Wasted Children and Wasted Time: A Challenge to Meeting the Nutrition Sustainable Development Goals with a High Economic Impact to Ethiopia

Abstract
:1. Introduction
2. Materials and Methods
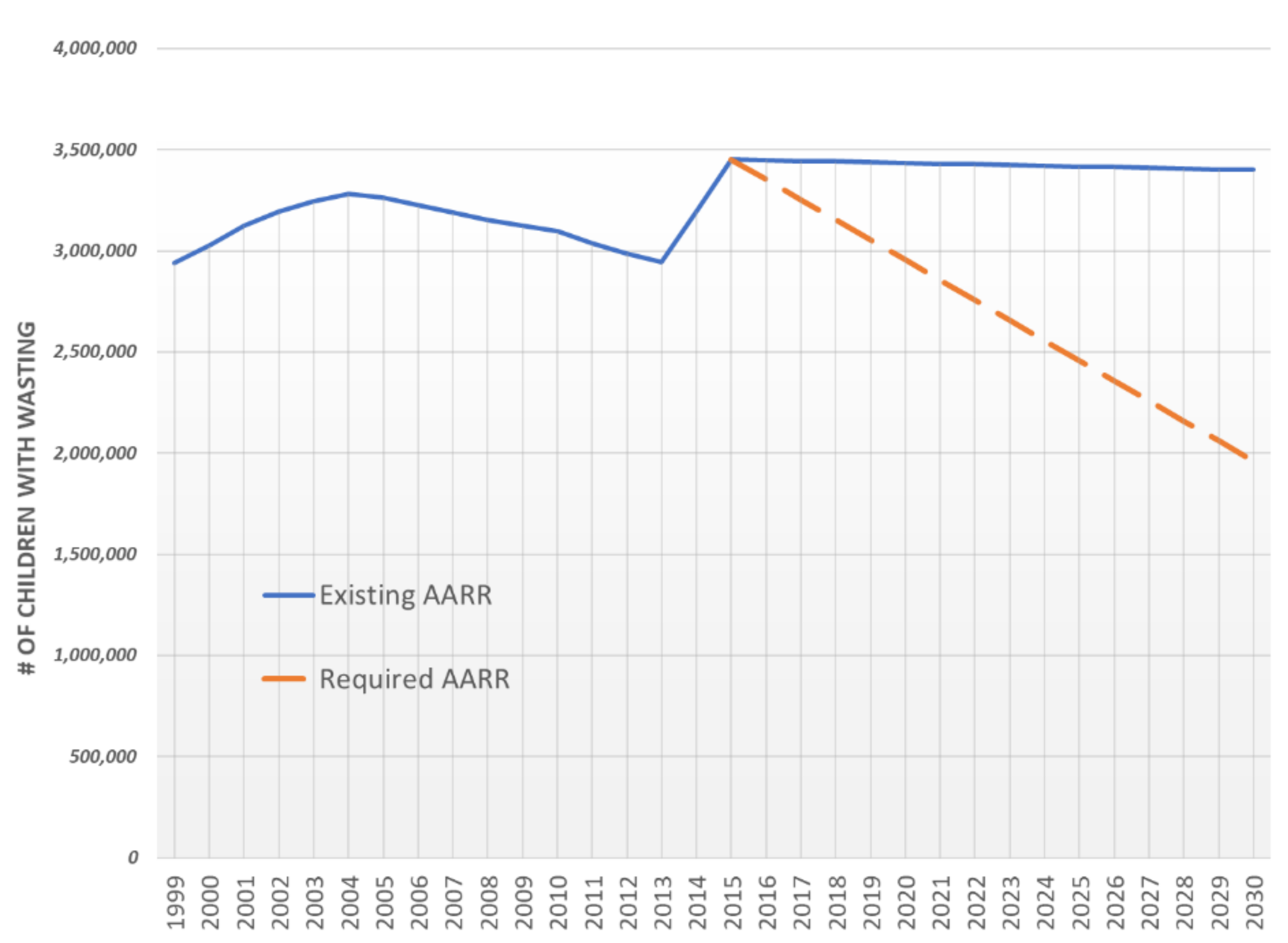
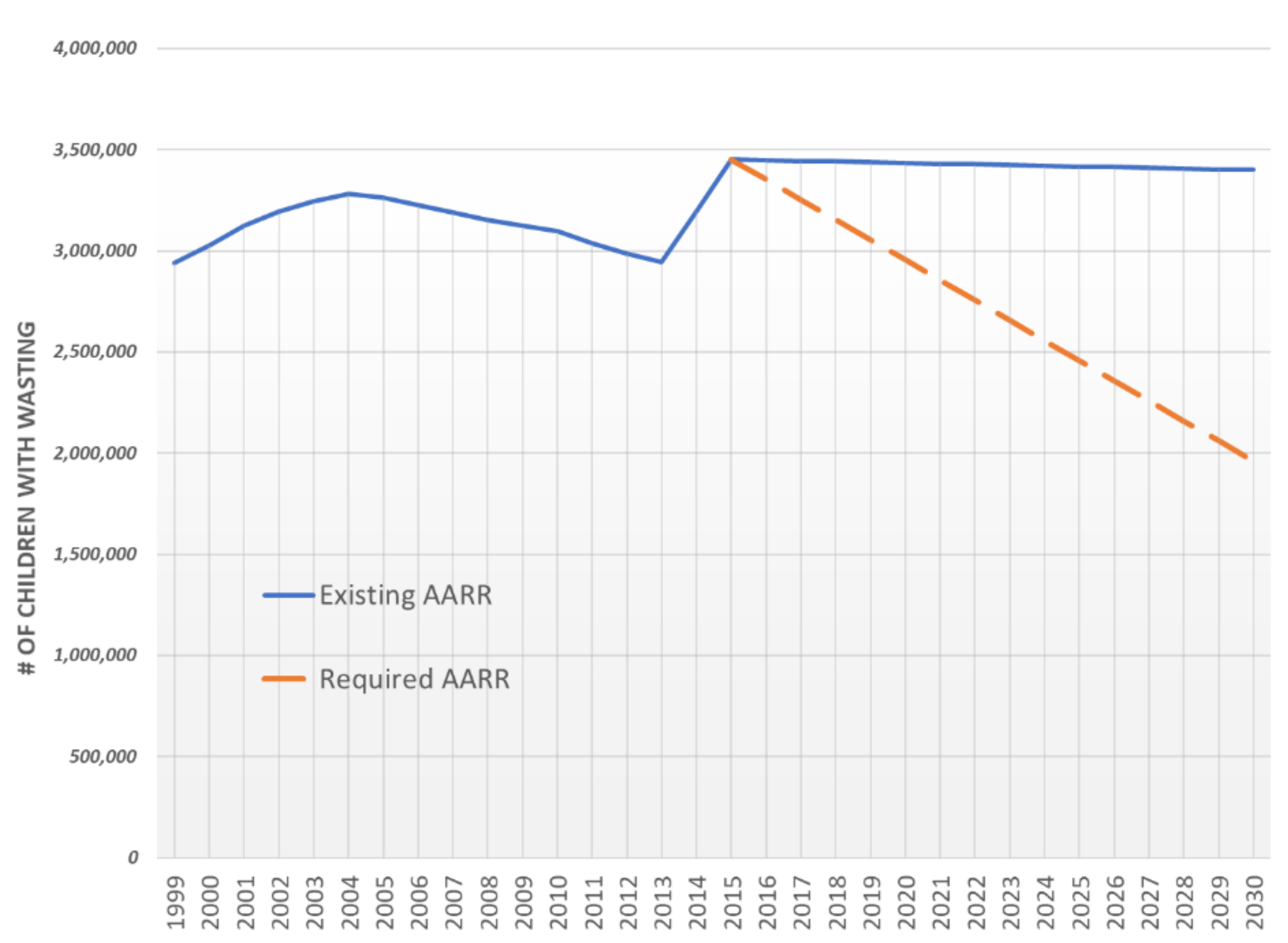
2.1. Annual Average Rate of Reduction Calculation
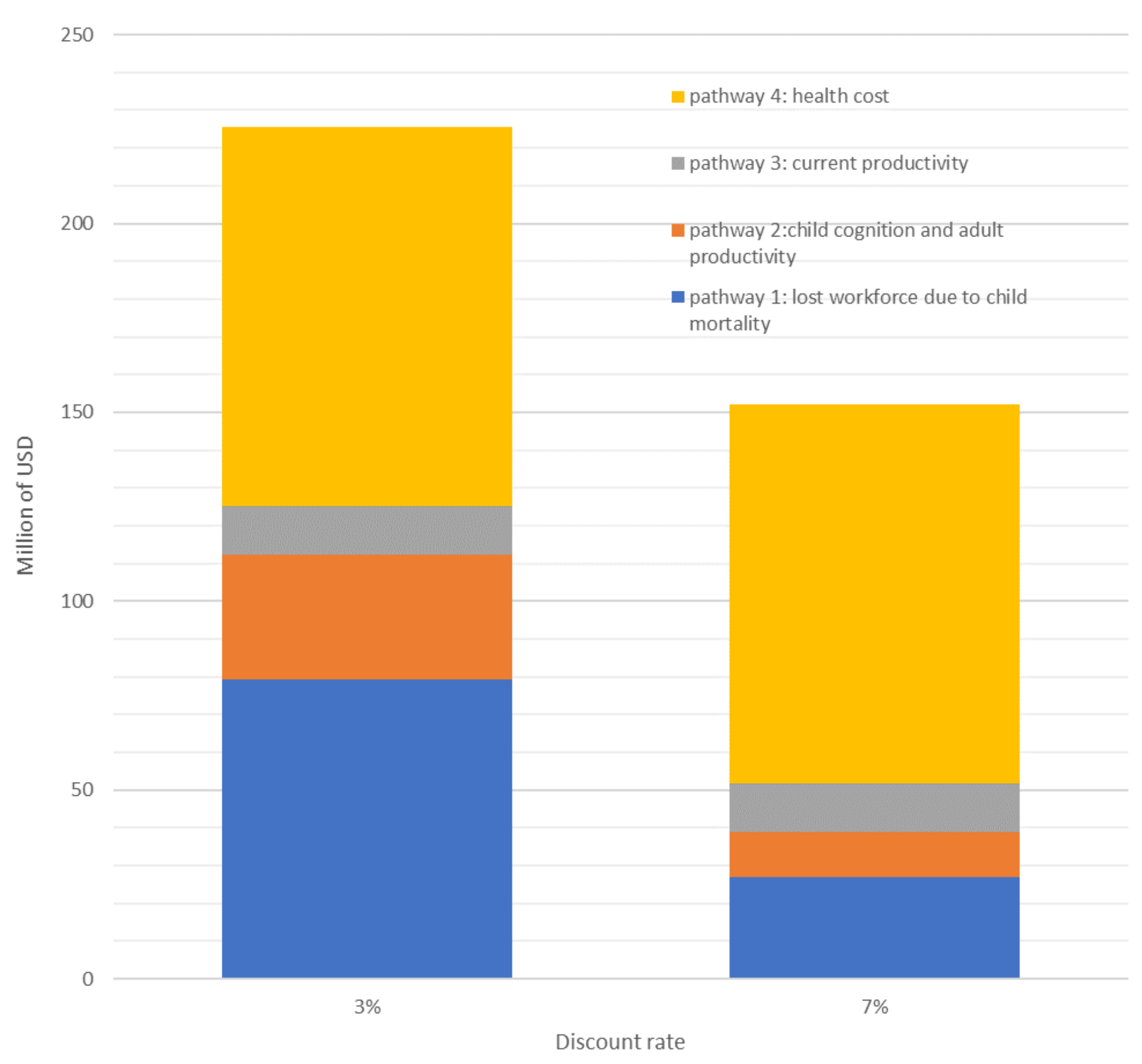
2.2. Consequence Model: Economic Burden of Wasting in 2019
2.2.1. Pathway 1: Child Mortality Attributable to Malnutrition, and Estimated Value of Workforce Lost to Child Mortality
- Population attributable risk: The population attributable risk (PAR) is a function of the prevalence of the nutrition indicator along with the severity of the mortality risk, as expressed by the relative risk (RR: see Table 1). It is calculated with the following formula: (Prevalence × (RR − 1))/(1 + (Prevalence × (RR − 1))).
- Mortality in risk group affected: number of deaths per year based on national data
- Labor force participation: All: 91.2%, Male: 88.4%, and Female: 73.4% [20]
- Average earnings: 790/year USD, based on World Bank estimates
- Net present value: Net present value (NPV) is a subjective factor used to define the value of future goods or services and expresses that value in current currency. To calculate this NPV of lost future earnings due to the various indicators of malnutrition, we used a 3% discount rate, recommended by the World Bank for social investments [21]. As a sensitivity parameter, a 7% discount rate was also used, as recommended by other organizations [22].
