The Influence of Response Inhibition Training on Food Consumption and Implicit Attitudes toward Food among Female Restrained Eaters



Abstract
1. Introduction
2. Experiment 1
2.1. Method
2.1.1. Participants
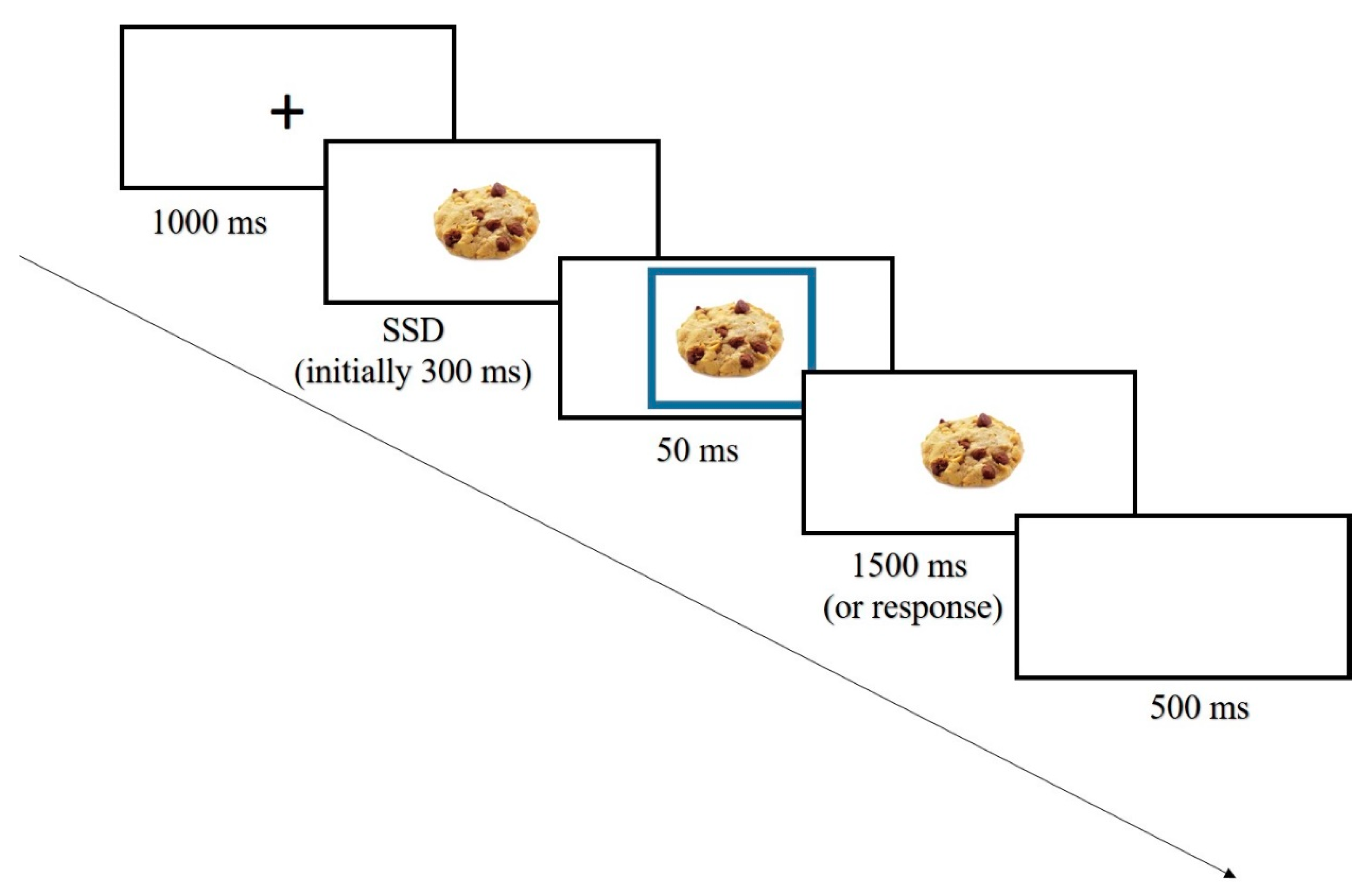
2.1.2. Procedure
2.1.3. Measures
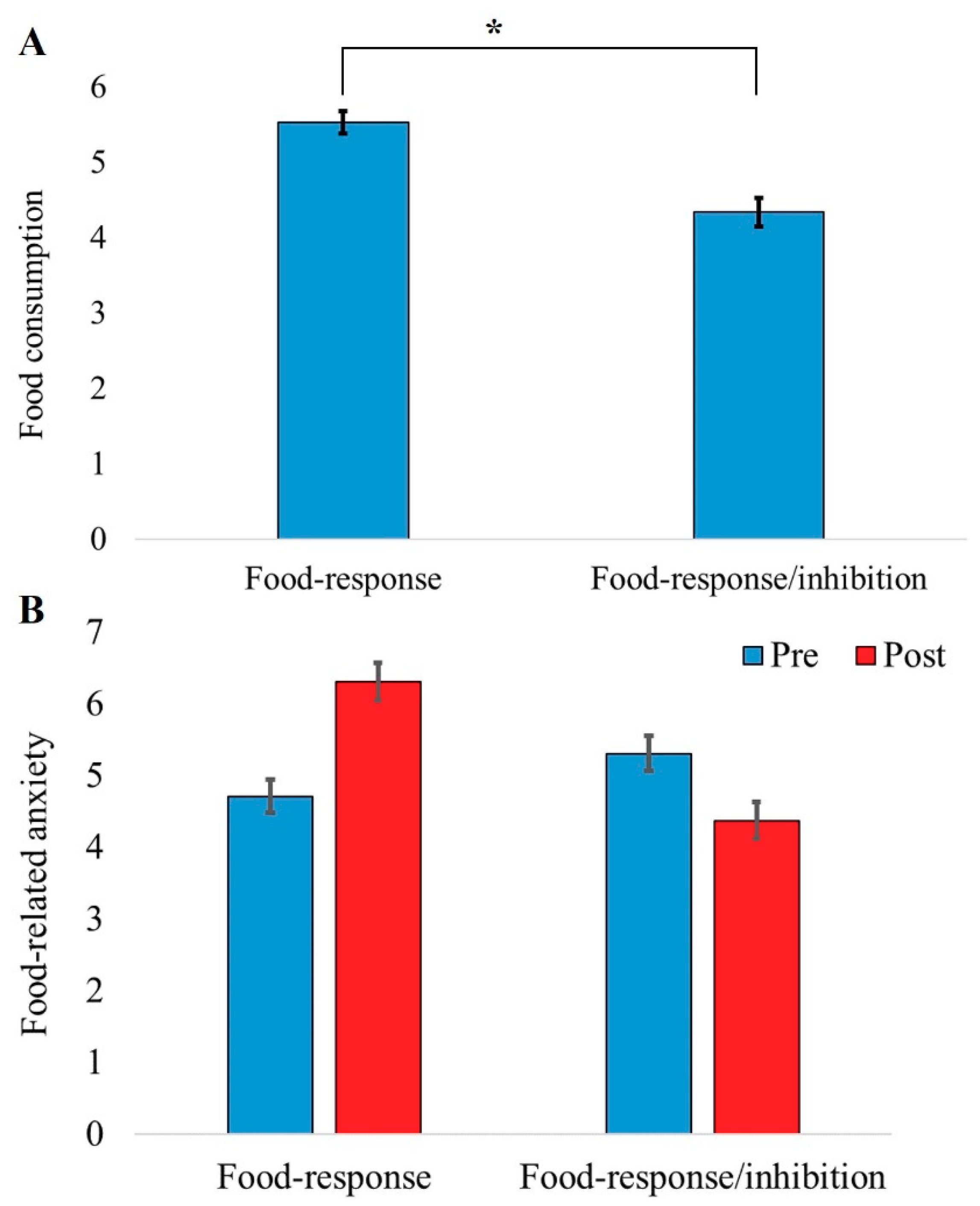
2.2. Results
2.3. Discussion Experiment 1
3. Experiment 2
3.1. Method
3.1.1. Participants
3.1.2. Procedure
3.1.3. Measures
3.2. Results
3.3. Discussion Experiment 2
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Tuschl, R.J. From dietary restraint to binge eating: Some theoretical considerations. Appetite 1990, 14, 105–109. [Google Scholar] [CrossRef]
- Houben, K.; Jansen, A. Lacking skills to improve self-control: Reward-induced loss of inhibitory control and overeating in restrained eaters. J. Exp. Psychopathol. 2014, 5, 29–37. [Google Scholar] [CrossRef]
- Jansen, A.; van den Hout, M. On being led into temptation: “Counterregulation” of dieters after smelling a “preload”. Addict. Behav. 1991, 16, 247–253. [Google Scholar] [CrossRef]
- Hagan, K.E.; Forbush, K.T.; Chen, P.Y. Is dietary restraint a unitary or multi-faceted construct? Psychol. Assess. 2017, 29, 1249–1260. [Google Scholar] [CrossRef]
- Polivy, J.; Herman, C.P. Restrained eating and food cues: Recent findings and conclusions. Curr. Obes. Rep. 2017, 6, 79–85. [Google Scholar] [CrossRef]
- Diamond, A. Executive functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef]
- Bartholdy, S.; Dalton, B.; O’Daly, O.G.; Campbell, I.C.; Schmidt, U. A systematic review of the relationship between eating, weight and inhibitory control using the stop signal task. Neurosci. Biobehav. Rev. 2016, 64, 35–62. [Google Scholar] [CrossRef]
- Wu, M.; Hartmann, M.; Skunde, M.; Herzog, W.; Friederich, H.C. Inhibitory control in bulimic-type eating disorders: A systematic review and meta-analysis. PLoS ONE 2013, 8, e83412. [Google Scholar] [CrossRef]
- Houben, K.; Nederkoorn, C.; Jansen, A. Eating on impulse: The relation between overweight and food-specific inhibitory control. Obesity 2014, 22, 6–8. [Google Scholar] [CrossRef]
- Lavagnino, L.; Arnone, D.; Cao, B.; Soares, J.C.; Selvaraj, S.; Brockmeyer, T.; Sinno, M.H.; Skunde, M.; Wu, M.; Woehning, A.; et al. Inhibitory control in obesity and binge eating disorder: A systematic review and meta-analysis of neurocognitive and neuroimaging studies. Neurosci. Biobehav. Rev. 2016, 9, 299–309. [Google Scholar] [CrossRef]
