Validity and Reproducibility of a Culture-Specific Food Frequency Questionnaire in Lebanon

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
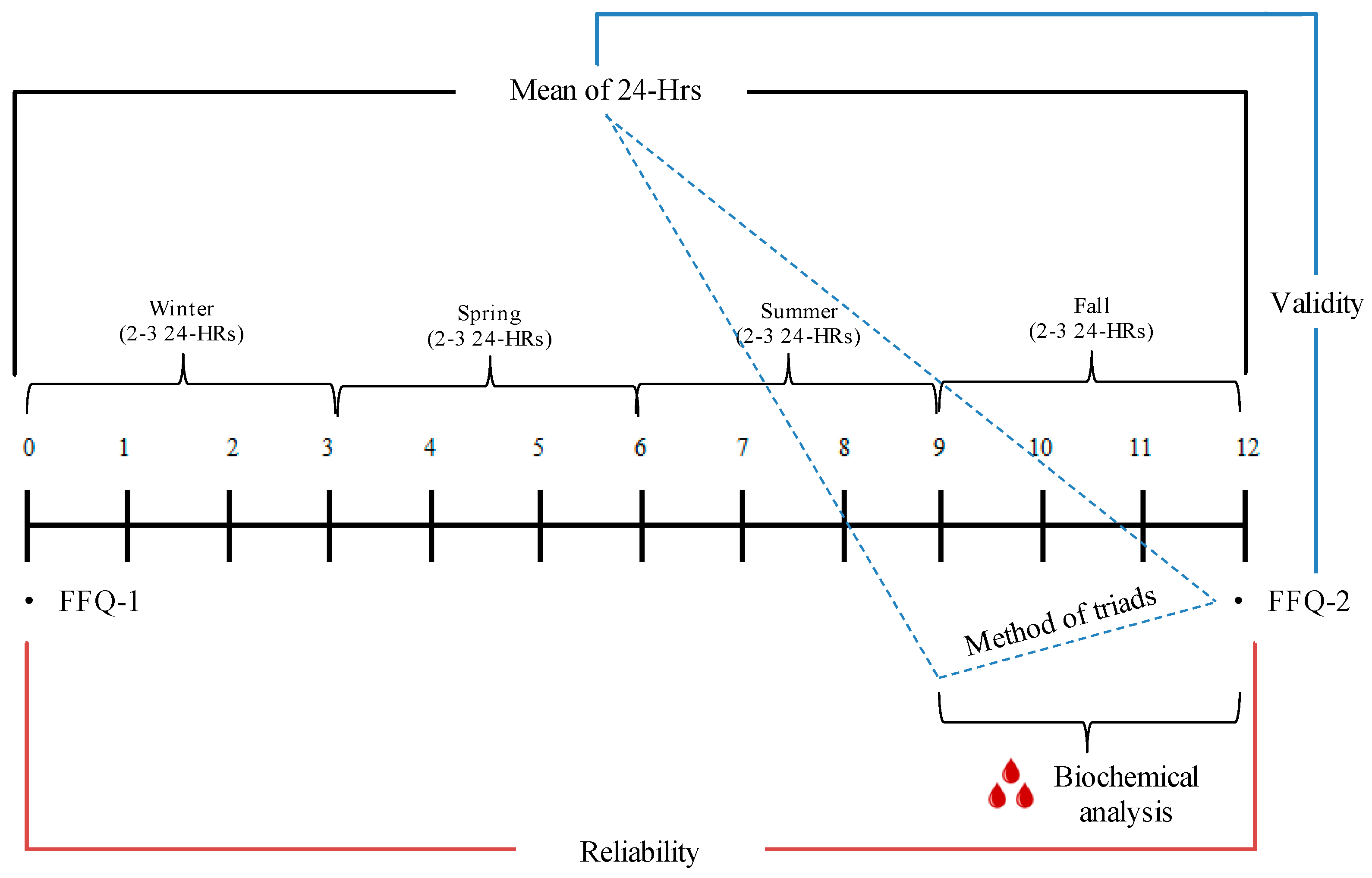
2.2. Study Design
2.3. Data Collcetion
2.4. Dietary Assessment: Food Frequency Questionnaire (FFQ): Development and Collection
2.5. Dietary Assessment: 24-h Recalls (24-HRs) Using the Multiple Pass Food Recall Approach
2.6. Blood Sample Collection and Laboratory Analysis
2.7. Baseline Anthropometric Assessment and Socio-Demographic and Lifestyle Questionnaire
