Negative Affectivity and Emotion Dysregulation as Mediators between ADHD and Disordered Eating: A Systematic Review

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
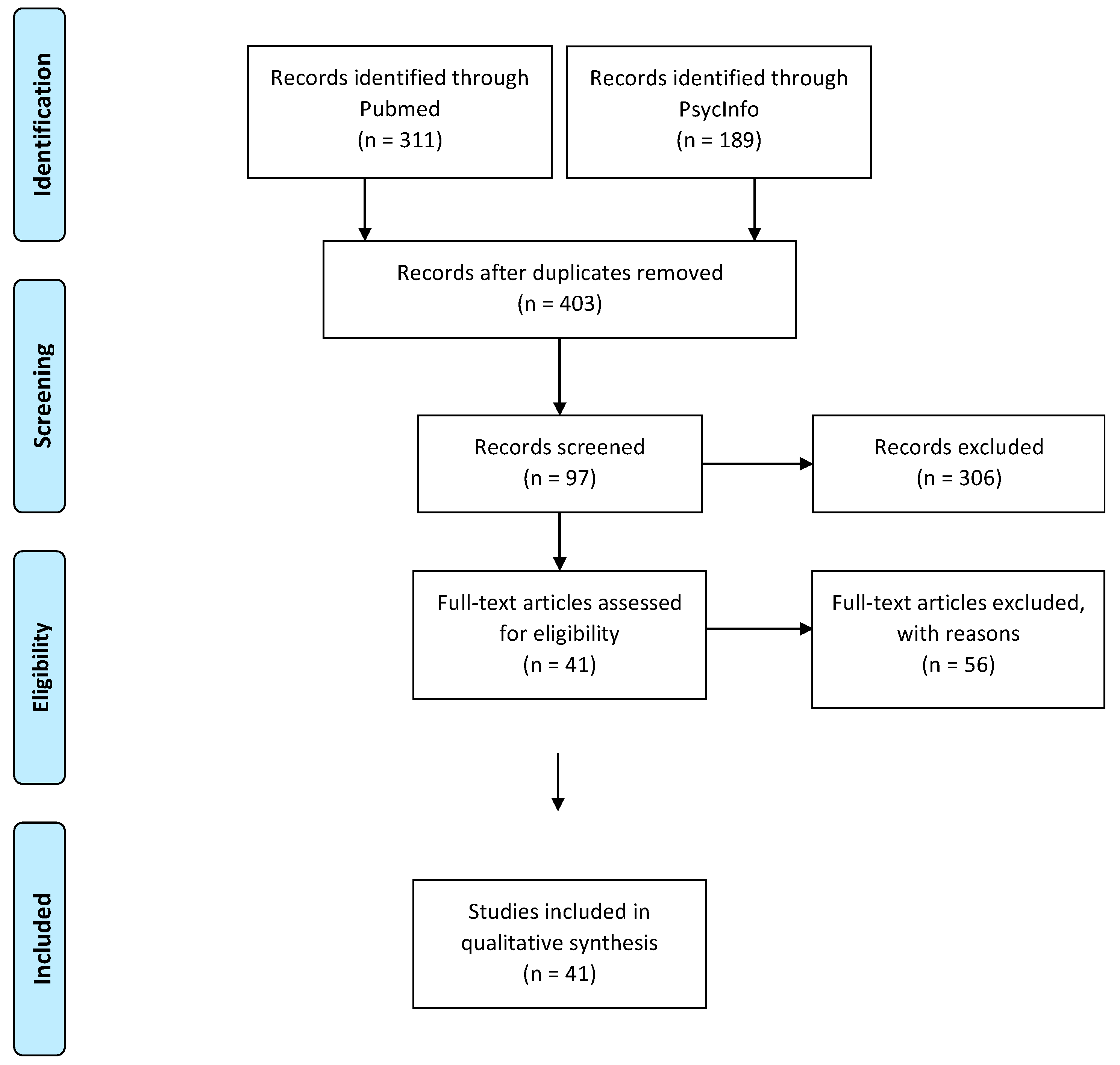
2.1. Literature Search
2.2. Data Extraction
3. Results
- -
- -
- -
- -
- -
- No access to full text (n = 1) [102]
3.1. Article Characteristics
3.1.1. Country of Investigation
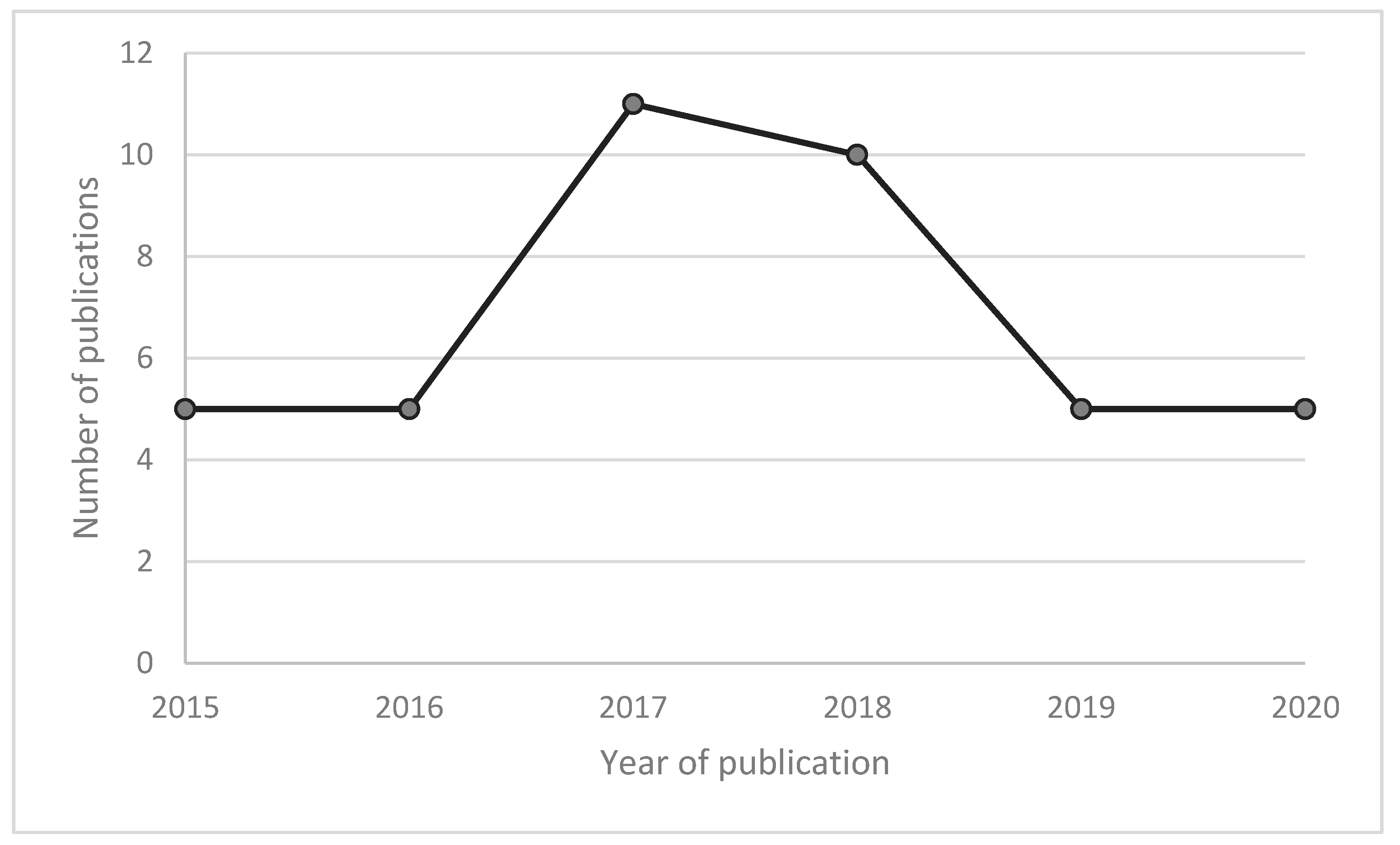
3.1.2. Year of Publication
3.1.3. Study Design
3.1.4. Age of Interest
3.1.5. Population
3.1.6. ADHD Assessment and Medication
3.1.7. Disordered Eating Assessment Tools
3.2. Association between ADHD and Disordered Eating
3.2.1. Prevalence of Disordered Eating in Individuals with ADHD
Children and Adolescents
Adults
3.2.2. Prevalence of ADHD in Individuals with Disordered Eating
Children and Adolescents
Adults
3.2.3. ADHD and Disordered Eating
Children and Adolescents
Adults
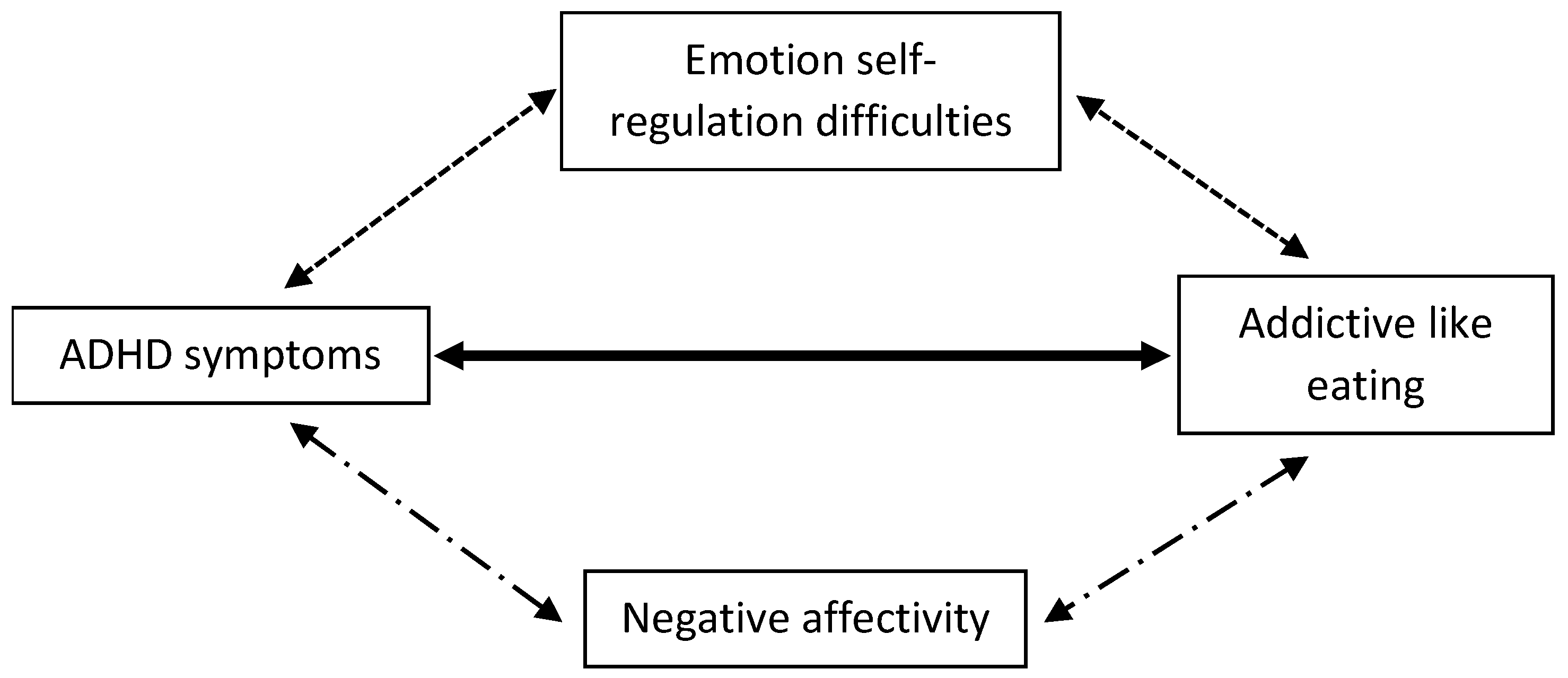
3.3. Indirect Association between ADHD and Disordered Eating through Negative Affectivity and Disrupted Emotion Self-Regulation
3.3.1. ADHD, Negative Affectivity, and Disrupted Emotion Self-Regulation
Children and Adolescents
Adults
3.3.2. Negative Affectivity and Disrupted Emotion Self-Regulation as Mediators in the Association between ADHD and Disordered Eating
Children and Adolescents
Adults
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kooij, J.J.S.; Bijlenga, D.; Salerno, L.; Jaeschke, R.; Bitter, I.; Balázs, J.; Thome, J.; Dom, G.; Kasper, S.; Nunes Filipe, C.; et al. Updated European Consensus Statement on diagnosis and treatment of adult ADHD. Eur. Psychiatry 2019, 56, 14–34. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.; Sanders, S.; Doust, J.; Beller, E.; Glasziou, P. Prevalence of attention-deficit/hyperactivity disorder: A systematic review and meta-analysis. Pediatrics 2015, 135, e994-e1001. [Google Scholar] [CrossRef] [PubMed]
- Polanczyk, G.; De Lima, M.S.; Horta, B.L.; Biederman, J.; Rohde, L.A. The worldwide prevalence of ADHD: A systematic review and metaregression analysis. Am. J. Psychiatry 2007, 164, 942–948. [Google Scholar] [CrossRef] [PubMed]
- Faraone, S.V.; Biederman, J.; Mick, E. The age-dependent decline of attention deficit hyperactivity disorder: A meta-analysis of follow-up studies. Psychol. Med. 2006, 36, 159–165. [Google Scholar] [CrossRef]
- Cortese, S.; Adamo, N.; Del Giovane, C.; Mohr-Jensen, C.; Hayes, A.J.; Carucci, S.; Atkinson, L.Z.; Tessari, L.; Banaschewski, T.; Coghill, D.; et al. Comparative efficacy and tolerability of medications for attention-deficit hyperactivity disorder in children, adolescents, and adults: A systematic review and network meta-analysis. The Lancet Psychiatry 2018, 5, 727–738. [Google Scholar] [CrossRef]
- Daley, D.; Van Der Oord, S.; Ferrin, M.; Cortese, S.; Danckaerts, M.; Doepfner, M.; Van Den Hoofdakker, B.J.; Coghill, D.; Thompson, M.; Asherson, P.; et al. Practitioner review: Current best practice in the use of parent training and other behavioural interventions in the treatment of children and adolescents with attention deficit hyperactivity disorder. J. Child Psychol. Psychiatry Allied Discip. 2017, 59, 932–947. [Google Scholar] [CrossRef]
- Cortese, S.; Moreira-Maia, C.R.; St Fleur, D.; Morcillo-Peñalver, C.; Rohde, L.A.; Faraone, S.V. Association between ADHD and obesity: A systematic review and meta-analysis. Am. J. Psychiatry 2016, 173, 34–43. [Google Scholar] [CrossRef]
- Nigg, J.T.; Johnstone, J.M.; Musser, E.D.; Long, H.G.; Willoughby, M.; Shannon, J. Attention-deficit/hyperactivity disorder (ADHD) and being overweight/obesity: New data and meta-analysis. Clin. Psychol. Rev. 2016, 43, 67–79. [Google Scholar] [CrossRef]
- Nazar, B.P.; de Sousa Pinna, C.M.; Suwwan, R.; Duchesne, M.; Freitas, S.R.; Sergeant, J.; Mattos, P. ADHD Rate in Obese Women with Binge Eating and Bulimic Behaviors from a Weight-Loss Clinic. J. Atten. Disord. 2016, 20, 610–616. [Google Scholar] [CrossRef]
- Hilbert, A.; Kurz, S.; Dremmel, D.; Weihrauch Blüher, S.; Munsch, S.; Schmidt, R. Cue reactivity, habituation, and eating in the absence of hunger in children with loss of control eating and attention-deficit/hyperactivity disorder. Int. J. Eat. Disord. 2018, 51, 223–232. [Google Scholar] [CrossRef]
- Brunault, P.; Frammery, J.; Montaudon, P.; De Luca, A.; Hankard, R.; Ducluzeau, P.H.; Cortese, S.; Ballon, N. Adulthood and childhood ADHD in patients consulting for obesity is associated with food addiction and binge eating, but not sleep apnea syndrome. Appetite 2019, 136, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Gearhardt, A.N.; Corbin, W.R.; Brownell, K.D. Preliminary validation of the Yale Food Addiction Scale. Appetite 2009, 52, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Romo, L.; Ladner, J.; Kotbagi, G.; Morvan, Y.; Saleh, D.; Tavolacci, M.P.; Kern, L. Attention-deficit hyperactivity disorder and addictions (substance and behavioral): Prevalence and characteristics in a multicenter study in France. J. Behav. Addict. 2018, 7, 743–751. [Google Scholar] [CrossRef] [PubMed]
- Gearhardt, A.N.; Corbin, W.R.; Brownell, K.D. Development of the Yale Food Addiction Scale Version 2.0. Psychol. Addict. Behav. 2016, 30, 113–121. [Google Scholar] [CrossRef]
- Mills, J.G.; Thomas, S.J.; Larkin, T.A.; Deng, C. Overeating and food addiction in Major Depressive Disorder: Links to peripheral dopamine. Appetite 2020, 148, 104586. [Google Scholar] [CrossRef]
- Mies, G.W.; Treur, J.L.; Larsen, J.K.; Halberstadt, J.; Pasman, J.A.; Vink, J.M. The prevalence of food addiction in a large sample of adolescents and its association with addictive substances. Appetite 2017, 118, 97–105. [Google Scholar] [CrossRef]
- Mason, S.M.; Flint, A.J.; Roberts, A.L.; Agnew-Blais, J.; Koenen, K.C.; Rich-Edwards, J.W. Posttraumatic stress disorder symptoms and food addiction in women by timing and type of trauma exposure. JAMA Psychiatry 2014, 71, 1271–1278. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; ISBN 9782294743382. [Google Scholar]
