1. Introduction
Malnutrition is one of the most serious public health challenges globally; nearly one in three people suffer from at least one form of malnutrition manifested as wasting, stunting, micro-nutrient deficiency, and/or overweight or obesity [
1]. In the past two decades, the number of overweight individuals in Africa has significantly increased. This is a major concern especially in light of the remaining high prevalence of undernutrition in this region [
2,
3]. The occurrence of both under-and over nutrition in the same population is often referred to as the “double burden of malnutrition” [
4]. The driving forces are multifaceted, including changes in dietary and physical activity patterns related to transitions in livelihoods; moving from traditional food systems dependent upon subsistence farming to dependence upon income generation and the market [
1]. These transitions are more prominent in transient urban settings where they contribute to an excess intake of energy, insufficient amounts of micro-nutrients and limited physical activity [
5,
6,
7].
Despite the various health benefits of fruits and vegetables including reducing risk for non-communicable diseases, the consumption is generally low [
8]. An aggregated result from 28 low-and middle-income countries exemplified this with only 18% (95 CI: 16.6–19.4%) of the population meeting the recommended 400 g/day serving [
9]. Traditional diets rich in fiber, high in vegetable and fruit varieties are being substituted by diets rich in oils, fats, and sugars, often in the form of ultra-processed foods [
10,
11]. The shift in diet can be partially explained by changes in food systems; whereby the rise of industrial production of cheap foods is making ultra-processed food more accessible [
12,
13,
14].
With regards to food accessibility, the importance of the “food environment” is underscored [
13,
15,
16]. The food environment which encompasses domains such as accessibility, availability, and affordability is an interface whereby individuals interact with the wider food system for food purchase and consumption [
17]. Logically, individuals can only eat from the range of things that are available to them, and availability of an adequate supply of healthy food has been consistently associated with a healthy diet [
18]. The availability of fresh healthy foods has also been improved by the development of advanced agricultural technologies and transport systems that can provide cold chain equipment to preserve perishables. However, as these technologies are undeveloped in low income settings 40% of fresh food does not reach consumers due to post-harvest loss [
19,
20].
Another important dimension relating to diet is affordability [
18]. In low income urban areas where availability is limited, only the economically better-off families manage to access a wide range of the recommended food groups [
20,
21]. Despite sufficient access to markets, dietary choices are influenced by price [
22]. The results from a multi-country study showed that individuals from low income countries spend more than half of their income in order to meet dietary recommendations [
23]. The high cost prevents poorer households from affording a nutritionally adequate diet [
22]. This is more common in urban areas where most households’ only source of food is that which is purchased. Furthermore, less healthy alternatives are often inexpensive, have a longer shelf-life, require little preparation, and have an alluring taste, making them both convenient and desirable for the women who are responsible for purchasing and preparing food for the family [
13,
24,
25].
Mothers/caretakers have a significant role in shaping the diet of the household as they generally determine which foods are bought and prepared within the home. Mothers draw on wealth and food security of the household as well as their own education to fulfill this responsibility. Studies have shown that households with better socioeconomic resources enjoy a more nutritious diet, as opposed to their disadvantaged counterparts whose diet consists of much less fiber, fruits, and vegetables [
26,
27,
28]. Households with educated mothers have been shown to have a higher consumption of fruits and vegetables as well as better diet diversity [
9,
29,
30]. On the contrary, in some contexts, higher maternal education has also been associated with higher consumption of sugary drinks and more processed foods [
31]. Moreover, although households in the highest wealth groups had a more diverse diet [
26,
32], they have also been associated with an increase in overweight/obesity [
33,
34].
The fundamental cause of the double burden of malnutrition is energy imbalance; “energy excess” for obesity and “energy and nutrient deficiencies” for undernutrition [
35]. Hence the promotion of good nutrition presents an opportunity to avert the occurrence of both forms of malnutrition [
34]. However, there is limited research, in particular concerning the food environments in sub-Saharan African countries, which makes designing holistic and contextualized policies problematic. Therefore, understanding how availability and affordability shapes the family diet is important. This study aims to understand the quality of diet being consumed among families in Addis Ababa, and to what extent social stratification and perceptions of availability and affordability affect healthy food consumption.
4. Discussion
This study found that all family food groups were perceived to be available in the market. A few food groups (cereals, other vegetables, and legumes) were perceived as affordable by the majority and were also consumed to a large extent. On the contrary, micronutrient rich foods (vitamin A rich fruits and vegetables and dark green leafy vegetables) as well as animal source protein rich foods (meat, dairy, and eggs) showed a considerable variation in perceived affordability as well as consumption with a clear stratification in terms of household wealth and maternal education. Evaluation of the relative contribution of affordability, wealth, and maternal education to consumption of family foods showed, with a few exceptions, that all three of them independently explained consumption of the various family foods; higher perceptions of affordability and socioeconomic resources were associated with higher prevalence of consumption.
