The Prevalence of Orthorexia Nervosa in Polish and Lebanese Adults and Its Relationship with Sociodemographic Variables and BMI Ranges: A Cross-Cultural Perspective


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. Measures
2.2.1. Translation Procedure of the Questionnaire Used in a Lebanese Sample
2.2.2. ON
2.2.3. Sociodemographic Variables
2.3. Statistical Analysis
3. Results
3.1. Sociodemographic Characteristics of the Sample Population
3.2. Factor Analysis of the DOS and EHQ Scales in a Lebanese Sample
3.3. Prevalence of ON: A Cross-Cultural Comparison
3.4. Correlates of ON: Cognitions, Behaviors, and Feelings Related to an Extreme Focus on Healthy Eating
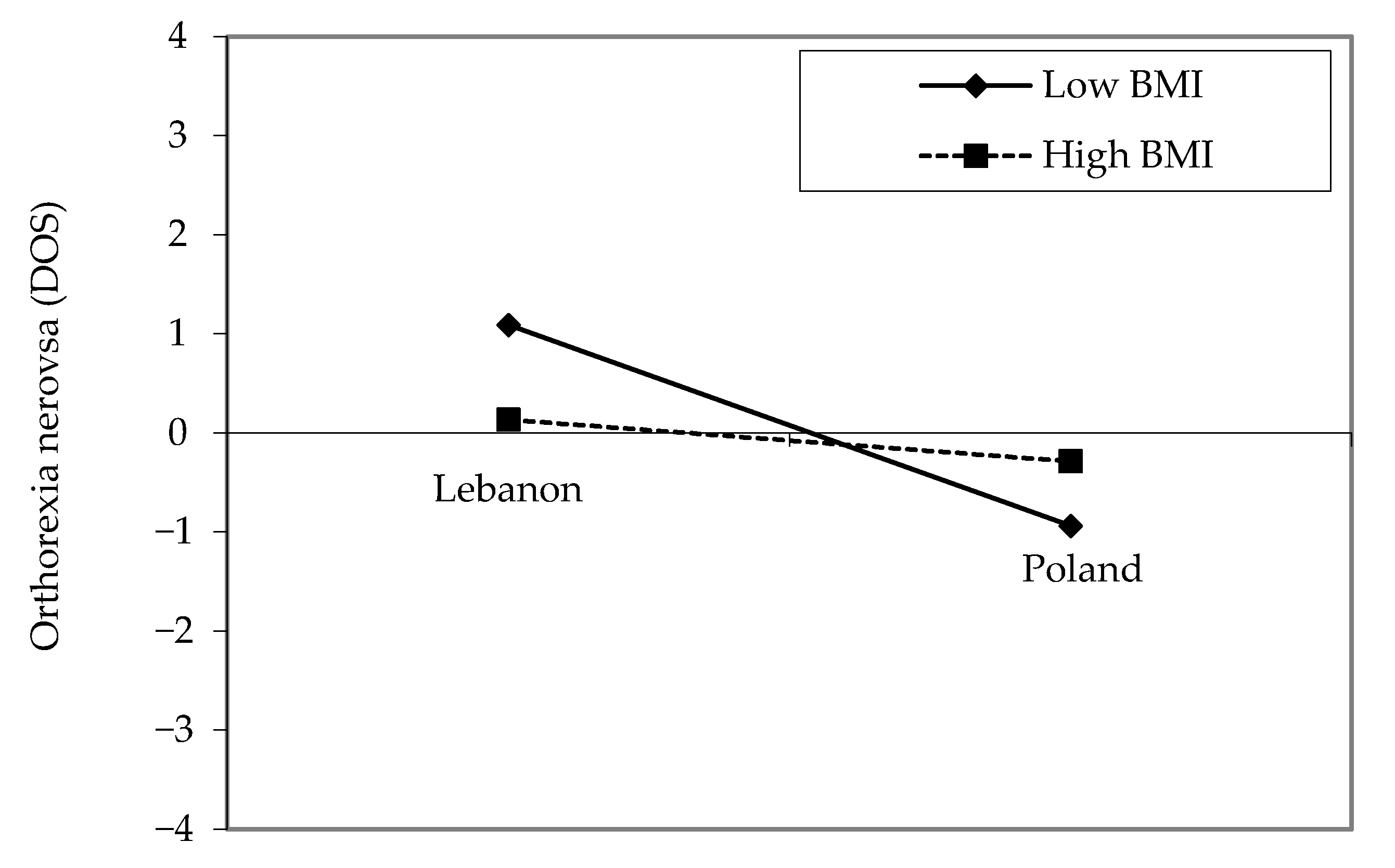
3.5. Correlates of ON: Sociodemographic Variables and Body Mass Index
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rangel, C.; Dukeshire, S.; MacDonald, L. Diet and anxiety. An exploration into the orthorexic society. Appetite 2012, 58, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Ambwani, S.; Shippe, M.; Gao, Z.; Austin, S.B. Is #cleaneating a healthy or harmful dietary strategy? Perceptions of clean eating and associations with disordered eating among young adults. J. Eat. Disord. 2019, 7, 17. [Google Scholar] [PubMed]
- Staudacher, H.M.; Harer, K.N. When clean eating goes dirty. Lancet Gastroenterol. Hepatol. 2018, 3, 668. [Google Scholar] [CrossRef]
- Bratman, S. Health food junkie. Yoga J. 1997, 136, 42–50. [Google Scholar]
- Bratman, S.; Knight, D. Health Food Junkies: Overcoming the Obsession with Healthful Eating; Broadway Books: New York, NY, USA, 2000. [Google Scholar]
- Cena, H.; Barthels, F.; Cuzzolaro, M.; Bratman, S.; Brytek-Matera, A.; Dunn, T.; Varga, M.; Missbach, B.; Donini, L.M. Definition and diagnostic criteria for orthorexia nervosa: A narrative review of the literature. Eat. Weight Disord. 2019, 24, 209–246. [Google Scholar] [CrossRef]
- Dunn, T.M.; Bratman, S. On orthorexia nervosa: A review of the literature and proposed diagnostic criteria. Eat. Behav. 2016, 21, 11–17. [Google Scholar] [CrossRef]
- Greville-Harris, M.; Smithson, J.; Karl, A. What are people’s experiences of orthorexia nervosa? A qualitative study of online blogs. Eat. Weight Disord. 2020, 25, 1693–1702. [Google Scholar] [CrossRef]
- Lopes, R.; Melo, R.; Dias Pereira, B. Orthorexia nervosa and comorbid depression successfully treated with mirtazapine: A case report. Eat. Weight Disord. 2020, 25, 163–167. [Google Scholar] [CrossRef]