- Granero, R.; Hilker, I.; Agüera, Z.; Jiménez-Murcia, S.; Sauchelli, S.; Islam, M.A.; Fagundo, A.B.; Sánchez, I.; Riesco, N.; Dieguez, C.; et al. Food Addiction in a Spanish Sample of Eating Disorders: DSM-5 Diagnostic Subtype Differentiation and Validation Data. Eur. Eat. Disorders Rev. 2014, 22, 389–396. [Google Scholar] [CrossRef]
- El Archi, S.; Brunault, P.; Ballon, N.; Réveillère, C.; Barrault, S. Differential association between food craving, food addiction and eating-related characteristics in persons at risk for eating disorders. Rev. Eur. Psychol. Appl. 2020, 7. [Google Scholar] [CrossRef]
- Maxwell, A.L.; Gardiner, E.; Loxton, N.J. Investigating the relationship between reward sensitivity, impulsivity, and food addiction: A systematic review. Eur. Eat. Disord. Rev. 2020, 22, 368–384. [Google Scholar] [CrossRef]
- Steadman, K.M.; Knouse, L.E. Is the Relationship between ADHD Symptoms and Binge Eating Mediated by Impulsivity? J. Atten. Disord. 2016, 20, 907–912. [Google Scholar] [CrossRef] [PubMed]
- Ortal, S.; van de Geurt, G.; Johan, F.; Itai, B.; Nir, Y.; Iliyan, I.; van den Wim, B. The role of different aspects of impulsivity as independent risk factors for substance use disorders in patients with ADHD: A review. Curr. Drug Abuse Rev. 2015, 8, 119–133. [Google Scholar] [CrossRef]
- Romo, L.; Rémond, J.J.; Coeffec, A.; Kotbagi, G.; Plantey, S.; Boz, F.; Kern, L.; Coeffec, Á.A.; Kotbagi, Á.G.; Plantey, Á.S.; et al. Gambling and Attention Deficit Hyperactivity Disorders (ADHD) in a Population of French Students. J Gambl. Stud. 2015, 31, 1261–1272. [Google Scholar] [CrossRef]
- Whiteside, S.P.; Lynam, D.R. The five factor model and impulsivity: Using a structural model of personality to understand impulsivity. Pers. Individ. Dif. 2001, 30, 669–689. [Google Scholar] [CrossRef]
- Egan, T.E.; Dawson, A.E.; Wymbs, B.T. Substance Use in Undergraduate Students with Histories of Attention-Deficit/Hyperactivity Disorder (ADHD): The Role of Impulsivity. Subst. Use Misuse 2017, 52, 1375–1386. [Google Scholar] [CrossRef]
- Brunault, P.; Mathieu, S.; Faussat, C.; Barrault, S.; Varescon, I. Impulsivity facets and cognitive distortions associated with problem gambling: Differences between ADHD and non-ADHD gamblers. Rev. Eur. Psychol. Appl. 2020, 70, 100559. [Google Scholar] [CrossRef]
- Van Emmerik-Van Oortmerssen, K.; Van De Glind, G.; Van Den Brink, W.; Smit, F.; Crunelle, C.L.; Swets, M.; Schoevers, R.A. Prevalence of attention-deficit hyperactivity disorder in substance use disorder patients: A meta-analysis and meta-regression analysis. Drug Alcohol Depend. 2012, 122, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Anker, E.; Bendiksen, B.; Heir, T. Comorbid psychiatric disorders in a clinical sample of adults with ADHD, and associations with education, work and social characteristics: A cross-sectional study. BMJ Open 2018, 8. [Google Scholar] [CrossRef]
- Mathews, C.L.; Morrell, H.E.R.; Molle, J.E. Video game addiction, ADHD symptomatology, and video game reinforcement. Am. J. Drug Alcohol Abuse 2019, 45, 67–76. [Google Scholar] [CrossRef]
- Evren, B.; Evren, C.; Dalbudak, E.; Topcu, M.; Kutlu, N. Relationship of internet addiction severity with probable ADHD and difficulties in emotion regulation among young adults. Psychiatry Res. 2018, 269, 494–500. [Google Scholar] [CrossRef]
- Mestre-Bach, G.; Steward, T.; Potenza, M.N.; Granero, R.; Fernández-Aranda, F.; Mena-Moreno, T.; Magaña, P.; Vintró-Alcaraz, C.; del Pino-Gutiérrez, A.; Menchón, J.M.; et al. The Role of ADHD Symptomatology and Emotion Dysregulation in Gambling Disorder. J. Atten. Disord. 2019. [Google Scholar] [CrossRef]
- Grall-Bronnec, M.; Wainstein, L.; Augy, J.; Bouju, G.; Feuillet, F.; Vénisse, J.L.; Sébille-Rivain, V. Attention deficit hyperactivity disorder among pathological and at-risk gamblers seeking treatment: A hidden disorder. Eur. Addict. Res. 2011, 17, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Young, K.S. Caught in the Net: How to Recognize the Sign of Internet Addiction and a Winning Strategy for Recovery; John Wiley & Sons: New York, NY, USA, 1998; ISBN 0471191590. [Google Scholar]
- Gross, J.J.; Thompson, R.A. Emotion Regulation: Conceptual Foundations. Available online: https://www.researchgate.net/publication/303248970_Emotion_Regulation_Conceptual_Foundations (accessed on 4 June 2020).
- Sheppes, G.; Suri, G.; Gross, J.J. Emotion Regulation and Psychopathology. Annu. Rev. Clin. Psychol. 2015, 11, 379–405. [Google Scholar] [CrossRef] [PubMed]
- Corbisiero, S.; Stieglitz, R.D.; Retz, W.; Rösler, M. Is emotional dysregulation part of the psychopathology of ADHD in adults? ADHD Atten. Deficit Hyperact. Disord. 2013, 5, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Fox, H.C.; Axelrod, S.R.; Paliwal, P.; Sleeper, J.; Sinha, R. Difficulties in emotion regulation and impulse control during cocaine abstinence. Drug Alcohol Depend. 2007, 89, 298–301. [Google Scholar] [CrossRef] [PubMed]
- Prefit, A.-B.; Mirela Cândea, D.; Szentagotai-Tătar, A. Emotion regulation across eating pathology: A meta-analysis. Appetite 2019, 143, 104438. [Google Scholar] [CrossRef]
- Masi, G.; Fantozzi, P.; Muratori, P.; Bertolucci, G.; Tacchi, A.; Villafranca, A.; Pfanner, C.; Cortese, S. Emotional dysregulation and callous unemotional traits as possible predictors of short-term response to methylphenidate monotherapy in drug-naïve youth with ADHD. Compr. Psychiatry 2020, 100, 152178. [Google Scholar] [CrossRef]
- Lenzi, F.; Cortese, S.; Harris, J.; Masi, G. Pharmacotherapy of emotional dysregulation in adults with ADHD: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2018, 84, 359–367. [Google Scholar] [CrossRef] [PubMed]
- Beheshti, A.; Chavanon, M.L.; Christiansen, H. Emotion dysregulation in adults with attention deficit hyperactivity disorder: A meta-analysis. BMC Psychiatry 2020, 20, 120. [Google Scholar] [CrossRef] [PubMed]
- Seymour, K.E.; Chronis-Tuscano, A.; Iwamoto, D.K.; Kurdziel, G.; MacPherson, L. Emotion regulation mediates the association between ADHD and depressive symptoms in a community sample of youth. J. Abnorm. Child Psychol. 2014, 42, 611–621. [Google Scholar] [CrossRef]