2.8. Sample Size for the Diet-Diet Comparison or Diet-Biochemical Comparison
2.9. Statistical Analysis
3. Results
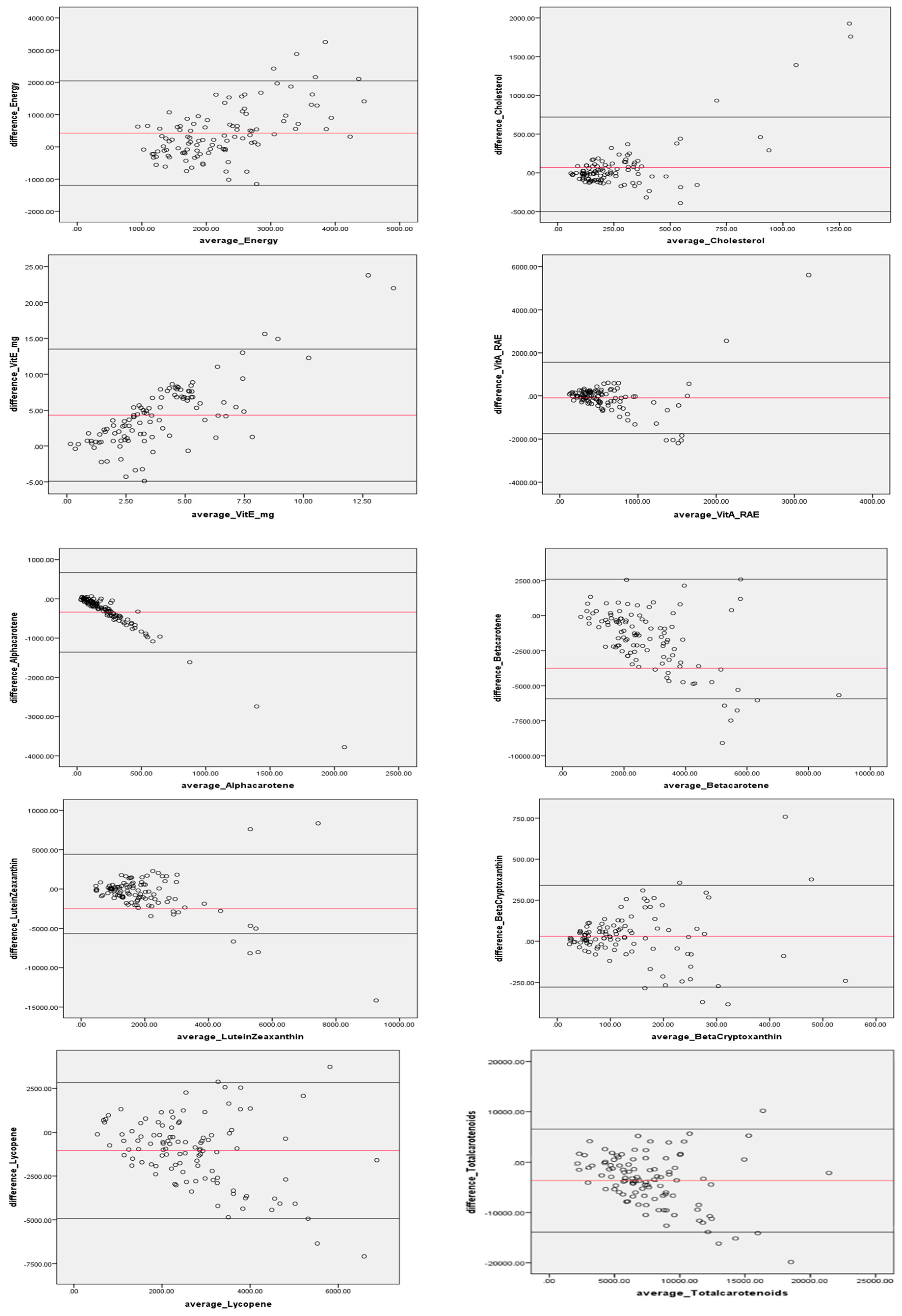
3.1. Diet-Diet FFQ Validity
3.2. FFQ Reproducibility
4. Discussion
4.1. FFQ Validity: Diet-Diet and Diet-Biochemical Comparisons
4.2. FFQ Validity: Diet-biochemical Correlations
4.3. FFQ Reproducibility
4.4. Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Noncommunicable Diseases: Progress Monitor 2017. Available online: https://apps.who.int/iris/bitstream/handle/10665/258940/9789241513029-eng.pdf?sequence=1 (accessed on 4 October 2019).
