Association of the Modified Mediterranean Diet Score (mMDS) with Anthropometric and Biochemical Indices in US Career Firefighters

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Dietary Assessment
2.3. Physical Activity
2.4. Outcome Assessments
2.5. Covariate Assessment
2.6. Statistical Analysis
2.7. Ethics Statement
3. Results
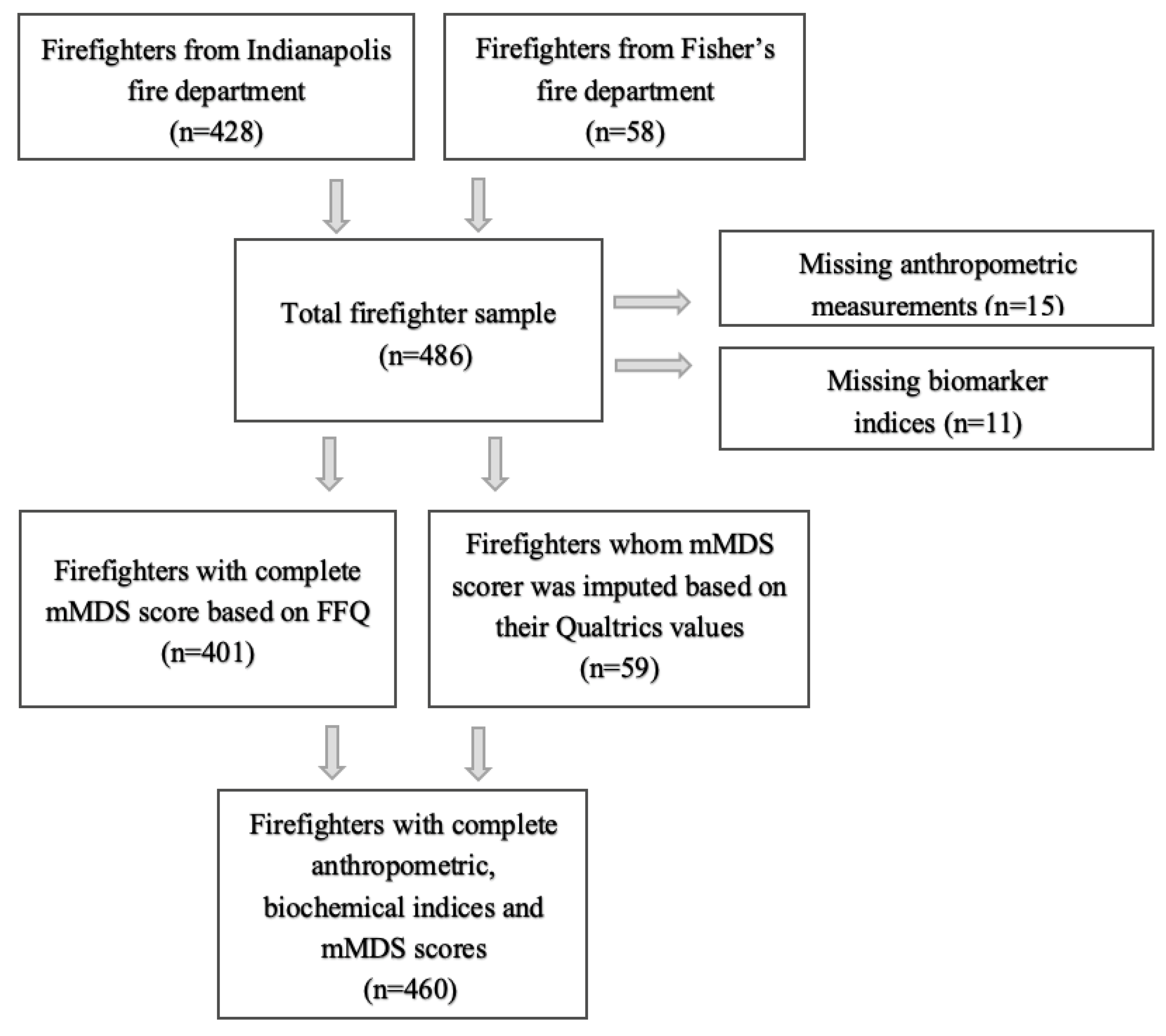
3.1. Sampling Procedure and Outcome
3.2. General Characteristics of the Firefighters
3.3. Association of the Modified Mediterranean Diet Score with Anthropometric and Biochemical Indices
3.4. Effects of a Unitary Increase in the Modified Mediteranean Score on Anthropometric Measures, Blood Pressure, and Biochemical Indices
3.5. Effects of Single Components of the Modified Mediteranean Score on Anthropometric Measures, Blood Pressure, and Biochemical Indices
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Total Cholesterol-HDL Ratio > 6 | Triglycerides ≥ 150 mg/dL | Glucose ≥ 100 mg/dL | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No (N = 374) | Yes (N = 27) | p Value | No (N = 300) | Yes (N = 100) | p Value | No (N = 243) | Yes (N = 158) | p Value | |||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||||
| Total mMDS | 22.23 | 6.80 | 18.19 | 6.63 | 0.003 | 22.47 | 6.80 | 20.44 | 6.86 | 0.010 | 22.12 | 6.67 | 21.70 | 7.15 | 0.549 |
| Single item mMDS | |||||||||||||||
| Fast food consumption * | 1.57 | 0.95 | 1.00 | 0.83 | 0.003 | 1.66 | 0.93 | 1.14 | 0.92 | <.001 | 1.51 | 0.97 | 1.56 | 0.93 | 0.634 |
| Fruit consumption | 1.57 | 0.90 | 1.22 | 0.70 | 0.049 | 1.58 | 0.91 | 1.44 | 0.82 | 0.163 | 1.58 | 0.94 | 1.49 | 0.80 | 0.270 |
| Vegetable consumption | 2.56 | 1.06 | 2.44 | 0.93 | 0.586 | 2.53 | 1.05 | 2.63 | 1.08 | 0.396 | 2.56 | 1.07 | 2.54 | 1.03 | 0.841 |
| Sweet desserts consumption | 1.85 | 1.57 | 0.96 | 1.22 | 0.004 | 1.93 | 1.57 | 1.37 | 1.50 | 0.002 | 1.76 | 1.57 | 1.84 | 1.56 | 0.625 |
| Cooking oil or fat use at home | 2.12 | 1.85 | 1.63 | 1.74 | 0.185 | 2.12 | 1.86 | 1.99 | 1.84 | 0.554 | 2.22 | 1.83 | 1.88 | 1.86 | 0.073 |
| Fried food consumption | 1.56 | 1.18 | 0.89 | 0.93 | 0.004 | 1.58 | 1.19 | 1.30 | 1.10 | 0.037 | 1.47 | 1.18 | 1.58 | 1.17 | 0.374 |
| Breads or starches consumed at home | 1.75 | 1.48 | 1.67 | 1.52 | 0.782 | 1.82 | 1.47 | 1.50 | 1.51 | 0.062 | 1.73 | 1.49 | 1.77 | 1.48 | 0.805 |
| Ocean fish consumption | 1.64 | 1.14 | 1.70 | 0.99 | 0.765 | 1.67 | 1.13 | 1.57 | 1.12 | 0.459 | 1.66 | 1.07 | 1.61 | 1.21 | 0.700 |
| Non-alcoholic beverages at home | 2.66 | 1.13 | 2.44 | 1.37 | 0.339 | 2.69 | 1.14 | 2.50 | 1.17 | 0.144 | 2.74 | 1.12 | 2.50 | 1.18 | 0.036 |
| Alcoholic beverages | 2.09 | 1.57 | 1.78 | 1.48 | 0.317 | 2.02 | 1.60 | 2.24 | 1.44 | 0.224 | 2.03 | 1.59 | 2.13 | 1.54 | 0.516 |
| Wine consumption | 0.81 | 0.98 | 0.89 | 1.01 | 0.679 | 0.81 | 0.98 | 0.82 | 0.99 | 0.953 | 0.83 | 0.99 | 0.78 | 0.98 | 0.645 |
| Legumes consumption | 0.67 | 1.26 | 0.74 | 1.29 | 0.791 | 0.66 | 1.26 | 0.74 | 1.29 | 0.585 | 0.71 | 1.29 | 0.63 | 1.23 | 0.510 |