- Strahler, J.; Hermann, A.; Walter, B.; Stark, R. Orthorexia nervosa: A behavioral complex or a psychological condition? J. Behav. Addict. 2018, 7, 1143–1156. [Google Scholar] [CrossRef]
- Plichta, M.; Jezewska-Zychowicz, M. Orthorexic tendency and eating disorders symptoms in Polish students: Examining differences in eating behaviors. Nutrients 2020, 12, 218. [Google Scholar] [CrossRef]
- Varga, M.; Dukay-Szabo, S.; Tury, F.; van Furth, E.F. Evidence and gaps in the literature on orthorexia nervosa. Eat. Weight Disord. 2013, 18, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Parra-Fernandez, M.L.; Onieva-Zafra, M.D.; Fernandez-Martinez, E.; Abreu-Sanchez, A.; Fernandez-Munoz, J.J. Assessing the prevalence of orthorexia nervosa in a sample of university students using two different self-report measures. Int. J. Environ. Res. Public Health 2019, 16, 2459. [Google Scholar] [CrossRef] [PubMed]
- Dunn, T.M.; Gibbs, J.; Whitney, N.; Starosta, A. Prevalence of orthorexia nervosa is less than 1 %: Data from a us sample. Eat. Weight Disord. 2017, 22, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Brytek-Matera, A. The Polish version of the Düsseldorf Orthorexia Scale (PL-DOS) and its comparison with English version of the DOS (E-DOS). Eat. Weight Disord. 2020. [Google Scholar] [CrossRef]
- Chard, C.A.; Hilzendegen, C.; Barthels, F.; Stroebele-Benschop, N. Psychometric evaluation of the English version of the Dusseldorf Orthorexie Scale (DOS) and the prevalence of orthorexia nervosa among a U.S. student sample. Eat. Weight Disord. 2019, 24, 275–281. [Google Scholar] [CrossRef]
- Zhou, X.; Schneider, S.C.; Cepeda, S.L.; Storch, E.A. Orthorexia nervosa in China: An exploration of phenomenology and clinical correlates among university students. J. Cogn Psychother 2020, 34, 225–241. [Google Scholar] [CrossRef]
- Parra-Fernandez, M.L.; Rodriguez-Cano, T.; Onieva-Zafra, M.D.; Perez-Haro, M.J.; Casero-Alonso, V.; Fernandez-Martinez, E.; Notario-Pacheco, B. Prevalence of orthorexia nervosa in university students and its relationship with psychopathological aspects of eating behaviour disorders. BMC Psychiatry 2018, 18, 364. [Google Scholar] [CrossRef]
- Asil, E.; Surucuoglu, M.S. Orthorexia nervosa in turkish dietitians. Ecol. Food Nutr. 2015, 54, 303–313. [Google Scholar] [CrossRef]
- Depa, J.; Schweizer, J.; Bekers, S.K.; Hilzendegen, C.; Stroebele-Benschop, N. Prevalence and predictors of orthorexia nervosa among german students using the 21-item-dos. Eat. Weight Disord. 2017, 22, 193–199. [Google Scholar] [CrossRef]
