measuring Tools
2.6. Statistical Methods and Analyses
3. Results
3.1. Demographic Profile of Participants
3.2. Nutrient Profile
3.3. Changes in Metabolic Syndrome Components
3.4. Changes in MetS Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rao, D.P.; Dai, S.; Lagace, C.; Krewski, D. Metabolic syndrome and chronic disease. Chronic Dis. Inj. Can. 2014, 34, 36–45. [Google Scholar] [PubMed]
- American Heart Association. Symptoms and Diagnosis of Metabolic Syndrome. Available online: http://www.heart.org/HEARTORG/Conditions/More/MetabolicSyndrome/Symptoms-and-Diagnosis-of-Metabolic-Syndrome_UCM_301925_Article.jsp (accessed on 20 August 2019).
- National Heart Lung and Blood Institute. What is Metabolic Syndrome? Available online: https://www.nhlbi.nih.gov/health-topics/metabolic-syndrome# (accessed on 10 September 2019).
- Grundy, S.M. Metabolic syndrome pandemic. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.X.; Chaudhary, N.; Akinyemiju, T. Metabolic syndrome prevalence by race/ethnicity and sex in the United States, National Health and Nutrition Examination Survey, 1988–2012. Prev. Chronic Dis. 2017, 14, E24. [Google Scholar] [CrossRef] [PubMed]
- Beltran-Sanchez, H.; Harhay, M.O.; Harhay, M.M.; McElligott, S. Prevalence and trends of metabolic syndrome in the adult U.S. population, 1999–2010. J. Am. Coll. Cardiol. 2013, 62, 697–703. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S.; Giles, W.H.; Dietz, W.H. Prevalence of the metabolic syndrome among US adults: Findings from the third National Health and Nutrition Examination Survey. JAMA 2002, 287, 356–359. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Martínez, P.; Mikhailidis, D.P.; Athyros, V.G.; Bullo, M.; Couture, P.; Covas, M.I.; de Koning, L.; Delgado-Lista, J.; Díaz-López, A.; Drevon, C.A.; et al. Lifestyle recommendations for the prevention and management of metabolic syndrome: An international panel recommendation. Nutr. Rev. 2017, 75, 307–326. [Google Scholar] [CrossRef]
- Rizzo, N.S.; Sabaté, J.; Jaceldo-Siegl, K.; Fraser, G.E. Vegetarian dietary patterns are associated with a lower risk of metabolic syndrome: The adventist health study 2. Diabetes Care 2011, 34, 1225–1227. [Google Scholar] [CrossRef]
- Babio, N.; Bullo, M.; Salas-Salvado, J. Mediterranean diet and metabolic syndrome: The evidence. Public Health Nutr. 2009, 12, 1607–1617. [Google Scholar] [CrossRef]
- Salas-Salvadó, J.; Fernández-Ballart, J.; Ros, E.; Martinez-Gonzalez, M.A.; Fitó, M.; Estruch, R.; Corella, D.; Fiol, M.; Gómez-Gracia, E.; Arós, F.; et al. Effect of a Mediterranean diet supplemented with nuts on metabolic syndrome status: One-year results of the PREDIMED randomized trial. JAMA Intern. Med. 2008, 168, 2449–2458. [Google Scholar] [CrossRef]
- Ros, E. Health benefits of nut consumption. Nutrients 2010, 2, 652–682. [Google Scholar] [CrossRef]
- King, J.C.; Blumberg, J.; Ingwersen, L.; Jenab, M.; Tucker, K.L. Tree nuts and peanuts as components of a healthy diet. J. Nutr. 2008, 138, 1736S–1740S. [Google Scholar] [CrossRef] [PubMed]