- Swinburn, B.A.; Sacks, G.; Lo, S.K.; Westerterp, K.R.; Rush, E.C.; Rosenbaum, M.; Luke, A.; Schoeller, D.A.; Delany, J.P.; Butte, N.F.; et al. Estimating the Changes in Energy Flux That Characterize the Rise in Obesity Prevalence. Am. J. Clin. Nutr. 2009, 89, 1723–1728. [Google Scholar] [CrossRef]
- Lim, J.; Park, H.S. Trends in the Prevalence of Underweight, Obesity, Abdominal Obesity and Their Related Lifestyle Factors in Korean Young Adults, 1998–2012. Obes. Res. Clin. Pract. 2018, 12, 358–364. [Google Scholar] [CrossRef]
- Naja, F.; Hwalla, N.; Itani, L.; Salem, M.; Azar, S.T.; Zeidan, M.N.; Nasreddine, L. Dietary Patterns and Odds of Type 2 Diabetes in Beirut, Lebanon: A Case–Control Study. Nutr. Metab. Nutr. 2012, 9, 111. [Google Scholar] [CrossRef]
- Nasreddine, L.; Naja, F.; Sibai, A.; Helou, K.; Adra, N.; Hwalla, N. Trends in Nutritional Intakes and Nutrition-Related Cardiovascular Disease Risk Factors in Lebanon: The Need for Immediate Action. Leban. Med. J. 2014, 62, 83–91. [Google Scholar] [CrossRef]
- Nasreddine, L.; Tamim, H.; Itani, L.; Nasrallah, M.P.; Isma’Eel, H.; Nakhoul, N.F.; Abou-Rizk, J.; Naja, F. A Minimally Processed Dietary Pattern Is Associated with Lower Odds of Metabolic Syndrome among Lebanese Adults. Public Health Nutr. 2017, 21, 160–171. [Google Scholar] [CrossRef]
- Smith-Warner, S.A.; Spiegelman, D.; Yaun, S.-S.; Adami, H.-O.; Beeson, W.L.; Brandt, P.A.V.D.; Folsom, A.R.; Fraser, G.E.; Freudenheim, J.L.; Goldbohm, R.A.; et al. Intake of Fruits and Vegetables and Risk of Breast Cancer: A Pooled Analysis of Cohort Studies. JAMA 2001, 285, 769–776. [Google Scholar] [CrossRef]
- Zeng, L.; Hu, S.; Chen, P.; Wei, W.; Tan, Y. Macronutrient Intake and Risk of Crohn’s Disease: Systematic Review and Dose–Response Meta-Analysis of Epidemiological Studies. Nutrients 2017, 9, 500. [Google Scholar] [CrossRef]
- Aune, D.; Keum, N.; Giovannucci, E.; Fadnes, L.T.; Boffetta, P.; Greenwood, D.C.; Tonstad, S.; Vatten, L.J.; Riboli, E.; Norat, T. Dietary Intake and Blood Concentrations of Antioxidants and the Risk of Cardiovascular Disease, Total Cancer, and All-Cause Mortality: A Systematic Review and Dose-Response Meta-Analysis of Prospective Studies. Am. J. Clin. Nutr. 2018, 108, 1069–1091. [Google Scholar] [CrossRef]
- Sharma, S. Development and Use of Ffq among Adults in Diverse Settings across the Globe. Proc. Nutr. Soc. 2011, 70, 232–251. [Google Scholar] [CrossRef]
- Day, N.E.; McKeown, N.; Wong, M.; Welch, A.; Bingham, S. Epidemiological Assessment of Diet: A Comparison of a 7-Day Diary with a Food Frequency Questionnaire Using Urinary Markers of Nitrogen, Potassium and Sodium. Int. J. Epidemiol. 2001, 30, 309–317. [Google Scholar] [CrossRef]
- Willett, W. Nutritional Epidemiology; Oxford University Press: Oxford, UK, 2012. [Google Scholar]
- York, E. (Ed.) Nutritional Epidemiology, 2nd ed.; Oxford University Press: Oxford, UK, 1998. [Google Scholar]
- Henríquez-Sánchez, P.; Sánchez-Villegas, A.; Doreste-Alonso, J.; Ortiz-Andrellucchi, A.; Pfrimer, K.; Serra-Majem, L. Dietary Assessment Methods for Micronutrient Intake: A Systematic Review on Vitamins. Br. J. Nutr. 2009, 102, S10–S37. [Google Scholar] [CrossRef]
- Stevens, J.; Metcalf, P.A.; Dennis, B.H.; Tell, G.S.; Shimakawa, T.; Folsom, A.R. Reliability of a Food Frequency Questionnaire by Ethnicity, Gender, Age and Education. Nutr. Res. 1996, 16, 735–745. [Google Scholar] [CrossRef]
- Shim, J.-S.; Oh, K.; Kim, H.C. Dietary Assessment Methods in Epidemiologic Studies. Epidemiol. Health 2014, 36, e2014009. [Google Scholar] [CrossRef]
- Bijani, A.; Esmaili, H.; Ghadimi, R.; Babazadeh, A.; Rezaei, R.; Cumming, R.G.; Hosseini, S.R. Development and Validation of a Semi-Quantitative Food Frequency Questionnaire among Older People in North of Iran. Casp. J. Intern. Med. 2018, 9, 78–86. [Google Scholar]
- Dehghan, M.; Al-Hamad, N.; McMillan, C.R.; Prakash, P.; Merchant, A.T. Comparison of a Semi-Quantitative Food Frequency Questionnaire with 24-Hour Dietary Recalls to Assess Dietary Intake of Adult Kuwaitis. Saudi Med. J. 2009, 30, 159–161. [Google Scholar]
- Gosadi, I.M.; Alatar, A.A.; Otayf, M.M.; AlJahani, D.M.; Ghabbani, H.M.; AlRajban, W.A.; Alrsheed, A.M.; Al-Nasser, K.A. Development of a Saudi Food Frequency Questionnaire and Testing Its Reliability and Validity. Saudi Med. J. 2017, 38, 636–641. [Google Scholar] [CrossRef]
- Hamdan, M.; Monteagudo, C.; Lorenzo-Tovar, M.-L.; Tur, J.-A.; Olea-Serrano, F.; Mariscal-Arcas, M. Development and Validation of a Nutritional Questionnaire for the Palestine Population. Public Health Nutr. 2013, 17, 2512–2518. [Google Scholar] [CrossRef]
- Malekshah, A.F.; Kimiagar, M.; Saadatian-Elahi, M.; Pourshams, A.; Nouraie, M.; Goglani, G.; Hoshiarrad, A.; Sadatsafavi, M.; Golestan, B.; Yoonesi, A.; et al. Validity and Reliability of a New Food Frequency Questionnaire Compared to 24 H Recalls and Biochemical Measurements: Pilot Phase of Golestan Cohort Study of Esophageal Cancer. Eur. J. Clin. Nutr. 2006, 60, 971–977. [Google Scholar] [CrossRef]
- Tayyem, R.F.; AbuMweis, S.S.; Bawadi, H.A.; Agraib, L.; Bani-Hani, K. Validation of a Food Frequency Questionnaire to Assess Macronutrient and Macronutrient Intake among Jordanians. Acad. Nutr. Diet. 2014, 114, 1046–1052. [Google Scholar]
- Naja, F.; Nasreddine, L.; Itani, L.; Chamieh, M.C.; Adra, N.; Sibai, A.M.; Hwalla, N. Dietary Patterns and Their Association with Obesity and Sociodemographic Factors in a National Sample of Lebanese Adults. Public Health Nutr. 2011, 14, 1570–1578. [Google Scholar] [CrossRef]
- Naja, F.; Hwalla, N.; Itani, L.; Baalbaki, S.; Sibai, A.; Nasreddine, L. A Novel Mediterranean Diet Index from Lebanon: Comparison with Europe. Eur. J. Nutr. 2014, 54, 1229–1243. [Google Scholar] [CrossRef]
- WHO. Technical Paper: Regional Strategy on Nutrition 2010–2019. Available online: http://applications.emro.who.int/docs/EM_RC57_4_en.pdf (accessed on 7 February 2019).
