Effect of Added Sugar on the Consumption of A Lipid-Based Nutrient Supplement Among 7–24-Month-Old Children

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting, Design and Participants
2.2. SQ-LNS Products
2.3. Randomization and Blinding
2.4. Study Procedures
2.5. Measures
2.6. Sample Size Calculation
2.7. Statistical Analysis
2.7.1. Analysis of Initial and Final Exposure Data
2.7.2. Analysis of Consumption during the Home Exposure Period
3. Results
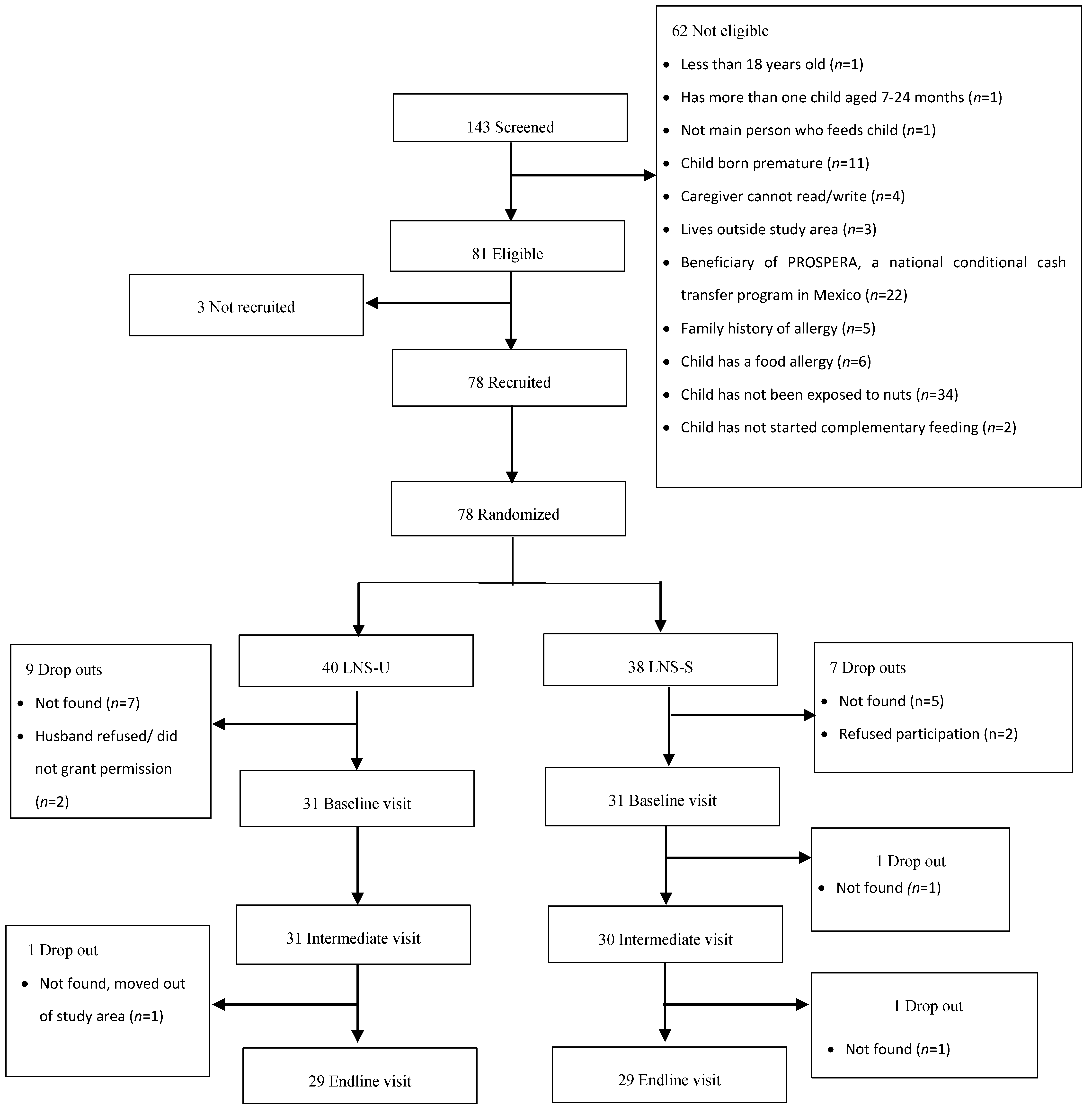
3.1. Participants
3.2. Acceptability of SQ-LNS
3.2.1. Consumption during Initial and Final Exposure
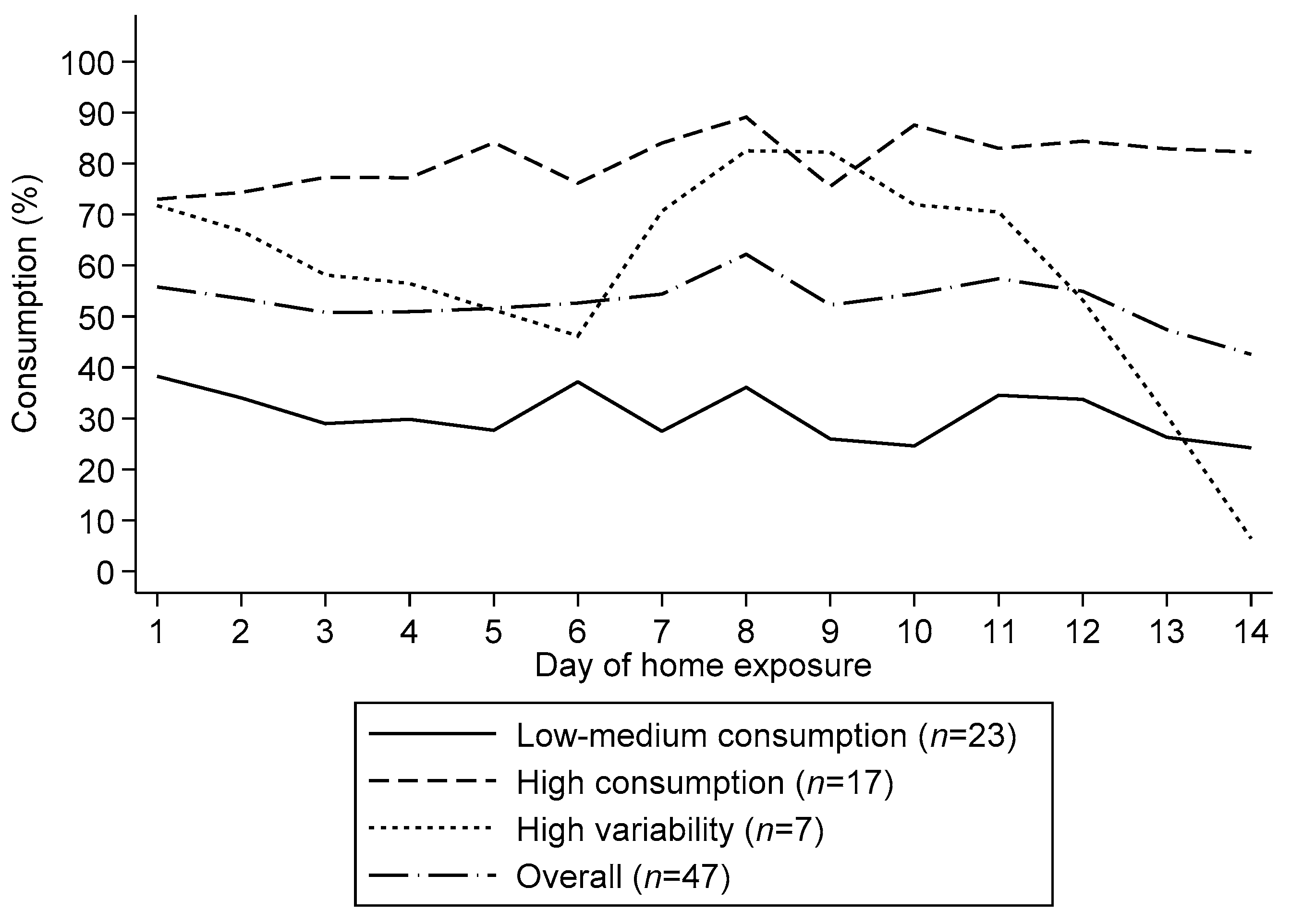
3.2.2. Consumption during the Home Exposure Period
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bhutta, Z.A.; Ahmed, T.; Black, R.E.; Cousens, S.; Dewey, K.; Giugliani, E.; Haider, B.A.; Kirkwood, B.; Morris, S.S.; Sachdev, H.; et al. What works? Interventions for maternal and child undernutrition and survival. Lancet 2008, 371, 417–440. [Google Scholar] [CrossRef]
- Bhutta, Z.A.; Das, J.K.; Rizvi, A.; Gaffey, M.F.; Walker, N.; Horton, S.; Webb, P.; Lartey, A.; Black, R.E. Evidence-based interventions for improvement of maternal and child nutrition: What can be done and at what cost? Lancet 2013, 382, 452–477. [Google Scholar] [CrossRef]
- Adu-Afarwuah, S.; Lartey, A.; Okronipa, H.; Ashorn, P.; Peerson, J.M.; Arimond, M.; Ashorn, U.; Zeilani, M.; Vosti, S.; Dewey, K.G. Small-quantity, lipid-based nutrient supplements provided to women during pregnancy and 6 mo postpartum and to their infants from 6 mo of age increase the mean attained length of 18-mo-old children in semi-urban Ghana: A randomized controlled trial 1,2. Am. J. Clin. Nutr. 2016, 104, 797–808. [Google Scholar] [CrossRef] [PubMed]
- Prado, E.L.; Abbeddou, S.; Jimenez, E.Y.; Somé, J.W.; Ouédraogo, Z.P.; Vosti, S.A.; Dewey, K.G.; Brown, K.H.; Hess, S.Y.; Ouédraogo, J.B. Lipid-based nutrient supplements plus malaria and diarrhea treatment increase infant development scores in a cluster-randomized trial in Burkina Faso. J. Nutr. 2016, 146, 814–822. [Google Scholar] [CrossRef] [PubMed]