- Del Gobbo, L.C.; Falk, M.C.; Feldman, R.; Lewis, K.; Mozaffarian, D. Effects of tree nuts on blood lipids, apolipoproteins, and blood pressure: Systematic review, meta-analysis, and dose-response of 61 controlled intervention trials. Am. J. Clin. Nutr. 2015, 102, 1347–1356. [Google Scholar] [CrossRef] [PubMed]
- Blanco Mejia, S.; Kendall, C.W.; Viguiliouk, E.; Augustin, L.S.; Ha, V.; Cozma, A.I.; Mirrahimi, A.; Maroleanu, A.; Chiavaroli, L.; Leiter, L.A.; et al. Effect of tree nuts on metabolic syndrome criteria: A systematic review and meta-analysis of randomised controlled trials. BMJ Open 2014, 4, e004660. [Google Scholar] [CrossRef] [PubMed]
- Hayes, D.; Angove, M.J.; Tucci, J.; Dennis, C. Walnuts (Juglans regia) chemical composition and research in human health. Crit. Rev. Food Sci. Nutr. 2016, 56, 1231–1241. [Google Scholar] [CrossRef]
- Sánchez-González, C.; Ciudad, C.J.; Noé, V.; Izquierdo-Pulido, M. Health benefits of walnut polyphenols: An exploration beyond their lipid profile. Crit. Rev. Food Sci. Nutr. 2017, 57, 3373–3383. [Google Scholar] [CrossRef]
- Ros, E.; Izquierdo-Pulido, M.; Sala-Vila, A. Beneficial effects of walnut consumption on human health: Role of micronutrients. Curr. Opin. Clin. Nutr. Metab. Care 2018, 21, 498–504. [Google Scholar] [CrossRef]
- Wu, H.; Pan, A.; Yu, Z.; Qi, Q.; Lu, L.; Zhang, G.; Yu, D.; Zong, G.; Zhou, Y.; Chen, X.; et al. Lifestyle counseling and supplementation with flaxseed or walnuts influence the management of metabolic syndrome. J. Nutr. 2010, 140, 1937–1942. [Google Scholar] [CrossRef]
- Mukuddem-Petersen, J.; Stonehouse Oosthuizen, W.; Jerling, J.C.; Hanekom, S.M.; White, Z. Effects of a high walnut and high cashew nut diet on selected markers of the metabolic syndrome: A controlled feeding trial. Br. J. Nutr. 2007, 97, 1144–1153. [Google Scholar] [CrossRef]
- Babio, N.; Toledo, E.; Estruch, R.; Ros, E.; Martínez-González, M.A.; Castañer, O.; Bulló, M.; Corella, D.; Arós, F.; Gómez-Gracia, E.; et al. Mediterranean diets and metabolic syndrome status in the PREDIMED randomized trial. Can. Med. Assoc. J. 2014, 186, E649–E657. [Google Scholar] [CrossRef]
- Rajaram, S.; Valls-Pedret, C.; Cofan, M.; Sabaté, J.; Serra-Mir, M.; Perez-Heras, A.M.; Arechiga, A.; Casaroli-Marano, R.P.; Alforja, S.; Sala-Vila, A.; et al. The Walnuts and Healthy Aging study (WAHA): Protocol for a nutritional intervention trial with walnuts on brain aging. Front. Aging Neurosci. 2016, 8, 333. [Google Scholar] [CrossRef]
- World Health Organization. Energy and Protein Requirements; Technical Report Series, 724. WHO: Geneva, Switzerland, 1985. [Google Scholar]
- Hivert, M.F.; Grant, R.W.; Shrader, P.; Meigs, J.B. Identifying primary care patients at risk for future diabetes and cardiovascular disease using electronic health records. BMC Health Serv. Res. 2009, 9, 170. [Google Scholar] [CrossRef] [PubMed]