- Jomaa, L.; Hwalla, N.; Itani, L.; Chamieh, M.C.; Sibai, A.; Naja, F. A Lebanese Dietary Pattern Promotes Better Diet Quality among Older Adults: Findings from a National Cross-Sectional Study. BMC Geriatr. 2016, 16, 85. [Google Scholar] [CrossRef]
- Naja, F.; Nasreddine, L.; Itani, L.; Adra, N.; Sibai, A.M.; Hwalla, N. Association between Dietary Patterns and the Risk of Metabolic Syndrome among Lebanese Adults. Eur. J. Nutr. 2011, 52, 97–105. [Google Scholar] [CrossRef]
- WHO. Noncommunicable Diseases Country Profiles 2014. Available online: https://apps.who.int/iris/bitstream/handle/10665/128038/9789241507509_eng.pdf (accessed on 7 February 2019).
- AUB. Aub—Facts and Figures. American University of Beirut. Available online: http://www.aub.edu.lb/main/about/Pages/facts.aspx (accessed on 7 January 2016).
- Waterbury, J. Going Outside Aub’s Walls. Available online: https://www.aub.edu.lb/president/Documents/speeches/2007/opening-ceremony-07.pdf (accessed on 7 February 2019).
- Nasreddine, L.; Naja, F.; Chamieh, M.C.; Adra, N.; Sibai, A.-M.; Hwalla, N. Trends in Overweight and Obesity in Lebanon: Evidence from Two National Cross-Sectional Surveys (1997 and 2009). BMC Public Health 2012, 12, 798. [Google Scholar] [CrossRef]
- Dehghan, M.; Al Hamad, N.; Yusuf, S.; Nusrath, F.; Yusuf, S.; Merchant, A.T. Development of a Semi-Quantitative Food Frequency Questionnaire for Use in United Arab Emirates and Kuwait Based on Local Foods. Nutr. J. 2005, 4, 18. [Google Scholar] [CrossRef]
- Gunes, F.E.; Imeryuz, N.; Akalin, A.; Bekiroglu, N.; Alphan, E.; Oguz, A.; Dehghan, M. Development and Validation of a Semi-Quantitative Food Frequency Questionnaire to Assess Dietary Intake in Turkish Adults. J. Pak. Med. Assoc. 2015, 65, 756–763. [Google Scholar]
- Posner, B.M.; Smigelski, C.; Duggal, A.; Morgan, J.L.; Cobb, J.; Cupples, L.A. Validation of Two-Dimensional Models for Estimation of Portion Size in Nutrition Research. J. Am. Diet. Assoc. 1992, 92, 738–741. [Google Scholar]
- Bingham, S.A.; Gill, C.; Welch, A.; Day, K.; Cassidy, A.; Khaw, K.T.; Sneyd, M.J.; Key, T.J.A.; Roe, L.; Day, N.E. Comparison of Dietary Assessment Methods in Nutritional Epidemiology: Weighed Records V. 24 H Recalls, Food-Frequency Questionnaires and Estimated-Diet Records. Br. J. Nutr. 1994, 72, 619–643. [Google Scholar] [CrossRef]
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The Us Department of Agriculture Automated Multiple-Pass Method Reduces Bias in the Collection of Energy Intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [CrossRef]
- Nancy, R.; Perloff, B.; Ingwersen, L.; Steinfeldt, L.; Anand, J. An Overview of Usda’s Dietary Intake Data System. J. Food Compos. Anal. 2004, 17, 545–555. [Google Scholar]
- De Roos, A.J.; Arab, L.; Renner, J.B.; Craft, N.; Luta, G.; Helmick, C.G.; Hochberg, M.C.; Jordan, J.M. Serum Carotenoids and Radiographic Knee Osteoarthritis: The Johnston County Osteoarthritis Project. Public Health Nutr. 2001, 4, 935–942. [Google Scholar] [CrossRef][Green Version]
- WHO. Multicentre Growth Reference Study, and Mercedes de Onis. Reliability of Anthropometric Measurements in the Who Multicentre Growth Reference Study. Acta Paediatr. 2006, 95, 38–46. [Google Scholar]
- Naja, F.; Jomaa, L.; Itani, L.; Zidek, J.; El Labban, S.; Sibai, A.; Hwalla, N. Environmental Footprints of Food Consumption and Dietary Patterns among Lebanese Adults: A Cross-Sectional Study. Nutr. J. 2018, 17, 85. [Google Scholar] [CrossRef]