- Prado, E.L.; Adu-Afarwuah, S.; Lartey, A.; Ocansey, M.; Ashorn, P.; Vosti, S.A.; Dewey, K.G. Effects of pre- and post-natal lipid-based nutrient supplements on infant development in a randomized trial in Ghana. Early Hum. Dev. 2016, 99, 43–51. [Google Scholar] [CrossRef]
- Prado, E.L.; Maleta, K.; Ashorn, P.; Ashorn, U.; Vosti, S.A.; Sadalaki, J.; Dewey, K.G. Effects of maternal and child lipid-based nutrient supplements on infant development: A randomized trial in Malawi. Am. J. Clin. Nutr. 2016, 103, 784–793. [Google Scholar] [CrossRef]
- Adu-Afarwuah, S.; Lartey, A.; Brown, K.H.; Zlotkin, S.; Briend, A.; Dewey, K.G. Randomized comparison of 3 types of micronutrient supplements for home fortification of complementary foods in Ghana: Effects on growth and motor development 14. Am. J. Clin. Nutr. 2007, 86, 412–432. [Google Scholar] [CrossRef]
- Adu-Afarwuah, S.; Lartey, A.; Okronipa, H.; Ashorn, P.; Zeilani, M.; Peerson, J.M.; Arimond, M.; Vosti, S.; Dewey, K.G. Lipid-based nutrient supplement increases the birth size of infants of primiparous women in Ghana 1-3. Am. J. Clin. Nutr. 2015, 101, 835–881. [Google Scholar] [CrossRef]
- Arimond, M.; Zeilani, M.; Jungjohann, S.; Brown, K.H.; Ashorn, P.; Allen, L.H.; Dewey, K.G.; Dewey, K. Considerations in developing lipid-based nutrient supplements for prevention of undernutrition: Experience from the International Lipid-Based Nutrient Supplements (iLiNS) Project. Matern. Child Nutr. 2015, 11, 31–61. [Google Scholar] [CrossRef]
- Dewey, K.G.; Mridha, M.K.; Matias, S.L.; Arnold, C.D.; Cummins, J.R.; Khan, M.S.A.; Maalouf-Manasseh, Z.; Siddiqui, Z.; Ullah, M.B.; Vosti, S.A. Lipid-based nutrient supplementation in the first 1000 d improves child growth in Bangladesh: A cluster-randomized effectiveness trial. Am. J. Clin. Nutr. 2017, 105, 944–957. [Google Scholar] [CrossRef]
- Hess, S.Y.; Abbeddou, S.; Jimenez, E.Y.; Somé, J.W.; Vosti, S.A.; Ouédraogo, Z.P. Small-Quantity Lipid-Based Nutrient Supplements, Regardless of Their Zinc Content, Increase Growth and Reduce the Prevalence of Stunting and Wasting in Young Burkinabe Children: A Cluster-Randomized Trial. PLoS ONE 2015, 10, 122242. [Google Scholar] [CrossRef] [PubMed]