- Anwar, Y.A.; Giacco, S.; McCabe, E.J.; Tendler, B.E.; White, W.B. Evaluation of the efficacy of the Omron HEM-737 IntelliSense device for use on adults according to the recommendations of the Association for the Advancement of Medical Instrumentation. Blood Press. Monit. 1998, 3, 261–265. [Google Scholar] [PubMed]
- Sala-Vila, A.; Harris, W.S.; Cofan, M.; Perez-Heras, A.M.; Pinto, X.; Lamuela-Raventos, R.M.; Covas, M.I.; Estruch, R.; Ros, E. Determinants of the omega-3 index in a Mediterranean population at increased risk for CHD. Br. J. Nutr. 2011, 106, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Richardson, M.T.; Leon, A.S.; Jacobs, D.R., Jr.; Ainsworth, B.E.; Serfass, R. Comprehensive evaluation of the Minnesota Leisure Time Physical Activity Questionnaire. J. Clin. Epidemiol. 1994, 47, 271–281. [Google Scholar] [CrossRef]
- Molina, L.; Sarmiento, M.; Peñafiel, J.; Donaire, D.; Garcia-Aymerich, J.; Gomez, M.; Ble, M.; Ruiz, S.; Frances, A.; Schröder, H.; et al. Validation of the Regicor Short Physical Activity Questionnaire for the adult population. PLoS ONE 2017, 12, e0168148. [Google Scholar] [CrossRef]
- Haskell, W.L.; Lee, I.M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1423–1434. [Google Scholar]
- Bitok, E.; Jaceldo-Siegl, K.; Rajaram, S.; Serra-Mir, M.; Roth, I.; Feitas-Simoes, T.; Ros, E.; Sabaté, J. Favourable nutrient intake and displacement with long-term walnut supplementation among elderly: Results of a randomised trial. Br. J. Nutr. 2017, 118, 201–209. [Google Scholar] [CrossRef]
- Domenech, M.; Serra-Mir, M.; Roth, I.; Freitas-Simoes, T.; Valls-Pedret, C.; Cofán, M.; López, A.; Sala-Vila, A.; Calvo, C.; Rajaram, S.; et al. Effect of a walnut diet on office and 24-h ambulatory blood pressure in elderly individuals: Findings from the Walnuts And Healthy Aging (WAHA) randomized trial. Hypertension 2019, 73, 1049–1057. [Google Scholar] [CrossRef]
- Casas, R.; Sacanella, E.; Urpi-Sarda, M.; Chiva-Blanch, G.; Ros, E.; Martinez-Gonzalez, M.A.; Covas, M.I.; Lamuela-Raventos, R.M.; Salas-Savlvadó, J.; Fiol, M.; et al. The effects of the Mediterranean diet on biomarkers of vascular wall inflammation and plaque vulnerability in subjects with high risk for cardiovascular disease: A randomized trial. PLoS ONE 2014, 9, e100084. [Google Scholar] [CrossRef]
- O’Neil, C.E.; Keast, D.R.; Nicklas, T.A.; Fulgoni, V.L., 3rd. Nut consumption is associated with decreased health risk factors for cardiovascular disease and metabolic syndrome in U.S. adults: NHANES 1999–2004. J. Am. Coll. Cardiol. 2011, 30, 502–510. [Google Scholar] [CrossRef]
- West, S.G.; Krick, A.L.; Klein, L.C.; Zhao, G.; Wojtowicz, T.F.; McGuiness, M.; Bagshaw, D.M.; Wagner, P.; Ceballos, R.M.; Holub, B.J.; et al. Effects of diets high in walnuts and flax oil on hemodynamic responses to stress and vascular endothelial function. J. Am. Coll. Cardiol. 2010, 29, 595–603. [Google Scholar] [CrossRef]
- Casas-Agustench, P.; Lopez-Uriarte, P.; Ros, E.; Bullo, M.; Salas-Salvado, J. Nuts, hypertension and endothelial function. Nutr. Metab. Cardiovasc. Dis. 2011, S21–S33. [Google Scholar] [CrossRef] [PubMed]