- Melki, I.S.; Beydoun, H.A.; Khogali, M.; Tamim, H.; Yunis, K.A. Household Crowding Index: A Correlate of Socioeconomic Status and Inter-Pregnancy Spacing in an Urban Setting. J. Epidemiol. Community Health 2004, 58, 476–480. [Google Scholar] [CrossRef]
- Nasreddine, L.; Naja, F.; Akl, C.; Chamieh, M.C.; Karam, S.; Sibai, A.-M.; Hwalla, N. Dietary, Lifestyle and Socio-Economic Correlates of Overweight, Obesity and Central Adiposity in Lebanese Children and Adolescents. Nutrients 2014, 6, 1038–1062. [Google Scholar] [CrossRef]
- Naja, F.; Hwalla, N.; Fossian, T.; Zebian, D.; Nasreddine, L. Validity and Reliability of the Arabic Version of the Household Food Insecurity Access Scale in Rural Lebanon. Public Health Nutr. 2014, 18, 251–258. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Helou, K.; El Helou, N.; Mahfouz, M.; Mahfouz, Y.; Salameh, P.; Harmouche-Karaki, M. Validity and Reliability of an Adapted Arabic Version of the Long International Physical Activity Questionnaire. BMC Public Health 2017, 18, 1–8. [Google Scholar] [CrossRef]
- Cade, J.; Thompson, R.; Burley, V.; Warm, D. Development, Validation and Utilisation of Food-Frequency Questionnaires—A Review. Public Health Nutr. 2002, 5, 567–587. [Google Scholar] [CrossRef]
- Goldberg, G.R.; Black, A.E.; Jebb, S.A.; Cole, T.J.; Murgatroyd, P.R.; Coward, W.A.; Prentice, A.M. Critical Evaluation of Energy Intake Data Using Fundamental Principles of Energy Physiology: 1. Derivation of Cut-Off Limits to Identify under-Recording. Eur. J. Clin. Nutr. 1991, 45, 569–581. [Google Scholar]
- Bland, J.M.; Altman, D. Altman. Statistical Methods for Assessing Agreement between Two Methods of Clinical Measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Nebeling, L.C.; Forman, M.R.; Graubard, B.I.; Snyder, R.A. The Impact of Lifestyle Characteristics on Carotenoid Intake in the United States: The 1987 National Health Interview Survey. Am. J. Public Health 1997, 87, 268–271. [Google Scholar] [CrossRef][Green Version]
- Forman, M.R.; Zhang, J.; Gunter, E.; Yao, S.X.; Gross, M.; Qiao, Y.-L.; Graubard, B.I.; Taylor, P.R.; Keith, S.; Maher, M. Season-Specific Correlation between Dietary Intake of Fruits and Vegetables and Levels of Serum Biomarkers among Chinese Tin Miners at High Risk for Lung Cancer. Ann. N. Y. Acad. Sci. 1999, 889, 230–239. [Google Scholar] [CrossRef]
- Freedman, L.S.; Midthune, D.; Arab, L.; Prentice, R.L.; Subar, A.F.; Willett, W.; Neuhouser, M.L.; Tinker, L.E.; Kipnis, V. Combining a Food Frequency Questionnaire with 24-Hour Recalls to Increase the Precision of Estimation of Usual Dietary Intakes-Evidence from the Validation Studies Pooling Project. Am. J. Epidemiol. 2018, 187, 2227–2232. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159. [Google Scholar] [CrossRef] [PubMed]
- Kabagambe, E.K.; Baylin, A.; Allan, D.A.; Siles, X.; Spiegelman, N.; Campos, H. Spiegelman, and H. Campos. Application of the Method of Triads to Evaluate the Performance of Food Frequency Questionnaires and Biomarkers as Indicators of Long-Term Dietary Intake. Am. J. Epidemiol. 2001, 154, 1126–1135. [Google Scholar] [CrossRef]
- Athanasiadou, E.; Kyrkou, C.; Fotiou, M.; Tsakoumaki, F.; Dimitropoulou, A.; Polychroniadou, E.; Menexes, G.; Athanasiadis, A.P.; Biliaderis, C.G.; Michaelidou, A.-M. Michaelidou. Development and Validation of a Mediterranean Oriented Culture-Specific Semi-Quantitative Food Frequency Questionnaire. Nutrients 2016, 8, 522. [Google Scholar] [CrossRef]