- Mridha, M.K.; Matias, S.L.; Chaparro, C.M.; Paul, R.R.; Hussain, S.; Vosti, S.A.; Harding, K.L.; Cummins, J.R.; Day, L.T.; Saha, S.L.; et al. Lipid-based nutrient supplements for pregnant women reduce newborn stunting in a cluster-randomized controlled effectiveness trial in Bangladesh. Am. J. Clin. Nutr. 2016, 103, 236–249. [Google Scholar] [CrossRef] [PubMed]
- Adu-Afarwuah, S.; Lartey, A.; Zeilani, M.; Dewey, K.G. Acceptability of lipid-based nutrient supplements (LNS) among Ghanaian infants and pregnant or lactating women. Matern. Child Nutr. 2011, 7, 344–356. [Google Scholar] [CrossRef] [PubMed]
- Matias, S.L.; Chaparro, C.M.; Perez-Exposito, A.B.; Peerson, J.M.; Dewey, K.G. Acceptability of a Lipid-Based Nutrient Supplement among Guatemalan Infants and Young Children; FANTA: Washington, DC, USA, 2011. [Google Scholar]
- Phuka, J.; Ashorn, U.; Ashorn, P.; Zeilani, M.; Cheung, Y.B.; Dewey, K.G.; Manary, M.; Maleta, K. Acceptability of three novel lipid-based nutrient supplements among Malawian infants and their caregivers. Matern. Child Nutr. 2011, 7, 368–377. [Google Scholar] [CrossRef]
- Kroker-Lobos, M.F.; Pedroza-Tobias, A.; Pedraza, L.S.; Rivera, J.A. The double burden of undernutrition and excess body weight in Mexico. Am. J. Clin. Nutr. 2014, 100, 1652S–1658S. [Google Scholar] [CrossRef]
- Rivera, J.A.; Barquera, S.; González-Cossío, T.; Olaiz, G.; Sepúlveda, J. Nutrition transition in Mexico and in other Latin American countries. Nutr. Rev. 2004, 62, S149–S157. [Google Scholar] [CrossRef]
- World Health Organization. Infant and Young Child Feeding: Model Chapter for Textbooks for Medical Students and Allied Health Professionals; WHO: Geneva, Switzerland, 2009. [Google Scholar]
- Desor, J.A.; Maller, O.; Turner, R.E. Taste in acceptance of sugars by human infants. J. Comp. Physiol. Psychol. 1973, 84, 496–501. [Google Scholar] [CrossRef]
- Maone, T.R.; Mattes, R.D.; Bernbaum, J.C.; Beauchamp, G.K. A new method for delivering a taste without fluids to preterm and term infants. Dev. Psychobiol. 1990, 23, 179–191. [Google Scholar] [CrossRef]
- Forestell, C.A.; Mennella, J.A. Early determinants of fruit and vegetable acceptance. Pediatrics 2007, 120, 1247–1254. [Google Scholar] [CrossRef]
- Mennella, J.A.; Nicklaus, S.; Jagolino, A.L.; Yourshaw, L.M. Variety is the spice of life: Strategies for promoting fruit and vegetable acceptance during infancy. Physiol. Behav. 2008, 94, 29–38. [Google Scholar] [CrossRef]