- Salas-Salvado, J.; Guasch-Ferre, M.; Bullo, M.; Sabaté, J. Nuts in the prevention and treatment of metabolic syndrome. Am. J. Clin. Nutr. 2014, 399S–407S. [Google Scholar] [CrossRef] [PubMed]
- Guasch-Ferré, M.; Li, J.; Hu, F.B.; Salas-Salvadó, J.; Tobias, D.K. Effects of walnut consumption on blood lipids and other cardiovascular risk factors: An updated meta-analysis and systematic review of controlled trials. Am. J. Clin. Nutr. 2018, 108, 174–187. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.J.; Nam, G.E.; Seo, J.A.; Yoon, T.; Seo, I.; Lee, J.H.; Im, D.; Bahn, K.N.; Jeong, S.A.; Kang, T.S.; et al. Nut consumption has favorable effects on lipid profiles of Korean women with metabolic syndrome. Nutr. Res. 2014, 34, 814–820. [Google Scholar] [CrossRef] [PubMed]
- Jaceldo-Siegl, K.; Haddad, E.; Oda, K.; Fraser, G.E.; Sabaté, J. Tree nuts are inversely associated with metabolic syndrome and obesity: The Adventist health study-2. PLoS ONE 2014, 9, e85133. [Google Scholar] [CrossRef] [PubMed]
- Sabaté, J.; Fraser, G.E.; Burke, K.; Knutsen, S.F.; Bennett, H.; Lindsted, K.D. Effects of walnuts on serum lipid levels and blood pressure in normal men. N. Engl. J. Med. 1993, 328, 603–607. [Google Scholar] [CrossRef]
- Iwamoto, M.; Imaizumi, K.; Sato, M.; Hirooka, Y.; Sakai, K.; Takeshita, A.; Kono, M. Serum lipid profiles in Japanese women and men during consumption of walnuts. Eur. J. Clin. Nutr. 2002, 56, 629–637. [Google Scholar] [CrossRef]
- Zambon, D.; Sabaté, J.; Munoz, S.; Campero, B.; Casals, E.; Merlos, M.; Laguna, J.C.; Ros, E. Substituting walnuts for monounsaturated fat improves the serum lipid profile of hypercholesterolemic men and women: A randomized crossover trial. Ann. Intern. Med. 2000, 132, 538–546. [Google Scholar] [CrossRef]
- Kris-Etherton, P.M. Walnuts decrease risk of cardiovascular disease: A summary of efficacy and biologic mechanisms. J. Nutr. 2014, 144, 547S–554S. [Google Scholar] [CrossRef]
- Damasceno, N.R.; Sala-Vila, A.; Cofan, M.; Perez-Heras, A.M.; Fito, M.; Ruiz-Gutierrez, V.; Martinez-Gonzalez, M.A.; Corella, D.; Aros, F.; Estruch, R.; et al. Mediterranean diet supplemented with nuts reduces waist circumference and shifts lipoprotein subfractions to a less atherogenic pattern in subjects at high cardiovascular risk. Atherosclerosis 2013, 230, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Gulati, S.; Misra, A.; Pandey, R.M.; Bhatt, S.P.; Saluja, S. Effects of pistachio nuts on body composition, metabolic, inflammatory and oxidative stress parameters in Asian Indians with metabolic syndrome: A 24-wk, randomized control trial. Nutrition 2014, 30, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Sala-Vila, A.; Valls-Pedret, C.; Rajaram, S.; Coll-Padrós, N.; Cofán, M.; Serra-Mir, M.; Pérez-Heras, A.; Roth, I.; Freitas-Simoes, T.; Doménech, M.; et al. Effect of a 2-year diet intervention with walnuts on cognitive decline. The Walnuts And Healthy Aging (WAHA) study: A randomized controlled trial. Am. J. Clin. Nutr. 2020, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.; Park, H.; Kim, S.; Kim, J. Decrease in HDL-C is associated with age and household income in adults from the Korean National Health and Nutrition Examination Survey 2017: Correlation analysis of low HDL-C and poverty. Int. J. Environ. Res. Public Health 2019, 16, 3329. [Google Scholar] [CrossRef] [PubMed]