| Nuts consumption | 1.39 | 1.62 | 0.81 | 1.44 | 0.073 | 1.40 | 1.62 | 1.20 | 1.61 | 0.277 | 1.32 | 1.59 | 1.41 | 1.66 | 0.612 |
References
- Soares, E.M.K.V.K.; Smith, D.; Porto, L.G.G. Worldwide prevalence of obesity among firefighters: A systematic review protocol. BMJ Open 2020, 10, e031282. [Google Scholar] [CrossRef] [PubMed]
- Tsismenakis, A.J.; Christophi, C.A.; Burress, J.W.; Kinney, A.M.; Kim, M.; Kales, S.N. The obesity epidemic and future emergency responders. Obesity 2009, 17, 1648–1650. [Google Scholar] [CrossRef] [PubMed]
- Lavie, C.J.; Milani, R.V.; Ventura, H.O. Obesity and cardiovascular disease. risk factor, paradox, and impact of weight loss. J. Am. Coll. Cardiol. 2009, 53, 1925–1932. [Google Scholar] [CrossRef] [PubMed]
- Dunlay, S.M.; Givertz, M.M.; Aguilar, D.; Allen, L.A.; Chan, M.; Desai, A.S.; Deswal, A.; Dickson, V.V.; Kosiborod, M.N.; Lekavich, C.L.; et al. Type 2 diabetes mellitus and heart failure, a scientific statement from the American Heart Association and Heart Failure Society of America. J. Card. Fail. 2019, 25, 584–619. [Google Scholar] [CrossRef] [PubMed]
- Donovan, R.; Nelson, T.; Peel, J.; Lipsey, T.; Voyles, W.; Israel, R.G. Cardiorespiratory fitness and the metabolic syndrome in firefighters. Occup. Med. 2009, 59, 487–492. [Google Scholar] [CrossRef]
- Soteriades, E.S.; Hauser, R.; Kawachi, I.; Liarokapis, D.; Christiani, D.C.; Kales, S.N. Obesity and cardiovascular disease risk factors in firefighters: A prospective cohort study. Obes. Res. 2005, 13, 1756–1763. [Google Scholar] [CrossRef]
- Navarro, K.M.; Kleinman, M.T.; Mackay, C.E.; Reinhardt, T.E.; Balmes, J.R.; Broyles, G.A.; Ottmar, R.D.; Naher, L.P.; Domitrovich, J.W. Wildland firefighter smoke exposure and risk of lung cancer and cardiovascular disease mortality. Environ. Res. 2019, 173, 462–468. [Google Scholar] [CrossRef]
- Kales, S.; Smith, D.L. Firefighting and the heart. Circulation 2017, 135, 1296–1299. [Google Scholar] [CrossRef]
- Smith, D.L.; Haller, J.M.; Korre, M.; Fehling, P.C.; Sampani, K.; Porto, L.G.G.; Christophi, C.A.; Kales, S.N. Pathoanatomic findings associated with duty-related cardiac death in US firefighters: A case-control study. J. Am. Heart Assoc. 2018, 7, e009446. [Google Scholar] [CrossRef]
- Smith, D.L.; Haller, J.M.; Korre, M.; Sampani, K.; Porto, L.G.G.; Fehling, P.C.; Christophi, C.A.; Kales, S.N. The relation of emergency duties to cardiac death among US firefighters. Am. J. Cardiol. 2019, 123, 736–741. [Google Scholar] [CrossRef]
- Kahn, S.A.; Leonard, C.; Siordia, C. Firefighter fatalities: Crude mortality rates and risk factors for line of duty injury and death. J. Burn Care Res. 2018, 40, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Deming, N.J.; Moore, K.; Alam, T. Cardiorespiratory fitness decline in aging firefighters. Am. J. Public Health 2020, 110, E1. [Google Scholar] [CrossRef] [PubMed]
- Neovius, M.; Kark, M.; Rasmussen, F. Association between obesity status in young adulthood and disability pension. Int. J. Obes. 2008, 32, 1319–1326. [Google Scholar] [CrossRef] [PubMed]