- Sullivan, S.A.; Birch, L.L. Pass the Sugar, Pass the Salt: Experience Dictates Preference. Dev. Psychol. 1990, 26, 546–551. [Google Scholar] [CrossRef]
- Sullivan, S.A.; Birch, L.L. Infant Dietary Experience and Acceptance of Solid Foods. Pediatrics 1994, 93, 271–277. [Google Scholar] [PubMed]
- Wardle, J.; Herrera, M.L.; Cooke, L.; Gibson, E.L. Modifying children’s food preferences: The effects of exposure and reward on acceptance of an unfamiliar vegetable. Eur. J. Clin. Nutr. 2003, 57, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Birch, L.L.; McPhee, L.; Shoba, B.C.; Pirok, E.; Steinberg, L. What kind of exposure reduces children’s food neophobia?. Looking vs. tasting. Appetite 1987, 9, 171–178. [Google Scholar] [CrossRef]
- Caton, S.J.; Blundell, P.; Ahern, S.M.; Nekitsing, C.; Olsen, A.; Møller, P.; Hausner, H.; Remy, E.; Nicklaus, S.; Chabanet, C.; et al. Learning to Eat Vegetables in Early Life: The Role of Timing, Age and Individual Eating Traits. PLoS ONE 2014, 9, e97609. [Google Scholar] [CrossRef]
- Hess, S.Y.; Bado, L.; Aaron, G.J.; Ouédraogo, J.B.; Zeilani, M.; Brown, K.H. Acceptability of zinc-fortified, lipid-based nutrient supplements (LNS) prepared for young children in Burkina Faso. Matern. Child Nutr. 2011, 7, 357–367. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95. [Google Scholar] [CrossRef]
- Wold Health Organization Multicentre Growth Reference Study Group. WHO Child Growth Standards Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age Methods and Development Department of Nutrition for Health and Development; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- Wooldridge, J.M. Count, Fractional and Other Nonnegative Responses. In Econometric Analysis of Cross Section and Panel Data; MIT Press: Cambridge, MA, USA, 2010. [Google Scholar]
- Galef, B.G.; Sherry, D.F. Mother’s milk: A medium for transmission of cues reflecting the flavor of mother’s diet. J. Comp. Physiol. Psychol. 1973, 83, 374–378. [Google Scholar] [CrossRef]
- Hepper, P.G.; Wells, D.L.; Dornan, J.C.; Lynch, C. Long-term flavor recognition in humans with prenatal garlic experience. Dev. Psychobiol. 2013, 55, 568–574. [Google Scholar] [CrossRef]