- Bauer, B.W.; Gustafsson, H.C.; Nigg, J.; Karalunas, S.L. Working Memory Mediates Increased Negative Affect and Suicidal Ideation in Childhood Attention-Deficit/Hyperactivity Disorder. J. Psychopathol. Behav. Assess. 2018, 40, 180–193. [Google Scholar] [CrossRef] [PubMed]
- Karalunas, S.L.; Fair, D.; Musser, E.D.; Aykes, K.; Iyer, S.P.; Nigg, J.T. Subtyping attention-deficit/hyperactivity disorder using temperament dimensions: Toward biologically based nosologic criteria. JAMA Psychiatry 2014, 71, 1015–1024. [Google Scholar] [CrossRef]
- Emilsson, M.; Gustafsson, P.; Öhnström, G.; Marteinsdottir, I. Impact of personality on adherence to and beliefs about ADHD medication, and perceptions of ADHD in adolescents. BMC Psychiatry 2020, 2. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.F.; Silva, K.; Kecojevic, A.; Schrager, S.M.; Bloom, J.J.; Iverson, E.; Lankenau, S.E. Coping and emotion regulation profiles as predictors of nonmedical prescription drug and illicit drug use among high-risk young adults. Drug Alcohol Depend. 2013, 132, 165–171. [Google Scholar] [CrossRef]
- Jacobs, D.F. An overarching theory of addictions: A new paradigm for understanding and treating addictive behaviours. In Proceedings of the National Academy of Sciences Meeting, Washington, DC, USA, 27 April 1998. [Google Scholar]
- Ahn, J.S.; Min, S.; Kim, M.H. The role of uncontrolled eating and screen time in the link of attention deficit hyperactivity disorder with weight in late childhood. Psychiatry Investig. 2017, 14, 808–816. [Google Scholar] [CrossRef]
- Donnchadha, S.; Bramham, J.; Greene, C. Rethinking the association between overweight/obesity and ADHD in children: A longitudinal and psychosocial perspective. Ir. J. Psychol. Med. 2020, 1–14. [Google Scholar] [CrossRef]
- Dreber, H.; Reynisdottir, S.; Angelin, B.; Hemmingsson, E. Who is the treatment-seeking young adult with severe obesity: A comprehensive characterization with emphasis on mental health. PLoS ONE 2015, 1. [Google Scholar] [CrossRef] [PubMed]
- Eiffener, E.; Eli, K.; Ek, A.; Sandvik, P.; Somaraki, M.; Kremers, S.; Sleddens, E.; Nowicka, P. The influence of preschoolers’ emotional and behavioural problems on obesity treatment outcomes: Secondary findings from a randomized controlled trial. Pediatr. Obes. 2019, 14, e12556. [Google Scholar] [CrossRef]
- Fruchter, E.; Marom-Harel, H.; Fenchel, D.; Kapra, O.; Ginat, K.; Portuguese, S.; Weiser, M. Functioning of Young Adults with ADHD in the Military. J. Atten. Disord. 2019, 23, 1470–1474. [Google Scholar] [CrossRef]
- Goulardins, J.B.; Rigoli, D.; Piek, J.P.; Kane, R.; Palácio, S.G.; Casella, E.B.; Nascimento, R.O.; Hasue, R.H.; Oliveira, J.A. The relationship between motor skills, ADHD symptoms, and childhood body weight. Res. Dev. Disabil. 2016, 55, 279–286. [Google Scholar] [CrossRef]
- Granato, M.F.; Ferraro, A.A.; Lellis, D.M.; Casella, E.B. Associations between attention-deficit hyperactivity disorder (ADHD) treatment and patient nutritional status and height. Behav. Neurol. 2018, 2, 7341529. [Google Scholar] [CrossRef] [PubMed]
- Guenzel, N.; Schober, D.J. Psychiatric Comorbidities and BMI: An Exploratory Analysis. Issues Ment. Health Nurs. 2017, 38, 698–704. [Google Scholar] [CrossRef] [PubMed]
- Hagman, E.; Danielsson, P.; Brandt, L.; Svensson, V.; Ekbom, A.; Marcus, C. Childhood Obesity, Obesity Treatment Outcome, and Achieved Education: A Prospective Cohort Study. J. Adolesc. Health 2017, 61, 508–513. [Google Scholar] [CrossRef] [PubMed]
- Hanć, T.; Słopień, A.; Wolańczyk, T.; Szwed, A.; Czapla, Z.; Durda, M.; Dmitrzak-Węglarz, M.; Ratajczak, J. Attention-deficit/hyperactivity disorder is related to decreased weight in the preschool period and to increased rate of overweight in school-age boys. J. Child Adolesc. Psychopharmacol. 2015, 25, 691–700. [Google Scholar] [CrossRef]
- Inoue, Y.; Howard, A.G.; Stickley, A.; Yazawa, A.; Gordon-Larsen, P. Sex and racial/ethnic differences in the association between childhood attention-deficit/hyperactivity disorder symptom subtypes and body mass index in the transition from adolescence to adulthood in the United States. Pediatr. Obes. 2019, 14, e12498. [Google Scholar] [CrossRef]
- Aguirre-Castaneda, R.L.; Kumar, S.; Voigt, R.G.; Leibson, C.L.; Barbaresi, W.J.; Weaver, A.L.; Killian, J.M.; Katusic, S.K. Childhood Attention-Deficit/Hyperactivity Disorder, Sex, and Obesity: A Longitudinal Population-Based Study. Mayo Clin. Proc. 2016, 91, 352–361. [Google Scholar] [CrossRef]
- Jang, B.Y.; Bu, S.Y. Nutritional Status of Korean Children and Adolescents with Attention Deficit Hyperactivity Disorder (ADHD). Clin. Nutr. Res. 2017, 6, 112. [Google Scholar] [CrossRef]
- Kummer, A.; Barbosa, I.G.; Rodrigues, D.H.; Rocha, N.P.; Da Silva Rafael, M.; Pfeilsticker, L.; Simõese Silva, A.C.; Teixeira, A.L. Frequency of overweight and obesity in children and adolescents with autism and attention deficit/hyperactivity disorder. Rev. Paul. Pediatr. 2016, 34, 71–77. [Google Scholar] [CrossRef]
- Kwak, Y.S.; Jung, Y.E.; Kim, M.D. Prevalence and correlates of attention-deficit hyperactivity disorder symptoms in korean college students. Neuropsychiatr. Dis. Treat. 2015, 11, 797–802. [Google Scholar] [CrossRef]
- Leib, S.; Gilon Mann, T.; Stein, D.; Vusiker, I.; Tokatly Latzer, I.; Ben-Ami, M.; Feigin, A.; Dubnov-Raz, G. High prevalence of attention-deficit/hyperactivity disorder in adolescents with severe obesity seeking bariatric surgery. Acta Paediatr. Int. J. Paediatr. 2019, 109, 581–586. [Google Scholar] [CrossRef]
- Lentferink, Y.E.; Van De Garde, E.M.W.; Knibbe, C.A.J.; Van Der Vorst, M.M.J. Psychostimulants: Influence on body mass index and height in a pediatric population with attention-deficit/hyperactivity disorder? J. Child Adolesc. Psychopharmacol. 2018, 28, 530–536. [Google Scholar] [CrossRef]
- Mellström, E.; Forsman, C.; Engh, L.; Hallerbäck, M.U.; Wikström, S. Methylphenidate and Reduced Overweight in Children with ADHD. J. Atten. Disord. 2020, 24, 246–254. [Google Scholar] [CrossRef]