- Gramaglia, C.; Gambaro, E.; Delicato, C.; Marchetti, M.; Sarchiapone, M.; Ferrante, D.; Roncero, M.; Perpina, C.; Brytek-Matera, A.; Wojtyna, E.; et al. Orthorexia nervosa, eating patterns and personality traits: A cross-cultural comparison of Italian, Polish and Spanish university students. BMC Psychiatry 2019, 19, 235. [Google Scholar] [CrossRef]
- Cho, H.-B.; Hyun, M.-H. Orthorexia nervosa, fear of obesity. Stress 2020, 28, 68–75. [Google Scholar] [CrossRef]
- He, J.; Ma, H.; Barthels, F.; Fan, X. Psychometric properties of the Chinese version of the Dusseldorf Orthorexia Scale: Prevalence and demographic correlates of orthorexia nervosa among Chinese university students. Eat. Weight Disord. 2019, 24, 453–463. [Google Scholar] [CrossRef] [PubMed]
- Strahler, J.; Haddad, C.; Salameh, P.; Sacre, H.; Obeid, S.; Hallit, S. Cross-cultural differences in orthorexic eating behaviors: Associations with personality traits. Nutrition 2020, 77, 110811. [Google Scholar] [CrossRef] [PubMed]
- Farchakh, Y.; Hallit, S.; Soufia, M. Association between orthorexia nervosa, eating attitudes and anxiety among medical students in Lebanese universities: Results of a cross-sectional study. Eat. Weight Disord. 2019, 24, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Haddad, C.; Obeid, S.; Akel, M.; Honein, K.; Akiki, M.; Azar, J.; Hallit, S. Correlates of orthorexia nervosa among a representative sample of the Lebanese population. Eat. Weight Disord. 2019, 24, 481–493. [Google Scholar] [CrossRef]
- Depa, J.; Barrada, J.R.; Roncero, M. Are the motives for food choices different in orthorexia nervosa and healthy orthorexia? Nutrients 2019, 11, 697. [Google Scholar] [CrossRef]
- Barthels, F.; Barrada, J.R.; Roncero, M. Orthorexia nervosa and healthy orthorexia as new eating styles. PLoS ONE 2019, 14, e0219609. [Google Scholar] [CrossRef]
- McComb, S.E.; Mills, J.S. Orthorexia nervosa: A review of psychosocial risk factors. Appetite 2019, 140, 50–75. [Google Scholar] [CrossRef]
- Turner, P.G.; Lefevre, C.E. Instagram use is linked to increased symptoms of orthorexia nervosa. Eat. Weight Disord. 2017, 22, 277–284. [Google Scholar] [CrossRef]
- Missbach, B.; Hinterbuchinger, B.; Dreiseitl, V.; Zellhofer, S.; Kurz, C.; Konig, J. When eating right, is measured wrong! A validation and critical examination of the ORTO-15 questionnaire in German. PLoS ONE 2015, 10, e0135772. [Google Scholar] [CrossRef]