- Svaldi, J.; Naumann, E.; Trentowska, M.; Schmitz, F. General and food-specific inhibitory deficits in binge eating disorder. Int. J. Eat. Disord. 2014, 47, 534–542. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.E.; Mason, T.B.; Schaefer, L.M.; Juarascio, A.; Dvorak, R.; Weinbach, N.; Crosby, R.D.; Wonderlich, S.A. Examining intra-individual variability in food-related inhibitory control and negative affect as predictors of binge eating using ecological momentary assessment. J. Psychiatr. Res. 2019. [Google Scholar] [CrossRef] [PubMed]
- Weinbach, N.; Lock, J.; Bohon, C. Superior response inhibition to high-calorie foods in adolescents with anorexia nervosa. Behav. Res. Ther. 2020, 124, 103441. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Hill, L.; Peck, S.K.; Wierenga, C.E.; Kaye, W.H. Applying neurobiology to the treatment of adults with anorexia nervosa. J. Eat. Disord. 2016, 4, 31. [Google Scholar] [CrossRef] [PubMed]
- Nederkoorn, C.; Van Eijs, Y.; Jansen, A. Restrained eaters act on impulse. Pers. Individ. Dif. 2004, 37, 1651–1658. [Google Scholar] [CrossRef]
- Dong, D.; Lei, X.; Jackson, T.; Wang, Y.; Su, Y.; Chen, H. Altered regional homogeneity and efficient response inhibition in restrained eaters. Neuroscience 2014, 266, 116–126. [Google Scholar] [CrossRef]
- Ganor-Moscovitz, N.; Weinbach, N.; Canetti, L.; Kalanthroff, E. The effect of food-related stimuli on inhibition in high vs. low restrained eaters. Appetite 2018, 131, 53–58. [Google Scholar] [CrossRef]
- Jones, A.; Hardman, C.A.; Lawrence, N.; Field, M. Cognitive training as a potential treatment for overweight and obesity: A critical review of the evidence. Appetite 2018, 124, 50–67. [Google Scholar] [CrossRef]
- Jones, A.; Di Lemma, L.C.G.; Robinson, E.; Christiansen, P.; Nolan, S.; Tudur-Smith, C.; Field, M. Inhibitory control training for appetitive behaviour change: A meta-analytic investigation of mechanisms of action and moderators of effectiveness. Appetite 2016, 97, 16–28. [Google Scholar] [CrossRef]