All of the family food types with the exception of fish were reported to be available by 90% or more of the respondents. This gives a clear indication that most foods required for a healthy diet are perceived to be available for the vast majority of households. The high availability of foods may be explained by the diversities in food retail alternatives and a high dependability on informal markets which makes the food market more responsive to the need of vulnerable segments of the population [
44,
45]. This, in turn, makes the more vulnerable less susceptible to food deserts which often occur in urban high-income settings with a high dependence on supermarkets [
45]. Another explanation for high availability could be that the supply is increasingly following the demand of the population; as the population size increases, the produce coming to the capital may be increasing. This is especially true for cereals/white roots/tubers which constitutes a major part of the staple diet [
46].
While a social stratification was shown, the three food groups (cereals/white roots and tubers, legumes, and other vegetables) were considered affordable by a large proportion of the households as well as were consumed by almost all. Across all social strata, consumption of these three types of foods was the same or higher than what households reported to be able to afford. On the contrary, for the other food groups, households consumed less than what they can afford. This could be due to the interplay of many other factors such as preferences, ability to prepare the foods in the family food groups in terms of having adequate cooking space, time, and skills, all of which have been identified as potential drivers for food choices [
13,
47,
48,
49].
The high consumption of cereals and white roots/tubers observed here is consistent with national food consumption survey which reported more than 65% of the energy intake of the population is from carbohydrates [
46]. Part of the explanation for the affordability of cereals could be high production [
50]; the surplus production could potentially make it slightly more affordable than other items in the market. These perceptions align to the realities of the cost of food in Ethiopia [
51]. Except for cereals and white roots/tubers, the price of all other food group categories, particularly vitamin A rich dark green leafy vegetables and animal source food, are increasing markedly [
51]. Part of the increase in price of perishable foods could be due to infrastructure and transportation systems resulting in large post-harvest losses [
20]. This may also push the price of fruits and vegetables higher. As was reflected earlier, affordability rather than availability is a more serious challenge in improving the family diet in urban settings [
21]. Except for dark green leafy vegetables, both micronutrient rich foods (vitamin A rich fruits and vegetables) as well as protein rich foods (meat, dairy and eggs) were neither perceived affordable nor actually consumed by the majority of the households. The high cost of a nutritious diet makes the poor more vulnerable; for example, in low income countries 29% of a household’s income is required to purchase one serving of fruits [
23]. In another study where they estimated the cost of a recommended healthy diet relative to households per capita, they found that the cost exceeded the total income for 20% of the world’s populations [
52], making it impossible for poor households to meet dietary recommendations.
Households in the highest wealth quintile had higher odds of consuming both micronutrient rich foods (vitamin A rich fruits and vegetables and dark green leafy vegetables) as well as protein rich foods (meat, dairy, and eggs). The difference in consumption between households in the highest compared to the lowest wealth quintile was nearly double for both micronutrient rich as well as animal source protein rich foods and remained significant after adjusting for known confounding factors. Other studies have also shown that higher household wealth status significantly improved purchase and consumption of a diverse diet [
26,
53]. The better-off households were less vulnerable to price fluctuations putting them in a better position for a more planned diet than the poor households [
5,
47].
Perceptions of affordability were associated with higher odds of consumption of the food groups. This is in line with studies on fruits and vegetables that have shown these food groups were perceived expensive and hence consumed in a limited amount particularly among the disadvantaged groups [
26,
54]. Individuals from the lowest wealth quintile may not have adequate cold storage options such as refrigerators to store short-lived items such as meat, dairy, and even fruit and vegetable leading to purchases for one-time use, thus paying higher prices to retailers, which renders these items more unaffordable [
55]. Food items that were considered affordable, were widely consumed by our study groups indicating cost is a strong determinant for their diets [
22,
56].
Maternal education level was also associated with better consumption of a variety of food groups. In households with college educated mothers, consumption of both micronutrient and animal source food was higher compared to households with mothers who never attended/finished a grade. Studies have shown that mothers’ awareness of dietary recommendations and nutrition knowledge as well as diet-related diseases are important factors in diet quality [
29]. Understanding the health value of food items is linked to years of schooling; higher levels of schooling have been associated with improved diet diversity [
57]. Another possible explanation for the improvement in consumption of different food groups is the fact that educated mothers, are often working outside home, have more self-efficacy in making decisions and subsequently a better income, all of which have been shown to improve the diet of the family [
30,
58].