- Pieters, M.; Oosthuizen, W.; Jerling, J.C.; Loots, D.T.; Mukuddem-Petersen, J.; Hanekom, S.M. Clustering of haemostatic variables and the effect of high cashew and walnut diets on these variables in metabolic syndrome patients. Blood Coagul. Fibrinolysis 2005, 16, 429–437. [Google Scholar] [CrossRef]
- Fernandez-Montero, A.; Bes-Rastrollo, M.; Beunza, J.J.; Barrio-Lopez, M.T.; de la Fuente-Arrillaga, C.; Moreno-Galarraga, L.; Martinez-Gonzalez, M.A. Nut consumption and incidence of metabolic syndrome after 6-year follow-up: The SUN (Seguimiento Universidad de Navarra, University of Navarra Follow-up) cohort. Public Health Nutr. 2013, 16, 2064–2072. [Google Scholar] [CrossRef]
- Ibarrola-Jurado, N.; Bullo, M.; Guasch-Ferre, M.; Ros, E.; Martinez-Gonzalez, M.A.; Corella, D.; Fiol, M.; Warnberg, J.; Estruch, R.; Roman, P.; et al. Cross-sectional assessment of nut consumption and obesity, metabolic syndrome and other cardiometabolic risk factors: The PREDIMED study. PLoS ONE 2013, 8, e57367. [Google Scholar] [CrossRef]
- Gallagher, D.; Ruts, E.; Visser, M.; Heshka, S.; Baumgartner, R.N.; Wang, J.; Pierson, R.N.; Pi-Sunyer, F.X.; Heymsfield, S.B. Weight stability masks sarcopenia in elderly men and women. Am. J. Physiol. Endocrinol. Metab. 2000, 279, E366–E375. [Google Scholar] [CrossRef]
- Forbes, G.B. Longitudinal changes in adult fat-free mass: Influence of body weight. Am. J. Clin. Nutr. 1999, 70, 1025–1031. [Google Scholar] [CrossRef]
- Zamboni, M.; Zoico, E.; Scartezzini, T.; Mazzali, G.; Tosoni, P.; Zivelonghi, A.; Gallagher, D.; De Pergola, G.; Di Francesco, V.; Bosello, O. Body composition changes in stable-weight elderly subjects: The effect of sex. Aging Clin. Exp. Res. 2003, 15, 321–327. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Control | Walnut | Total (n = 625) | ||
|---|---|---|---|---|---|
| MetS- (n = 199) | MetS+ (n = 107) | MetS- (n = 187) | MetS+ (n = 132) | ||
| Center, n (%) | |||||
| LLU | 101 (50.8) | 44 (41.1) | 97 (51.9) | 57 (43.2) | 299 (48.0) |
| BCN | 98 (49.2) | 63 (58.9) | 90 (48.1) | 75 (56.8) | 326 (2.0) |
| Age, y, mean (SD) | 68.7 (3.4) | 69.1 (3.6) | 69.4 (3.7) | 69.2 (3.7) | 69.1 (3.6) |
| Body weight, kg, mean (SD) | 69.7 (13.0) | 80.8 (15.7) | 68.5 (12.3) | 80.5 (16.7) | 73.5 (15.2) |
| Gender, n (%) | |||||
| Women | 145 (72.9) | 64 (59.8) | 125 (66.8) | 86 (65.2) | 420 (67.1) |
| Men | 54 (27.1) | 43 (40.2) | 62 (33.2) | 46 (34.8) | 205 (32.9) |
| Race, n (%) | |||||
| LLU | |||||
| White | 76 (75.3) | 34 (77.3) | 78 (80.4) | 43 (75.4) | 231 (77.3) |
| Hispanics | 9 (8.9) | 6 (13.6) | 9 (9.3) | 8 (14.0) | 32 (10.7) |
| Black | 6 (5.9) | 3 (6.8) | 7 (7.2) | 5 (8.8) | 21 (7.0) |