- Hebert, J.R.; Gupta, P.C.; Bhonsle, R.B.; Sinor, P.N.; Mehta, H.; Mehta, F.S. Development and Testing of a Quantitative Food Frequency Questionnaire for Use in Gujarat, India. Public Health Nutr. 1999, 2, 39–50. [Google Scholar] [CrossRef]
- Jackson, M.; Walker, S.; Cade, J.; Forrester, T.; Cruickshank, J.K.; Wilks, R. Reproducibility and Validity of a Quantitative Food-Frequency Questionnaire among Jamaicans of African Origin. Public Health Nutr. 2001, 4, 971–980. [Google Scholar] [CrossRef] [PubMed]
- Yuan, C.; Spiegelman, D.; Rimm, E.B.; Rosner, B.A.; Stampfer, M.J.; Barnett, J.B.; Chavarro, J.E.; Subar, A.F.; Sampson, L.K.; Willett, W.C. Validity of a Dietary Questionnaire Assessed by Comparison with Multiple Weighed Dietary Records or 24-Hour Recalls. Am. J. Epidemiol. 2017, 185, 570–584. [Google Scholar] [CrossRef] [PubMed]
- Jackson, M.D.; Motswagole, B.S.; Kwape, L.D.; Kobue-Lekalake, R.I.; Rakgantswana, T.B.; Mongwaketse, T.; Mokotedi, M.; Jackson-Malete, J. Validation and Reproducibility of an Ffq for Use among Adults in Botswana. Public Health Nutr. 2012, 16, 1995–2004. [Google Scholar] [CrossRef]
- Sichieri, R.; Everhart, J. Validity of a Brazilian Food Frequency Questionnaire against Dietary Recalls and Estimated Energy Intake. Nutr. Res. 1998, 18, 1649–1659. [Google Scholar] [CrossRef]
- Fernandez-Ballarth, J.; Pinol, J.; Josep, L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martinez-Gonzalez, M.; Salas-Salvado, J.; et al. Relative Validity of a Semi-Quantitative Food-Frequency Questionnaire in an Elderly Mediterranean Population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef] [PubMed]
- Hodge, A.M.; Simpson, J.A.; Fridman, M.; Rowley, K.; English, D.R.; Giles, G.G.; Su, Q.; O’Dea, K. Evaluation of an Ffq for Assessment of Antioxidant Intake Using Plasma Biomarkers in an Ethnically Diverse Population. Public Health Nutr. 2009, 12, 2438–2447. [Google Scholar] [CrossRef]
- Yuan, C.; Spiegelman, D.; Rimm, E.B.; Rosner, B.A.; Stampfer, M.J.; Barnett, J.B.; Chavarro, J.E.; Rood, J.C.; Harnack, L.J.; Sampson, L.K.; et al. Relative Validity of Nutrient Intakes Assessed by Questionnaire, 24-Hour Recalls, and Diet Records as Compared with Urinary Recovery and Plasma Concentration Biomarkers: Findings for Women. Am. J. Epidemiol. 2017, 187, 1051–1063. [Google Scholar] [CrossRef] [PubMed]
- Aoun, C.; Daher, R.B.; El Osta, N.; Papazian, T.; Khabbaz, L.R. Reproducibility and Relative Validity of a Food Frequency Questionnaire to Assess Dietary Intake of Adults Living in a Mediterranean Country. PLoS ONE 2019, 14, e0218541. [Google Scholar] [CrossRef]
- Harmouche-Karaki, M.; Mahfouz, M.; Obeyd, J.; Salameh, P.; Mahfouz, Y.; Helou, K. Development and Validation of a Quantitative Food Frequency Questionnaire to Assess Dietary Intake among Lebanese Adults. Nutr. J. 2020, 19, 1–19. [Google Scholar] [CrossRef]
- Masson, L.F.; McNeill, G.; Tomany, J.O.; Simpson, J.A.; Peace, H.S.; Wei, L.; Grubb, D.A.; Bolton-Smith, C. Statistical Approaches for Assessing the Relative Validity of a Food-Frequency Questionnaire: Use of Correlation Coefficients and the Kappa Statistic. Public Health Nutr. 2003, 6, 313–321. [Google Scholar] [CrossRef]
- Collins, C.E.; Boggess, M.M.; Watson, J.F.; Guest, M.; Duncanson, K.; Pezdirc, K.; Rollo, M.E.; Hutchesson, M.J.; Burrows, T.L. Reproducibility and Comparative Validity of a Food Frequency Questionnaire for Australian Adults. Clin. Nutr. 2014, 33, 906–914. [Google Scholar] [CrossRef]