- Kalanthroff, E.; Steinman, S.A.; Schmidt, A.B.; Campeas, R.; Simpson, H.B. Piloting a personalized computerized inhibitory training program for individuals with obsessive-compulsive disorder. Psychother. Psychosom. 2018, 87, 52–55. [Google Scholar] [CrossRef]
- Chen, Z.; Veling, H.; Dijksterhuis, A.; Holland, R.W. Do impulsive individuals benefit more from food go/no-go training? Testing the role of inhibition capacity in the no-go devaluation effect. Appetite 2018, 124, 99–110. [Google Scholar] [CrossRef]
- Chen, Z.; Veling, H.; De Vries, S.P.; Bijvank, B.O.; Janssen, I.M.C.; Dijksterhuis, A.; Holland, R.W. Go/No-Go training changes food evaluation in both morbidly obese and normal-weight individuals. J. Consult. Clin. Psychol. 2018, 86, 980–990. [Google Scholar] [CrossRef]
- Chen, Z.; Veling, H.; Dijksterhuis, A.; Holland, R.W. How does not responding to appetitive stimuli cause devaluation: Evaluative conditioning or response inhibition? J. Exp. Psychol. Gen. 2016, 145, 1687–1701. [Google Scholar] [CrossRef]
- Van Strien, T.; Frijters, J.E.R.; Bergers, G.P.A.; Defares, P.B. The Dutch Eating Behavior Questionnaire (DEBQ) for assessment of restrained, emotional, and external eating behavior. Int. J. Eat. Disord. 1986, 5, 295–315. [Google Scholar] [CrossRef]
- Blechert, J.; Meule, A.; Busch, N.A.; Ohla, K. Food-pics: An image database for experimental research on eating and appetite. Front. Psychol. 2014, 5, 617. [Google Scholar] [CrossRef]
- Robinson, E.; Haynes, A.; Hardman, C.A.; Kemps, E.; Higgs, S.; Jones, A. The bogus taste test: Validity as a measure of laboratory food intake. Appetite 2017, 116, 223–231. [Google Scholar] [CrossRef]
- Evers, C.; Dingemans, A.; Junghans, A.F.; Boevé, A. Feeling bad or feeling good, does emotion affect your consumption of food? A meta-analysis of the experimental evidence. Neurosci. Biobehav. Rev. 2018, 92, 195–208. [Google Scholar] [CrossRef]
- Papies, E.K.; Stroebe, W.; Aarts, H. Who likes it more? Restrained eaters’ implicit attitudes towards food. Appetite 2009, 53, 279–287. [Google Scholar] [CrossRef]
- Verbruggen, F.; Logan, G.D.; Stevens, M.A. STOP-IT: Windows executable software for the stop-signal paradigm. Behav. Res. Methods 2008, 40, 479–483. [Google Scholar] [CrossRef]
- Zhou, Y.; Liu, Y.; Du, J.; Chen, H. Effects of food exposure on food-related inhibitory control in restrained eaters: An ERP study. Neurosci. Lett. 2018, 672, 130–135. [Google Scholar] [CrossRef]