| Other | 10 (9.9) | 1 (2.3) | 3 (3.1) | 1 (1.8) | 15 (5.0) |
| BCN (Caucasian) | 98 (100) | 63 (100) | 90 (100) | 75 (100) | 326 (100) |
| Education, n (%) | |||||
| Secondary or less | 83 (41.7) | 45 (42.1) | 71 (38.0) | 55 (41.7) | 254 (40.5) |
| Post-secondary | 116 (58.3) | 62 (57.9) | 116 (62.0) | 77 (58.3) | 371 (59.5) |
| Ever smoker, n (%) | |||||
| Never | 177 (88.9) | 82 (76.6) | 160 (85.6) | 107 (81.1) | 526 (84.2) |
| Yes | 22 (11.1) | 25 (23.4) | 27 (14.4) | 25 (18.9) | 99 (15.8) |
| MetS Components, mean (SD) | |||||
| BMI, kg/m2 | 26.2 (4.2) | 30.2 (4.0) | 25.3 (3.3) | 29.6 (4.4) | 27.3 (4.5) |
| Systolic BP, mm Hg | 125.2 (16.9) | 130.9 (15.8) | 122.8 (14.7) | 131.6 (13.9) | 126.8 (15.9) |
| Diastolic BP, mm Hg | 77.0 (9.4) | 80.0 (8.6) | 75.6 (8.8) | 81.3 (7.7) | 78.0 (9.0) |
| Triglycerides, mg/dL | 86.7 (31.5) | 126.6 (51.5) | 85.9 (30.1) | 130.7 (57.5) | 102.6 (46.5) |
| HDL cholesterol, mg/dL | 60.8 (14.3) | 51.0 (12.0) | 59.3 (15.1) | 49.8 (14.1) | 56.4 (14.9) |
| Fasting serum glucose, mg/dL | 93.5 (12.4) | 105.6 (18.1) | 92.5 (11.5) | 107.1 (17.0) | 98.1 (15.7) |
| Medications, n (%) | |||||
| Antihypertensive agents | |||||
| No | 128 (64.3) | 34 (31.8) | 130 (69.5) | 41 (31.1) | 333 (53.3) |
| Yes | 71 (35.7) | 73 (68.2) | 57 (30.5) | 91 (68.9) | 292 (46.7) |
| Antidiabetic agents | |||||
| No | 196 (98.5) | 94 (87.9) | 183 (97.9) | 114 (86.4) | 587 (93.9) |
| Yes | 3 (1.5) | 13 (12.1) | 4 (2.1) | 18 (13.6) | 38 (6.1) |
| Statins | |||||
| No | 159 (79.9) | 52 (48.6) | 165 (88.2) | 51 (38.6) | 427 (68.3) |
| Yes | 40 (20.1) | 55 (51.4) | 22 (11.8) | 81 (61.4) | 198 (31.7) |
| Other lipid lowering drugs | |||||
| No | 197 (99.0) | 99 (92.5) | 186 (99.5) | 126 (95.5) | 608 (97.3) |
| Yes | 2 (1.0) | 8 (7.5) | 1 (0.5) | 6 (4.5) | 17 (2.7) |
| Physical activity MET median (IQR) | 2825 (2670) | 2124 (2757) | 2797 (2218) | 2381 (2785) | 2625 (2666) |
| Nutrients | Control (n = 312) Mean * (SD) | Walnut (n = 324) Mean * (SD) | P-Value ** |
|---|---|---|---|
| Energy (kcal) | 1632.5 (376) | 1842.3 (442) | <0.0001 |
| Total carbohydrate, g/d | 186.8 (56) | 189.6 (63) | 0.621 |
| Total protein, g/d | 70.7 (18) | 75.8 (18) | 0.0003 |
| Total Fat, g/d | 66.8 (19) | 89.3 (23) | <0.0001 |
| SFA, g/d | 19.2 (8) | 20.8 (8) | 0.005 |
| MUFA, g/d | 30.0 (11) | 32.0 (12) | 0.027 |
| PUFA, g/d | 11.5 (5) | 29.6 (7) | <0.0001 |
| α-Linolenic acid, mcg/d | 1.1 (1) | 4.6 (1) | <0.0001 |
| Linoleic acid, mcg/d | 9.7 (5) | 24.3 (6) | <0.0001 |
| Total fiber, g/d | 19.1 (7) | 22.0 (8) | <0.0001 |
| Total carbohydrate (%E) | 45.2 (8) | 40.3 (7) | <0.0001 |
| Total protein (%E) | 17.6 (4) | 16.6 (3) | 0.001 |
| Total fat (%E) | 36.0 (6) | 42.8 (6) | <0.0001 |
| Total SFA (%E) | 10.3 (3) | 9.9 (2) | 0.074 |
| Total MUFA (%E) | 16.3 (5) | 15.3 (5) | 0.013 |
| Total PUFA (%E) | 6.2 (2) | 14.4 (3) | <0.0001 |
| Variables | Baseline | Year 2 | Difference (year 2 Minus Baseline) | Group × Time Interaction P-value ** | |
|---|---|---|---|---|---|