- Linde, J.A.; Andrade, K.; MacLehose, R.F.; Mitchell, N.R.; Harnack, L.; Cousins, J.M.; Graham, D.J.; Jeffery, R.W. HealthWorks: Results of a multi-component group-randomized worksite environmental intervention trial for weight gain prevention. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 14. [Google Scholar] [CrossRef]
- Baur, D.M.; Christophi, C.A.; Cook, E.F.; Kales, S. Age-Related decline in cardiorespiratory fitness among career firefighters: Modification by physical activity and adiposity. J. Obes. 2012, 2012, 1–6. [Google Scholar] [CrossRef]
- Eleftheriou, D.; Benetou, V.; Trichopoulou, A.; La Vecchia, C.; Bamia, C. Mediterranean diet and its components in relation to all-cause mortality: Meta-analysis. Br. J. Nutr. 2018, 120, 1081–1097. [Google Scholar] [CrossRef]
- Barbagallo, M.; Barbagallo, M. Mediterranean diet and longevity. Eur. J. Cancer Prev. 2004, 13, 453–456. [Google Scholar] [CrossRef]
- Bo, S.; Ponzo, V.; Goitre, I.; Fadda, M.; Pezzana, A.; Beccuti, G.; Gambino, R.; Cassader, M.; Soldati, L.; Broglio, F. Predictive role of the Mediterranean diet on mortality in individuals at low cardiovascular risk: A 12-year follow-up population-based cohort study. J. Transl. Med. 2016, 14, 91. [Google Scholar] [CrossRef]
- Korre, M.; Tsoukas, M.A.; Frantzeskou, E.; Yang, J.; Kales, S. Mediterranean diet and workplace health promotion. Curr. Cardiovasc. Risk Rep. 2014, 8, 1–7. [Google Scholar] [CrossRef]
- Nissensohn, M.; Román-Viñas, B.; Sánchez-Villegas, A.; Piscopo, S.; Serra-Majem, L. The Effect of the Mediterranean diet on hypertension: A systematic review and meta-analysis. J. Nutr. Educ. Behav. 2016, 48, 42–53.e1. [Google Scholar] [CrossRef]
- Korre, M.; Sotos-Prieto, M.; Kales, S. Survival Mediterranean style: Lifestyle changes to improve the health of the US fire service. Front. Public Health 2017, 5, 7–13. [Google Scholar] [CrossRef]
- Benhammou, S.; Heras-González, L.; Ibáñez-Peinado, D.; Barceló, C.; Hamdan, M.; Rivas, A.; Mariscal-Arcas, M.; Olea-Serrano, F.; Monteagudo, C. Comparison of Mediterranean diet compliance between European and non-European populations in the Mediterranean basin. Appetite 2016, 107, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef]
- Malakou, E.; Linardakis, M.; Armstrong, M.E.; Zannidi, D.; Foster, C.; Johnson, L.; Papadaki, A. The combined effect of promoting the Mediterranean diet and physical activity on metabolic risk factors in adults: A systematic review and meta-analysis of randomised controlled trials. Nutrients 2018, 10, 1577. [Google Scholar] [CrossRef] [PubMed]
- Sotos-Prieto, M.; Moreno-Franco, B.; Ordovás, J.M.; León, M.; Casasnovas, J.A.; Peñalvo, J.L. Design and development of an instrument to measure overall lifestyle habits for epidemiological research: The Mediterranean Lifestyle (MEDLIFE) index. Public Health Nutr. 2015, 18, 959–967. [Google Scholar] [CrossRef] [PubMed]