- Forstmann, B.U.; Jahfari, S.; Scholte, H.S.; Wolfensteller, U.; van den Wildenberg, W.P.M.; Ridderinkhof, K.R. Function and structure of the right inferior frontal cortex predict individual differences in response inhibition: A model-based approach. J. Neurosci. 2008, 28, 9790–9796. [Google Scholar] [CrossRef]
- White, C.N.; Congdon, E.; Mumford, J.A.; Karlsgodt, K.H.; Sabb, F.W.; Freimer, N.B.; London, E.D.; Cannon, T.D.; Bilder, R.M.; Poldrack, R.A. Decomposing decision components in the stop-signal task: A model-based approach to individual differences in inhibitory control. J. Cogn. Neurosci. 2014, 26, 1601–1614. [Google Scholar] [CrossRef]
- Congdon, E.; Mumford, J.A.; Cohen, J.R.; Galvan, A.; Aron, A.R.; Xue, G.; Miller, E.; Poldrack, R.A. Engagement of large-scale networks is related to individual differences in inhibitory control. Neuroimage 2010, 53, 653–663. [Google Scholar] [CrossRef] [PubMed]
- Adams, S.; Mokrysz, C.; Attwood, A.S.; Munafò, M.R. Resisting the urge to smoke: Inhibitory control training in cigarette smokers. R. Soc. Open Sci. 2017, 4, 170045. [Google Scholar] [CrossRef] [PubMed]
- Houben, K.; Havermans, R.C.; Nederkoorn, C.; Jansen, A. Beer à no-go: Learning to stop responding to alcohol cues reduces alcohol intake via reduced affective associations rather than increased response inhibition. Addiction 2012, 107, 1280–1287. [Google Scholar] [CrossRef]
- Houben, K.; Jansen, A. Chocolate equals stop. Chocolate-specific inhibition training reduces chocolate intake and go associations with chocolate. Appetite 2015, 87, 318–323. [Google Scholar] [CrossRef]
- Allom, V.; Mullan, B.; Hagger, M. Does inhibitory control training improve health behaviour? A meta-analysis. Health Psychol. Rev. 2016, 10, 168–186. [Google Scholar] [CrossRef]
- Schaumberg, K.; Anderson, D.A.; Anderson, L.M.; Reilly, E.E.; Gorrell, S. Dietary restraint: What’s the harm? A review of the relationship between dietary restraint, weight trajectory and the development of eating pathology. Clin. Obes. 2016, 6, 89–100. [Google Scholar] [CrossRef]
- Polivy, J.; Herman, C.P.; Mills, J.S. What is restrained eating and how do we identify it? Appetite 2020, 155, 104820. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Experiment 1 | ||||