- Costa, C.B.; Hardan-Khalil, K. Orthorexia nervosa and obsessive-compulsive behavior among college students in the United States. J. Nurs. Educ. Pract. 2019, 9, 67–75. [Google Scholar] [CrossRef]
- Oberle, C.D.; Lipschuetz, S.L. Orthorexia symptoms correlate with perceived muscularity and body fat, not bmi. Eat. Weight Disord. 2018, 23, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Luck-Sikorski, C.; Jung, F.; Schlosser, K.; Riedel-Heller, S.G. Is orthorexic behavior common in the general public? A large representative study in Germany. Eat. Weight Disord. 2019, 24, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Oberle, C.D.; Samaghabadi, R.O.; Hughes, E.M. Orthorexia nervosa: Assessment and correlates with gender, bmi, and personality. Appetite 2017, 108, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Barrada, J.R.; Roncero, M. Bidimensional structure of the orthorexia: Development and initial validation of a new instrument. Anales De Psicología/Ann. Psychol. 2018, 34, 283–291. [Google Scholar] [CrossRef]
- Godefroy, V.; Trinchera, L.; Dorard, G. Optimizing the empirical assessment of orthorexia nervosa through EHQ and clarifying its relationship with BMI. Eat. Weight Disord. 2020. [Google Scholar] [CrossRef]
- Gramaglia, C.; Brytek-Matera, A.; Rogoza, R.; Zeppegno, P. Orthorexia and anorexia nervosa: Two distinct phenomena? A cross-cultural comparison of orthorexic behaviours in clinical and non-clinical samples. BMC Psychiatry 2017, 17, 75. [Google Scholar] [CrossRef]
- Barthels, F.; Meyer, F.; Pietrowsky, R. [Duesseldorf Orthorexia Scale–construction and evaluation of a questionnaire measuring orthorexic eating behavior]. Z. Klin. Psychol. Psychother. 2015, 44, 97–105. [Google Scholar] [CrossRef]
- Gleaves, D.H.; Graham, E.C.; Ambwani, S. Measuring “orthorexia”: Development of the Eating Habits Questionnaire. Int. J. Educ. Psychol. Assess. 2013, 12, 1–18. [Google Scholar]
- Brytek-Matera, A.; Plasonja, N.; Décamps, G. Assessing orthorexia nervosa: Validation of the Polish version of the Eating Habits Questionnaire in a general population sample. Nutrients 2020, 12, 3820. [Google Scholar] [CrossRef]
- World Health Organization. Body Mass Index—BMI. Available online: Https://www.Euro.Who.Int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 1 September 2020).
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences, 2nd ed.; L. Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Regional Strategy on Nutrition 2010–2019. Available online: Https://applications.Emro.Who.Int/docs/em_rc57_4_en.Pdf (accessed on 4 September 2020).