- Della Corte, C.; Mosca, A.; Vania, A.; Alterio, A.; Iasevoli, S.; Nobili, V. Good adherence to the Mediterranean diet reduces the risk for NASH and diabetes in pediatric patients with obesity: The results of an Italian Study. Nutrition 2017, 39–40, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Serra-Majem, L.; Román-Viñas, B.; Sanchez-Villegas, A.; Guasch-Ferré, M.; Corella, D.; La Vecchia, C. Benefits of the Mediterranean diet: Epidemiological and molecular aspects. Mol. Asp. Med. 2019, 67, 1–55. [Google Scholar] [CrossRef]
- Foscolou, A.; Magriplis, E.; Tyrovolas, S.; Soulis, G.; Bountziouka, V.; Mariolis, A.; Piscopo, S.; Valacchi, G.; Anastasiou, F.; Gotsis, E.; et al. Lifestyle determinants of healthy ageing in a Mediterranean population: The multinational MEDIS study. Exp. Gerontol. 2018, 110, 35–41. [Google Scholar] [CrossRef]
- Izadi, V.; Tehrani, H.; Haghighatdoost, F.; Dehghan, A.; Surkan, P.J.; Azadbakht, L. Adherence to the DASH and Mediterranean diets is associated with decreased risk for gestational diabetes mellitus. Nutrition 2016, 32, 1092–1096. [Google Scholar] [CrossRef]
- Panagiotakos, D.B.; Georgousopoulou, E.N.; Pitsavos, C.; Chrysohoou, C.; Metaxa, V.; Georgiopoulos, G.; Kalogeropoulou, K.; Tousoulis, D.; Stefanadis, C. Ten-Year (2002–2012) cardiovascular disease incidence and all-cause mortality, in urban Greek population: The ATTICA Study. Int. J. Cardiol. 2015, 180, 178–184. [Google Scholar] [CrossRef]
- Panagiotakos, D.B.; Pitsavos, C.; Stefanadis, C. Dietary patterns: A Mediterranean diet score and its relation to clinical and biological markers of cardiovascular disease risk. Nutr. Metab. Cardiovasc. Dis. 2006, 16, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 2599–2608. [Google Scholar] [CrossRef] [PubMed]
- Naska, A.; Trichopoulou, A. Back to the future: The Mediterranean diet paradigm. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 216–219. [Google Scholar] [CrossRef] [PubMed]
- Gnagnarella, P.; Dragà, D.; Misotti, A.M.; Sieri, S.; Spaggiari, L.; Cassano, E.; Baldini, F.; Soldati, L.; Maisonneuve, P. Validation of a short questionnaire to record adherence to the Mediterranean diet: An Italian experience. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 1140–1147. [Google Scholar] [CrossRef] [PubMed]
- Abu-Saad, K.; Endevelt, R.; Goldsmith, R.; Shimony, T.; Nitsan, L.; Shahar, D.R.; Keinan-Boker, L.; Ziv, A.; Kalter-Leibovici, O. Adaptation and predictive utility of a Mediterranean diet screener score. Clin. Nutr. 2019, 38, 2928–2935. [Google Scholar] [CrossRef] [PubMed]
- Guasch-Ferré, M.; Salas-Salvadó, J.; Ros, E.; Estruch, R.; Corella, D.; Fitó, M.; Martinez-Gonzalez, M.; Arós Borau, F.; Gómez-Gracia, E.; Fiol, M.; et al. The PREDIMED trial, Mediterranean diet and health outcomes: How strong is the evidence? Nutr. Metab. Cardiovasc. Dis. 2017, 27, 624–632. [Google Scholar] [CrossRef]
- Martínez-González, M.Á.; García-Arellano, A.; Toledo, E.; Salas-Salvadó, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schröder, H.; Arós, F.; Gómez-Gracia, E.; et al. A 14-Item Mediterranean diet assessment tool and obesity indexes among high-risk subjects: The PREDIMED Trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef]