| Factor | Food response (n = 32) | Food response/inhibition (n = 32) | t | p-value |
| Age | 24.06 (2.4) [19–32] | 24.13 (2.2) [19–31] | t(62) = 0.11 | 0.914 |
| BMI | 23.85 (3.3) [18.4–30.1] | 24.16 (4.1) [15.2–35] | t(62) = 0.34 | 0.736 |
| DEBQ-R | 3.07 (2.88) [2.6–3.6] | 3.08 (0.3) [2.6–3.6] | t(62) = 0.13 | 0.898 |
| Experiment 2 | ||||
| Food response (n = 23) | Food response/inhibition (n = 24) | p-value | ||
| Age | 25.04 (4.1) [20–40] | 26.54 (6.6) [20–49] | t(45) = 0.94 | 0.354 |
| BMI | 24.08 (3.7) [8.8–34.2] | 25.33 (3.5) [20.3–35] | t(45) = 1.18 | 0.243 |
| DEBQ-R | 3.81 (0.5) [3.1–4.6] | 3.78 (0.5) [3.1–5] | t(45) = -0.18 | 0.859 |
| Factor | Positive Valence | Negative Valence | ||||||
|---|---|---|---|---|---|---|---|---|
| Pre-Training | Post-Training | Pre-Training | Post-Training | |||||
| Non-food | Food | Non-food | Food | Non-food | Food | Non-food | Food | |
| Food response/inhibition | 646 (97) [0.91] | 623 (93) [0.95] | 645 (92) [0.84] | 573 (79) [0.96] | 614 (96) [0.95] | 647 (111) [0.86] | 560 (80) [0.97] | 612 (98) [0.87] |
| Food response | 621 (89) [0.87] | 592 (76) [0.93] | 613 (85) [0.87] | 569 (78) [0.95] | 569 (71) [0.97] | 625 (84) [0.87] | 558 (67) [0.97] | 598 (86) [0.89] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weinbach, N.; Keha, E.; Leib, H.; Kalanthroff, E. The Influence of Response Inhibition Training on Food Consumption and Implicit Attitudes toward Food among Female Restrained Eaters. Nutrients 2020, 12, 3609. https://doi.org/10.3390/nu12123609
Weinbach N, Keha E, Leib H, Kalanthroff E. The Influence of Response Inhibition Training on Food Consumption and Implicit Attitudes toward Food among Female Restrained Eaters. Nutrients. 2020; 12(12):3609. https://doi.org/10.3390/nu12123609
Chicago/Turabian StyleWeinbach, Noam, Eldad Keha, Hila Leib, and Eyal Kalanthroff. 2020. "The Influence of Response Inhibition Training on Food Consumption and Implicit Attitudes toward Food among Female Restrained Eaters" Nutrients 12, no. 12: 3609. https://doi.org/10.3390/nu12123609
APA StyleWeinbach, N., Keha, E., Leib, H., & Kalanthroff, E. (2020). The Influence of Response Inhibition Training on Food Consumption and Implicit Attitudes toward Food among Female Restrained Eaters. Nutrients, 12(12), 3609. https://doi.org/10.3390/nu12123609