- Naja, F.; Jomaa, L.; Itani, L.; Zidek, J.; El Labban, S.; Sibai, A.M.; Hwalla, N. Environmental footprints of food consumption and dietary patterns among Lebanese adults: A cross-sectional study. Nutr. J. 2018, 17, 85. [Google Scholar] [CrossRef] [PubMed]
- Garduno, J.A.; Arevalo, A.; Garcia, J.J. Bond and small-molecule activation with low-valent nickel complexes. Dalton Trans. 2015, 44, 13419–13438. [Google Scholar] [CrossRef] [PubMed]
- Alkerwi, A.; Sauvageot, N.; Malan, L.; Shivappa, N.; Hebert, J.R. Association between nutritional awareness and diet quality: Evidence from the observation of cardiovascular risk factors in Luxembourg (ORISCAV-LUX) study. Nutrients 2015, 7, 2823–2838. [Google Scholar] [CrossRef]
- Bahn, R.A.; Nisr, R.; El Labban, S. Food policy in Lebanon. In Reference Module in Food Science; Elsevier: London, UK, 2018. [Google Scholar]
- Morinaka, T.; Wozniewicz, M.; Jeszka, J.; Bajerska, J.; Nowaczyk, P.; Sone, Y. Westernization of dietary patterns among young Japanese and Polish females—A comparison study. Ann. Agric. Environ. Med. 2013, 20, 122–130. [Google Scholar]
- Plichta, M.; Jezewska-Zychowicz, M.; Gębski, J. Orthorexic Tendency in Polish Students: Exploring Association with Dietary Patterns, Body Satisfaction and Weight. Nutrients 2019, 11, 100. [Google Scholar] [CrossRef]
- Naja, F.; Nasreddine, L.; Itani, L.; Chamieh, M.C.; Adra, N.; Sibai, A.M.; Hwalla, N. Dietary patterns and their association with obesity and sociodemographic factors in a national sample of Lebanese adults. Public Health Nutr. 2011, 14, 1570–1578. [Google Scholar] [CrossRef]
- Naja, F.; Nasreddine, L.; Itani, L.; Adra, N.; Sibai, A.M.; Hwalla, N. Association between dietary patterns and the risk of metabolic syndrome among Lebanese adults. Eur. J. Nutr. 2013, 52, 97–105. [Google Scholar] [CrossRef]
- Banna, J.C.; Gilliland, B.; Keefe, M.; Zheng, D. Cross-cultural comparison of perspectives on healthy eating among Chinese and American undergraduate students. BMC Public Health 2016, 16, 1015. [Google Scholar] [CrossRef]


{kind=link}
| Polish Adults (n = 743) | Lebanese Adults (n = 519) | Degree of Freedom | Pearson Chi-Square, p-Value | Effect Size | |
|---|---|---|---|---|---|
| Frequency (%) | Frequency (%) | ||||
| Sex | |||||
| Male | 172 (23.1%) | 222 (44.0%) | 60.27, p < 0.001 | VCramer 0.220 | |
| Female | 571 (76.9%) | 283 (56.0%) | |||
| Marital status | |||||
| Single | 653 (87.9%) | 264 (51.7%) | 202.16, p < 0.001 | VCramer 0.402 | |
| Married | 90 (12.1%) | 247 (48.3%) | |||
| Mean ± SD | Mean ± SD | Student’s t, p-value | |||
| Age (years) | 24.80 ± 6.76 | 35.83 ± 14.48 | 1255 | 18.10, p < 0.001 | Cohen’s d 0.976 |
| Body Mass Index (kg/m2) | 22.96 ± 3.66 | 24.45 ± 4.34 | 1214 | 6.42, p < 0.001 | Cohen’s d 0.371 |
| Factor Analysis of the DOS Items According to the Promax Rotation in Lebanon. | |||||
|---|---|---|---|---|---|
| Question | Item Number | Factor 1 | Factor 2 | h2 Communalities | Item-Factor Correlation * |
| I have the feeling of being excluded by my friends and colleagues due to my strict nutrition rules | 7 | 0.982 | 0.720 | 0.612 | |
| I try to avoid getting invited over to friends for dinner if I know that they do not pay attention to healthy nutrition | 4 | 0.825 | 0.586 | 0.646 | |