- Mennella, J.A.; Beauchamp, G.K. Maternal Diet Alters the Sensory Qualities of Human Milk and the Nursling’s Behavior. Pediatrics 1991, 88, 737–744. [Google Scholar]
- Mennella, J.A.; Beauchamp, G.K. The effects of repeated exposure to garlic-flavored milk on the nursling’s behavior. Pediatr. Res. 1993, 34, 805–808. [Google Scholar] [CrossRef] [PubMed]
- Mennella, J.A.; Jagnow, C.P.; Beauchamp, G.K. Prenatal and postnatal flavor learning by human infants. Pediatrics 2001, 107. [Google Scholar] [CrossRef] [PubMed]
- Mennella, J.A.; Johnson, A.; Beauchamp, G.K. Garlic ingestion by pregnant women alters the odor of amniotic fluid. Chem. Senses 1995, 20, 207–209. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, R.J.; Whybrow, S. Energy density, diet composition and palatability: Influences on overall food energy intake in humans. Physiol. Behav. 2004, 81, 755–764. [Google Scholar] [CrossRef]
- Williams, R.A.; Roe, L.S.; Rolls, B.J. Assessment of satiety depends on the energy density and portion size of the test meal. Obesity 2014, 22, 318–324. [Google Scholar] [CrossRef]
- Ramsay, S.A.; Roe, A.J.; Davis, J.N.; Price, W.J.; Johnson, S.L. Repeated exposures and child centered nutrition phrases increases young children’s consumption and liking of lentils. Food Qual. Prefer. 2017, 62, 317–322. [Google Scholar] [CrossRef]
- Ventura, A.K.; Worobey, J. Early influences on the development of food preferences. Curr. Biol. 2013, 23, R401–R408. [Google Scholar] [CrossRef]
- Jønsson, S.R.; Angka, S.; Olsen, K.; Tolver, A.; Olsen, A. Repeated exposure to vegetable-enriched snack bars may increase children’s liking for the bars—But not for the vegetables. Appetite 2019, 140, 1–9. [Google Scholar] [CrossRef]
- Dalenberg, J.R.; Nanetti, L.; Renken, R.J.; de Wijk, R.A.; ter Horst, G.J. Dealing with Consumer Differences in Liking during Repeated Exposure to Food; Typical Dynamics in Rating Behavior. PLoS ONE 2014, 9, e93350. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | LNS-U n = 28 | LNS-S n = 28 | Total n = 56 |
|---|---|---|---|
| Caregiver characteristics | |||
| Age, years | 26.4 ± 5.5 | 27.7 ± 7.1 | 27.52 ± 6.23 |