- Teufel-Shone, N.I. Development of Culturally Competent Food-Frequency Questionnaires. Am. J. Clin. Nutr. 1997, 65, 1173S–1178S. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristic a | Total (N = 107) | Provided Blood Sample | p-Value c | |
|---|---|---|---|---|
| Yes (n = 67) | No (n = 40) | |||
| Age (years) b | 38.4 ± 0.9 | 38.5 ± 1.1 | 38.3 ± 9.5 | 0.899 |
| Male | 65(60.7) | 50(74.6) | 15(37.5) | 0.000 |
| Female | 42(39.2) | 17(25.4) | 25(62.5) | |
| Residents outside Beirut | 59(55.1) | 43(64.2) | 16(40.0) | 0.015 |
| Married | 60 (56.1) | 41(61.2) | 19(47.5) | 0.167 |
| Education level | ||||
| Up to intermediate level | 24(22.4) | 18(26.9) | 6(15.0) | 0.209 |
| High school | 14(13.1) | 10(14.9) | 4(10.0) | |
| University/technical diploma | 69(64.5) | 39(58.2) | 30(75.0) | |
| Non-academic employment | 91(85.0) | 59(88.1) | 32(80.0) | 0.258 |
| Monthly income ≥USD 2000 | 55(51.4) | 29(43.3) | 26(65.0) | 0.030 |
| Crowding index ≥1 individual/room | 56(52.3) | 41(61.2) | 15(37.5) | 0.018 |
| Current smoker | 58(54.2) | 43(64.2) | 15(37.5) | 0.007 |
| Physical activity level | ||||
| Low | 26(24.3) | 14(20.9) | 12(30.0) | 0.432 |
| Moderate | 69(64.5) | 44(65.7) | 25(62.5) | |
| High | 12(11.2) | 9(13.4) | 3(7.5) | |
| Body Mass Index (kg/m2) | ||||
| Normal (18.5–24.9) | 29(27.1) | 8(11.9) | 21(52.5) | 0.000 |
| Overweight (25.0–29.9) | 42(39.3) | 34(50.7) | 8(20.0) | |
| Obese (≥30) | 36(33.6) | 25(37.3) | 11(27.5) | |
| Number of 24-HRs completed during the study | ||||
| 8 | 4(3.7) | 2(3.0) | 2(5.0) | 0.678 |
| 9 | 17(15.9) | 9(13.4) | 8(20.0) | |
| 10 | 23(21.5) | 16(23.9) | 7(17.5) | |
| 11 | 48(44.9) | 32(47.8) | 16(40.0) | |
| 12 | 15(14.0) | 8(11.9) | 7(17.5) | |
| Nutrient | FFQ-2 | 24-HRs | FFQ-2 vs. 24-HRs |
|---|---|---|---|
| Mean ± SD a | Mean ± SD a | Spearman’s r b | |
| Energy (kcal) | 2538.5 ± 1065.5 | 1992.7 ± 612.5 | 0.65 ** |
| Proteins (g) | 93.5 ± 51.8 | 74.7 ± 26.8 | 0.34 ** |
| Carbohydrate (g) | 280.4 ± 132.9 | 216.9 ± 74.5 | 0.44 ** |
| Fiber, Total (g) | 23.6 ± 11.0 | 18.3 ± 6.7 | 0.55 ** |
| Fat, Total (g) | 113.2 ± 52.1 | 90.1 ± 29.5 | 0.45 ** |
| Cholesterol (mg) | 305.1 ± 363.5 | 236.5 ± 148.3 | 0.44 ** |
| Vitamin A (RAE) | 564.8 ± 670.6 | 655.7 ± 568.8 | 0.29 * |
| α-tocopherol (mg) | 14.3 ± 7.4 | 10.2 ± 4.4 | 0.52 ** |
| α-carotene (μg) | 77.3 ± 47.3 | 415.9 ± 510.4 | 0.17 |
| β-carotene (μg) | 1963.5 ± 1221.5 | 3630.6 ± 2196.2 | 0.29 * |
| Lutein+Zeaxanthin | 1703.9 ± 1469.3 | 2318.6 ± 2246.0 | 0.24 * |
| β-cryptoxanthin | 151.0 ± 127.6 | 120.3 ± 123.8 | 0.23 * |
| Lycopene | 2194.3 ± 1278.8 | 3240.8 ± 1837.7 | 0.18 |
| Total carotenoids | 6068.8 ± 3554.2 | 9726.1 ± 3554.2 | 0.22 * |
| Nutrient | Plasma Biomarkers (µg/mL) | 24-HRs (µg) ⁱ | FFQ-2 (µg) ⁱ | Plasma Biomarkers vs. 24-HRs | Plasma Biomarkers vs. FFQ-2 | ||
|---|---|---|---|---|---|---|---|
| Mean ± SD | r 1 | r 2 | r 1 | r 2 | |||
| α-carotene | 0.07 ± 0.04 | 368.10 ± 520.76 | 83.78 ± 54.46 | 0.23 | 0.37 ** | 0.35 ** | 0.38 ** |
| β-carotene b | 0.32 ± 0.13 | 3415.57 ± 2064.03 | 2128.01 ± 1390.64 | 0.39 ** | 0.46 ** | 0.55 ** | 0.59 ** |
| Lutein+Zeaxanthin | 0.40 ± 0.14 | 2024.59 ± 1384.79 | 1925.19 ± 1734.62 | 0.22 | 0.18 | 0.40 ** | 0.34 ** |
| β-cryptoxanthin | 0.13 ± 0.09 | 108.54 ± 115.73 | 163.94 ±146.34 | 0.41 ** | 0.36 ** | 0.37 ** | 0.29 * |