2.2.2. Pathway 2: Child Cognition Deficit Resulting in Inferior School Performance and Adult Productivity
2.2.3. Pathway 3: Current Value of Reduced Productivity in Working Adults
2.2.4. Pathway 4: Current Value of Preventable Treatment Cost
- 10% of the SAM children will go through a stabilization center (UNICEF Ethiopia estimates)
- Cost, including supply, training, and monitoring: 40.27 USD/child for moderately wasted children (MAM), 80 USD/child for a severely wasted child (SAM) in out-patient treatment (OPT), 120 USD/child for a SAM in a stabilization center (SC) and then OPT
- Cost of labor: to estimate the cost of the health extension worker (HEW) during the following visits, we have estimated that he works 196 h/month and receives a salary of 150 USD/month. Therefore, his cost per hour of work is equal to 0.76 USD. A similar calculation was done for a health worker (HW) who works 196 h/month and receives a salary of 198 USD/month. His cost per hour will be equal to 1.01 USD. If we consider that each contact with a wasted child is 20 min, a MAM child with eight visits will cost 1.8 USD, a SAM child (OTP) with 12 visits will each cost 2.7 USD, while a SAM child (SC+OTP) with 19 visits will costs 4.9 USD.
2.3. Calculation of Averted SAM Cases and Potential Economic Saving Model over theYear
2.3.1. Averted SAM Cases
2.3.2. Potential Economic Saving Model over the Year
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Black, R.E.; Allen, L.H.; Bhutta, Z. Maternal and child undernutrition: Global and regional exposures and health consequences. Lancet 2008, 371, 243–260. [Google Scholar] [CrossRef]
- Olofin, I.; McDonald, C.M.; Ezzati, M.; Flaxman, S.; Black, R.E.; Fawzi, W.W.; Caulfield, L.E.; Danaei, G. Associations of suboptimal growth with all-cause and cause-specific mortality in children under five years: A pooled analysis of ten prospective studies. PLoS ONE 2013, 8, e64636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Central Statistical Agency (CSA). Ethiopia Demographic and Health Survey 2000; Central Statistical Authority: Addis Ababa, Ethiopia; ORC Macro: Calverton, MD, USA, 2001.
- Ethiopian Public Health Institute (EPHI); ICF. Ethiopia Mini Demographic and Health Survey 2019; Ministry of Health Addis Ababa: Addis Ababa, Ethiopia; The DHS Program ICF: Rockville, MD, USA, 2019. [CrossRef]
- Central Statistical Agency; ORC Macro. Ethiopia Demographic and Health Survey 2005; Central Statistical Agency: Addis Ababa, Ethiopia; ORC Macro: Calverton, MD, USA, 2006.
- EDHS 2016 Team. Ethiopian Demographic and Health Survey; Report; Central Statistical Agency: Addis Ababa, Ethiopia; The DHS Program ICF: Rockville, MD, USA, 2016.
- Garzón, C.; Kiess, L.; Lutter, C.; Cuadrado, C. The Cost of the Double Burden of Malnutrition: Social and Economic Impact; Ministry Educ. Public Heal; Economic Commission for Latin America and the Caribbean: Santiago, Chile, 2017.
- Dione, J.; Omamo, S.W.; Diop, A.; Kaloko, M.S. The Cost of Hunger in Ethiopia. Implications for the Growth and Transformation of Ethiopia. The Social and Economic Impact of Child Undernutrition in Ethiopia; Summary Report; World Food Programme: Addis Ababa, Ethiopia, 2013.
- Hoddinott, J. The Economics of Reducing Malnutrition in Sub-Saharan Africa. 2016. Available online: http://glopan.org/invest-in-nutrition (accessed on 12 November 2020).
- Beddington, J.; Kufuor, J. The Cost of Malnutrition: Why Policy Action Is Urgent; Technical Brief No. 3; Global Panel on Agriculture and Food Systems for Nutrition: London, UK, 2016. [Google Scholar]
- Hoddinott, J. The economic cost of malnutrition. In The Road to Good Nutrition; Karger Publishers: Basel, Switzerland, 2013. [Google Scholar]
- Measure Evaluation. Ethiopia Demographic and Health Survey, 2010; Central Statistical Agency: Addis Ababa, Ethiopia; Measure DHS, ICF Macro: Calverton, MD, USA, 2011.