| Adjusted Mean (95% CI) | Adjusted Mean (95% CI) | Mean (95% CI) | P-value * | ||
| BMI | |||||
| Control | 27.5 (27.3, 27.7) | 27.5 (27.3, 27.8) | 0.03 (0.0, 0.06) a | 0.025 | 0.696 |
| Walnut | 27.1 (26.9, 27.3) | 27.2 (26.9, 27.4) | 0.04 (0.01, 0.07) a | 0.004 | |
| Systolic BP | |||||
| Control | 128.0 (126.4,129.7) | 128.0 (126.3, 129.8) | 0.01 (−1.7, 1.67) a | 0.99 | 0.265 |
| Walnut | 126.9 (125.3, 128.5) | 125.6 (123.9, 127.3) | −1.30 (−2.9, 0.31) a | 0.114 | |
| Diastolic BP | |||||
| Control | 78.2 (77.3, 79.2) | 78.2 (77.1, 79.2) | −0.08 (−1.07, 0.92) a | 0.88 | 0.369 |
| Walnut | 77.8 (76.9, 78.8) | 77.1 (76.1, 78.1) | −0.71 (−1.68, 0.26) a | 0.15 | |
| HDL-C | |||||
| Control | 55.2 (53.8, 56.6) | 52.4 (51.0, 53.8) | 0.95 (0.93, 0.97) b | <0.0001 | 0.836 |
| Walnut | 52.8 (51.6, 54.1) | 50.0 (48.8, 51.3) | 0.95 (0.93, 0.96) b | <0.0001 | |
| Triglycerides | |||||
| Control | 93.2 (89.2, 97.3) | 89.4 (85.3, 93.7) | 0.96 (0.93, 0.99) b | 0.02 | 0.484 |
| Walnut | 96.6 (92.6, 100.7) | 91.1 (87.1, 95.3) | 0.94 (0.91, 0.98) b | 0.0007 | |
| FBG | |||||
| Control | 96.8 (95.5, 98.1) | 95.7 (94.3, 97.2) | 0.99 (0.98, 1.0) b | 0.086 | 0.194 |
| Walnut | 97.7 (96.4, 99.0) | 97.8 (96.4, 99.2) | 1.0 (0.99, 1.0) b | 0.923 | |
| Year 2 vs. Baseline OR (95% CI) | P-Value | Group × Time Interaction P-value | |
|---|---|---|---|
| Control | 1.11 (0.78, 1.59) | 0.555 | |
| Walnut | 1.25 (0.89, 1.75) | 0.192 | 0.62 |
| Walnut vs. Control OR (95% CI) | P-value | |
|---|---|---|
| Reversion rate | 0.70 (0.31, 1.58) | 0.395 |
| Incidence rate | 1.29 (0.67, 2.49) | 0.441 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Abdrabalnabi, A.; Rajaram, S.; Bitok, E.; Oda, K.; Beeson, W.L.; Kaur, A.; Cofán, M.; Serra-Mir, M.; Roth, I.; Ros, E.; et al. Effects of Supplementing the Usual Diet with a Daily Dose of Walnuts for Two Years on Metabolic Syndrome and Its Components in an Elderly Cohort. Nutrients 2020, 12, 451. https://doi.org/10.3390/nu12020451
Al Abdrabalnabi A, Rajaram S, Bitok E, Oda K, Beeson WL, Kaur A, Cofán M, Serra-Mir M, Roth I, Ros E, et al. Effects of Supplementing the Usual Diet with a Daily Dose of Walnuts for Two Years on Metabolic Syndrome and Its Components in an Elderly Cohort. Nutrients. 2020; 12(2):451. https://doi.org/10.3390/nu12020451
Chicago/Turabian StyleAl Abdrabalnabi, Ahmed, Sujatha Rajaram, Edward Bitok, Keiji Oda, W. Lawrence Beeson, Amandeep Kaur, Montserrat Cofán, Mercè Serra-Mir, Irene Roth, Emilio Ros, and et al. 2020. "Effects of Supplementing the Usual Diet with a Daily Dose of Walnuts for Two Years on Metabolic Syndrome and Its Components in an Elderly Cohort" Nutrients 12, no. 2: 451. https://doi.org/10.3390/nu12020451
APA StyleAl Abdrabalnabi, A., Rajaram, S., Bitok, E., Oda, K., Beeson, W. L., Kaur, A., Cofán, M., Serra-Mir, M., Roth, I., Ros, E., & Sabaté, J. (2020). Effects of Supplementing the Usual Diet with a Daily Dose of Walnuts for Two Years on Metabolic Syndrome and Its Components in an Elderly Cohort. Nutrients, 12(2), 451. https://doi.org/10.3390/nu12020451