- Zaragoza-Martí, A.; Cabañero-Martínez, M.J.; Hurtado-Sánchez, J.A.; Laguna-Pérez, A.; Ferrer-Cascales, R. Evaluation of Mediterranean diet adherence scores: A systematic review. BMJ Open 2018, 8, 1–8. [Google Scholar] [CrossRef]
- Yang, J.; Farioli, A.; Korre, M.; Kales, S.N. Modified Mediterranean Diet score and cardiovascular risk in a north American working population. PLoS ONE 2014, 9, e87539. [Google Scholar] [CrossRef]
- Sotos-Prieto, M.; Cash, S.B.; Christophi, C.; Folta, S.C.; Moffatt, S.; Muegge, C.M.; Korre, M.; Mozaffarian, D.; Kales, S.N. Rationale and design of feeding America’s bravest: Mediterranean diet-based intervention to change firefighters’ eating habits and improve cardiovascular risk profiles. Contemp. Clin. Trials 2017, 61, 101–107. [Google Scholar] [CrossRef]
- Willett, W.C.; Sampson, L.; Stampfer, M.J.; Rosner, B.; Bain, C.; Witschi, J.; Hennekens, C.H.; Speizer, F.E. Reproducibility and validity of a semiquantitative food frequency questionnaire. Am. J. Epidemiol. 1985, 122, 51–65. [Google Scholar] [CrossRef] [PubMed]
- Salvini, S.; Hunter, D.J.; Sampson, L.; Stampfer, M.J.; Colditz, G.A.; Rosner, B.; Willett, W.C. Food-Based validation of a dietary questionnaire: The effects of week-to-week variation in food consumption. Int. J. Epidemiol. 1989, 18, 858–867. [Google Scholar] [CrossRef] [PubMed]
- Sotos-Prieto, M.; Christophi, C.; Black, A.; Furtado, J.D.; Song, Y.; Magiatis, P.; Papakonstantinou, A.; Melliou, E.; Moffatt, S.; Kales, S.N. Assessing validity of self-reported dietary intake within a Mediterranean diet cluster randomized controlled trial among US firefighters. Nutrients 2019, 11, 2250. [Google Scholar] [CrossRef]
- Jackson, A.S.; Blair, S.N.; Mahar, M.T.; Wier, L.T.; Ross, R.M.; Stuteville, J.E. Prediction of functional aerobic capacity without exercise testing. Med. Sci. Sports Exerc. 1990, 22, 863–870. [Google Scholar] [CrossRef] [PubMed]
- Hershey, M.S.; Sotos-Prieto, M.; Ruiz-Canela, M.; Martínez-González, M.Á.; Cassidy, A.; Moffatt, S.; Kales, S. Anthocyanin intake and physical activity: Associations with the lipid profile of a US working population. Molecules 2020, 25, 4398. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R. Anti-Inflammatory effects of the Mediterranean diet: The experience of the PREDIMED study. Proc. Nutr. Soc. 2010, 69, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Amato, M.; Bonomi, A.; Laguzzi, F.; Veglia, F.; Tremoli, E.; Werba, J.P.; Giroli, M.G. Overall dietary variety and adherence to the Mediterranean diet show additive protective effects against coronary heart disease. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1315–1321. [Google Scholar] [CrossRef]
- Merino, J.; Kones, R.; Ros, E. Effects of Mediterranean diet on endothelial function. In Endothelium and Cardiovascular Diseases; Academic Press: Cambridge, MA, USA, 2018; pp. 363–389. [Google Scholar]
- Romaguera, D.; Norat, T.; Mouw, T.; May, A.M.; Bamia, C.; Slimani, N.; Travier, N.; Besson, H.; Luan, J.; Wareham, N.; et al. Adherence to the Mediterranean Diet is associated with lower abdominal adiposity in European men and women. J. Nutr. 2009, 139, 1728–1737. [Google Scholar] [CrossRef]