- UNICEF. Technical Note How to calculate Average Annual Rate of Reduction (AARR) of Underweight Prevalence 2007. Available online: File:///C:/Users/alaillou/Downloads/Technical_Note_AARR_185.pdf (accessed on 12 November 2020).
- Moench-Pfanner, R.; Silo, S.; Laillou, A.; Wieringa, F.; Hong, R.; Hong, R.; Poirot, E.; Bagriansky, J. The economic burden of malnutrition in pregnant women and children under 5 years of age in Cambodia. Nutrients 2016, 8, 292. [Google Scholar] [CrossRef] [PubMed]
- Bagriansky, J.; Champa, N.; Pak, K.; Whitney, S.; Laillou, A. The economic consequences of malnutrition in Cambodia, more than 400 million US dollar lost annually. Asia Pac. J. Clin. Nutr. 2014, 23, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Bagriansky, J. The Economic Consequences of Malnutrition in Albania; MDGF/UN: Tirana, Albania, 2010. Available online: http://www.mdgfund.org/sites/default/files/Cost%20benefit%20analysis.pdf (accessed on 12 November 2020).
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; De Onis, M.; Uauy, R.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- WHO. Global Health Observatory Data Repository—Child Mortality by Cause, by Country, 2000–2010; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Moench-Pfanner, R.; Laillou, A.; Berger, J. Introduction: Large-scale fortification, an important nutrition-specific intervention. Food Nutr. Bull. 2012, 33 (Suppl. 4), S255–S259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- 2020. Available online: https://data.worldbank.org/indicator/SL.TLF.CACT.NE.ZS?locations=ET (accessed on 5 October 2020).
- Lea, R.A. World development report 1993: Investing in health. Forum Dev. Stud. 1993, 20, 114–117. [Google Scholar] [CrossRef]
- Arrow, K.; Cropper, M.; Gollier, C.; Groom, B.; Heal, G.; Newell, R.; Sterner, T.; Nordhaus, W.; Pindyck, R.; Pizer, W.; et al. Determining benefits and costs for future generations. Science 2013, 341, 349–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grantham-McGregor, S.; Cheung, Y.B.; Cueto, S.; Glewwe, P.; Richter, L.; Strupp, B. Developmental potential in the first 5 years for children in developing countries. Lancet 2007, 369, 60–70. [Google Scholar] [CrossRef] [Green Version]
- Haddad, L.J.; Bouis, H.E. The impact of nutritional status on agriculture productivity: Wage evidence from the Philippines. Oxf. Bull. Econ. Stat. 1991, 53, 45–68. [Google Scholar] [CrossRef]
- Khara, T.; Mwangome, M.; Ngari, M.; Dolan, C. Children concurrently wasted and stunted: A meta-analysis of prevalence data of children 6–59 months from 84 countries. Matern. Child Nutr. 2018, 14, e12515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tekeste, A.; Wondafrash, M.; Azene, G.; Deribe, K. Cost effectiveness of community-based and in-patient therapeutic feeding programs to treat severe acute malnutrition in Ethiopia. Cost Eff. Resour. Alloc. 2012, 10, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baye, K.; Hirvonen, K. Seasonality: A missing link in preventing undernutrition. Lancet Child Adolesc. Health 2020, 4, e3. [Google Scholar] [CrossRef]
- Stobaugh, H.C.; Mayberry, A.; McGrath, M.; Bahwere, P.; Zagre, N.M.; Manary, M.J.; Black, R.; Lelijveld, N. Relapse after severe acute malnutrition: A systematic literature review and secondary data analysis. Matern. Child Nutr. 2019, 12, 452–462. [Google Scholar] [CrossRef] [PubMed]
- Mertens, A.; Benjamin-Chung, J.; Colford, J.M.; Hubbard, A.E.; van der Laan, M.; Coyle, J.; Cai, W.; Jilek, W.; Dayal, S.; Nguyen, A.; et al. Child wasting and concurrent stunting in low—And middle-income countries. medRxiv 2020. [Google Scholar] [CrossRef]