- Mohammadi, M.R.; Mostafavi, S.-A.; Hooshyari, Z.; Khaleghi, A.; Ahmadi, N. Body Mass Index Status across Different Psychiatric Disorders in a National Survey amongst Children and Adolescents: To Identify the Role of Gender. Iran J Psychatry 2019, 14, 253–264. [Google Scholar] [CrossRef]
- Pauli-Pott, U.; Reinhardt, A.; Bagus, E.; Wollenberg, B.; Schroer, A.; Heinzel-Gutenbrunner, M.; Becker, K. Psychosocial risk factors underlie the link between attention deficit hyperactivity symptoms and overweight at school entry. Eur. Child Adolesc. Psychiatry 2017, 26, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Bonaventura, I.; Granero, R.; Ezpeleta, L. The relationship between weight status and emotional and behavioral problems in Spanish preschool children. J. Pediatr. Psychol. 2015, 40, 455–463. [Google Scholar] [CrossRef]
- Racicka, E.; Hanć, T.; Giertuga, K.; Bryńska, A.; Wolańczyk, T. Prevalence of Overweight and Obesity in Children and Adolescents with ADHD: The Significance of Comorbidities and Pharmacotherapy. J. Atten. Disord. 2018, 22, 1095–1108. [Google Scholar] [CrossRef] [PubMed]
- Bisset, M.; Rinehart, N.; Sciberras, E. Body dissatisfaction and weight control behaviour in children with ADHD: A population-based study. Eur. Child Adolesc. Psychiatry 2019, 28, 1507–1516. [Google Scholar] [CrossRef] [PubMed]
- Sciberras, E.; Bisset, M.; Hazell, P.; Nicholson, J.M.; Anderson, V.; Lycett, K.; Jongeling, B.; Efron, D. Health-related impairments in young children with ADHD: A community-based study. Child. Care. Health Dev. 2016, 42, 709–717. [Google Scholar] [CrossRef]
- Skoglund, C.; Kopp Kallner, H.; Skalkidou, A.; Wikström, A.K.; Lundin, C.; Hesselman, S.; Wikman, A.; Sundström Poromaa, I. Association of Attention-Deficit/Hyperactivity Disorder with Teenage Birth among Women and Girls in Sweden. JAMA Netw. Open 2019, 2, e1912463. [Google Scholar] [CrossRef] [PubMed]
- Taymur, I.; Budak, E.; Onen, S.; Bicer, B.; Dilektasll, E.; Cayci, M.; Demirci, H.; Gungor, B.B. The Relationship between Childhood and Adult Attention-Deficit-Hyperactivity Disorder and General Psychop athological Features in Individuals Who Apply for Bariatric Surgery. Bariatr. Surg. Pract. Patient Care 2016, 11, 116–122. [Google Scholar] [CrossRef]
- Türkoğlu, S.; Çetin, F.H. The relationship between chronotype and obesity in children and adolescent with attention deficit hyperactivity disorder. Chronobiol. Int. 2019, 36, 1138–1147. [Google Scholar] [CrossRef]
- Van Eck, K.; Morse, M.; Flory, K. The Role of Body Image in the Link between ADHD and Depression Symptoms among College Students. J. Atten. Disord. 2018, 22, 435–445. [Google Scholar] [CrossRef] [PubMed]
- Wynchank, D.; Bijlenga, D.; Lamers, F.; Kooij, J.J.S.; Bron, T.I.; Beekman, A.T.F.; Penninx, B.W.J.H. The Association between Metabolic Syndrome, Obesity-Related Outcomes, and ADHD in Adults with Comorbid Affective Disorders. J. Atten. Disord. 2018, 22, 460–471. [Google Scholar] [CrossRef] [PubMed]
- Zhang, A.; Li, S.; Zhang, Y.; Jiang, F.; Jin, X.; Ma, J. Nocturnal enuresis in obese children: A nation-wide epidemiological study from China. Sci. Rep. 2019, 9, 8414. [Google Scholar] [CrossRef]
- Türkoğlu, S.; Bilgiç, A.; Akça, Ö.F. ADHD symptoms, breast-feeding and obesity in children and adolescents. Pediatr. Int. 2015, 57, 546–551. [Google Scholar] [CrossRef] [PubMed]
- Bowling, A.B.; Tiemeier, H.W.; Jaddoe, V.W.V.; Barker, E.D.; Jansen, P.W. ADHD symptoms and body composition changes in childhood: A longitudinal study evaluating directionality of associations. Pediatr. Obes. 2018, 13, 567–575. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Kuja-Halkola, R.; Sjölander, A.; Serlachius, E.; Cortese, S.; Faraone, S.V.; Almqvist, C.; Larsson, H. Shared familial risk factors between attention-deficit/hyperactivity disorder and overweight/obesity—A population-based familial coaggregation study in Sweden. J. Child Psychol. Psychiatry Allied Discip. 2017, 58, 711–718. [Google Scholar] [CrossRef]
- Cho, Y.J.; Choi, R.; Park, S.; Kwon, J. Parental smoking and depression, and attention-deficit hyperactivity disorder in children and adolescents: Korean national health and nutrition examination survey 2005–2014. Asia-Pac. Psychiatry 2018, 10, e12327. [Google Scholar] [CrossRef]
- Çöl, N.; Gökçen, C.; Demırcıoğlu Kiliç, B.; Karadağ, M. Prevalence of obesity/hypertension in children and adolescents with ADHD and evaluation of total body composition. Anatol. J. Psychiatry 2019, 20, 93–100. [Google Scholar] [CrossRef]
- Çolpan, M.; Eray, Ş.; Eren, E.; Vural, A.P. Perceived Expressed Emotion, Emotional and Behavioral Problems and Self-Esteem in Obese Adolescents: A Case-Control Study. J. Clin. Res. Pediatr. Endocrinol. 2018, 10, 357–363. [Google Scholar] [CrossRef]
- Cook, B.G.; Li, D.; Heinrich, K.M. Obesity, Physical Activity, and Sedentary Behavior of Youth with Learning Disabilities and ADHD. J. Learn. Disabil. 2015, 48, 563–576. [Google Scholar] [CrossRef] [PubMed]
- Corvey, K.; Menear, K.S.; Preskitt, J.; Goldfarb, S.; Menachemi, N. Obesity, Physical Activity and Sedentary Behaviors in Children with an Autism Spectrum Disorder. Matern. Child Health J. 2016, 20, 466–476. [Google Scholar] [CrossRef] [PubMed]
- Karjalainen, L.; Gillberg, C.; Råstam, M.; Wentz, E. Eating disorders and eating pathology in young adult and adult patients with ESSENCE. Compr. Psychiatry 2016, 66, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Linthavong, O.; O’Shea, T.M.; Allred, E.; Perrin, E.; Bauserman, M.; Joseph, R.M.; Leviton, A.; Heeren, T.C.; Kuban, K.C.K. Neurocognitive and Health Correlates of Overweight and Obesity among Ten-Year-Old Children Born Extremely Preterm. J. Pediatr. 2018, 200, 84–90e4. [Google Scholar] [CrossRef]
- Vitelli, O.; Tabarrini, A.; Miano, S.; Rabasco, J.; Pietropaoli, N.; Forlani, M.; Parisi, P.; Villa, M.P. Impact of obesity on cognitive outcome in children with sleep-disordered breathing. Sleep Med. 2015, 16, 625–630. [Google Scholar] [CrossRef]
- Bleck, J.R.; DeBate, R.D.; Olivardia, R. The Comorbidity of ADHD and Eating Disorders in a Nationally Representative Sample. J. Behav. Health Serv. Res. 2015, 42, 437–451. [Google Scholar] [CrossRef]