- Mattei, J.; Sotos-Prieto, M.; Bigornia, S.J.; Noel, S.E.; Tucker, K.L. The Mediterranean diet score is more strongly associated with favorable cardiometabolic risk factors over 2 years than other diet quality indexes in puerto rican adults. J. Nutr. 2017, 147, 661–669. [Google Scholar] [CrossRef]
- Aoun, C.; Papazian, T.; Helou, K.; El Osta, N.; Khabbaz, L.R. Comparison of five international indices of adherence to the Mediterranean diet among healthy adults: Similarities and differences. Nutr. Res. Pract. 2019, 13, 333–343. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Naska, A.; Orfanos, P.; Trichopoulos, D. Mediterranean diet in relation to body mass index and waist-to-hip ratio: The Greek European prospective investigation into cancer and nutrition study. Am. J. Clin. Nutr. 2005, 82, 935–940. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Ruiz-Gutiérrez, V.; Covas, M.I.; Fiol, M.; Gómez-Gracia, E.; López-Sabater, M.C.; Vinyoles, E.; et al. Effects of a Mediterranean-style diet on cardiovascular risk factors a randomized trial. Ann. Intern. Med. 2006, 145, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N. Engl. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef] [PubMed]
- Sahingoz, S.A.; Sanlier, N. Compliance with Mediterranean Diet Quality Index (KIDMED) and nutrition knowledge levels in adolescents. A case study from Turkey. Appetite 2011, 57, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Krauss, R.M.; Eckel, R.H.; Howard, B.; Appel, L.J.; Daniels, S.R.; Deckelbaum, R.J.; Erdman, J.W.; Kris-Etherton, P.; Goldberg, I.J.; Kotchen, T.A.; et al. AHA Dietary Guidelines: Revision 2000: A statement for healthcare professionals from the Nutrition Committee of the American Heart Association. Circulation 2000, 102, 2284–2299. [Google Scholar] [CrossRef]
- Willett, W.C. The Mediterranean diet: Science and practice. Public Health Nutr. 2006, 9, 105–110. [Google Scholar] [CrossRef]
- Mozaffarian, D. Dietary and policy priorities for cardiovascular disease, diabetes, and obesity. Circulation 2016, 133, 187–225. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; Hershey, M.S.; Zazpe, I.; Trichopoulou, A. Transferability of the Mediterranean diet to non-mediterranean countries. What is and what is not the Mediterranean diet. Nutrients 2017, 9, 1226. [Google Scholar] [CrossRef]
- Soriguer, F.; Rojo-Martínez, G.; Dobarganes, M.C.; Almeida, J.M.G.; Esteva, I.; Beltrán, M.; De Adana, M.S.R.; Tinahones, F.; Gómez-Zumaquero, J.M.; García-Fuentes, E.; et al. Hypertension is related to the degradation of dietary frying oils. Am. J. Clin. Nutr. 2003, 78, 1092–1097. [Google Scholar] [CrossRef]
- Godos, J.; Rapisarda, G.; Marventano, S.; Galvano, F.; Mistretta, A.; Grosso, G. Association between polyphenol intake and adherence to the Mediterranean diet in Sicily, southern Italy. NFS J. 2017, 8, 1–7. [Google Scholar] [CrossRef]