- Stobaugh, H.C.; Rogers, B.L.; Rosenberg, I.H.; Webb, P.; Maleta, K.M.; Manary, M.J.; Trehan, I. Children with poor linear growth are at risk for repeated relapse to wasting after recovery from moderate acute malnutrition. J. Nutr. 2018, 133, 4021S–4026S. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Diseases Topic | RR |
|---|---|
| Pneumonia among children with anthropometric indicator zscore < −3SD | 9.7 |
| Pneumonia among children with anthropometric indicator −3SD < zscore < −2SD | 4.7 |
| Pneumonia among children with anthropometric indicator −2SD < zscore < −1SD | 1.9 |
| Diarrhea among children with anthropometric indicator zscore < −3SD | 12.3 |
| Diarrhea among children with anthropometric indicator −3SD < zscore < −2SD | 3.4 |
| Diarrhea among children with anthropometric indicator −2SD < zscore < −1SD | 1.6 |
| Measles among children with anthropometric indicator zscore < −3SD | 9.6 |
| Measles among children with anthropometric indicator −3SD < zscore < −2SD | 2.6 |
| Measles among children with anthropometric indicator −2SD < zscore < −1SD | 1 |
| Other among children with anthropometric indicator zscore < −3SD | 11.2 |
| Other among children with anthropometric indicator −3SD < zscore < −2SD | 2.7 |
| Other among children with anthropometric indicator −2SD < zscore <−1SD | 1.7 |
| Wasting Target (Prevalence in % by 2030) | Estimated AARR Required * | Number of Moderately Wasted Children (MAM) Adverted Cases | Number of Severe Acute Malnutrition (SAM) Averted Cases |
|---|---|---|---|
| ≤5% (SDG target) | 5.4% | 5.5 million | 2.4 million |
| 5–6% | 3.7% | 4.0 million | 1.7 million |
| 7% | 2.2% | 2.5 million | 1.1 million |
| 8% | 0.9% | 1 million | 0.43 million |
| Annual Average Rate of Reduction (AARR) | Pathway 1: Lost Workforce due to Child Mortality * | Pathway 2: Child Cognition and Adult Productivity * | Pathway 3: Current Productivity ** | Pathway 4: Health Cost ** | Total Capital Saved in Million USD | |
|---|---|---|---|---|---|---|
| 3% discount rate | 5.40% | 88.7 | 79.2 | 82.2 | 439.8 | 689.9 |
| 3.70% | 66.4 | 79.2 | 59.7 | 319.6 | 524.9 | |
| 2.20% | 45.4 | 79.2 | 37.3 | 199.7 | 361.6 | |
| 0.90% | 25.4 | 79.2 | 14.9 | 79.7 | 199.2 | |
| 7% discount rate | 5.40% | 55.2 | 17.02 | 82.2 | 439.8 | 594.22 |
| 3.70% | 47 | 17.02 | 59.7 | 319.6 | 443.32 | |
| 2.20% | 40.2 | 17.02 | 37.3 | 199.7 | 294.22 | |
| 0.90% | 33.5 | 17.02 | 14.9 | 79.7 | 145.12 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laillou, A.; Baye, K.; Meseret, Z.; Darsene, H.; Rashid, A.; Chitekwe, S. Wasted Children and Wasted Time: A Challenge to Meeting the Nutrition Sustainable Development Goals with a High Economic Impact to Ethiopia. Nutrients 2020, 12, 3698. https://doi.org/10.3390/nu12123698
Laillou A, Baye K, Meseret Z, Darsene H, Rashid A, Chitekwe S. Wasted Children and Wasted Time: A Challenge to Meeting the Nutrition Sustainable Development Goals with a High Economic Impact to Ethiopia. Nutrients. 2020; 12(12):3698. https://doi.org/10.3390/nu12123698
Chicago/Turabian StyleLaillou, Arnaud, Kaleab Baye, Zelalem Meseret, Hiwot Darsene, Abdulai Rashid, and Stanley Chitekwe. 2020. "Wasted Children and Wasted Time: A Challenge to Meeting the Nutrition Sustainable Development Goals with a High Economic Impact to Ethiopia" Nutrients 12, no. 12: 3698. https://doi.org/10.3390/nu12123698
APA StyleLaillou, A., Baye, K., Meseret, Z., Darsene, H., Rashid, A., & Chitekwe, S. (2020). Wasted Children and Wasted Time: A Challenge to Meeting the Nutrition Sustainable Development Goals with a High Economic Impact to Ethiopia. Nutrients, 12(12), 3698. https://doi.org/10.3390/nu12123698