| Parity | 2.1 ± 1.2 | 2.0 ± 0.9 | 2.12 ± 1.06 |
| BMI, kg/m2 | 25.5 ± 5.1 | 26.8 ± 4.5 | 26.2 ± 4.8 |
| Relationship to child | |||
| Mother | 27 (96.4) | 27 (96.4) | 27 (96.4) |
| Grandmother | 1 (3.6) | 1 (3.6) | 1 (3.6) |
| Marital Status | |||
| Married, living with partner | 5 (17.9) | 6 (21.4) | 11 (19.6) |
| Free union | 17 (60.7) | 19 (67.9) | 36 (64.3) |
| Other 2 | 6 (21.4) | 3 (10.7) | 9 (16.1) |
| Education level completed | |||
| None 3 | 0 (0.0) | 1 (3.6) | 1 (3.6) |
| Elementary school | 7 (25.0) | 7 (25.0) | 14 (25.0) |
| Middle school | 13 (46.4) | 13 (46.4) | 26 (46.4) |
| High school | 5 (17.7) | 3 (10.7) | 8 (14.3) |
| Technical or college/university | 3 (10.7) | 4 (14.3) | 7 (12.5) |
| Occupation | |||
| Stays at home | 21 (75.0) | 26 (92.9) | 47 (83.9) |
| Formal or informal work 4 | 7 (25.0) | 2 (7.1) | 9 (16.1) |
| Child characteristics | |||
| Gestational age at birth | 39.3 ± 1.4 | 39.4 ± 1.0 | 39.4 ± 1.2 |
| Age category | |||
| 7 to 12 months | 14 (50.0) | 12 (42.9) | 26 (46.4) |
| 13 to 24 months | 14 (50.0) | 16 (57.1) | 30 (53.6) |
| Sex | |||
| Male | 17 (60.7) | 7 (25.0) | 24 (42.9) |
| Female | 11 (39.3) | 21 (75.0) | 32 (57.1) |
| Nutritional status indicators | |||
| Length, cm | 76.8 ± 6.1 | 74.6 ± 6.0 | 75.7 ± 6.1 |
| Weight, kg | 10.0 ± 1.5 | 9.1 ± 1.3 | 9.5 ± 1.4 |
| Length for age, LAZ | −0.5 ± 1.0 | −1.1 ± 1.0 | −0.8 ± 1.0 |
| Weight for age, WAZ | −0.1 ± 1.0 | −0.6 ± 0.9 | −0.3 ± 1.0 |
| Weight for length, WLZ | 0.3 ± 0.9 | −0.1 ± 1.0 | 0.1 ± 1.0 |
| BMIZ | 0.3 ± 0.9 | 0.02 ± 0.97 | 0.2 ± 0.9 |
| Household characteristics | |||
| Food insecurity | 23 (85.2) | 21 (75.0) | 44 (80.0) |
| Available services | |||
| Electricity | 28 (100.0) | 28 (100.0) | 56 (100.0) |
| Pipe water in home 5 | 26 (92.9) | 26 (92.9) | 52 (92.8) |
| Sanitary facility (toilet) 6 | 19 (67.8) | 23 (82.1) | 42 (75.0) |
| Bottled water | 23 (85.2) | 22 (78.6) | 45 (81.8) |
| LNS-U n = 28 | LNS-S n = 28 | LNS-S vs. LNS-U | |
|---|---|---|---|
| Raw estimates | |||
| Initial, % | 44.0 (31.4, 58.5) | 34.8 (25.3, 44.0) | −9.2 (−25.5, 6.0) |
| Final, % | 38.5 (27.8, 54.0) | 31.5 (21.6, 43.0) | −7.0 (−24.5, 8.9) |
| Change | −5.5 (−21.0, 9.3) | −3.3 (−16.8, 13.6) | 2.2 (−17.2, 24.4) |