- Pérez-Martínez, P.; Mikhailidis, D.P.; Athyros, V.G.; Bullo, M.; Couture, P.; Covas, M.I.; De Koning, L.; Delgado-Lista, J.; Díaz-López, A.; Drevon, C.A.; et al. Lifestyle recommendations for the prevention and management of metabolic syndrome: An international panel recommendation. Nutr. Rev. 2017, 75, 307–326. [Google Scholar] [CrossRef] [PubMed]
- Morin, S.J.; Gaziano, J.M.; Djoussé, L. Relation between plasma phospholipid oleic acid and risk of heart failure. Eur. J. Nutr. 2017, 57, 2937–2942. [Google Scholar] [CrossRef] [PubMed]
- Gurevich, K.; Poston, W.S.C.; Anders, B.; Ivkina, M.A.; Archangelskaya, A.; Jitnarin, N.; Starodubov, V.I. Obesity prevalence and accuracy of BMI-defined obesity in Russian firefighters. Occup. Med. 2016, 67, 61–63. [Google Scholar] [CrossRef] [PubMed]

| Characteristic | N | |
|---|---|---|
| Male gender, n (%) | 448 | 423 (94.4) |
| Age (years), mean (SD) | 460 | 46.7 (8.3) |
| Race, n (%) | 311 | |
| Caucasian | 266 (85.5) | |
| African American | 39 (12.5) | |
| Other | 6 (1.9) | |
| Currently smoking, n (%) | 314 | 15 (4.8) |
| Physical activity *, n (%) | 307 | |
| Low | 39 (12.7) | |
| Medium | 65 (21.2) | |
| High | 203 (66.1) | |
| Hours sitting per week, median (Q1–Q3) | 300 | 15 (10–24) |
| Number of meals at the firehouse, median (Q1–Q3) | 309 | 3 (2–3) |
| FFQ mMDS, mean (SD) | 460 | 21.88 (6.68) |
| Anthropometric variables | ||
| BMI (kg/m2), mean (SD) | 460 | 30.01 (4.39) |
| Normal weight | 74 | 16% |
| Overweight | 156 | 34% |
| Obese | 230 | 50% |
| Waist circumference (cm), mean (SD) | 459 | 99.7 (12.5) |
| Body fat percentage (%), mean (SD) | 458 | 28.10 (6.55) |
| Blood pressure variables | ||
| Resting SBP (mmHg), mean (SD) | 460 | 125.5 (11.2) |
| Resting DBP (mmHg), mean (SD) | 460 | 79.1 (6.8) |
| Biochemical variables | ||
| Total Cholesterol (mg/dL), mean (SD) | 460 | 197.1 (37.7) |
| HDL-Cholesterol (mg/dL), mean (SD) | 460 | 48.5 (11.4) |
| LDL-Cholesterol (mg/dL), mean (SD) | 452 | 123.5 (32.6) |
| Total Cholesterol/HDL ratio, mean (SD) | 460 | 4.26 (1.32) |
| Triglycerides (mg/dL), mean (SD) | 459 | 126.0 (76.6) |
| Glucose (mg/dL), mean (SD) | 460 | 99.5 (19.6) |
| mMDS | |||||||
|---|---|---|---|---|---|---|---|
| Risk Factor | 1st Quartile | 2nd Quartile | 3rd Quartile | 4th Quartile | P Trend * | P Trend † | P Trend ‡ |
| Number of subjects | 106 | 122 | 118 | 114 | |||
| Anthropometric variables | |||||||
| BMI (kg/m2) | 30.59 (4.06) | 30.14 (4.82) | 30.17 (4.70) | 29.16 (3.77) | 0.023 | 0.030 | 0.914 |
| Waist circumference (cm) | 102.0 (11.6) | 100.6 (13.6) | 99.3 (12.9) | 96.8 (11.0) | 0.001 | 0.002 | 0.685 |
| Body fat percentage (%) | 28.96 (5.64) | 28.61 (6.38) | 28.42 (7.06) | 26.42 (6.75) | 0.005 | 0.002 | 0.886 |
| Blood pressure variables | |||||||
| Resting SBP (mmHg) | 125.7 (10.8) | 124.7 (11.4) | 126.6 (12.7) | 125.1 (9.5) | 0.980 | 0.836 | 0.515 |
| Resting DBP (mmHg) | 79.6 (7.2) | 78.8 (6.7) | 79.3 (6.3) | 78.6 (7.1) | 0.418 | 0.522 | 0.927 |
| Biochemical variables | |||||||
| Total Cholesterol (mg/dL) | 200.2 (36.6) | 193.1 (37.0) | 198.2 (41.4) | 197.5 (35.4) | 0.894 | 0.876 | 0.742 |
| HDL-Cholesterol (mg/dL) | 45.6 (10.1) | 48.6 (11.9) | 48.7 (11.5) | 50.9 (11.4) | 0.001 | 0.002 | 0.022 |