| My thoughts constantly revolve around healthy nutrition and I organize my day around it | 8 | 0.718 | 0.670 | 0.769 | |
| I find it difficult to go against my personal dietary rules | 9 | 0.686 | 0.634 | 0.734 | |
| If I eat something I consider unhealthy, I feel really bad | 6 | 0.613 | 0.633 | 0.768 | |
| I feel upset after eating unhealthy foods | 10 | 0.575 | 0.533 | 0.684 | |
| Eating healthy food is more important to me than indulgence/enjoying the food | 1 | 0.917 | 0.724 | 0.663 | |
| I have certain nutrition rules that I adhere to | 2 | 0.906 | 0.713 | 0.670 | |
| I can only enjoy eating foods considered healthy | 3 | 0.749 | 0.611 | 0.692 | |
| I like that I pay more attention to healthy nutrition than other people | 5 | 0.632 | 0.650 | 0.750 | |
| Percentage of variance explained | 64.74 | 51.91 | 12.83 | ||
| Cronbach’s alpha | 0.896 | 0.870 | 0.836 | ||
| Factor Analysis of the EHQ Items According to the Promax Rotation in Lebanon. | ||||||
|---|---|---|---|---|---|---|
| Question | Item Number | Factor 1 | Factor 2 | Factor 3 | h2 Communalities | Item-Factor Correlation * |
| I turn down social offers that involve eating unhealthy food. | 2 | 0.452 | 0.531 | 0.812 | ||
| I follow a diet with many rules. | 4 | 0.602 | 0.567 | 0.795 | ||
| I am distracted by thoughts of eating healthily. | 6 | 0.738 | 0.552 | 0.8001 | ||
| I only eat what my diet allows. | 7 | 0.722 | 0.571 | 0.838 | ||
| My healthy eating is a significant source of stress in my relationships. | 8 | 0.828 | 0.696 | 0.834 | ||
| My diet affects the type of employment I would take. | 10 | 0.782 | 0.642 | 0.813 | ||
| In the past year, friends or family members have told me that I’m overly concerned with eating healthily. | 13 | 0.705 | 0.557 | 0.866 | ||
| I have difficulty finding restaurants that serve the foods I eat. | 14 | 0.552 | 0.536 | 0.832 | ||
| Few foods are healthy for me to eat. | 16 | 0.466 | 0.720 | 0.773 | ||
| I go out less since I began eating healthily. | 17 | 0.677 | 0.545 | 0.846 | ||
| I spend more than three hours a day thinking about healthy food. | 18 | 0.737 | 0.585 | 0.844 | ||
| I follow a health-food diet rigidly. | 20 | 0.738 | 0.565 | 0.856 | ||
| I am more informed than others about healthy eating. | 1 | 0.775 | 0.603 | 0.698 | ||
| The way my food is prepared is important in my diet. | 3 | 0.799 | 0.656 | 0.702 | ||
| My eating habits are superior to others. | 5 | 0.658 | 0.599 | 0.787 | ||
| My diet is better than other people’s diets. | 11 | 0.751 | 0.595 | 0.832 | ||
| I prepare food in the most healthful way. | 21 | 0.668 | 0.516 | 0.764 | ||
| I have made efforts to eat more healthily over time. | 9 | 0.566 | 0.535 | 0.595 | ||
| I feel in control when I eat healthily. | 12 | 0.677 | 0.642 | 0.749 | ||
| Eating the way I do gives me a sense of satisfaction. | 15 | 0.707 | 0.617 | 0.629 | ||
| I feel great when I eat healthily. | 19 | 0.635 | 0.509 | 0.493 | ||
| Percentage of variance explained | 58.76 | 45.77 | 8.22 | 7.77 | ||
| Cronbach’s alpha | 0.969 | 0.969 | 0.893 | 0.807 | ||
| Variable | Polish Adults (n = 743,571 Women) | Lebanese Adults (n = 519,283 Women) |
|---|---|---|
| Düsseldorf Orthorexia Scale (DOS) M ± SD | 17.7 ± 5.1 f: 17.8 ± 4.8 m: 17.2 ± 6.0 | 20.0 ± 7.0 f: 20.4 ± 7.1 m: 19.6 ± 6.8 |
| DOS risk categories | ||
| Having ON (DOS ≥ 30) n, % within sex | f: 12 (2.1%) m: 7 (4.1%) | f: 26 (9.3%) m: 17 (7.7%) |