- Do, E.K.; Haberstick, B.C.; Williams, R.B.; Lessem, J.M.; Smolen, A.; Siegler, I.C.; Fuemmeler, B.F. The role of genetic and environmental influences on the association between childhood ADHD symptoms and BMI. Int. J. Obes. 2019, 43, 33–42. [Google Scholar] [CrossRef]
- Grant, J.E.; Redden, S.A.; Lust, K.; Chamberlain, S.R. Nonmedical use of stimulants is associated with riskier sexual practices and other forms of impulsivity. J. Addict. Med. 2018, 12, 474–480. [Google Scholar] [CrossRef]
- Groß-Lesch, S.; Dempfle, A.; Reichert, S.; Jans, T.; Geissler, J.; Kittel-Schneider, S.; Nguyen, T.T.; Reif, A.; Lesch, K.P.; Jacob, C.P. Sex- and Subtype-Related Differences in the Comorbidity of Adult ADHDs. J. Atten. Disord. 2016, 20, 855–866. [Google Scholar] [CrossRef]
- Guerdjikova, A.I.; Blom, T.J.; Mori, N.; Matthews, A.; Cummings, T.; Casuto, L.L.; McElroy, S.L. Lisdexamfetamine in Pediatric Binge Eating Disorder: A Retrospective Chart Review. Clin. Neuropharmacol. 2019, 42, 214–216. [Google Scholar] [CrossRef]
- Güngör, S.; Celiloğlu, Ö.S.; Raif, S.G.; Özcan, Ö.Ö.; Selimoğlu, M.A. Malnutrition and Obesity in Children with ADHD. J. Atten. Disord. 2016, 20, 647–652. [Google Scholar] [CrossRef] [PubMed]
- Miesch, M.; Deister, A. Attention-deficit/hyperactivity disorder (ADHD) in adult psychiatry: Data on 12-month prevalence, risk factors and comorbidity. Fortschr. Neurol. Psychiatr. 2019, 87, 32–38. [Google Scholar] [CrossRef]
- Penninx, B.W.J.H.; Lange, S.M.M. Metabolic syndrome in psychiatric patients: Overview, mechanisms, and implications. Dialogues Clin. Neurosci. 2018, 20, 63–73. [Google Scholar]
- Pugh, S.J.; Hutcheon, J.A.; Richardson, G.A.; Brooks, M.M.; Himes, K.P.; Day, N.L.; Bodnara, L.M. Gestational weight gain, prepregnancy body mass index and offspring attention-deficit hyperactivity disorder symptoms and behaviour at age 10. BJOG An Int. J. Obstet. Gynaecol. 2016, 123, 2094–2103. [Google Scholar] [CrossRef]
- Munsch, S.; Dremmel, D.; Wilhelm, P.; Baierlé, S.; Fischer, S.; Hilbert, A. To eat or not to eat: Reward delay impulsivity in children with loss of control eating, attention deficit hyperactivity disorder, a double diagnosis, and healthy children. PLoS ONE 2019, 14, e0221814. [Google Scholar] [CrossRef] [PubMed]
- Oswalt, S.B.; Lederer, A.M.; Chestnut-Steich, K.; Day, C.; Halbritter, A.; Ortiz, D. Trends in college students’ mental health diagnoses and utilization of services, 2009–2015. J. Am. Coll. Health 2020, 68, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Welch, E.; Ghaderi, A.; Swenne, I. A comparison of clinical characteristics between adolescent males and females with eating disorders. BMC Psychiatry 2015, 15, 45. [Google Scholar] [CrossRef] [PubMed]
- Lewis, E.; Gittelsohn, J.; Baker, C. More Frequent Family Meals Associated with Greater Risk of Obesity in Youth with and without ADHD (P11-115-19). Curr. Dev. Nutr. 2019, 3, 195190753. [Google Scholar] [CrossRef]
- Reinblatt, S.P.; Leoutsakos, J.M.S.; Mahone, E.M.; Forrester, S.; Wilcox, H.C.; Riddle, M.A. Association between binge eating and attention-deficit/hyperactivity disorder in two pediatric community mental health clinics. Int. J. Eat. Disord. 2015, 48, 505–511. [Google Scholar] [CrossRef]
- Wentz, E.; Björk, A.; Dahlgren, J. Is there an overlap between eating disorders and neurodevelopmental disorders in children with obesity? Nutrients 2019, 11, 2496. [Google Scholar] [CrossRef]
- Reinblatt, S.P.; Mahone, E.M.; Tanofsky-Kraff, M.; Lee-Winn, A.E.; Yenokyan, G.; Leoutsakos, J.M.S.; Moran, T.H.; Guarda, A.S.; Riddle, M.A. Pediatric loss of control eating syndrome: Association with attention-deficit/hyperactivity disorder and impulsivity. Int. J. Eat. Disord. 2015, 48, 580–588. [Google Scholar] [CrossRef] [PubMed]
- Bisset, M.; Rinehart, N.; Sciberras, E. DSM-5 eating disorder symptoms in adolescents with and without attention-deficit/hyperactivity disorder: A population-based study. Int. J. Eat. Disord. 2019, 52, 855–862. [Google Scholar] [CrossRef]
- Capusan, A.J.; Yao, S.; Kuja-Halkola, R.; Bulik, C.M.; Thornton, L.M.; Bendtsen, P.; Marteinsdottir, I.; Thorsell, A.; Larsson, H. Genetic and environmental aspects in the association between attention-deficit hyperactivity disorder symptoms and binge-eating behavior in adults: A twin study. Psychol. Med. 2017, 47, 2866–2878. [Google Scholar] [CrossRef]
- Jacob, L.; Haro, J.M.; Koyanagi, A. Attention deficit hyperactivity disorder symptoms and disordered eating in the English general population. Int. J. Eat. Disord. 2018, 51, 942–952. [Google Scholar] [CrossRef]
- Ziobrowski, H.; Brewerton, T.D.; Duncan, A.E. Associations between ADHD and eating disorders in relation to comorbid psychiatric disorders in a nationally representative sample. Psychiatry Res. 2018, 260, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Gorlin, E.I.; Dalrymple, K.; Chelminski, I.; Zimmerman, M. Diagnostic profiles of adult psychiatric outpatients with and without attention deficit hyperactivity disorder. Compr. Psychiatry 2016, 70, 90–97. [Google Scholar] [CrossRef]
- Porteret, R.; Bouchez, J.; Baylé, F.J.; Varescon, I. L’impulsivité dans le TDAH: Prévalence des troubles du contrôle des impulsions et autres comorbidités, chez 81 adultes présentant un trouble déficit de l’attention/hyperactivité (TDA/H). Encephale 2016, 42, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Gowey, M.A.; Stromberg, S.E.; Lim, C.S.; Janicke, D.M. The moderating role of body dissatisfaction in the relationship between ADHD symptoms and disordered eating in pediatric overweight and obesity. Child. Health Care 2017, 46, 15–33. [Google Scholar] [CrossRef]
- Egbert, A.H.; Wilfley, D.E.; Eddy, K.T.; Boutelle, K.N.; Zucker, N.; Peterson, C.B.; Celio Doyle, A.; Le Grange, D.; Goldschmidt, A.B. Attention-Deficit/Hyperactivity Disorder Symptoms Are Associated with Overeating with and without Loss of Control in Youth with Overweight/Obesity. Child. Obes. 2018, 14, 50–57. [Google Scholar] [CrossRef]