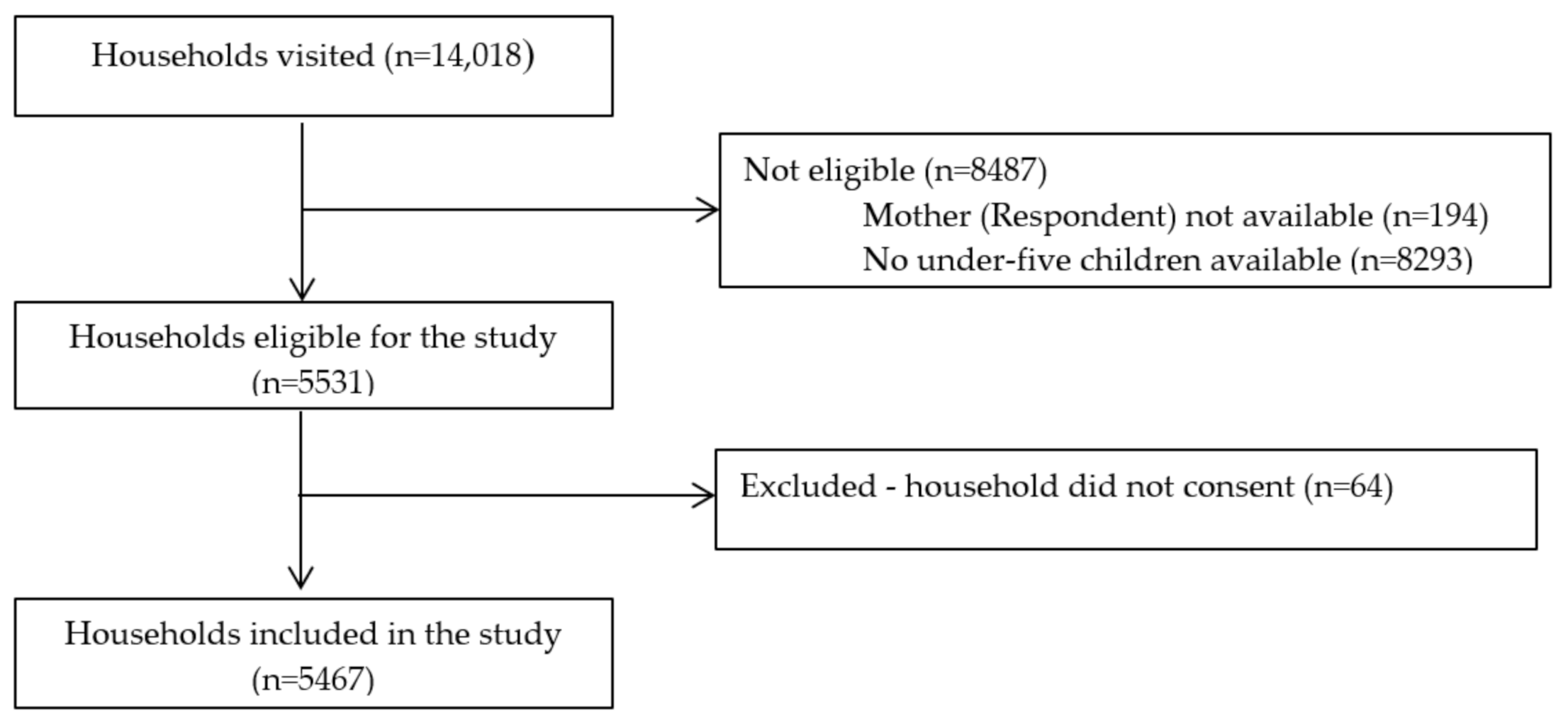
This study is the largest survey in Addis Ababa on the subject matter and draws a sample from all 116 districts (the smallest administrative unit) of the city. To cover seasonal variations due to the availability of food items, the survey was conducted in two rounds; in what is referred to as the season of plenty and the season of scarcity. The response rate was very high in almost all districts. Thus, the findings are a fair representation of the situation in Addis Ababa. That said, cautious interpretation is advised when attempting to generalize the results to other contexts as Addis Ababa presents a slightly different demographic compared to other cities within Ethiopia, due to its diverse population drawing/migrating from all corners of the country.
For this study we developed two new measures: perceived availability and perceived affordability of foods. The translation of the concepts into Amharic were discussed with native speakers in and outside of the research team before pilot testing. In the pilot testing we found that the concepts were easily understood. Preliminary comparison between perceived availability and our simultaneously collected data on actual availability of foods in the residential neighborhoods show good agreement. Further, preliminary analyses show that perceptions of affordability have a socio-economic stratification in the way it is expected. However, while perception-based measurements provide an understanding of people’s perceptions it is difficult to know what their imbedded dimension are. We suggest further research on this.
We used a standard method for sampling of households. As the sampling is based on selection of a physical dwelling (even if at times of low standard) it does exclude homeless inhabitants of Addis Ababa, unfortunately this is almost unavoidable. Finally, the limitations are as always, a risk of potential social desirability in responses as well as residual confounding in statistical analyses.

 ,
, 

{kind=link}