| At risk of developing ON (DOS 25–29) n, % within sex | f: 42 (7.4%) m: 10 (5.8%) | f: 55 (19.6%) m: 33 (15.0%) |
| Having no risk of ON (DOS ≤ 24) n, % within sex | f: 517 (90.5%) m: 155 (90.1%) | f: 200 (71.2%) m: 170 (77.3%) |
| Düsseldorf Orthorexia Scale (DOS) r, p | ||
|---|---|---|
| Polish Adults | Lebanese Adults | |
| Knowledge of healthy eating | 0.396, p < 0.001 | −0.635, p < 0.001 |
| Z, p | −20.38; p < 0.001 | |
| Problems associated with healthy eating | 0.493, p < 0.001 | −0.633, p < 0.001 |
| Z, p | −22.43; p < 0.001 | |
| Feeling positively about healthy eating | 0.325, p < 0.001 | −0.628, p < 0.001 |
| Z, p | −18.75; p < 0.001 | |
| F Value | p | Partial Eta Squared η2 | |
|---|---|---|---|
| Dependent variable: EHQ problems score | |||
| Country (Poland vs. Lebanon *) | 1766.35 | <0.001 | 0.598 |
| Sex (females vs. males *) | 0.334 | 0.563 | 0.00001 |
| Interaction sex-country | 2.501 | 0.114 | 0.002 |
| Dependent variable: EHQ knowledge score | |||
| Country (Poland vs. Lebanon *) | 543.36 | <0.001 | 0.314 |
| Sex (females vs. males *) | 0.573 | 0.449 | 0.00001 |
| Interaction sex-country | 15.00 | <0.001 | 0.012 |
| Dependent variable: EHQ feelings score | |||
| Country (Poland vs. Lebanon *) | 141.81 | <0.001 | 0.107 |
| Sex (females vs. males *) | 0.032 | 0.858 | 0.00001 |
| Interaction sex-country | 14.68 | <0.001 | 0.012 |
| DOS Sum Score | ||
|---|---|---|
| Polish Adults | Lebanese Adults | |
| Age | ||
| r, p | −0.030, 0.410 | 0.021, 0.638 |
| Z, p | 0.884, 0.188 | |
| Marital status | ||
| Single | 17.68 ± 5.13 | 20.35 ± 7.42 |
| Married | 17.43 ± 4.89 | 20.10 ± 6.51 |
| p marital status | 0.402 | |
| p country | <0.001 | |
| p country * marital status | 0.991 | |
| BMI categories | ||
| Underweight | 16.33 ± 8.47 | 17.76 ± 8.43 |
| Normal weight | 17.56 ± 5.01 | 21.11 ± 7.35 |
| Overweight | 17.89 ± 5.54 | 19.74 ± 6.16 |
| Obesity | 18.36 ± 4.55 | 17.86 ± 6.11 |
| p BMI category | 0.112 | |
| p country | 0.045 | |
| p country * BMI category | 0.008 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brytek-Matera, A.; Sacre, H.; Staniszewska, A.; Hallit, S. The Prevalence of Orthorexia Nervosa in Polish and Lebanese Adults and Its Relationship with Sociodemographic Variables and BMI Ranges: A Cross-Cultural Perspective. Nutrients 2020, 12, 3865. https://doi.org/10.3390/nu12123865
Brytek-Matera A, Sacre H, Staniszewska A, Hallit S. The Prevalence of Orthorexia Nervosa in Polish and Lebanese Adults and Its Relationship with Sociodemographic Variables and BMI Ranges: A Cross-Cultural Perspective. Nutrients. 2020; 12(12):3865. https://doi.org/10.3390/nu12123865
Chicago/Turabian StyleBrytek-Matera, Anna, Hala Sacre, Anna Staniszewska, and Souheil Hallit. 2020. "The Prevalence of Orthorexia Nervosa in Polish and Lebanese Adults and Its Relationship with Sociodemographic Variables and BMI Ranges: A Cross-Cultural Perspective" Nutrients 12, no. 12: 3865. https://doi.org/10.3390/nu12123865
APA StyleBrytek-Matera, A., Sacre, H., Staniszewska, A., & Hallit, S. (2020). The Prevalence of Orthorexia Nervosa in Polish and Lebanese Adults and Its Relationship with Sociodemographic Variables and BMI Ranges: A Cross-Cultural Perspective. Nutrients, 12(12), 3865. https://doi.org/10.3390/nu12123865