- Rojo-Moreno, L.; Arribas, P.; Plumed, J.; Gimeno, N.; García-Blanco, A.; Vaz-Leal, F.; Luisa Vila, M.; Livianos, L. Prevalence and comorbidity of eating disorders among a community sample of adolescents: 2-year follow-up. Psychiatry Res. 2015, 227, 52–57. [Google Scholar] [CrossRef]
- Mohammadi, M.R.; Mostafavi, S.A.; Hooshyari, Z.; Khaleghi, A.; Ahmadi, N.; Molavi, P.; Armani Kian, A.; Safavi, P.; Delpisheh, A.; Talepasand, S.; et al. Prevalence, correlates and comorbidities of feeding and eating disorders in a nationally representative sample of Iranian children and adolescents. Int. J. Eat. Disord. 2019, 53, 349–361. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.M.; Lim, M.H.; Kwon, H.J.; Yoo, S.J.; Kim, E.J.; Kim, J.W.; Ha, M.; Paik, K.C. Associations between attention-deficit/hyperactivity disorder symptoms and dietary habits in elementary school children. Appetite 2018, 127, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, F.; Georgiadou, E.; Bartsch, M.; Langenberg, S.; Müller, A.; De Zwaan, M. Attention Deficit Hyperactivity Disorder Prevalence and Correlates Pre- and Post-Bariatric Surgery: A Comparative Cross-Sectional Study. Obes. Facts 2017, 10, 1–11. [Google Scholar] [CrossRef]
- Brewerton, T.D.; Duncan, A.E. Associations between Attention Deficit Hyperactivity Disorder and Eating Disorders by Gender: Results from the National Comorbidity Survey Replication. Eur. Eat. Disord. Rev. 2016, 24, 536–540. [Google Scholar] [CrossRef] [PubMed]
- Woldeyohannes, H.O.; Soczynska, J.K.; Maruschak, N.A.; Syeda, K.; Wium-Andersen, I.K.; Lee, Y.; Cha, D.S.; Xiao, H.X.; Gallaugher, L.A.; Dale, R.M.; et al. Binge eating in adults with mood disorders: Results from the International Mood Disorders Collaborative Project. Obes. Res. Clin. Pract. 2015, 10, 531–543. [Google Scholar] [CrossRef]
- Svedlund, N.E.; Norring, C.; Ginsberg, Y.; von Hausswolff-Juhlin, Y. Symptoms of Attention Deficit Hyperactivity Disorder (ADHD) among adult eating disorder patients. BMC Psychiatry 2017, 17, 19. [Google Scholar] [CrossRef]
- Svedlund, N.E.; Norring, C.; Ginsberg, Y.; von Hausswolff-Juhlin, Y. Are treatment results for eating disorders affected by ADHD symptoms? A one-year follow-up of adult females. Eur. Eat. Disord. Rev. 2018, 26, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Halevy-Yosef, R.; Bachar, E.; Shalev, L.; Pollak, Y.; Enoch-Levy, A.; Gur, E.; Weizman, A.; Stein, D. The complexity of the interaction between binge-eating and attention. PLoS ONE 2019, 14, e0215506. [Google Scholar] [CrossRef] [PubMed]
- Carlucci, S.; Ivanova, I.; Bissada, H.; Tasca, G.A. Validity and reliability of the attention deficit hyperactivity disorder self-report scale (ASRS-v1.1) in a clinical sample with eating disorders. Eat. Behav. 2017, 26, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Sala, L.; Martinotti, G.; Carenti, M.L.; Romo, L.; Oumaya, M.; Pham-Scottez, A.; Rouillon, F.; Gorwood, P.; Janiri, L. Attention-deficit/hyperactivity disorder symptoms and psychological comorbidity in eating disorder patients. Eat. Weight Disord. 2018, 23, 513–519. [Google Scholar] [CrossRef]
- Kurz, S.; Schoebi, D.; Dremmel, D.; Kiess, W.; Munsch, S.; Hilbert, A. Satiety regulation in children with loss of control eating and attention-deficit/hyperactivity disorder: A test meal study. Appetite 2017, 116, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Tong, L.; Shi, H.; Li, X. Associations among ADHD, abnormal eating and overweight in a non-clinical sample of Asian children. Sci. Rep. 2017, 7, 2844. [Google Scholar] [CrossRef]
- Leventakou, V.; Micali, N.; Georgiou, V.; Sarri, K.; Koutra, K.; Koinaki, S.; Vassilaki, M.; Kogevinas, M.; Chatzi, L. Is there an association between eating behaviour and attention-deficit/hyperactivity disorder symptoms in preschool children? J. Child Psychol. Psychiatry Allied Discip. 2016, 57, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Fuemmeler, B.F.; Sheng, Y.; Schechter, J.C.; Do, E.; Zucker, N.; Majors, A.; Maguire, R.; Murphy, S.K.; Hoyo, C.; Kollins, S.H. Associations between attention deficit hyperactivity disorder symptoms and eating behaviors in early childhood. Pediatr. Obes. 2020, 15, e12631. [Google Scholar] [CrossRef]
- Yilmaz, Z.; Javaras, K.N.; Baker, J.H.; Thornton, L.M.; Lichtenstein, P.; Bulik, C.M.; Larsson, H. Association between Childhood to Adolescent Attention Deficit/Hyperactivity Disorder Symptom Trajectories and Late Adolescent Disordered Eating. J. Adolesc. Health 2017, 61, 140–146. [Google Scholar] [CrossRef]
- Sonneville, K.R.; Calzo, J.P.; Horton, N.J.; Field, A.E.; Crosby, R.D.; Solmi, F.; Micali, N. Childhood hyperactivity/inattention and eating disturbances predict binge eating in adolescence. Psychol. Med. 2015, 45, 2511–2520. [Google Scholar] [CrossRef]
- Zhang, Z.; Robinson, L.; Jia, T.; Quinlan, E.B.; Tay, N.; Chu, C.; Barker, E.D.; Banaschewski, T.; Barker, G.J.; Bokde, A.L.W.; et al. Development of Disordered Eating Behaviors and Comorbid Depressive Symptoms in Adolescence: Neural and Psychopathological Predictors. Biol. Psychiatry 2020. In press. [Google Scholar] [CrossRef]
- Nazar, B.P.; Trindade, A.P.; Leslie, M.; Malloy-Diniz, L.F.; Sergeant, J.; Treasure, J.; Mattos, P. Eating disorders impact on vigilance and decision making of a community sample of treatment naive attention-deficit/hyperactivity disorder young adults. Front. Psychiatry 2018, 9, 531. [Google Scholar] [CrossRef]
- Van der Oord, S.; Braet, C.; Cortese, S.; Claes, L. Testing the dual pathway model of ADHD in obesity: A pilot study. Eat. Weight Disord. 2017, 23, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Ferre, F.; Cambra, J.; Ovejero, M.; Basurte-Villamor, I.; Navarrete, F.F. Influence of attention deficit hyperactivity disorder symptoms on quality of life and functionality in adults with eating disorders. Actas Esp. Psiquiatr. 2017, 45, 98–107. [Google Scholar]
- Christian, C.; Martel, M.M.; Levinson, C.A. Emotion regulation difficulties, but not negative urgency, are associated with attention-deficit/hyperactivity disorder and eating disorder symptoms in undergraduate students. Eat. Behav. 2020, 36, 101344. [Google Scholar] [CrossRef] [PubMed]