| LDL-Cholesterol (mg/dL) | 127.3 (32.7) | 119.5 (30.1) | 124.4 (35.3) | 123.6 (32.2) | 0.703 | 0.690 | 0.587 |
| Total Cholesterol/HDL ratio | 4.60 (1.31) | 4.19 (1.58) | 4.27 (1.28) | 4.03 (0.96) | 0.004 | 0.007 | 0.020 |
| Triglycerides (mg/dL) | 140.8 (85.9) | 118.4 (62.7) | 129.2 (88.4) | 116.9 (65.7) | 0.071 | 0.107 | 0.364 |
| Glucose (mg/dL) | 99.9 (14.3) | 100.9 (23.2) | 98.6 (20.5) | 98.6 (18.9) | 0.450 | 0.594 | 0.770 |
| Linear Regression Models | ||||||
|---|---|---|---|---|---|---|
| Adjusted by Gender and Age | Adjusted by Age, Gender, Race, Physical Activity, and Smoking | |||||
| Risk Factor | Β Coefficient | SE | p Value | Β Coefficient | SE | p Value |
| Anthropometric variables | ||||||
| BMI (kg/m2) | −0.080 | 0.030 | 0.008 | −0.026 | 0.038 | 0.490 |
| Waist circumference (in) | −0.114 | 0.031 | <0.001 | −0.045 | 0.039 | 0.241 |
| Body fat percentage (%) | −0.141 | 0.043 | 0.001 | −0.028 | 0.057 | 0.627 |
| Blood pressure variables | ||||||
| Resting SBP (mmHg) | −0.041 | 0.076 | 0.590 | 0.004 | 0.107 | 0.969 |
| Resting DBP (mmHg) | −0.056 | 0.046 | 0.223 | −0.037 | 0.062 | 0.552 |
| Biochemical variables | ||||||
| Total Cholesterol (mg/dL) | −0.160 | 0.264 | 0.546 | −0.289 | 0.332 | 0.385 |
| HDL Cholesterol (mg/dL) | 0.254 | 0.075 | <0.001 | 0.286 | 0.100 | 0.004 |
| LDL Cholesterol (mg/dL) | −0.193 | 0.230 | 0.402 | −0.341 | 0.300 | 0.256 |
| Total cholesterol-HDL ratio | −0.028 | 0.009 | 0.002 | −0.030 | 0.010 | 0.002 |
| Triglycerides (mg/dL) | −1.010 | 0.532 | 0.058 | −0.909 | 0.644 | 0.159 |
| Glucose (mg/dL) | −0.137 | 0.135 | 0.313 | −0.155 | 0.186 | 0.404 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romanidou, M.; Tripsianis, G.; Hershey, M.S.; Sotos-Prieto, M.; Christophi, C.; Moffatt, S.; Constantinidis, T.C.; Kales, S.N. Association of the Modified Mediterranean Diet Score (mMDS) with Anthropometric and Biochemical Indices in US Career Firefighters. Nutrients 2020, 12, 3693. https://doi.org/10.3390/nu12123693
Romanidou M, Tripsianis G, Hershey MS, Sotos-Prieto M, Christophi C, Moffatt S, Constantinidis TC, Kales SN. Association of the Modified Mediterranean Diet Score (mMDS) with Anthropometric and Biochemical Indices in US Career Firefighters. Nutrients. 2020; 12(12):3693. https://doi.org/10.3390/nu12123693
Chicago/Turabian StyleRomanidou, Maria, Grigorios Tripsianis, Maria Soledad Hershey, Mercedes Sotos-Prieto, Costas Christophi, Steven Moffatt, Theodoros C. Constantinidis, and Stefanos N. Kales. 2020. "Association of the Modified Mediterranean Diet Score (mMDS) with Anthropometric and Biochemical Indices in US Career Firefighters" Nutrients 12, no. 12: 3693. https://doi.org/10.3390/nu12123693
APA StyleRomanidou, M., Tripsianis, G., Hershey, M. S., Sotos-Prieto, M., Christophi, C., Moffatt, S., Constantinidis, T. C., & Kales, S. N. (2020). Association of the Modified Mediterranean Diet Score (mMDS) with Anthropometric and Biochemical Indices in US Career Firefighters. Nutrients, 12(12), 3693. https://doi.org/10.3390/nu12123693