| Lycopene a | 0.38 ± 0.12 | 3178.56 ± 1838.48 | 2382.33 ± 1499.60 | 0.15 | 0.13 | 0.21 | 0.24 |
| Vitamin A d | 0.58 ± 0.16 | 680.39 ± 605.29 | 653.60 ± 822.29 | −0.09 | −0.09 | 0.04 | 0.15 |
| Nutrient | Plasma Biomarker (µg/mL) | Fall 24-HRs | Fall 24-HRs and FFQ-2 ⁱ | Plasma Biomarkers vs. Fall 24-HRs | Plasma Biomarkers vs. Fall 24-HRs and FFQ-2 | ||
|---|---|---|---|---|---|---|---|
| Mean ± SD | r 1 | r 2 | r 1 | r 2 | |||
| α-carotene | 0.07 ± 0.04 | 368.73 ± 931.58 | 226.25 ± 475.53 | 0.29 * | 0.27 * | 0.31 * | 0.46 ** |
| β-carotene b | 0.32 ± 0.13 | 3364.09 ± 3303.89 | 2746.05 ± 1991.15 | 0.25 * | 0.26 * | 0.42 ** | 0.47 ** |
| Lutein+Zeaxanthin | 0.40 ± 0.14 | 2208.02 ± 2880.18 | 2066.61 ± 1797.02 | 0.24 | 0.19 | 0.37 ** | 0.30 * |
| β-cryptoxanthin | 0.13 ± 0.09 | 119.91 ± 201.83 | 141.93 ± 139.78 | 0.31 * | 0.27 * | 0.38 ** | 0.27 * |
| Lycopene a | 0.38 ± 0.12 | 2597.29 ± 2739.25 | 2489.82 ± 1765.30 | 0.16 | 0.18 | 0.25 * | 0.32 ** |
| Vitamin A d | 0.58 ± 0.16 | 789.62 ± 1475.13 | 721.61 ± 845.18 | −0.16 | −0.09 | −0.01 | 0.04 |
| Nutrients | FFQ-1 | FFQ-2 | FFQ-1 vs. FFQ-2 | ||
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | ICC # | Weighted Kappa | Same and Adjacent % Agreement | |
| Energy (kcal) | 3061.8 ± 1479.4 | 2538.5 ± 1066.5 | 0.85 ** | 0.56 | 95.3 |
| Protein (g) | 112.2 ± 59.8 | 93.5 ± 51.8 | 0.44 * | 0.56 | 92.5 |
| Carbohydrate(g) | 345.6 ± 178.0 | 280.4 ± 132.9 | 0.56 ** | 0.51 | 90.7 |
| Fiber, Total(g) | 27.4 ± 12.9 | 23.6 ± 11.0 | 0.64 ** | 0.50 | 85.1 |
| Fat, Total(g) | 134.1 ± 67.4 | 113.2 ± 52.1 | 0.67 ** | 0.49 | 89.7 |
| Cholesterol(mg) | 345.4 ± 298.7 | 305.1 ± 363.5 | 0.55 ** | 0.46 | 85.1 |
| α-Tocopherol(mg) | 16.0 ± 8.6 | 14.3 ± 7.4 | 0.56 ** | 0.39 | 86.0 |
| Vitamin A (RAE) | 694.1 ± 786.9 | 564.8 ± 670.6 | 0.44 ** | 0.40 | 85.1 |
| α-carotene(μg) | 93.0 ± 60.7 | 77.3 ± 47.3 | 0.62 ** | 0.36 | 82.2 |
| β-carotene(μg) | 2328.4 ± 1333.4 | 1963.5 ± 1221.5 | 0.58 ** | 0.36 | 84.1 |
| Lutein+Zeaxanthin | 2116.1 ± 1762.7 | 1703.9 ± 1469.3 | 0.36 * | 0.25 | 74.8 |
| β-cryptoxanthin | 210.8 ± 157.2 | 151.0 ± 127.6 | 0.70 ** | 0.38 | 80.4 |
| Lycopene | 3180.3 ± 3151.1 | 2194.3 ± 1287.8 | 0.63 ** | 0.32 | 82.2 |
| Total Carotenoids | 7861.0 ± 5135.3 | 6068.8 ± 3554.2 | 0.53 ** | 0.33 | 80.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
El Sayed Ahmad, R.; Baroudi, M.; Shatila, H.; Nasreddine, L.; Chokor, F.A.Z.; Chehab, R.F.; Forman, M.R.; Naja, F. Validity and Reproducibility of a Culture-Specific Food Frequency Questionnaire in Lebanon. Nutrients 2020, 12, 3316. https://doi.org/10.3390/nu12113316
El Sayed Ahmad R, Baroudi M, Shatila H, Nasreddine L, Chokor FAZ, Chehab RF, Forman MR, Naja F. Validity and Reproducibility of a Culture-Specific Food Frequency Questionnaire in Lebanon. Nutrients. 2020; 12(11):3316. https://doi.org/10.3390/nu12113316
Chicago/Turabian StyleEl Sayed Ahmad, Raeda, Mariam Baroudi, Hibeh Shatila, Lara Nasreddine, Fatima Al Zahraa Chokor, Rana F. Chehab, Michele R. Forman, and Farah Naja. 2020. "Validity and Reproducibility of a Culture-Specific Food Frequency Questionnaire in Lebanon" Nutrients 12, no. 11: 3316. https://doi.org/10.3390/nu12113316
APA StyleEl Sayed Ahmad, R., Baroudi, M., Shatila, H., Nasreddine, L., Chokor, F. A. Z., Chehab, R. F., Forman, M. R., & Naja, F. (2020). Validity and Reproducibility of a Culture-Specific Food Frequency Questionnaire in Lebanon. Nutrients, 12(11), 3316. https://doi.org/10.3390/nu12113316