- Hanson, J.A.; Phillips, L.N.; Hughes, S.M.; Corson, K. Attention-deficit hyperactivity disorder symptomatology, binge eating disorder symptomatology, and body mass index among college students. J. Am. Coll. Health 2019, 68, 543–549. [Google Scholar] [CrossRef]
- Koch, S.V.; Andersson, M.; Hvelplund, C.; Skovgaard, A.M. Mental disorders in referred 0–3-year-old children: A population-based study of incidence, comorbidity and perinatal risk factors. Eur. Child Adolesc. Psychiatry 2020. [Google Scholar] [CrossRef]
- Kaisari, P.; Dourish, C.T.; Rotshtein, P.; Higgs, S. Associations between core symptoms of attention deficit hyperactivity disorder and both binge and restrictive eating. Front. Psychiatry 2018, 9, 103. [Google Scholar] [CrossRef] [PubMed]
- Williamson, T.M.; Campbell, T.S.; Telfer, J.A.; Rash, J.A. Emotion Self-Regulation Moderates the Association between Symptoms of ADHD and Weight Loss after Bariatric Surgery. Obes. Surg. 2017, 28, 1553–1561. [Google Scholar] [CrossRef] [PubMed]
- Reinblatt, S.P. Are Eating Disorders Related to Attention Deficit/Hyperactivity Disorder? Curr. Treat. Options Psychiatry 2015, 2, 402–412. [Google Scholar] [CrossRef]
- Keshen, A.; Ivanova, I. Reduction of Bulimia Nervosa Symptoms after Psychostimulant Initiation in Patients with Comorbid ADHD: Five Case Reports. Eat. Disord. 2013, 21, 360–369. [Google Scholar] [CrossRef]
- Anderson, L.M.; Smith, K.M.; Schaefer, L.M.; Crosby, R.D.; Cao, L.; Engel, S.G.; Crow, S.J.; Wonderlich, S.A.; Peterson, C.B. Predictors and Moderators of Treatment Outcome in a Randomized Clinical Trial for Binge-Eating Disorder. J. Consult. Clin. Psychol. 2020, 88, 631–642. [Google Scholar] [CrossRef]
- Cortese, S.; Bernardina, B.D.; Mouren, M.-C. Attention-Deficit/Hyperactivity Disorder (ADHD) and Binge Eating. Nutr. Rev. 2008, 65, 404–411. [Google Scholar] [CrossRef]
- Fletcher, P.C.; Kenny, P.J. Food addiction: A valid concept? Neuropsychopharmacology 2018, 43, 2506–2513. [Google Scholar] [CrossRef]
- Cortese, S.; Konofal, E.; Bernardina, B.D.; Mouren, M.C.; Lecendreux, M. Does excessive daytime sleepiness contribute to explaining the association between obesity and ADHD symptoms? Med. Hypotheses 2008, 70, 12–16. [Google Scholar] [CrossRef]
- Quaranta, G.; Barbuti, M.; Alessandro, P.; Colombini, P.; Moriconi, M.; Gemmellaro, T.; Tripodi, B.; Palagini, L.; Schiavi, E.; Perugi, G. Relationships among Delayed Sleep Phase Disorder, Emotional Dysregulation, and Affective Temperaments in Adults with Attention Deficit Hyperactivity Disorder and Cyclothymia. J. Nerv. Ment. Dis. 2020, 32769692. [Google Scholar] [CrossRef]


 : [9,11,103,105,112,113,116,117,120,121,122,123,124,126,127,129,130,131,132,133,134,135,136,137,138].
: [9,11,103,105,112,113,116,117,120,121,122,123,124,126,127,129,130,131,132,133,134,135,136,137,138].  : [135].
: [135].  : [108,109,112,126,137,138].
: [108,109,112,126,137,138].

{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria | ||
|---|---|---|---|
| I1 | Key words cited in the abstract | E1 | Key words not cited in the title/abstract |
| I2 | Date of publication: January 2015 to June 2020 | E2 | Publication before January 2015 |
| I3 | Journal article with peer-review | E3 | Book chapter, letter to the editor or other non-empirical type of publications |
| I4 | Written in English or French | E4 | Paper not written in English or French |
| I5 | Empirical research | E5 | Review and meta-analysis papers |
| I6 | Focus on the association between ADHD and eating behavior | E6 | Focus on treatment, medical imaging, genetics |
| I7 | ADHD and disordered eating symptoms in the same individual | E7 | Focus on the impact of parents’ disordered eating or BMI on their child’s ADHD symptoms |
| I8 | Assessment of ADHD and disordered eating symptoms | ||
| Population | Country | Children- Adolescents | Adults | ADHD Diagnosis Instruments | N | Age Mean (SD) (Years) | Gender Female (%) | Disordered Eating | ADHD Symptoms | Non-ADHD Symptoms | Statistics | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Disordered Eating Prevalence (%) | n | Disordered Eating Prevalence (%) | Odds Ratio | 95% Confidence Intervals | p | |||||||||
| General population | |||||||||||||||
| [105] | USA | x | K-SADS PL and CRPS | 79 | 11.0 (1.9) | 48.1 | LOC-E | 31 | 70.5 | 7 | 20 | 12.68 | 3.11–51.64 a | ||
| [106] | Australia | x | SDQ or parent-reported ADHD diagnosis or medication | 2672 | 14.9 (0.3) | 0 | Regular objective BE | 2.9 | 0.3 | 9.4 | 1.7–52.8 | ||||
| Partial syndrome BN | 1.6 | 1.5 | 1.0 | 0.1–8.0 | |||||||||||
| Partial syndrome BED | 1.3 | 0.2 | 6.2 | 0.6–61.1 | |||||||||||
| 100 | Regular objective BE | 6.5 | 2.2 | 3.1 | 0.7–14.0 | ||||||||||
| Partial syndrome BN | 6.5 | 3.6 | 1.9 | 0.4–8.2 | |||||||||||
| Partial syndrome BED | 0 | 0.6 | - | - | |||||||||||
| [107] | Sweden | x | DSM-IV criteria | 18,029 | 33.6 (7.6) | 55.6 | BE behavior | 113 | 7.17 | - | 3.65 | 2.72–4.91 | |||
| DSM-5 BE behavior | 58 | 3.72 | - | 3.01 | 2.09–4.35 | ||||||||||
| DSM-5 BED | 7 | 0.45 | - | 2.55 | 1.11–5.86 | ||||||||||
| DSM-5 BN | 48 | 3.11 | - | 3.09 | 2.09–4.56 | ||||||||||
| [108] | UK | x | ASRS | 7403 | 46.3 (18.6) | 51.4 | Self-sick for feeling full | 8.5 | 2.7 | 2.79 | 1.76–4.42 b | ||||
| 1.26 | 0.63–2.51 c | ||||||||||||||
| Uncontrolled eating | 22.8 | 6.4 | 3.94 | 2.94–5.28 b | |||||||||||
| 1.67 | 1.14–2.46 c | ||||||||||||||
| Possible ED | 19.2 | 5.7 | 3.48 | 2.56–4.72 b | |||||||||||
| 1.32 | 0.82–2.13 c | ||||||||||||||
| [13] | France | x | WURS-25 + ASRS | 1517 | 20.6 (3.6) | 68.2 | Food addiction | 12 | 14.1 | 57 | 4.0 | 2.27 | 1.05–4.88 d | ||
| Any ED | 28 | 32.9 | 249 | 17.4 | 1.33 | 0.76–2.33 d | |||||||||
| [109] | USA | x | DIS-IV (childhood) + adult ACDS | 4719 | 31 (DNS) | 52.1 | Past 12-month any ED | 9.74 | 4.23–22.40 b | ||||||
| 2.84 | 1.22–6.63 c | ||||||||||||||
| Past 12-month BED | 4.53 | 1.82–11.24 b | |||||||||||||
| 1.65 | 0.67–4.04 c | ||||||||||||||
| Past 12-month BN | 28.24 | 6.33–126.01 b | |||||||||||||
| 5.04 | 1.15–22.08 c | ||||||||||||||
| Past 12-month subthreshold BED | 5.55 | 1.90–16.24 b | |||||||||||||
| 3.83 | 0.94–15.67 c | ||||||||||||||