| Covariate-adjusted estimates | |||
| Initial, % | 38.1 (26.3, 50.8) | 40.1 (30.4, 50.7) | 2.1 (−14.3, 18.1) |
| Final, % | 34.4 (22.6, 47.0) | 36.7 (25.4, 48.9) | 2.3 (−15.1, 19.3) |
| Change | −3.6 (−18.1, 11.5) | −3.4 (−17.1, 12.2) | 0.2 (−20.3, 18.7) |
| LNS-U n = 28 | LNS-S n = 28 | LNS-S vs. LNS-U | |
|---|---|---|---|
| Raw estimates | |||
| Initial, % | 42.9 (17.9, 57.1) | 39.3 (25.0, 60.7) | −3.6 (−32.1, 17.9) |
| Final, % | 32.1 (17.9, 53.6) | 25.0 (10.7, 42.9) | −7.1 (−28.6, 17.9) |
| Change | −10.7 (−32.1, 14.3) | −14.3 (−39.3, 10.7) | −3.6 (−32.1, 32.1) |
| Covariate-adjusted estimates | |||
| Initial, % | 32.1 (17.5, 52.3) | 47.9 (28.3, 65.6) | 15.7 (−10.3, 40.5) |
| Final, % | 25.5 (12.3, 43.6) | 33.4 (15.3, 52.3) | 7.9 (−17.7, 31.2) |
| Change | −6.6 (−27.6, 14.4) | −14.5 (−40.3, 10.7) | −7.9 (−41.7, 24.8) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okronipa, H.; Quezada-Sánchez, A.D.; Johnson, S.L.; Rawlinson, C.; Pacheco-Miranda, S.; Venosa López, M.; Gonzalez Navarrete, W.; Arenas, A.B. Effect of Added Sugar on the Consumption of A Lipid-Based Nutrient Supplement Among 7–24-Month-Old Children. Nutrients 2020, 12, 3069. https://doi.org/10.3390/nu12103069
Okronipa H, Quezada-Sánchez AD, Johnson SL, Rawlinson C, Pacheco-Miranda S, Venosa López M, Gonzalez Navarrete W, Arenas AB. Effect of Added Sugar on the Consumption of A Lipid-Based Nutrient Supplement Among 7–24-Month-Old Children. Nutrients. 2020; 12(10):3069. https://doi.org/10.3390/nu12103069
Chicago/Turabian StyleOkronipa, Harriet, Amado D. Quezada-Sánchez, Susan L. Johnson, Cloe Rawlinson, Selene Pacheco-Miranda, Mónica Venosa López, Wendy Gonzalez Navarrete, and Anabelle Bonvecchio Arenas. 2020. "Effect of Added Sugar on the Consumption of A Lipid-Based Nutrient Supplement Among 7–24-Month-Old Children" Nutrients 12, no. 10: 3069. https://doi.org/10.3390/nu12103069
APA StyleOkronipa, H., Quezada-Sánchez, A. D., Johnson, S. L., Rawlinson, C., Pacheco-Miranda, S., Venosa López, M., Gonzalez Navarrete, W., & Arenas, A. B. (2020). Effect of Added Sugar on the Consumption of A Lipid-Based Nutrient Supplement Among 7–24-Month-Old Children. Nutrients, 12(10), 3069. https://doi.org/10.3390/nu12103069