| Psychiatry outpatients | |||||||||||||||
| [103] | USA | x | DSM-IV criteria | 252 | 10.8 (3.7) | 47.2 | BE | 28 | 26 | 3 | 2.0 | - | - | *** | |
| [110] | USA | x | SCID-IV | 1134 | 39.7 (14.4) | 58 | Any ED | 19 | 9.3 | 35 | 3.8 | 2.67 | 1.45–4.80 | ||
| Patients with obesity | |||||||||||||||
| [104] | Sweden | x | Medical records or DAWBA | 40 | 12.4 (3.0) | 48.7 | LOC-E | 5 | 55.6 | 21 | 67.7 | - | - | >0.05 | |
| [11] | France | x | DIVA 2.0 | 105 | 46.5 (10.7) | 86.7 | Food addiction | 8 | 28.6 | 7 | 9.1 | 4.00 | 1.29–12.40 | ||
| Significant distress in relation to food | 9 | 32.1 | 9 | 11.7 | 3.58 | 1.25–10.30 | |||||||||
| ADHD outpatients | |||||||||||||||
| [111] | France | x | Children-MINI adapted for adults | 81 | 34.8 (11.6) | 37 | Bulimia nervosa | 7 | 8.6 | - | - | - | - | - | |
| [29] | Norway | x | DSM-IV criteria | 533 | 36.2 (11.3) | 100 | Any ED | 36 | 13.0 | - | - | - | - | - | |
| 37.4 (10.7) | 0 | Any ED | 3 | 1.1 | - | - | - | - | - | ||||||
| Population | Country | Children-Adolescents | Adults | N | Age Mean (SD) (Years) | Gender Female (%) | Mean BMI or zBMI (SD) | ADHD Instruments | Childhood ADHD Prevalence (%) | Adult ADHD Prevalence |
|---|---|---|---|---|---|---|---|---|---|---|
| Non clinical population | ||||||||||
| [112] | USA | x | 220 | 10.3 (1.4) | 53.6 | 2.19 (0.38) | CBCL | 5.0 | ||
| Clinical obesity population | ||||||||||
| [113] | USA | x | 385 | 10.9 (2.3) | 63 | 2.26 (0.35) | CBCL | 11.0 | ||
| [104] | Sweden | x | 76 | 12.4 (3.0) | 48.7 | 3.40 (0.50) | Medical records or DAWBA | 18.4 | ||
| [9] | Brazil | x | 106 | 39.0 (10.7) | 100 | 39.21 (5.29) | K-SADS adapted for adults, DSM IV | 28.3 a | ||
| [117] | Germany | x | 120 | 41.0 (11.5) | 79.2 | 47.76 (7.41) | WURS-k + CAARS-S:S | 17.5 b | 8.3 a | |
| [11] | France | x | 105 | 46.4 (10.7) | 86.7 | 46.90 (7.80) | DIVA 2.0 | 35.2 b | 26.7 a | |
| Population | Country | Children- Adolescents | Adults | ADHD Instruments | N | Mean Age (SD) (Years) | Gender Female (%) | Disordered Eating | Disordered Eating | Non Disordered Eating | Statistics | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | ADHD Symptoms Prevalence (%) | n | ADHD Symptoms Prevalence (%) | Odds Ratio | 95% Confidence Intervals | p | |||||||||
| General population | |||||||||||||||
| [114] | Spain | x | K-SADS | 962 | DNS (12–16) | 47.8 | ED | 11 | 31.4 | 80 | 8.4 | 5.03 | 2.37–10.64 | ||
| [116] | Korea | x | K-ARS | 16,831 | 9.29 (1.71) | 50.2 | Every day overeating | 68 | 21.1 | - | - | ||||
| [115] | Iran | x | K-SADS PL | 27,111 | DNS (6–18) | 48.6 | Lifetime ED | - | 7.6 | - | 3.9 | 0.026 | |||
| [118] | USA | x | CIDI | 1686 | DNS (18–44) | 100 | Lifetime any ED | 18 | 21.9 | 75 | 5.7 | 4.51 | 2.01–10.15 b | ||
| Past 12-month any ED | 10 | 30.6 | 83 | 6.1 | 7.11 | 2.61–19.39 b | |||||||||
| Lifetime BED | 8 | 17.1 | 85 | 6.3 | 3.01 | 1.14–7.95 b | |||||||||
| Past 12-month BED | 4 | 19.3 | 89 | 6.5 | 3.57 | 1.06–12.09 b | |||||||||
| Lifetime BN | 10 | 33.2 | 83 | 6.1 | 7.93 | 2.75–22.85 b | |||||||||
| Past 12-month BN | 6 | 56.7 | 87 | 6.3 | 21.15 | 3.76–118-98 b | |||||||||
| Lifetime any binge | 16 | 18.7 | 77 | 5.9 | 3.66 | 1.71–7.87 b | |||||||||
| Past 12-month any binge | 8 | 19.4 | 85 | 6.3 | 3.71 | 1.68–8.20 b | |||||||||
| 0 | Lifetime any ED | 6 | 21.3 | 85 | 9.7 | 2.23 | 0.81–6.13 b | ||||||||
| Past 12-month any ED | 4 | 45.9 | 87 | 9.7 | 6.48 | 1.33–31.60 b | |||||||||
| Lifetime BED | 6 | 25.4 | 85 | 9.6 | 2.93 | 0.98–8.76 b | |||||||||
| Past 12-month BED | 4 | 45.9 | 87 | 9.7 | 6.47 | 1.33–31.61 b | |||||||||
| Lifetime BN | 1 | 66.9 | 90 | 9.9 | 18.18 | 1.39–238.40 b | |||||||||
| Lifetime any binge | 11 | 19.4 | 80 | 9.5 | 2.39 | 1.17–4.91 b | |||||||||
| Past 12-month any binge | 7 | 38.9 | 84 | 9.5 | 5.02 | 1.90–13.28 b | |||||||||
| Mood disorder outpatients a | |||||||||||||||
| [119] | Canada | x | MINI | 631 | 37.8–40.0 (12.0–12.4) | 59.0 | BE | 26 | 20.8 | 61 | 12.5 | 0.018 | |||
| ED patients | |||||||||||||||
| [120] | Sweden | x | ASRS | 1094 | 27.7 (8.7) | 100 | Any ED | 346 | 31.6 | - | - | ||||
| BED | 25 | 27.5 | - | - | |||||||||||
| BN | 156 | 37.1 | - | - | |||||||||||
| AN-BP | 13 | 35.1 | - | - | |||||||||||
| AN-R | 12 | 17.6 | - | - | |||||||||||
| EDNOS-BP | 102 | 31.0 | - | - | |||||||||||
| EDNOS-R | 38 | 25.7 | - | - | |||||||||||
| [121] | Sweden | x | ASRS | 443 | 27.5 (8.5) | 100 | Any ED | 45 | 10.2 | - | - | ||||
| [122] | Israel | x | x | K-SADS PL | 168 | DNS (15–28) | 100 | BE | - | 16.6 | - | 13.6 | 0.392 | ||
| BN | - | 12.0 | - | - | |||||||||||
| AN-BP | - | 28.0 | - | - | |||||||||||
| AN-R | - | 9.0 | - | - | |||||||||||
| [123] | Canada | x | ASRS | 500 | 27.6 (10.6) | 95.2 | Any ED | - | 49.8 | ||||||
| [124] | France | x | WURS + BAADS | 73 | 28.1 (7.3) | 100 | AN-R | 3 | 8.1 | - | - | ||||
| AN-BP | 9 | 32.1 | - | - | |||||||||||
| BN | 1 | 12.5 | - | - | |||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
El Archi, S.; Cortese, S.; Ballon, N.; Réveillère, C.; De Luca, A.; Barrault, S.; Brunault, P. Negative Affectivity and Emotion Dysregulation as Mediators between ADHD and Disordered Eating: A Systematic Review. Nutrients 2020, 12, 3292. https://doi.org/10.3390/nu12113292
El Archi S, Cortese S, Ballon N, Réveillère C, De Luca A, Barrault S, Brunault P. Negative Affectivity and Emotion Dysregulation as Mediators between ADHD and Disordered Eating: A Systematic Review. Nutrients. 2020; 12(11):3292. https://doi.org/10.3390/nu12113292
Chicago/Turabian StyleEl Archi, Sarah, Samuele Cortese, Nicolas Ballon, Christian Réveillère, Arnaud De Luca, Servane Barrault, and Paul Brunault. 2020. "Negative Affectivity and Emotion Dysregulation as Mediators between ADHD and Disordered Eating: A Systematic Review" Nutrients 12, no. 11: 3292. https://doi.org/10.3390/nu12113292
APA StyleEl Archi, S., Cortese, S., Ballon, N., Réveillère, C., De Luca, A., Barrault, S., & Brunault, P. (2020). Negative Affectivity and Emotion Dysregulation as Mediators between ADHD and Disordered Eating: A Systematic Review. Nutrients, 12(11), 3292. https://doi.org/10.3390/nu12113292